
Abstract
The non-Hodgkin lymphomas (NHLs) are a heterogeneous group of diseases with variable clinical outcomes. Autologous hematopoietic stem-cell transplantation (ASCT) as frontline, consolidative therapy has been evaluated based upon histological subtype of NHL. In this review, we summarize the major clinical trials guiding the use of frontline ASCT in NHL. With the constantly changing landscape of upfront therapy and multiple promising novel agents, the ability to conduct randomized trials to evaluate the benefit of consolidative ASCT is not only challenging but may be considered by some an inept utilization of resources. Our recommendation for consolidative ASCT is based on analyzing the current available data.
Keywords
Introduction
Non-Hodgkin lymphomas (NHLs) account for about 4% of all malignancies in the United States. Despite a rising incidence, death rates from NHL have been steadily declining. Strategies that have paved the way to improved outcomes over the last decade include the introduction of chemo-immunotherapy, high-dose therapy (HDT) and autologous hematopoietic stem-cell transplantation (ASCT) consolidation, allogeneic transplantation, decreased treatment-related toxicities, and reduced mortality due to improved supportive care. These modalities have undoubtedly improved survival rates. Disease relapse following upfront therapy remains problematic.
ASCT was first used as frontline, consolidative treatment for aggressive NHL in the early 1990s [Greb et al. 2008]. Since that time there have been numerous trials comparing frontline, consolidative ASCT with chemotherapy alone in patients with diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL). The management of patients with mantle cell lymphoma (MCL) poses a challenge due to an increased risk of relapse following initial remission. ASCT consolidation is an appropriate frontline modality to deepen the remission duration. More recently, there have been prospective trials and retrospective studies assessing the efficacy of frontline, consolidative ASCT compared with chemotherapy alone in patients with DLBCL.
Despite many clinical trials, there is no consensus on when to recommend ASCT consolidation in patients with NHL. In this review, we summarize the published clinical trials guiding the use of ASCT as frontline, consolidative treatment in patients with various subtypes of NHL. We also recommend the optimal timing for ASCT referral for each of these subtypes to help guide the oncologist.
Risk stratification of B- and T-cell lymphoma prior to ASCT
Lymphomas are a pathologically and prognostically diverse group of malignancies. Risk stratification based on prognostic indices for each of the subtypes of NHL is an important tool that has been validated to predict outcome in patients with NHL. In patients with DLBCL, the international prognostic index (IPI) [age, performance status (PS), lactate dehydrogenase (LDH), extranodal sites and stage] is used to assign each patient a risk score [Anonymous 1993; Sehn et al. 2007]. This has little utility in patients with MCL, for whom the European MCL network developed the MCL international prognostic index (MIPI) as an MCL-specific risk stratification tool. The prognostic factors included in MIPI are age, PS, LDH, white blood count at diagnosis, and Ki67 proliferation index [Hoster et al. 2008]. For patients with FL, the FL international prognostic index (FLIPI) score is calculated based on the patient’s age, disease stage, LDH, number of nodal sites, and hemoglobin level [Solal-Celigny et al. 2004]. The role of upfront transplantation was evaluated in patients with only advanced stage, symptomatic disease. For peripheral T-cell lymphoma (PTCL), the prognostic index (PIT) is based on age, PS, LDH and bone marrow involvement [Gallamini et al. 2004]. These factors independently predict overall survival (OS) of patients with PTCL. Ironically, patients with a high-risk PIT score have not been shown to benefit from consolidative ASCT in clinical trials to this point, likely due to their overall poor prognosis. This is further discussed in the sections below.
Role of consolidative ASCT in DLBCL following induction chemotherapy
Since DLBCL is the most common subtype of NHL, there have been multiple large randomized controlled trials (RCTs) assessing the benefit of frontline, consolidative ASCT compared with chemotherapy alone in patients with DLBCL. These studies have been limited primarily by the fact that patients were not stratified based on prognostic score, and randomization occurred prior to induction therapy so that patients with progressive disease were not able to complete their intended consolidative ASCT. It should be noted that not stratifying by IPI has been partially validated by a post hoc subgroup analysis showing that in prospective settings the IPI is not predictive of prognosis in patients with aggressive NHL receiving consolidative ASCT [Stiff et al. 2013]. The histological subgroups were variable as patients with aggressive histologies other than DLBCL were included in these studies. Most of these studies were also conducted in the pre-rituximab era. Table 1 summarizes the trials comparing consolidative ASCT with traditional chemotherapy [Verdonck et al. 1995; Gianni et al. 1997; Haioun et al. 2000; Kluin-Nelemans et al. 2001; Gisselbrecht et al. 2002; Kaiser et al. 2002; Martelli et al. 2003; Milpied et al. 2004; Olivieri et al. 2005; Betticher et al. 2006; Linch et al. 2010; Stiff et al. 2013].
Randomized controlled trials comparing consolidative, frontline autologous hematopoietic stem-cell transplantation (ASCT) in patients with diffuse large B-cell lymphoma (DLBCL).

aaIPI, age-adjusted international prognostic index; BEAC, carmustine, etoposide, cytarabine, cyclophosphamide; BEAM, dexamethasone, carmustine, etoposide, cytarabine, melphalan; CHOEP, cyclophosphamide, adriamycin, etoposide, vincristine, prednisone; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisone; CR, complete response; EFS, event-free survival; IPI, international prognostic index; MACOP-B, methotrexate, adriamycin, cyclophosphamide, vincristine, prednisone, bleomycin; MTX, methotrexate; NS, nonsignificant; PR, partial response; R, rituximab; TBI, total body irradiation.
The most comprehensive and recent meta-analysis of the clinical trials data regarding frontline ASCT in patients with DLBCL was authored by Greb and colleagues and published in 2008 in the Cochrane Database of Systematic Reviews [Greb et al. 2008]. This meta-analysis drew data from 15 RCTs comparing OS and event-free survival (EFS) in patients with diffuse, aggressive NHL who received either frontline ASCT or chemotherapy alone. All the RCTs included in this meta-analysis were conducted in the pre-rituximab era, and the meta-analysis was updated most recently in June 2010, with no additional RCTs meeting inclusion criteria. This analysis concluded that there was not clear OS or EFS benefit to frontline ASCT compared with chemotherapy alone in patients with diffuse, aggressive NHL [Greb et al. 2008]. However, in patients with age-adjusted IPI (aaIPI) high-risk disease (scores 2–3) there was a nonsignificant trend toward OS and EFS benefit with frontline ASCT compared with chemotherapy alone [Greb et al. 2008].
Most of the studies included in the 2008 Cochrane meta-analysis were European multicenter RCTs, and the majority (10 of 14) of the trials were analyzed on an intention-to-treat basis. There was significant variability amongst the trials regarding the IPI scores of the patients, induction regimens before ASCT, control group chemotherapeutic regimens, and the proportion of patients randomized to ASCT who were able to receive ASCT. The IPI scores of patients in these RCTs ranged from a trial where patients with IPI high-risk disease were excluded [Milpied et al. 2004], to trials where only patients with IPI intermediate–high or high-risk disease were included [Haioun et al. 2000; Gisselbrecht et al. 2002; Martelli et al. 2003]. The variability in induction and control chemotherapeutic regimens is best summarized in Table 1. Finally, due primarily to rapid disease progression and patient dropout, the trials included in this meta-analysis exhibited significant variability in the proportion of patients who were randomized to ASCT and actually underwent ASCT (from a low of 60% of patients [Martelli et al. 2003] to 100% of patients [Gianni et al. 1997]).
For these aforementioned reasons, multiple sensitivity analyses were performed, and these analyses confirmed the conclusions regarding an overall lack of improvement in OS and EFS in patients with diffuse, aggressive NHL treated with frontline ASCT compared with chemotherapy alone. The trend toward improved OS and EFS in patients with IPI high-risk disease was noted when the 2002 trial by Gisselbrecht and colleagues was excluded from the meta-analysis [Gisselbrecht et al. 2002; Greb et al. 2008]. This trial was chosen for exclusion due to its exceptionally poor outcomes in patients with IPI high-risk disease receiving ASCT. These poor outcomes may be attributable to both the less intense induction regimen used in patients receiving ASCT compared with conventional chemotherapy [substituting epirubicin in lieu of doxorubicin in patients receiving ASCT versus dose-intensified ACVBP (doxorubicin, cyclophosphamide, vindesine, bleomycin and prednisone) in patients receiving conventional chemotherapy], and the inclusion of a large proportion of patients with very high-risk disease (T-cell lymphoma, bone marrow involvement, bulky disease and LDH elevation) whose ASCT was at high risk for contamination with malignant cells [Gisselbrecht et al. 2002].
The largest RCT comparing CHOP alone to frontline, consolidative ASCT was the UKLG LY02 trial, and it included 457 patients with DLBCL with aaIPI high-risk disease [Linch et al . 2010]. This trial showed a 5-year progression-free survival (PFS) of 44% for patients treated with ASCT compared with 38% in patients treated with CHOP alone (p = 0.89). The 5-year OS was 50% in both groups [Linch et al. 2010]. Most notably, only 56% of patients randomized to ASCT were able to receive their ASCT, and the data were analyzed in an intention-to-treat fashion [Linch et al. 2010]. In the conclusion of this study, the authors note that when patients with chemoresistant disease were excluded (only patients with complete remission after the first three cycles of CHOP were included), the 5-year PFS in the ASCT group was 63% compared with 42% in patients treated with CHOP alone [Linch et al. 2010].
The largest multicenter US trial was a phase III RCT comparing rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) or CHOP chemotherapy alone with frontline ASCT in patients with IPI intermediate–high or high-risk diffuse, aggressive NHL [Stiff et al. 2013]. In this study, 89% of patients had DLBCL, and the results showed improved PFS at 2 years (69% versus 55%, p = 0.005), but no improvement in 2-year OS in patients treated with frontline ASCT compared with R-CHOP alone (74% with ASCT versus 71%, p = 0.32). In a subset analysis, when only patients with IPI high-risk disease were analyzed, a statistically significant OS benefit at 2-year follow up was noted (82% versus 64%, p = 0.01) [Stiff et al. 2013]. Definite conclusions on the utility of ASCT in patients with high-risk DLBCL should not be derived from this subset analysis, but future studies are needed to validate this finding. Importantly, patients with no response to initial chemotherapy were excluded from this study, resulting in 93% of patients receiving their intended ASCT.
There are many factors that account for the negative results of the meta-analysis and UKLG LY02 trial, but when evaluating the largest trials included in this meta-analysis the suboptimal proportion of patients randomized to ASCT who received ASCT may be contributing. Specifically, the four largest RCTs included in the meta-analysis (accounting for 1141 patients or 46% of the patients analyzed in the OS analysis) achieved actual rates of ASCT of 65% [Kaiser et al. 2002], 68% [Olivieri et al. 2005], 74% [Haioun et al. 2000] and 74% [Gisselbrecht et al. 2002]. As previously mentioned, this was primarily due to patients with chemoresistant disease and patient refusal of ASCT.
To address the role of dose intensity in younger patients with intermediate–high and high-risk DLBCL, the German High Grade Lymphoma Study Group conducted a phase III trial comparing rituximab, cyclophosphamide, adriamycin, etoposide, vincristine, prednisone (R-CHOEP-14) with high-dose chemotherapy (R-Mega CHOEP) followed by repetitive ASCT. The 3-year EFS was 69.5% in the R-CHOEP-14 group and 61.4% in the R-Mega CHOEP group. Noticeably toxicities were significantly higher in the R-Mega CHOEP arm [Schmitz et al. 2012], suggesting dose intensity in younger patients adds toxicity without a major EFS benefit.
In summary, clinical trials investigating frontline, consolidative ASCT in the rituximab era in patients with intermediate or intermediate–high risk DLBCL do not appear to have better OS, though further ongoing investigations with alternative regimens may benefit younger patients.
ASCT consolidation in advanced FL
Given that FL is nearly as common as DLBCL in Western countries, there have been four large RCTs comparing outcomes in patients with advanced FL treated with frontline ASCT compared with chemotherapy alone. In 2012, a Cochrane review of these four RCTs showed no clear OS benefit to frontline ASCT, but noted a large PFS benefit to initial treatment with ASCT [Schaaf et al. 2012]. These four RCTs with 941 patients are summarized in Table 2 [Lenz et al. 2004; Sebban et al. 2006; Ladetto et al. 2008; Gyan et al. 2009].
Randomized controlled trials with consolidative, frontline autologous hematopoietic stem-cell transplantation (ASCT) in patients with follicular lymphoma.

CHOP, cyclophosphamide, doxorubicin, vincristine, prednisone; CR, complete response; Cy/TBI, cyclophosphamide/total body irradiation; DEXA-BEAM, dexamethasone, carmustine, etoposide, cytarabine, melphalan; EFS, event-free survival; FLIPI, follicular lymphoma international prognostic index; IPI, international prognostic index; NS, nonsignificant; PFS, progression-free survival; PR, partial response.
All the RCTs comparing consolidative, frontline ASCT with chemotherapy alone in patients with advanced FL were European, multicenter trials. Notably, over 80% of patients randomized to receive ASCT successfully completed ASCT, but there was heterogeneity in the induction chemotherapy regimens, control group chemotherapeutic regimens, and only one trial involved rituximab [Ladetto et al. 2008]. Also of note, the meta-analysis by Schaaf and colleagues in 2012 compared the rates of treatment-related mortality, secondary acute myeloid leukemia, secondary myelodysplastic syndrome, and secondary solid malignancies in patients receiving ASCT compared with chemotherapy alone, and there was no statistically significant difference [Schaaf et al. 2012]. However, it should be noted that there was a trend toward increased risk of secondary cancers in patients receiving high-dose induction therapy followed by ASCT compared with control patients in three of the RCTs [Lenz et al. 2004; Sebban et al. 2006; Gyan et al. 2009].
The largest RCT included in the aforementioned meta-analyses was conducted in France and Belgium and included 401 patients. This trial compared four cycles of CHOP followed by HDT (cyclophosphamide, mesna, etoposide, and split total body irradiation) and ASCT with six cycles of cyclophosphamide, doxorubicin, teniposide, prednisone, and interferon (CHVP-I). At 7-year follow up, OS was 76% in patients treated with ASCT compared with 71% in control patients (p = 0.53) [Sebban et al. 2006]. This was the only negative trial of the four RCTs with regards to EFS, as after 7 years the patients who had received an ASCT had an EFS of 38% compared with 28% among control patients (p = 0.11) [Sebban et al. 2006]. The three remaining RCTs with follow up ranging from 4 to 9 years showed at least a 25% absolute increase in PFS when comparing patients who had received ASCT with chemotherapy alone [Lenz et al. 2004; Ladetto et al. 2008; Gyan et al. 2009].
In summary, patients with advanced FL treated with frontline, consolidative ASCT have demonstrated improved PFS but not OS compared with patients with advanced FL treated with chemotherapy alone in clinical trials to date. The PFS benefit has also been established in the nontransplant rituximab maintenance or consolidative radioimmunotherapy studies, thus arguing against consolidative ASCT as an option in first complete remission in patients with advanced FL [Salles et al. 2011].
Consolidative ASCT in MCL
MCL comprises around 6% of all NHLs. Given the rarity of this disease, there have been very few RCTs comparing frontline, consolidative ASCT with maintenance therapy. The only RCT in patients with MCL was completed by Dreyling and colleagues and it consisted of consolidative ASCT compared with interferon α (IFNα) in young (under 65 years old) patients with advanced MCL who responded to induction CHOP. In this European multicenter trial involving 122 patients [Dreyling et al. 2005] at 3-year follow up, there was an improvement in PFS in patients who had received ASCT (54% versus 25%, p = 0.01) but no difference in OS (83% versus 77%, p = 0.18) [Dreyling et al. 2005]. Without an improvement in OS in the only RCT, and in light of encouraging results from a large, prospective trial of frontline treatment with only alternating rituximab and hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (R-HyperCVAD) and rituximab with high-dose methotrexate (HD MTX) and cytarabine without ASCT [Romaguera et al. 2010], there has been no consensus regarding the appropriate use of frontline, consolidative ASCT in young patients with MCL.
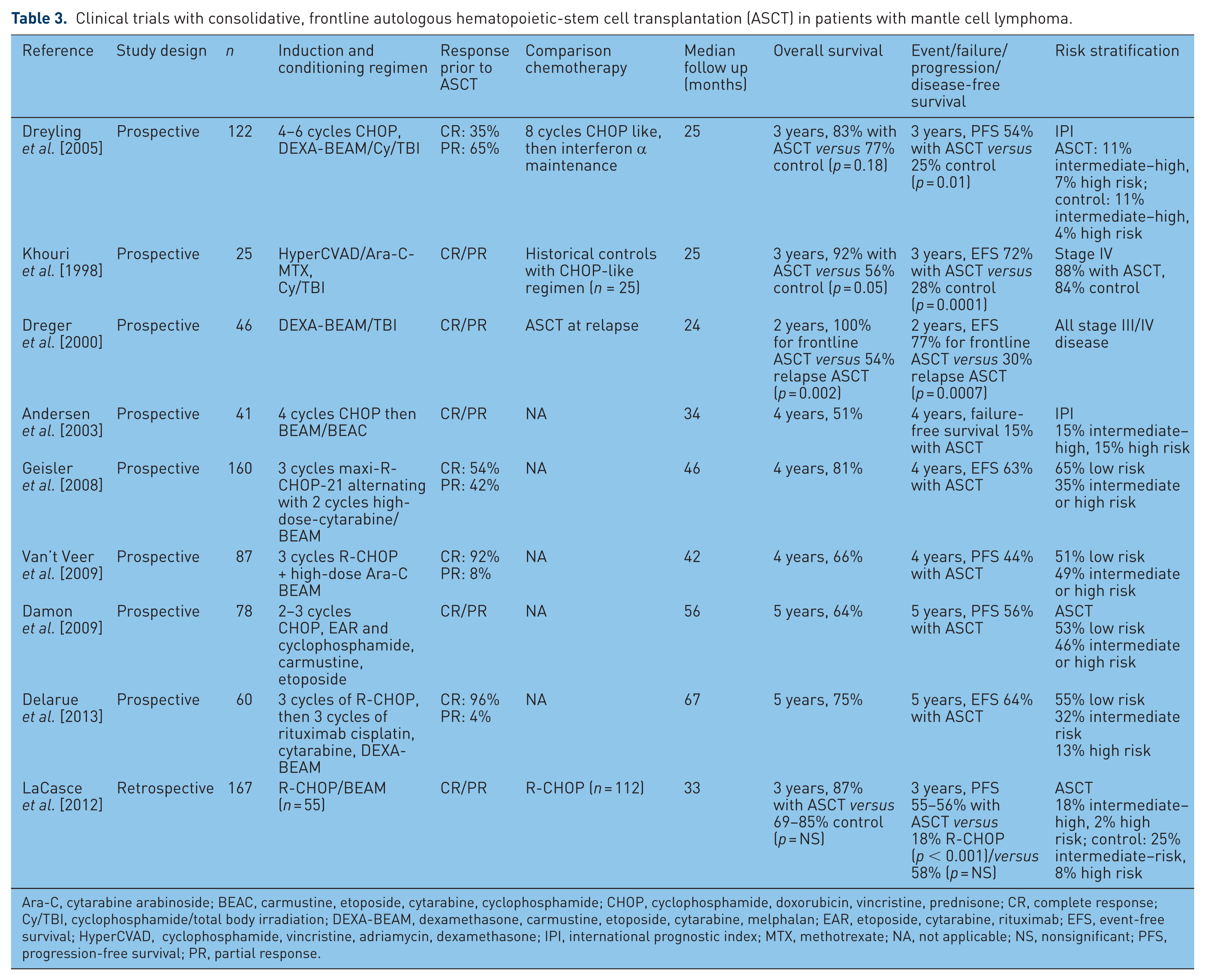
Adding to this RCT and critically analyzing the noncontrolled retrospective studies and prospective trials, there have been recent review articles which discuss frontline ASCT in young patients with MCL [Vose, 2013]. The authors discuss the multitude of prospective trials and retrospective studies specifically assessing ASCT as frontline, consolidative treatment in patients with MCL. Summary data from the eight largest prospective trials and one retrospective study involving 786 patients are included in Table 3 [Khouri et al. 1998; Dreger et al. 2000; Andersen et al. 2003; Gianni et al. 2003; Dreyling et al. 2005; Geisler et al. 2008; Damon et al. 2009; Van’t Veer et al. 2009; Ahmadi et al. 2012; LaCasce et al. 2012; Delarue et al. 2013].
Clinical trials with consolidative, frontline autologous hematopoietic-stem cell transplantation (ASCT) in patients with mantle cell lymphoma.
Ara-C, cytarabine arabinoside; BEAC, carmustine, etoposide, cytarabine, cyclophosphamide; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisone; CR, complete response; Cy/TBI, cyclophosphamide/total body irradiation; DEXA-BEAM, dexamethasone, carmustine, etoposide, cytarabine, melphalan; EAR, etoposide, cytarabine, rituximab; EFS, event-free survival; HyperCVAD, cyclophosphamide, vincristine, adriamycin, dexamethasone; IPI, international prognostic index; MTX, methotrexate; NA, not applicable; NS, nonsignificant; PFS, progression-free survival; PR, partial response.
The studies included in Table 3 are from multiple centers in both the United States and Europe. Induction regimens were highly variable, the studies rarely involved a direct comparison to patients treated with chemotherapy alone, and an exceptionally high rate of patients allocated to receive ASCT completed their transplant, in part because many of the trials were retrospective analyses.
Most notably amongst this dataset are the largest prospective trials and retrospective studies, each involving approximately 160 patients. Both were multicenter studies; the prospective trial was conducted in Europe [Geisler et al. 2008] and the retrospective study used US data [LaCasce et al. 2012]. In the retrospective US study, LaCasce and colleagues showed that even without ASCT, after 3 years R-HyperCVAD was more efficacious than R-CHOP in terms of PFS as frontline treatment for MCL (58% versus 18%, p < 0.001). The 3-year OS comparison between R-HyperCVAD and R-CHOP alone also showed a trend toward benefit for the R-HyperCVAD group (87% versus 69%, p = 0.07) [LaCasce et al. 2012]. Due to these differences between R-CHOP and R-HyperCVAD alone, the most notable comparison with ASCT is R-HyperCVAD without the R-CHOP group. This analysis showed that at 3 years there was no difference in OS (87% with ASCT versus 87% control) and PFS (55% with ASCT versus 58% control). Treatment complications requiring hospital admission were more significant in the R-HyperCVAD group compared with R-CHOP.
The prospective trial involved 160 patients from the Nordic Lymphoma Group, and it showed similar OS and EFS to the aforementioned retrospective study, without a comparison group. At 4 years, OS was 81% and EFS was 63% in patients treated with maxi-R-CHOP as induction before ASCT [Geisler et al. 2008].
Overall, the data for consolidative ASCT in patients with MCL should be interpreted with caution due to the lack of RCTs and the potential impact of hidden confounders. The studies that have been published have been somewhat variable but on multiple occasions have shown improvement in OS and PFS with frontline, consolidative ASCT compared with chemotherapy alone in patients with advanced MCL. Many centers advocate ASCT as frontline, consolidative therapy in young patients with MCL, but a large prospective trial by Romaguera and colleagues showing successful treatment with intensified chemotherapy alone has precluded a consensus regarding ASCT in patients with MCL [Romaguera et al. 2010].
Role of HDT and ASCT in primary central nervous system lymphoma at first response
Several phase II studies among immunocompetent patients with a variety of conditioning regimens have been published on the role of ASCT in patients with primary central nervous system lymphoma (PCNSL) after induction chemotherapy during first remission (Table 4) [Abrey et al. 2003; Colombat et al. 2006; Illerhaus et al. 2008; Yoon et al. 2011; Kiefer et al. 2012]. PCNSL is more common among those over the age of 65. This provides an increasing challenge to consider other modalities of therapy for patients who may not tolerate the combined modality therapy that includes HDT and ASCT. The original study by Colombat and colleagues reported the safety and efficacy of HD MTX based chemotherapy followed by HDT and ASCT in patients with newly diagnosed PCNSL. Twenty-five patients initially received two cycles of HD MTX, etoposide, carmustine and methylprednisolone, then one cycle of ifosfamide and cytarabine, followed by peripheral stem-cell collection. A total of 17 patients who exhibited a response to initial therapy then received HDT using carmustine, etoposide, cytarabine and melphalan, followed by ASCT. After ASCT, patients whose condition responded received whole-brain radiation therapy (WBRT) and those whose condition did not respond received salvage therapy followed by WBRT [30 Gray (Gy)]. Four of the 21 patients whose condition responded did not reach ASCT because of toxicity or refusal. With a median follow up of 34 months, the estimated 4-year EFS was 46% and OS was 64%. No evidence of late treatment-related toxicity was observed. This is an interesting observation as almost all patients received WBRT at a dose of 30 Gy [Colombat et al. 2006].
Clinical trials with consolidative, frontline autologous hematopoietic stem-cell transplantation (ASCT) in patients with primary central nervous system lymphoma.

Ara-C, cytarabine arabinoside; CR, complete response; Cy, cyclophosphamide; MBVP, methotrexate, carmustine, etoposide, methylprednisolone; MTX, methotrexate; NR, not reached; OS, overall survival.
In a similar study, Abrey and colleagues completed a phase II trial using HD MTX and cytarabine followed by HDT and ASCT in patients with newly diagnosed PCNSL. A total of 28 patients received induction chemotherapy, and then 14 patients with chemosensitive disease underwent HDT (carmustine, etoposide, cytarabine and melphalan) followed by ASCT. The median EFS was 5.6 months for all patients and 9.3 months for the 14 patients who underwent transplantation. Six of these 14 patients (43%) remained disease free at last follow up (median follow up of 28 months). Prospective neuropsychological evaluations revealed no evidence of treatment-related neurotoxicity. This study suggests that ASCT as frontline consolidation therapy is feasible in patients with newly diagnosed PCNSL, without evidence of significant long-term neurotoxicity [Abrey et al. 2003]. Dose intense consolidative regimens with etoposide and cytarabine (EA) following initial induction with methotrexate, temozolomide and rituximab (MTR) was evaluated in a small yet promising phase II study. The 4-year OS probability of survival was 65% in this radiation-sparing trial [Rubenstein et al. 2013].
While it should be noted that patients enrolled in phase II trials are subject to selection bias, early results of upfront HDT and ASCT are still encouraging. Despite the encouraging results of the phase II study of MTR EA, we eagerly await the results of the randomized trial of PCNSL that does not involve brain radiation or HDT/ASCT. Treatment modalities to sustain response without long-term neurocognitive effects are needed. Thiotepa has better brain penetration and carries theoretical advantages over other conditioning regimens based on its effective local blood–brain tissue penetration and needs to be considered in selected patients. It also carries excess toxicities in combination with busulfan-containing conditioning regimens [Reddy and Savani, 2012]. One promising approach to minimize long-term neurocognitive side effects and decrease relapse rates would be to consider lower radiation doses after ASCT. In the aforementioned studies, though there is no increased neurotoxicity reported with induction regimens, systemic toxicity of consolidative ASCT must be considered.
Consolidative ASCT for patients with PTCL following induction
Given the relative rarity of PTCL, the current data to guide decision-making regarding ASCT as frontline therapy are limited to prospective trials and retrospective studies. There are several studies that showed improved OS and PFS when patients with PTCL received frontline, consolidative ASCT compared with chemotherapy alone. Notable exceptions were patients with anaplastic lymphoma kinase (ALK) mutated anaplastic large cell lymphoma (ALCL), as these patients have favorable outcomes with anthracycline-containing chemotherapy alone, and patients with IPI high-risk or high-risk PIT scores at presentation, as these patients as a whole have not yet shown significant benefit from frontline, consolidative ASCT, albeit in subgroup analyses [Laport, 2010]. In Table 5, six of these trials involving 452 patients are summarized [Corradini et al. 2006; Feyler et al. 2007; Rodriguez et al. 2007a, 2007b; Mercadal et al. 2008; Reimer et al. 2009; Numata et al. 2010].
Prospective and retrospective trials as consolidative, frontline autologous hematopoietic stem-cell transplantation (ASCT) in patients with peripheral T cell lymphoma.

Ara-C, cytarabine arabinoside; BEAC, carmustine, etoposide, cytarabine, cyclophosphamide; BEAM, dexamethasone, carmustine, etoposide, cytarabine, melphalan; CHOEP, cyclophosphamide, adriamycin, etoposide, vincristine, prednisone; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisone; CR, complete response; Cy/TBI, cyclophosphamide/total body irradiation; EFS, event-free survival; ESHAP, etoposide, Solu Medrol, cytarabine, cisplatin; IPI, international prognostic index; PFS, progression-free survival; PIT, prognostic index in peripheral T-cell lymphoma; PR, partial response.
Similar to the RCTs involving patients with DLBCL and FL, induction regimens were highly variable, and all the prospective trials were analyzed on an intention-to-treat basis. As noted by Laport, the prospective trials generally reported worse outcomes than the retrospective studies, based on intention-to-treat methodology and the inclusion of patients in the ASCT group who were not able to reach transplant (the proportion who were able to receive ASCT ranged from 41% to 74% in prospective trials) [Laport, 2010].
The largest study assessing frontline, consolidative ASCT in patients with PTCL included 166 patients. Patients who were treated with six cycles of CHOEP followed by carmustine, etoposide, cytarabine and melphalan (BEAM) with ASCT were compared with historical control patients treated with CHOP or HyperCVAD. At 5 years, this RCT showed an OS of 50% and PFS of 43%, with historical control patients consistently achieving less than 30% 5-year survival and PFS [D’Amore et al. 2012].
Despite the lack of RCTs addressing the utility of frontline, consolidative ASCT in patients with PTCL, the prospective and retrospective trials consistently show an OS and PFS benefit to frontline, consolidative ASCT compared with chemotherapy alone in patients with PTCL, except in the aforementioned ALK-positive ALCL. Patients with high-risk IPI or PIT PTCL should be considered for ASCT based on their individual clinical situation, as the clinical trials data in this population have been suboptimally designed to draw definitive conclusions about the utility of ASCT in this population.
Current implications and future perspectives of consolidative ASCT in lymphoma
The efficacy of frontline, consolidative ASCT compared with chemotherapy alone in the treatment of NHL depends on multiple factors, including tumor histology, prognostic score, disease stage, and in some cases the presence or absence of molecular markers. The clinical trials data detailing outcomes of frontline, consolidative ASCT are summarized within the major histological subtypes of NHL.
While the data regarding frontline, consolidative ASCT in patients with DLBCL are the most readily available, they are also the most heterogeneous. What has been concluded at the current time is that patients with intermediate–high and high-risk IPI disease likely have improved PFS when treated with ASCT and in a subgroup analysis has been shown to improve OS in patients with high-risk IPI. Therefore, until we have data on novel induction regimens in the R-CHOP era, and in the absence of clinical trials, the best survival benefit may be achieved with ASCT consolidation following induction therapy for patients with high-risk IPI DLBCL.
In patients with advanced FL, it has been consistently shown in RCTs that frontline, consolidative ASCT improves PFS but not OS. Given that maintenance antibody therapy or radioimmunotherapy following initial induction impacts PFS, similar benefits may be derived with maintenance strategies. In patients with MCL, frontline, consolidative ASCT has shown improved OS and PFS compared with chemotherapy alone in multiple studies. We note that RCT data are lacking, and for this reason we conclude that ASCT is a reasonable consideration in young (under 65 years old) patients with newly diagnosed MCL [Geisler, 2012].
The international extranodal lymphoma study group is conducting a randomized phase II study comparing consolidative radiation therapy with HDT in patients with PCNSL. Until the results of this trial are available, we propose considering early HDT and ASCT after multiagent induction chemotherapy in patients who can tolerate HDT.
Based on non-RCT data, a subset of patients with PTCL appear to exhibit an OS and PFS benefit when treated with frontline, consolidative ASCT instead of chemotherapy alone. These are patients with intermediate-risk disease, excluding those with ALK-positive ALCL [Laport, 2010]. We would note that there are no sufficiently well designed clinical trial data to rule out the use of ASCT in patients with high-risk PTCL.
Across all types of B-cell NHLs, RCTs involving rituximab-containing chemotherapy regimens are scarce, and there is a primary need in future determinations of the appropriate use of frontline, consolidative ASCT to incorporate rituximab. Also, conducting clinical trials with specific subsets of patients who are most likely to benefit from frontline ASCT is a large area of need in future research (for example, only high-risk IPI for patients with DLBCL or low-risk PIT for patients with PTCL). Given the continuously improving chemotherapeutic and molecular-based therapies in development, identifying patients with NHL that will benefit most from frontline ASCT is a constant challenge. Clinical trials that involve novel agents in the induction regimen should therefore be powered to include the survival benefit achieved from consolidative ASCT.
It is certain that as agents that target pathways such as phosphoinositide-3 kinase, B-cell receptor, histone deacetylase or immunomodulators gain US Food and Drug Administration approval for various NHL histologies, the role and timing of ASCT becomes even more complex. Incorporating these agents as a maintenance strategy following auto transplants is certainly an attractive strategy. We believe that future clinical trials should aim to consider these novel agents in the peri- and post-transplant period.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that they have no conflict of interest.