
Abstract
Elotuzumab is a humanized monoclonal antibody targeting the extracellular domain of signaling lymphocytic activation molecule F7 (SLAMF7) highly expressed in multiple myeloma cells. Upon binding to myeloma cells, elotuzumab exerts its cytotoxic effects through antibody-dependent cellular cytotoxicity, the antibody-induced selective lysis of tumor cells by activated natural killer (NK) cells. Furthermore, elotuzumab has been shown to directly induce NK-cell activation by binding to SLAMF7 expressed on NK cells and to indirectly modulate T-cell function by promoting the secretion of cytokines from NK cells. In combination with lenalidomide and low-dose dexamethasone, elotuzumab has shown remarkable effects in patients with relapsed or refractory multiple myeloma. In these patients, the risk of disease progression or death was significantly reduced by 30% on elotuzumab. Currently, elotuzumab is being evaluated in various myeloma patient populations and combination regimens. This review discusses the use of elotuzumab as an antimultiple myeloma agent and provides an update on the results of recent clinical trials evaluating the safety and efficacy of elotuzumab for the treatment of multiple myeloma.
Introduction
Multiple myeloma (MM) is a mature B-cell malignancy characterized by monoclonal expansion of plasma cells in the bone marrow leading to bone destruction and marrow failure and accompanied by excessive production of monoclonal immunoglobulins (Igs) that produce an ‘M spike’ on serum protein electrophoresis [Raab et al. 2009]. In the United States (US), it accounts for an estimated 26,850 new cases diagnosed in 2015 (1.6% of all new cancer cases), with 11,240 deaths (1.9% of all cancer deaths) [Siegel et al. 2015]. In Europe, an estimated 40,570 new cases are expected for 2015, with 25,398 deaths [WHO and IARC, 2012].
Increased knowledge and understanding of the pathogenesis of MM has prompted the development of second- and third-generation proteasome inhibitors (PIs), immunomodulatory drugs (IMiDs) and alkylators, which has significantly improved outcome for patients with MM [Mateos et al. 2013]. Furthermore, drugs with novel mechanisms of action have been tested in relapsed/refractory MM (RRMM), such as agents acting on the cell cycle, epigenetic modifiers, agents acting on the unfolded protein response, signaling pathway inhibitors, and kinase inhibitors [Ocio et al. 2014]. Despite substantial progress to identify the selective vulnerability created by the underlying genomic instability and its clinical translation, MM remains an incurable disease with frequent relapse or development of drug resistance, indicating a significant unmet need for novel agents to treat this patient population.
Immunotherapy bears significant promise in myeloma treatment. Various immunotherapeutic approaches are currently being employed or evaluated, such as allogeneic stem cell transplantation, adoptive cellular immunotherapy, dendritic cell vaccines, chimeric antigen receptor (CAR) T-cell therapy and natural killer (NK)-cell-based therapies [Ayed et al. 2015]. In combination with other agents, antibody-based immunotherapy is employed in tailored regimens for patients with advanced disease. Monoclonal antibodies (mAbs) allow for the selective targeting of antigens on the myeloma cell and include cell-surface proteins involved in signaling, tumor growth and survival, such as growth factors and their receptors and adhesion molecules. Other targets include cellular and noncellular components of the bone marrow microenvironment that interact with myeloma cells, such as soluble growth factors and NK cells [Sondergeld et al. 2015; van de Donk et al. 2012].
The cytotoxic effects of mAbs may be executed by a variety of mechanisms including direct induction of growth arrest or apoptosis via targeting of signaling pathways, activation of macrophages via antibody-dependent cell-mediated phagocytosis, activation of the complement system to induce complement-dependent cytotoxicity (CDC) or activation of NK cells to induce antigen-dependent cellular cytotoxicity (ADCC) [Sondergeld et al. 2015; Golay and Introna, 2012; Richardson et al. 2011].
SLAMF7 as a therapeutic target
Signaling lymphocytic activation molecule (SLAM) family receptors are expressed in hematopoietic cells and play critical roles in normal immune regulation [Veillette and Guo, 2013]. Most of these receptors are ‘self-ligands’ (i.e. they recognize another molecule of the same receptor present on another cell as a ligand). Accordingly, SLAM family receptors can be triggered by interactions between either identical or different types of hematopoietic cells. The cytoplasmic tail of SLAM family receptors includes one or more immunoreceptor tyrosine-based switch motifs (ITSMs). Upon extracellular interaction, intracellular ITSMs undergo tyrosine phosphorylation and mediate binding to the SLAM-associated protein (SAP) family of adaptors: SAP and Ewing’s sarcoma-associated transcript 2 (EAT-2). Through recruiting downstream effectors in the presence or absence of the SAP family adaptors, the SLAM family receptors may mediate activating or inhibitory effects on immune cells [Liu et al. 2014; Cannons et al. 2011].
SLAMF7 (CS1; CCND3 subset 1; CRACC) is a cell-surface glycoprotein universally and highly expressed on normal and malignant plasma cells. SLAMF7 possesses one ITSM in its cytoplasmic domain and recruits EAT-2 to mediate activating effects. SLAMF7 has two isoforms, CS1-long (CS1-L) and CS1-short (CS1-S), which differ in the cytoplasmic domain and exhibit differential expression patterns among immune cells [Lee et al. 2007]. High SLAMF7 expression was observed in MM cells from various patient populations independent of high- or low-risk molecular profiles, molecular subtypes or the presence of cytogenetic abnormalities [Hsi et al. 2008; Tai et al. 2008]. SLAMF7 is not expressed by normal tissues or stem cells, with the exception of some leukocyte subsets, in particular NK cells, NK-like T cells, CD8+ T cells, activated monocytes and dendritic cells, which have lower expression levels compared with malignant plasma cells [Hsi et al. 2008].
SLAMF7 also exists as a soluble form (sSLAMF7). Low levels of circulating sSLAMF7 were detectable in the serum of patients with MM, but not in healthy donors [Tai et al. 2008]. Patients showed a significant decrease in free sSLAMF7 after treatment with bortezomib/dexamethasone or lenalidomide/dexamethasone, either with or without elotuzumab, suggesting a potential use of free sSLAMF7 as a surrogate for disease burden [Postelnek et al. 2015]. Furthermore, a significant dose- and time-dependent increase in sSLAMF7 following elotuzumab therapy has been observed, which likely reflected stabilization of the protein by binding to elotuzumab.
SLAMF7 was shown to be implicated in the activation of NK cell-mediated cytotoxicity and may play a role in the regulation of B lymphocyte proliferation during immune responses [Lee et al. 2007]. In NK cells, SLAMF7 mediates activating or inhibitory effects, depending on whether cells express or do not express the adaptor EAT-2 [Guo et al. 2015; Pérez-Quintero et al. 2014]. The precise function of SLAMF7 in MM is still unclear. SLAMF7 was expressed at adhesion-promoting uropod membranes of polarized MM cells. Short interfering RNA (siRNA) targeted to SLAMF7 inhibited MM cell adhesion to bone marrow stromal cells (BMSCs) suggesting that SLAMF7 may be involved in cell–cell adhesion [Tai et al. 2008].
Studies with SLAMF7-specific CARs confirmed the suitability of SLAMF7 as a potential target in MM. Both NK cells [Chu et al. 2014a] and T cells [Chu et al. 2014b] expressing second-generation CARs based on a single chain variable fragment of an antibody related to elotuzumab effectively redirected NK and T cells to secrete cytokines, degranulate and exhibit cytotoxic activity in response to MM cell lines and primary human myeloma cells in vitro. SLAMF7-directed NK and T cells also inhibited tumor growth and prolonged survival in an orthotopic MM xenograft mouse model [Chu et al. 2014a, 2014b].
Elotuzumab mechanism of action
Elotuzumab (EMPLICITI®, formerly HuLuc63) is a humanized IgG1 monoclonal antibody (mAb) targeting the extracellular domain of human SLAMF7, but does not interact with other members of the SLAM family [Veillette and Guo, 2013]. Elotuzumab was shown to induce lysis of human MM cell lines and primary myeloma cells in vitro in the presence of peripheral blood mononuclear cells or purified NK cells. Lysis was observed even in tumor cells of patients with MM resistant or refractory to standard therapies. In vivo, efficacy was observed in various xenograft models of human myeloma. Intravenous elotuzumab significantly induced tumor regression by triggering autologous ADCC against MM cells, an antibody-induced, selective lysis of tumor cells by activated NK cells [Hsi et al. 2008; Tai et al. 2008]. The Fab portion of elotuzumab binds the SLAMF7 expressed on MM cells, while the Fc portion of elotuzumab binds the activating Fc receptor CD16 on NK cells (Figure 1). These interactions trigger NK cell activation, release of cytotoxic granules and killing of the MM cells [Liu et al. 2014; Veillette and Guo, 2013].

Elotuzumab mechanism of action. The primary mechanism of action of elotuzumab against myeloma cells is NK cell-mediated ADCC (B). Elotuzumab also activates NK cells directly via SLAMF7 binding (A).
After administration of elotuzumab, no signals of CDC were detected. Furthermore, elotuzumab alone could not induce antiproliferation signals or cell death in MM cells. To mediate the antitumor activity of elotuzumab towards myeloma cells, the presence of functional NK cells was required [Hsi et al. 2008; Tai et al. 2008].
In addition to ADCC, elotuzumab directly induces activation of NK cells by binding to SLAMF7 expressed on NK cells (Figure 1). Upon ligation to SLAMF7 on NK cells, elotuzumab increased the percentage of NK cells expressing CD69 and CD69MFI, stimulatory receptors triggering NK cell-mediated cytolytic activity. Furthermore, elotuzumab induced interferon (IFN)-γ production and enhanced granzyme B release, promoting cytotoxicity against SLAMF7-positive MM cells but not against autologous SLAMF7-positive NK cells. This process appeared to be mediated by recruitment of the SAP adapter EAT-2 in NK cells and was associated with phosphorylation of downstream signal transduction proteins such as the extracellular signaling-regulated kinase (ERK), implicated in NK cell activation and cytotoxicity [Collins et al. 2013].
Elotuzumab may also interfere with adhesion of MM cells to bone marrow stem cells (BMSC) and thus add to the NK cell mediated antitumor activity. Although B-cell tumorigenesis results from genetic anomalies, the tumor microenvironment contributes significantly to the malignant transformation and pathogenesis [Shain et al. 2015]. Cell adhesion has been demonstrated to protect tumor cells from cell death through a number of mechanisms [Shain and Dalton, 2001]. In MM, the interactions of MM cells with the bone marrow microenvironment play a crucial role in cell survival, cell trafficking and drug resistance. In vitro, elotuzumab blocked SLAMF7-mediated adhesion of MM cells to BMSCs in a dose-dependent manner [Tai et al. 2008]. In the presence of BMSCs, elotuzumab inhibited MM cell viability, suggesting that elotuzumab may overcome the stimulatory effects of BMSCs on MM growth and survival and may enhance the sensitivity of MM cells to chemotherapy. Interestingly, binding of elotuzumab to SLAMF7-positive cells did not activate downstream signaling in MM cells, which is thought to be due to lack of intracellular EAT-2 in these cells [Collins et al. 2013].
Clinical studies of elotuzumab in multiple myeloma
Activity, efficacy and safety of elotuzumab alone and in combination with other agents have been assessed in several phase I–III clinical studies and are currently being further explored. An overview of completed and ongoing clinical studies of elotuzumab for the treatment of patients with MM is presented in Table 1.
Completed and ongoing clinical studies with elotuzumab in multiple myeloma.

ASCT, autologous stem cell transplant; B, bortezomib; d, low dose dexamethasone; Di, diphenhydramine; DLT, dose-limiting toxicity; E, elotuzumab; ESRD, end-stage renal disease; HR, hazard ratio; L, lenalidomide; MM, multiple myeloma; MTD, maximum tolerated dose; N, nivolumab; NRF, normal renal function; ORR, objective response rate; P, pomalidomide; PFS, progression-free survival; PK, pharmacokinetics; Pts, patients; R, ranitidine; RRMM, relapsed or refractory multiple myeloma; SD, stable disease; SLAMF7, signaling lymphocytic activation molecule F7; SRI, severe renal impairment, TTP, time to progression
The first-in-man study of elotuzumab (Study 1701) evaluated the safety and tolerability as well as pharmacokinetics and pharmacodynamics of elotuzumab in patients with RRMM. SLAMF7 receptors of marrow-derived CD38+ cells were found to be reliably saturated at dose levels of 10 and 20 mg elotuzumab per kg bodyweight administered intravenously every 2 weeks [Zonder et al. 2012]. While no objective responses were observed in this heavily pretreated patient population, nine patients (26.5%) had stable disease (SD) after four administrations of elotuzumab. Dose-limiting toxicities (DLTs) of elotuzumab were observed in one patient at 2.5 mg/kg and one patient at 20 mg/kg and included an episode of grade 3 increased serum creatinine and a grade 3 hypersensitivity reaction that resolved spontaneously within 24 hours, respectively. No maximum tolerated dose (MTD) was identified up to the maximum planned dose of 20 mg/kg. In general, adverse events (AEs) were mild to moderate in severity. Infusion reactions were among the most common AEs associated with elotuzumab and usually presented as chills, pyrexia, headache and flushing. The infusion-related AEs were mitigated by implementation of a premedication regimen consisting of methylprednisolone, diphenhydramine and paracetamol/acetaminophen prior to each elotuzumab infusion.
Currently a phase II biomarker study [ClinicalTrials.gov identifier: NCT1441973] is ongoing administering elotuzumab monotherapy to patients with high risk smoldering MM (Table 1). Sequential dose cohorts of 20 mg/kg elotuzumab once monthly or 10 mg/kg elotuzumab twice monthly will be analyzed for elotuzumab-induced changes in monoclonal protein and the percentage of NK cell subpopulations such as CD56dim/CD16+/CD3-/CD45+ NK cells in the bone marrow.
Elotuzumab is also being evaluated in combination with established MM therapies such as lenalidomide or bortezomib (Table 1). In ongoing studies, even quadruple regimens of elotuzumab, bortezomib, lenalidomide and dexamethasone are being assessed [ClinicalTrials.gov identifiers: NCT01668719, NCT02375555].
Combination therapy with lenalidomide
Lenalidomide is an IMiD approved for newly diagnosed MM patients ineligible for stem cell transplantation and, in combination with dexamethasone, for patients with relapsed MM. Its mechanisms of action involve multiple processes including enhancement of T-cell and NK-cell functions, suppression of angiogenesis, inhibition of tumor necrosis factor (TNF)-α production and direct repression of tumor cell growth [Chanan-Khan and Cheson, 2008; Weber et al. 2007].
Preclinically, the induction of myeloma cell death by elotuzumab was further enhanced when combined with lenalidomide. The combination of elotuzumab plus lenalidomide demonstrated superior anti-myeloma activity in in vitro and in vivo models of MM than either agent alone (Figure 2). On combination treatment, myeloma cell killing was enhanced by modulating NK cell function that coincided with the upregulation of adhesion and activation markers, including interleukin (IL)-2Rα expression, IL-2 production by CD3+CD56+ lymphocytes and TNF-α production [Balasa et al. 2015].

Antitumor effects of elotuzumab in combination with lenalidomide in a human xenograft mouse model of multiple myeloma. In a myeloma mouse xenograft model, the combination of elotuzumab plus lenalidomide significantly reduced tumor volume compared with either agent alone. Mice with established OPM2 xenograft tumors (average of ~100 mm2) were randomized into treatment groups (n = 8/group) and treated with control IgG1, lenalidomide + control IgG1, elotuzumab or elotuzumab + lenalidomide. Inverted triangles depict elotuzumab (filled) or lenalidomide (empty) dosing. (Reproduced from Balasa and colleagues [Balasa et al. 2015] © The Author(s) 2014).
Clinical data from a phase I/II study (Study 1703) of intravenous elotuzumab in combination with lenalidomide and low dose dexamethasone (E-L/d) demonstrated an overall response rate (ORR) of 84% and a median progression-free survival (PFS) of 29 months in patients with RRMM [Richardson et al. 2015], thus leading to two large phase III trials of this treatment regimen in first and second line settings (Study ELOQUENT-1 in patients with newly diagnosed, previously untreated MM and Study ELOQUENT-2 in patients with RRMM). For these studies, 28-day treatment cycles and a dosing schedule of 10 mg/kg on days 1, 8, 15, and 22 during the first two cycles and then on days 1 and 15 starting with the third cycle have been selected for elotuzumab. While ELOQUENT-1 is still ongoing, interim data of ELOQUENT-2 confirmed the previous results in patients with RRMM (Table 1). Treatment with lenalidomide/dexamethasone with or without elotuzumab (E-L/d versus L/d) showed an ORR of 79% on elotuzumab versus 66% on control treatment. With a median PFS of 19.4 months, patients receiving the triple combination had a significant relative reduction of 30% in the risk of disease progression or death [Lonial et al. 2015]. The PFS benefit of patients on E-L/d versus L/d was maintained over time as indicated by a 2-year PFS rate of 41% versus 27% and a 3-year PFS rate of 26% versus 18%, respectively. Accordingly, the PFS hazard ratio (HR) was 0.70 (95% CI 0.57–0.85; p = 0.0004) after 2 years and 0.73 (95% CI 0.60–0.89; p = 0.0014) after 3 years of follow up [Dimopoulos, 2015]. An interim analysis of overall survival (OS) revealed a HR of 0.77 (95% CI 0.61–0.97) indicating a strong trend (p = 0.0257) for treatment with E-L/d versus L/d [Dimopoulos, 2015].
In this phase III study, randomization of patients was stratified according to the baseline β2-microglobulin level, the number of previous therapies, and previous IMiD therapy. Patient baseline characteristics were balanced between the treatment groups of each study and reflected well the heterogeneous patient population characteristic for RRMM. With respect to PFS, the benefit of treatment with elotuzumab was consistent across various patient subgroups, including patients with resistance to the most recent line of therapy and those who had previous exposure to bortezomib or IMiDs, were ⩾65 years of age or had a high-risk cytogenetic profile, particularly the presence of the del(17p) variant (Figure 3) [Lonial et al. 2015]. Multivariate analysis suggested that the greatest benefit in PFS occurred among patients in whom MM had been diagnosed ⩾3.5 years before study entry (HR 0.55; 95% CI 0.44–0.70; p < 0.001), with a median survival of 26.0 months in the elotuzumab group versus 17.3 months in the control group [Lonial et al. 2015].
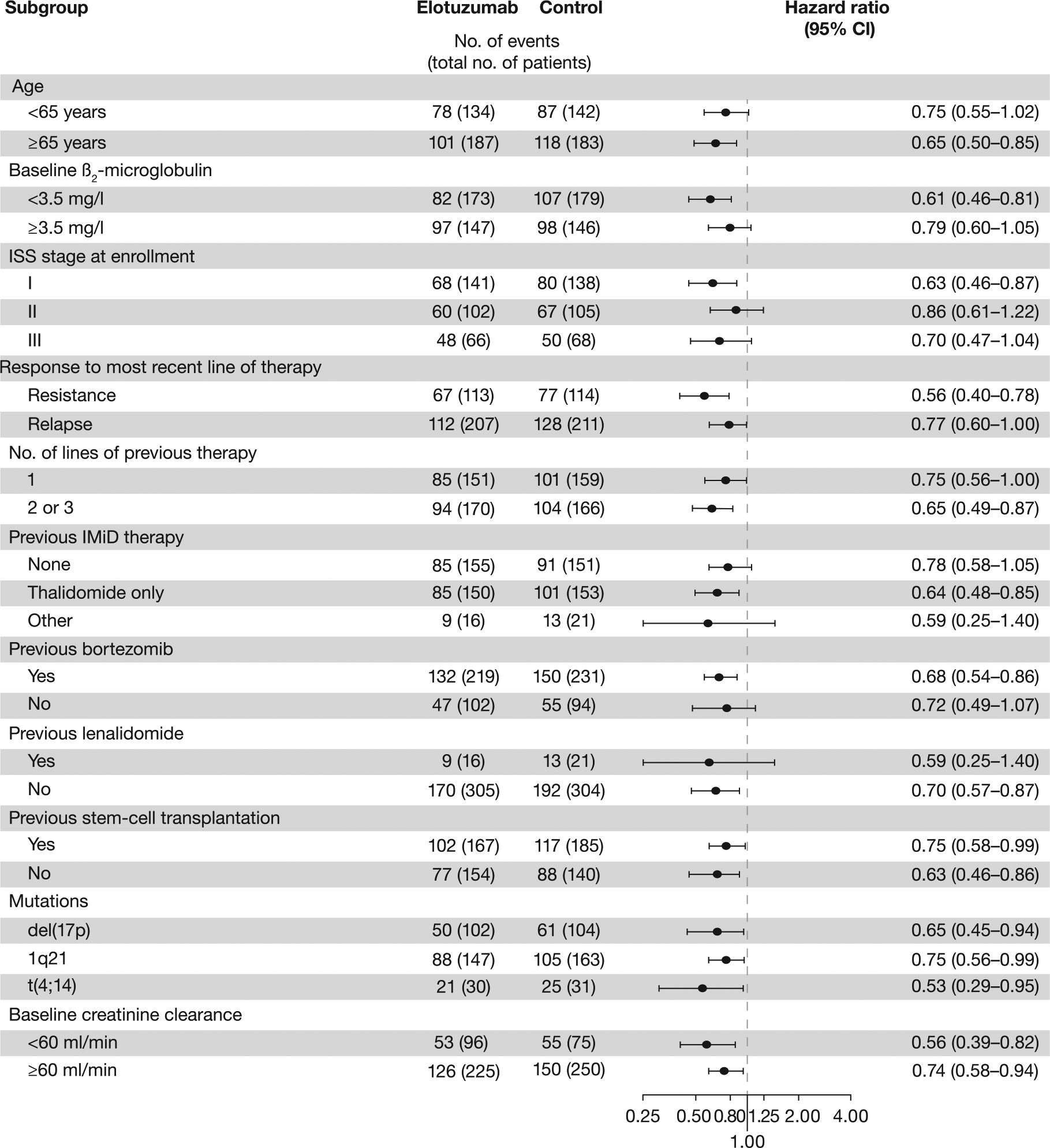
Subgroup analysis of progression-free survival in patients of Study ELOQUENT-2. The benefit for PFS on combination of elotuzumab plus lenalidomide and dexamethasone was consistent across key patient subgroups (From [Lonial et al. 2015] © 2015 Massachusetts Medical Society. Reprinted with permission).
Unfortunately, the influence of the IgG Fc receptor FcγRIIIa (CD16) gene polymorphism on PFS was not analyzed in this study. A high affinity ‘VV’ genotype of this receptor expressed on NK cells has been shown to result in enhanced ADCC [Weng and Levy, 2003; Cartron et al. 2002; see also next section: combination therapy with bortezomib]. Nevertheless, the benefit of E-L/d in PFS was further confirmed by means of multiple sensitivity analyses. Similar to PFS, the benefit in OS was also consistent across all predefined patient subgroups as indicated by the interim analysis performed after 3 years of follow up [Dimopoulos, 2015].
The combination of elotuzumab, lenalidomide and low-dose dexamethasone was generally well tolerated. The safety profile of intravenous elotuzumab was consistent across doses and did not appear to be dose-dependent. During dose-escalation, no DLTs were observed and the MTD was not reached at doses up to 20 mg/kg [Lonial et al. 2012]. In Study 1703, the most common treatment-emergent adverse events (TEAEs) included diarrhea, muscle spasms, fatigue, constipation and nausea. Overall, 57 patients (78%) had grade 3–4 AEs including lymphopenia in 15 patients and neutropenia in 14 patients [Richardson et al. 2015]. During phase III (Study ELOQUENT-2) [Lonial et al. 2015], addition of elotuzumab did not appear to increase the frequency or intensity of AEs known for the established combination of lenalidomide and dexamethasone. Hematological toxicities were frequently observed and comparable between the two treatment groups, except for lymphopenia of grade 3–4 which was observed in 77% of patients on elotuzumab versus 49% of patients in the control group. The increased rate of lymphopenia on elotuzumab may reflect alterations in lymphocyte trafficking, including NK cells. Despite this finding, there was no evidence of increased autoimmunity or other sequelae of immune dysregulation [Lonial et al. 2015]. Other common grade 3 or 4 AEs in the two treatment groups were fatigue and diarrhea. Serious AEs were reported in 65% and 57% of patients in the elotuzumab and the control group, respectively. In the elotuzumab group, infections were reported in 81% of patients versus 74% in the control group. After adjustment for drug exposure, rates of infection were equal in the two groups (197 events per 100 patient-years) [Lonial et al. 2015].
Infusion reactions such as pyrexia, chills, hypertension, nausea or rash were noted in only 10–11% of patients receiving elotuzumab [Lonial et al. 2015; Richardson et al. 2015]. Infusion reactions were mild to moderate in most patients and resolved the same day spontaneously or with treatment as indicated. No patient had a grade 4 or 5 reaction. Most infusion reactions (70%) occurred during the first dose of elotuzumab therapy and all but two patients continued treatment [Lonial et al. 2015]. To reduce the infusion time of elotuzumab, the flow rate was increased to 5 ml/min in several patients, resulting in an infusion time of <1 hour.
In patients with MM and various levels of renal impairment [ClinicalTrials.gov identifier: NCT-01393964] (Table 1), treatment with intravenous elotuzumab in combination with lenalidomide and dexamethasone did not reveal any significant differences in pharmacokinetic parameters or safety of elotuzumab [Berdeja et al. 2016]. Data collected in patients with normal renal function, severe renal impairment or end-stage renal disease support administration of elotuzumab without dose adjustment for renal function.
In summary, clinical study results were consistent with the preclinical data demonstrating synergy of elotuzumab in combination with lenalidomide. Data obtained in randomized controlled studies validate the added benefit of elotuzumab in patients with RRMM. Consequently, the US Food and Drug Administration (FDA) approved elotuzumab in combination with lenalidomide and dexamethasone for the treatment of patients with MM who have received one to three prior therapies.
The combination of elotuzumab and lenalidomide/dexamethasone is being further evaluated for the treatment of MM in several ongoing clinical studies (Table 1). Analyses include patients with earlier stages of MM (e.g. ELOQUENT-1), administration of elotuzumab as a 60 min infusion [ClinicalTrials.gov identifier: NCT021-59365] and determination of SLAMF7 expression of malignant plasma cells at progression [substudy of ClinicalTrials.gov identifier: NCT01-891643]. Furthermore, a quadruple combination regimen of elotuzumab, bortezomib, lenalidomide and dexamethasone is being explored in patients with newly diagnosed, high risk MM (SWOG S1211 study) and in patients with newly diagnosed, symptomatic MM [ClinicalTrials.gov identifier: NCT02375555]. The combination of elotuzumab plus lenalidomide, dexamethasone, diphenhydramine and ranitidine will be evaluated for maintenance therapy after autologous stem cell transplantation [ClinicalTrials.gov identifier: NCT02420860].
Combination therapy with bortezomib
Bortezomib is an oral PI approved for the treatment of patients with relapsed MM and is considered the standard of care for salvage therapy in both the US and EU. Bortezomib prevents degradation of ubiquitinated intracellular proteins by interfering with several cellular pathways including inhibition of nuclear factor (NF)ĸB and activation of caspase-8 and caspase-9, which results in apoptotic cell death [Strauss et al. 2007; Ling et al. 2003]. Of note, bortezomib was shown to enhance the susceptibility of tumor cells to NK cell-mediated killing [Hsi et al. 2008; Hallett et al. 2008].
In vitro, combination therapy of elotuzumab with bortezomib significantly lowered the half maximal effective concentration (EC50) of elotuzumab in myeloma cell lines and primary myeloma cells. Bortezomib enhanced ADCC-mediated MM cell death induced by elotuzumab via downregulation of the major histocompatibility complex (MHC) class I, an inhibitor of NK-cell function [van Rhee et al. 2009]. In vivo, combination therapy induced significantly better tumor growth inhibition compared with application of either agent alone. The mean tumor volumes were reduced by 89% (p < 0.001) and 87% (p < 0.001) compared with elotuzumab or bortezomib monotherapy, respectively. Bortezomib significantly potentiated the effects of elotuzumab, presumably by rendering myeloma more vulnerable to NK cell-mediated lysis [van Rhee et al. 2009].
Clinical data from a phase I study (Study 1702) of elotuzumab in combination with bortezomib in patients with RRMM revealed an ORR of 48% (13 of 27 evaluable patients; Table 1). 63% of patients (17 of 27 patients) achieved a minor response or better. Patients with high-risk cytogenetics exhibited an ORR of 70 % (7 of 10 patients). Notably, two of three patients (66.7%) refractory to bortezomib during prior treatments responded to the combination regimen. The median time to progression (TTP) was 9.46 months [Jakubowiak et al. 2012].
For a subsequent randomized controlled phase II study (Study CA204-009), 21-day treatment cycles and a dosing schedule of 10 mg/kg on days 1, 8 and 15 during the first two cycles, then on days 1 and 11 in cycle 3–8 and on days 1 and 15 of a 28-day cycle starting with the ninth cycle have been selected for elotuzumab. In 152 patients with RRMM, the combination of bortezomib and dexamethasone was evaluated with and without elotuzumab. A median PFS of 9.7 months was achieved on elotuzumab versus 6.9 months of the control group, leading to a PFS HR of 0.76 (p = 0.1256; Table 1). Stratified by prognostic factors, patients on elotuzumab even had a 38% reduction in the risk of progression or death. The 1-year PFS rate was 40% versus 33% and the 2-year PFS was 18% versus 11% in patients treated with elotuzumab or controls, respectively. An ORR of 66% was achieved in the elotuzumab group versus 63% in the control group. Early OS data favors the triple combination therapy including elotuzumab [Palumbo, 2015; Jakubowiak et al. 2015].
In this phase II study, randomization of patients was stratified and patient baseline characteristics were well balanced between the two treatment groups. As has been shown for the combination of elotuzumab with lenalidomide and dexamethasone, the benefit of treatment with elotuzumab in combination with bortezomib and dexamethasone was also consistent across various patient subgroups. Of note, a trend towards longer PFS was observed for patients homozygous for the high affinity FcγRIIIa V allele [Palumbo, 2015]. Polymorphism in the IgG Fc receptor FcγRIIIa gene (CD16) of NK cells has been described to influence the effectiveness of ADCC and antitumor effects following treatment with IgG1 antibodies [Weng and Levy, 2003; Cartron et al. 2002].
The combination of elotuzumab, bortezomib and low-dose dexamethasone was generally well tolerated. The safety profile of elotuzumab was consistent over time, with minimal incremental toxicity compared with bortezomib and dexamethasone alone. No DLTs were observed in the dose escalation phase (Study 1702); the MTD was not reached at doses up to 20 mg/kg elotuzumab in combination with bortezomib. The most frequent AEs (any grade) were fatigue (82%), anemia (71%), diarrhea (71%) and thrombocytopenia (68%), with the highest incidence of grade 3–4 AEs observed for lymphopenia (25%) and fatigue (14%). Overall, two elotuzumab-related serious AEs of chest pain and gastroenteritis occurred in one patient [Jakubowiak et al. 2012]. During phase II (Study 204-009), the most common AEs in patients treated with or without elotuzumab were infections and infestations (65 and 53%), diarrhea (43 and 33%), constipation (39 and 29%), cough (39 and 23%), anemia (37 and 28%), peripheral neuropathy (35 and 33%), and pyrexia (33 and 27%, respectively) [Jakubowiak, 2015]. Grade 3–4 AEs were reported in 53 patients (71%) on elotuzumab and 45 patients (60%) in the control group, and included thrombocytopenia in 7 patients (9%) versus 13 patients (17%) and infections in 17 patients (23%) versus 11 patients (15%) on elotuzumab versus controls, respectively [Palumbo et al. 2015].
Infusion reactions were noted in only five patients (7%) receiving elotuzumab, but were all of mild to moderate intensity (grade 1–2) and manageable. None of the patients discontinued due to an infusion reaction. There were no infusion reactions at the maximum planned infusion rate of 5 ml/min [Jakubowiak et al. 2015; Palumbo et al. 2015].
In summary, clinical results confirmed the nonclinical findings of additive to synergistic effects of a combination regimen with elotuzumab and bortezomib. In patients with RRMM, elotuzumab provides clinical benefit with limited added toxicity when combined with bortezomib and dexamethasone compared with bortezomib and dexamethasone alone. Data support the use of elotuzumab in combination with protease inhibitors.
Conclusion and future directions
Over the past decade, changes in myeloma treatment strategies have greatly improved patient outcomes. Despite these advances, MM remains an incurable disease. The current knowledge on pathogenesis and course of MM firmly supports the use of combination therapy rather than sequential administration of single agent therapies. With the development of new and highly active treatments including PIs, IMiDs and mAbs, triple or more combinations are expected to become the standard of care in MM, provided the selected combination regimens are safe and tolerable.
Elotuzumab is a first-in-class, humanized mAb directed against SLAMF7 receptors on the surface of MM cells. Monotherapy with elotuzumab demonstrated antitumor activity in patients with MM. In combination with established MM therapies, elotuzumab significantly increased the efficacy while being generally well tolerated. Data of randomized controlled trials revealed remarkable response and PFS rates for combination therapy of elotuzumab with lenalidomide or bortezomib being superior to the established treatment regimens. Of note, therapeutic effects with elotuzumab have actually been observed in elderly MM patients and in patients who have received several prior treatments for advanced disease. Addition of elotuzumab to combination therapy was associated with a similar safety profile as observed for lenalidomide or bortezomib alone, albeit with a higher incidence of infusion reactions and lymphopenia. However, both AEs were usually of mild to moderate intensities and manageable.
Data indicate that activation and engagement of the innate immune system to selectively kill myeloma cells can provide clinically meaningful and statistically significant improvements in myeloma patient outcomes. The antitumor immunity of elotuzumab is expected to be increased in patients with a functional immune system, hence data on treatment of patients at earlier stages are expected to confirm or even outperform the results of elotuzumab in RRMM. The selection of subgroups, such as patients with high affinity ‘VV’ genotype of the FcγRIIIa (CD16) receptor expressed on NK cells resulting in enhanced ADCC, may further increase the clinical benefit upon treatment with elotuzumab. Based on the observed efficacy together with a favorable safety profile, elotuzumab in combination with established therapies represents a new treatment option for patients with MM.
Ongoing clinical studies investigate therapies with elotuzumab in various MM patient populations including earlier stages and high-risk smoldering myeloma and in new treatment regimens such as the quadruple combination of elotuzumab, bortezomib, lenalidomide and dexamethasone. Nivolumab, an antibody targeting the immune checkpoint programmed cell death protein 1 (PD-1) on T cells resulting in a restored active T-cell response, is currently being evaluated in combination with elotuzumab, pomalidomide and dexamethasone in patients with RRMM [ClinicalTrials.gov identifier: NCT02726581]. In combination with other mAbs targeting myeloma cells (e.g. anti-CD38 antibodies such as daratumumab), elotuzumab may have the potential to overcome the resistance mechanisms frequently observed in patients with MM. Regimens will be optimized to best incorporate elotuzumab into existing strategies and to enable a more effective and targeted treatment of MM by evading mechanisms of resistance and improving patient outcomes.
Footnotes
Funding
Writing assistance was provided by Birgit Glasschroeder, PhD, and funded by Bristol-Myers Squibb.
Conflict of interest statement
The author has received travel grants, honoraria and research support from Celgene, Janssen, Novartis and Amgen.