
Abstract
Background:
Diffuse large B-cell lymphoma (DLBCL) is the most frequent non-Hodgkin lymphoma worldwide. The current standard of care is chemoimmunotherapy with an R-CHOP regimen. We aim to review the role of this regimen after two decades of being the standard of care.
Methods:
A comprehensive literature review of DLBCL, including the epidemiology, trials defining R-CHOP as the standard of care, as well as dose intensification and dose reduction schemes. Additionally, we briefly review the development of rituximab biosimilars and the addition of targeted drugs to R-CHOP in clinical trials.
Discussion:
R-CHOP cures approximately 70% of DLBCL patients. Dose-dense regimens do not show a benefit in response and increase toxicity. Dose reduction, particularly in elderly patients or with comorbidities, may be a treatment option. DLBCL constitutes a group of diseases that activate different biological pathways. Matching specific treatments to a defined genetic alteration is under development. Rituximab biosimilars have become available to a broader population, particularly in developing countries, where access to treatment is limited because of economic resources.
Conclusion:
DLBCL landscape is heterogeneous. R-CHOP immunochemotherapy has been a standard of care for two decades and cures approximately 70% of cases. Molecular characterization of patients is evolving and may have critical therapeutic implications.
Keywords
Diffuse large B-cell lymphoma
Non-Hodgkin lymphoma (NHL) is the seventh most common cancer in the United States. 1 The incidence rate in Europe is 3.8/100,000 per year. 2 In 2018, there were approximately 509,590 new cases and 248,724 deaths worldwide 3 ; diffuse large B-cell lymphoma (DLBCL) roughly accounts for 24% of all new cases of NHL each year.3,4
DLBCL is a defined entity within the 2016 World Health Organization (WHO) classification 5 and constitutes the most common of all aggressive types of B-cell lymphomas. Patients typically present with rapidly enlarging lymphadenopathy and constitutional symptoms which require immediate treatment. Moreover, 40% of patients have extranodal disease 6 ; in 8–9% of such cases, the extranodal site will be the primary site of presentation. 7 Different clinical scores have classified these patients into prognostic groups, with effects on response rates and survival. For instance, the International Prognostic Index (IPI) 8 includes five groups depending on age (>60 years), clinical stage, LDH levels, number of extranodal sites, and ECOG performance status. According to this score, high-risk patients had a 5-year overall survival (OS) of 32%, compared with 83% in low-risk patients. After adding rituximab as part of the standard treatment, Sehn et al. 9 reevaluated this score [revised-IPI (R-IPI)] and described only three prognostic groups: very good, good, and poor, with 4-year OS rates of 94%, 79%, and 55%, respectively. The National Comprehensive Cancer Network (NCCN)-IPI 10 identifies four groups: low, low-intermediate, high-intermediate, and high-risk, whose 5-year OS rates are, respectively, 96%, 82%, 64%, and 33%. These scores are summarized in Table 1. Ruppert et al. 11 recently compared these prognostic indices in more than 2000 DLBCL patients from seven multicenter clinical trials. Both the NCCN-IPI and R-IPI scores distinguish a subgroup with favorable long-term survival. Ruppert et al. concluded that the NCCN-IPI best discriminated between patients with poor and favorable OS. This index had the most remarkable absolute difference in OS.
Comparison of International Prognosis Indices in diffuse large B-cell lymphoma.

Serum lactate dehydrogenase upper limit of normal.
BM, bone marrow; CNS, central nervous system; ECOG, Eastern Cooperative Oncology Group performance status; GI, gastrointestinal; IPI, International Prognostic Index; LDH, lactate dehydrogenase; NCCN, National Comprehensive Cancer Network; R-IPI, revised IPI; ULN, upper limit of normal.
Although the NCCN-IPI prognostic index is widely recommended since it discriminates between low- and high-risk DLBCL patients better than IPI or R-IPI, most clinical trials studying DLBCL treatment have been conducted using the IPI or R-IPI scores, which are currently used.
Classification
DLBCL is morphologically, genetically, and clinically heterogeneous. It was subclassified in 2000 according to gene expression profiling (GEP) into two molecular subtypes. Patients with germinal center B-cell-like (GCB) DLBCL had better 5-year progression-free survival (PFS) rates than those with activated B-cell-like (ABC) DLBCL (76% versus 31%). 12 ABC DLBCL arises from B-cells that undergo germinal center reaction and increased genetic alterations of NF-κB modifiers and B-cell receptor signaling pathway elements, as well as disruption of terminal differentiation. In contrast, GCB DLBCL originates from the light zone of germinal centers and may have altered chromatin-modifying enzymes, disturbances in PI3K signaling, and BCL2 structural variants. 13 Since GEP is not available for routine diagnosis, researchers use immunohistochemistry to classify molecular subtypes into two main groups: germinal center and non-germinal center, according to Hans et al., 14 Choi et al. 15 or Tally et al. 16 nomograms. Gutierrez-Garcia et al. 17 compared these immunohistochemistry nomograms with GEP. They concluded that the proportion of misclassified cases in the GCB subset was as high as 41%, 48%, 30%, 60%, and 40% for Colomo, Hans, Muris, Choi, and Tally nomograms, respectively.
Therefore, the impact of these nomograms on survival is controversial,4,18,19 and outcomes may differ from what is expected of these nomograms, especially if other genes or proteins are analyzed.
The overexpression of MYC (>40%)/BCL2 (>50%) proteins in the absence of cytogenetic abnormalities is known as double-protein-expression lymphoma. Some authors have associated this lymphoma with poorer PFS and OS.20 –22 Johnson et al. 18 reported that MYC overexpression was associated with poorer OS only when BCL2 proteins were coexpressed (p < 0.001). Patients with key chromosomal rearrangements of MYC and BCL2 [double-hit lymphoma (DHL)] have shown poor response to standard treatments.23 –25 DHLs and triple-hit lymphomas are referred to as high-grade B-cell lymphoma with MYC, BCL2 and/or BCL6 rearrangements in the 2016 WHO classification. 5
The analysis of all MYC/BCL2/BLC6 rearrangements is not routinely performed. Actually the NCCN guidelines consider it essential to perform FISH to search for MYC rearrangements, as part on the initial work-up, in all cases of DLBCL. If MYC rearrangement is present, fluorescence in situ hybridisation (FISH) of BCL2 and BCL6 should also be performed, to rule out double or triple hit lymphoma. 19
Researchers at the British Columbia Cancer Agency 26 recently used next-generation sequencing and high-resolution SNP arrays, and they identified 62 single nucleotide variants (SNVs) in MYC and 190 SNVs in BCL2. They identified hotspot mutations with MYC (P72 and I 159) and BCL2 (A4, R6, K17, G47, H58, P59, A60, E124, A131, G197, and A198) in GCB DLBCL. All G-to-C transition mutations in MYC and BCL2 targeted WRCY motifs, which highly suggests that they are a consequence of somatic hypermutation. The presence of MYC TR or BCL2 GA was associated with shorter time to progression in ABC DLBCL. Likewise, MYC GA, MYC TR, BCL2 GA, and BCL2 TR were associated with an adverse outcome in GC DLBCL.
Moreover, a gene expression-based classifier has been used to define a molecular high-grade (MHG) group. 27 PFS at 36 months in the MHG group was 37%, whereas it was 72% in the other groups. Additionally, the lack of MHG signatures identified double-hit lymphomas without evidence of worse outcomes than other GCB DLBCL cases. MHG identified genes associated with a highly proliferative phenotype and shared features with centroblasts of the dark zone of the germinal center, in contrast to the centrocyte or light zones of other GCB lymphomas.
Validating these molecular signatures is a controversial focus of research in DLBCL. The Nebraska University currently has a program to refine and validate the prognostic profile of molecular signatures to improve diagnosis and outcome prediction in lymphoma patients. 27 All these findings have not yet been included in clinical scores defining the universal treatment of such patients.
R-CHOP as standard of care
CHOP regimen was the standard of care in the 1990s. 28 Other intensive chemotherapy regimens, such as m-BACOD, ProMACE-CytaBOM, or MACOP-B, increased toxicity without showing any benefit in response or survival rates.
Rituximab is a chimeric type 1 monoclonal antibody (MoAb) against CD20, present on the surface of B lymphocytes. Its mechanism of action includes complement-dependent cytotoxicity, antibody-dependent cellular cytotoxicity, and direct induction of apoptosis.29 –31 Combining rituximab and chemotherapy regimens improved the prognosis of B-cell lymphomas.
Rituximab was initially approved by the US Food and Drug Administration in 1997 and later in 1998 by the European Medicines Agency. 32 Chemoimmunotherapy is now the most common upfront treatment for DLBCL, including rituximab + CHOP, known as R-CHOP: intravenous (IV) rituximab, 375 mg/m2 on day 1; IV cyclophosphamide, 750 mg/m2 on day 1; IV doxorubicin, 50 mg/m2 on day 1; IV vincristine, 1.4 mg/m2, dose cap of 2 mg on day 1; and oral prednisone, 100 mg daily on days 1–5. 16
The clinical benefit of adding rituximab to chemotherapy in DLBCL was demonstrated in several clinical trials (Table 2). In 2002, the Groupe d’Etude des Lymphomes de l’Adulte (GELA) revealed in a comparative phase III trial a significantly higher complete response rate (76% versus 63%, p = 0.005) and longer event-free survival (EFS) (not reached versus 13 months, p < 0.001) and OS (p = 0.007) in elderly patients (aged 60–80 years) treated with R-CHOP versus patients receiving CHOP. 33 A longer follow-up confirmed these results. 34
Trials comparing CHOP versus R-CHOP.

R = rituximab (375 mg/m2). ++CHOP = cyclophosphamide, 750 mg/m2; doxorubicin, 50 mg/m2; vincristine, 1.4 mg/m2, with capping at 2 mg; and oral prednisone, 100 mg daily on days 1–5. +++CHOP like = CHOP ± etoposide.
DLBCL, diffuse large B-cell lymphoma; IPI, International Prognostic Index; OS, overall survival; PFS, progression-free survival.
The RICOVER-60 trial 35 compared six versus eight cycles of CHOP-14 (every two weeks) ± rituximab in 1222 randomized patients. This trial confirmed the benefit of adding rituximab to CHOP chemotherapy in elderly people: PFS increased from 47.56% to 66.5% when rituximab was added to six cycles of CHOP-14 (Table 2).
After demonstrating the benefit of R-CHOP in patients older than 60 years, the MabThera International Trial 36 included patients aged 18–60 in a comparative (R-CHOP-like versus CHOP-like alone) phase III trial. Longer 3-year EFS (79% versus 59%; p < 0.001) and higher OS rates (93% versus 84%; p = 0.001) were reported in patients treated with chemoimmunotherapy. Some patients who received etoposide + CHOP had better 3-year survival than CHOP alone, but this difference was nullified when rituximab was added. These trials placed rituximab, mainly combined with CHOP, as the standard first-line treatment in DLBCL patients.
According to the NCCN guidelines, 19 patients with early and bulky disease, and those with advanced disease, shall receive six cycles of R-CHOP ± radiotherapy. However, low-risk patients (stage I–II) could receive four cycles of R-CHOP + two additional doses of rituximab.19,37 As a whole, R-CHOP cures 70% of patients,2,38 –40 but patients with localized disease have an OS of up to 92%. 19
R-CHOP intensification
After demonstrating the benefits of R-CHOP chemotherapy, three trials evaluated whether increasing the dose density could further improve the response rate by comparing R-CHOP-14 (every two weeks) versus R-CHOP-21. The first trial was a randomized phase III trial 41 that included 1080 adult patients. Lower relapse-free survival was documented in the R-CHOP-14 group, but the 3-year OS was 78% versus 67% in R-CHOP-21 versus R-CHOP-14, respectively. The German Tumor Registry Lymphatic Neoplasms also demonstrated that dose-dense two-weekly R-CHOP-14 was not superior to the three-weekly R-CHOP-21 in German routine practice. 36 The LNH03-6B study 42 showed that dose-dense R-CHOP did not improve the efficacy in patients aged 60–80 years (3-year EFS was 56% versus 60% in R-CHOP 14 versus R-CHOP 21, respectively); the frequency of toxicity was similar among regimens. Based on these results, the intensification of R-CHOP-14 is not currently recommended.
Changes in dose administration, including infusion therapy in selected risk groups, have also been proposed. Two phase III trials focused on this question. The first one was the LNH-03-2B trial, which compared R-ACVBP versus R-CHOP in low-intermediate risk patients aged 18–59 years. It found similar response rates in both treatments, but the 3-year PFS (87% versus 73%) and OS (92% versus 84% in R-ACVBP versus R-CHOP, respectively) was better in patients treated with rituximab, doxorrubicine, vincristine, bleomicine, prednisone (R-ACVBP). 43 Despite these promising results, only a DLBCL subgroup was included; therefore, it cannot be extrapolated to all DLBCL subgroups and used in routine practice. The Intergroup Trial Alliance/CALGB 50303 compared six cycles of dose-adjusted (DA)-EPOCH-R with R-CHOP, 44 without showing any additional benefits in the 2-year PFS (78.9% versus 75%) and 2-year OS (86.5% versus 85.7%) in DA-EPOCH-R and R-CHOP, respectively.
Moreover, other strategies, such as intensification with autologous stem-cell transplantation, have been proposed to improve the response rates in high-risk patients. Cortelazzo et al. 45 compared eight cycles of dose-dense R-CHOP with R-CHOP followed by autologous stem-cell transplantation. They concluded that both treatments were equally effective in terms of overall response rate (83% versus 84%), PFS (65% versus 75%, p = 0.12), and OS (74% versus 77%, p = 0.64, in R-CHOP versus sequential therapy, respectively). Likewise, two prospective comparative trials developed by the SWOG, Eastern Cooperative Oncology Group, Leukemia Group B, Canadian NCIC Clinical Trials Group, 46 and German Tumor Registry Lymphatic Neoplasms 47 could not validate a benefit of consolidative transplantation as first-line treatment regarding OS in intermediate-high or high-risk patients.
Finally, positron emission tomography-computed tomography (PET-CT) as a tool to guide therapy in early non-responder patients was evaluated in the PETAL phase III trial. 48 PET-CT was performed after two R-CHOP cycles, and PET-positive patients were randomized to continue six additional cycles of R-CHOP (standard therapy) or six blocks with an intensive Burkitt lymphoma protocol. Response rates, EFS (52.4% versus 28.3%) and OS (64.8% versus 47.1%, in R-CHOP versus Burkitt protocol, respectively) did not improve in patients receiving a more intensive treatment.
According to these trials, high-dose therapy is not recommended as first-line treatment in DLBCL. Table 3 summarizes the results of the different modalities of treatment intensification.
Modalities of treatment intensification in DLBCL.*
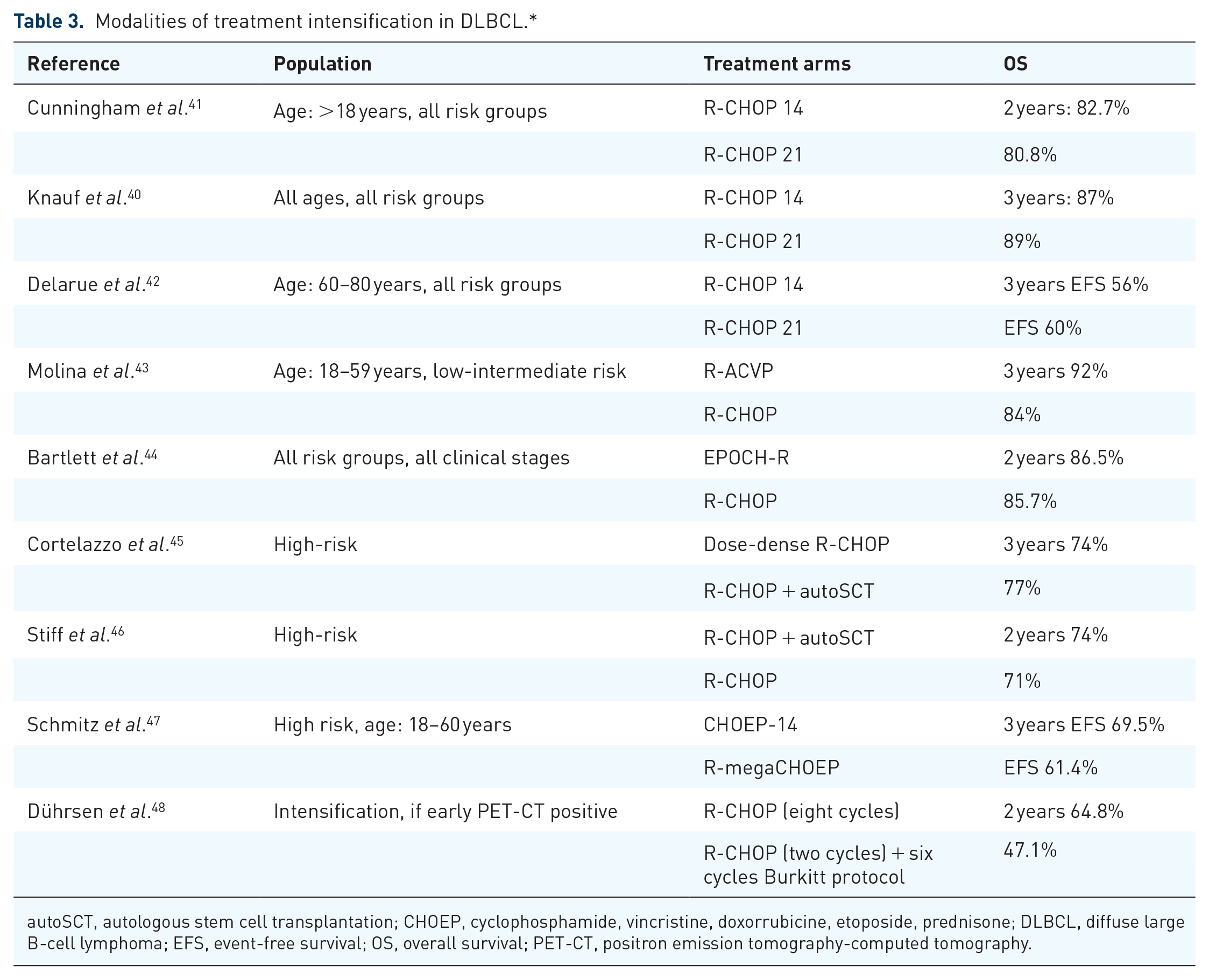
autoSCT, autologous stem cell transplantation; CHOEP, cyclophosphamide, vincristine, doxorrubicine, etoposide, prednisone; DLBCL, diffuse large B-cell lymphoma; EFS, event-free survival; OS, overall survival; PET-CT, positron emission tomography-computed tomography.
Low-intensity R-CHOP-like or R-CHOP-like in elderly patients
The GELA study demonstrated the safety and efficacy of R-CHOP in patients aged 60–80 years. Regardless of their biological age, patients may have comorbidities or altered organ function, which could increase the toxicity of the standard dose.49,50 Different attenuated immunochemotherapy regimens have been proposed to avoid excessive toxicity. These regimens include anthracycline-free therapy, 51 reducing the anthracycline dose,52 –55 substituting with pegylated doxorubicin, 56 reducing both anthracycline and cyclophosphamide doses,57,58 or splitting doxorubicin and cyclophosphamide into two days of administration. 45 The findings, shown in Table 4, indicate variability in response rates and OS. Some regimens showed low response rates and OS, while others showed no significant differences when compared with historical R-CHOP results. These regimens were included in either retrospective or single-arm prospective studies, which included populations with a wide range of ages and functional differences; therefore, the optimal regimen cannot be determined.
Tailored regimens guided by the Comprehensive Global Assessment (CGA) classified patients as fit, unfit, and frail 59 correlate with treatment outcomes regarding response rate, survival, and toxicity.19,60 Thus, elderly patients could be treated in prospective protocols to further validate the use of CGA as an aid in choosing the regimen that best matches the patient’s condition. This assessment will also be used in protocols testing targeted agents.
R-CHOP-like regimens proposed for elderly population.

R-CHOP = rituximab 375 mg/m2; cyclophosphamide, 750 mg/m2; doxorubicin, 50 mg/m2; vincristine, 1.4 mg/m2, with capping at 2 mg; and oral prednisone, 100 mg daily on days 1–5. ++R-CVP = rituximab 375 mg/m2; cyclophosphamide, 750 mg/m2; vincristine, 1.4 mg/m2, with capping at 2 mg; and oral prednisone, 100 mg daily on days 1–5. ++++R-miniCHOP, rituximab 375 mg/m2; cyclophosphamide, 500 mg/m2; doxorubicin, 25 mg/m2; vincristine, 1 mg/m2, with capping at 2 mg; and oral prednisone, 100 mg daily on days 1–5.
+R-ChOP, 50% reduction of anthracycline, rest of the drugs with the conventional dose.
AD, attenuated dose; CD, conventional dose; LD, liposomal doxorubicin; ORR, overall response rate; OS, overall survival; R-CEOP, rituximab 375 mg/m2; cyclophosphamide, 750 mg/m2; etoposide, 100 mg/m2, day, days 1-3; vincristine, 1.4 mg/m2, with capping at 2 mg; and oral prednisone, 100 mg daily on days 1–5.
Rituximab biosimilars
A biosimilar product is highly similar to a biological drug and has no clinically meaningful differences; however, there could be minor differences in inactive ingredients. According to the National Cancer Institute, a biosimilar must be “as safe as, work as well as, and work in the same way as” the original drug, and “be used in the same way, at the same dose, and for the same condition”. 61 The approval requirements vary according to regulatory agencies,62 –68 and the specific development process is not the objective of this review.
Eight biosimilars of rituximab have been approved by a regulatory health authority with preclinical and clinical information.69 –82 From all these biosimilars, only four were approved after conducting a comparative trial in DLBCL patients.
RTXM83 was evaluated in a multicenter, international, randomized, double-blind study, including 272 patients with low-risk DLBCL, based on the IPI score. The overall response was 83.6% for RTXM83 and 82.9% for rituximab, which fulfilled the predefined non-inferiority margin. 71 Safety and immunogenicity profiles were not significantly different between groups.
DRL-rituximab was compared with the reference MoAb in a prospective, double-blind trial which included 151 patients with advanced DLBCL from 44 centers in India. The results revealed equivalent pharmaockinetics (PK) parameters after cycle 1 and equivalent primary steady-state parameters area under curve (AUC)0–21 days and Cmax after cycle 6. Despite the secondary parameters at steady-state AUC0–24 weeks, confidence limits extended beyond the acceptable range. The efficacy (defined by a non-inferiority response rate), safety, and immunogenicity profiles were similar. 75
HLX01 was assessed in a phase III, multicenter, randomized, double-blind trial, including 406 patients; it showed a non-inferiority response rate (HLX01-CHOP: 94.1% versus R-CHOP 92.8%). Additionally, the safety and immunogenicity profiles were similar to the reference rituximab. 77
Reditux was introduced in India in 2007. A single-arm study including a small number of DLBCL patients reported a similar response, as well as pharmacokinetics/pharmacodynamics (PK/PD) profiles, compared with the published data for reference rituximab. 81
The remaining biosimilars were tested in other B-cell lymphomas. Around 20 more rituximab biosimilars are in development. 82
Beyond R-CHOP
R-CHOP remains the standard of care for DLBCL patients. However, almost one-third of patients relapse and have a poor prognosis; new strategies have thus been adopted to identify patients requiring another therapy. Many clinical trials have been conducted to improve results, such as adding maintenance therapies in low-grade lymphomas, 83 or targeted therapies. 84
Maintenance therapy
In contrast with low-grade B-cell lymphomas, the role of adding rituximab after achieving a response did not show an increase in EFS or OS in DLBCL.85 –89 Furthermore, a meta-analysis 90 indicated that maintenance rituximab significantly increased the incidence of neutropenia and the risk of infection, compared with observation group.
A multicenter, phase III, randomized trial 91 failed to demonstrate that using enzastaurin as maintenance therapy after R-CHOP as first-line treatment improved 4-year disease free survival (DFS) (70% versus 71%, enzastaurin versus placebo maintenance, respectively).
Lenalidomide has also been evaluated as maintenance treatment. A phase II randomized trial 92 comparing lenalidomide versus lenalidomide + rituximab after R-CHOP as first-line treatment did not show a benefit in high-risk patients in terms of 2-year DFS (86% versus 86) or OS (86% versus 95% for lenalidomide versus lenalidomide + rituximab maintenance, respectively). The phase III REMARC trial 93 assessed lenalidomide in high/high-intermediate risk patients aged 60–80 years as maintenance therapy for two years, or until toxicity or progressive disease. Median PFS was not reached in the lenalidomide group versus 58.9 months in the placebo group. However, OS was similar in both arms, with a median follow-up of 52 months. Although these results did not increase OS, they suggest a benefit of this immunomodulator drug after achieving complete response in older DLBCL patients (>60 years). Hence, these results require validation before being considered as a standard treatment.
Maintenance therapies using rituximab or enzastaurin are not currently indicated. After achieving an optimal response with R-CHOP, lenalidomide seems to be useful in high/high-risk older patients (>60 years), but these results require confirmation.
Attempts to enhance R-CHOP efficacy
Understanding the biology and cell-of-origin of DLBCL has changed first-line treatment approaches. After finding that ABC DLBCL has a poorer prognosis 17 and that the NF-κB pathway was active, the rationale of adding a proteasome inhibitor, bortezomib, to R-CHOP (BR-CHOP) was evaluated. The initial results of a comparative (R-CHOP versus BR-CHOP) phase II trial 94 suggested that adding bortezomib increased the 2-year PFS (77.6% for R-CHOP versus 82% for BR-CHOP). However, the phase III trial 95 in which patients were stratified using GEP and received R-CHOP ± bortezomib showed no benefits in PFS (70.1% versus 74.3% for R-CHOP and RB-CHOP, respectively). According to these results, adding bortezomib is not recommended.
Similarly, lenalidomide was evaluated to improve the response in previously untreated ABC DLBCL. A prospective, phase III, randomized trial compared lenalidomide-R-CHOP (R 2 -CHOP) versus placebo-R-CHOP. 96 The primary endpoint of PFS was not met, and the 2-year OS was similar in both groups (79% for R 2 -CHOP, 80% for placebo-R-CHOP). Thus, adding lenalidomide did not show any benefit.
Finally, another attempt to improve results in ABC DLBCL was to suppress BCR signaling with ibrutinib, an inhibitor of Bruton’s tyrosine kinase. A double-blind comparative trial 97 did not show that ibrutinib + R-CHOP improved EFS. However, a small benefit was observed in patients younger than 60 years in terms of EFS [hazard ratio (HR) 0.57], PFS (HR 0.55), and OS (HR 0.33). On the contrary, in patients older than 60 years ibrutinib-R-CHOP increased serious adverse events (63.4% versus 38.2%) and worsened EFS, PFS, and OS. The benefit observed in patients younger than 60 years requires confirmation in a prospective trial.
Although these drugs have shown a benefit in a subgroup of patients, they are not approved in the frontline of DLBLC treatment by any regulatory agency and are not recommended.
Matching treatment to genetic alterations
Researchers from the National Institutes of Health recently performed exome and transcriptome sequencing, targeted amplicon resequencing, and array-based DNA copy number analysis. They defined four prominent genetic subtypes, with differences in expression profile and survival after R-CHOP treatment, 98 two of which had a favorable prognosis:
BN2, based on BCL6 fusions and NOTCH2 mutations, with a 5-year OS of 65%;
EZB, based on EZH2 mutations and BCL2 translocations, with a 5-year OS of 68%.
They also defined two groups with a lower 5-year OS:
MCD, based on co-occurrence of MYD88 and CD79B mutations, 5-year OS of 26%;
N1, based on NOTCH1 mutations, 5-year OS of 36%.
Moreover, an international group of researchers 99 performed whole-exome sequencing with an expanded bait set to detect recurrent mutations, somatic copy number alterations, and structural variants. They analyzed genetic drivers in DLBCL patients treated with R-CHOP and proposed five clusters, each with predominant alterations: one low-risk ABC DLBCL, two subsets of GCB-DLBCL, an ABC/GCB DLBCL independent group with biallelic inactivation of TP53, CDKN2A loss, and associated genomic instability. The findings, shown in Table 5, indicate variability subtypes and possible treatments with available drugs. Supplemental material Table 1 online shows current clinical trials comparing the addition of a targeted drug to R-CHOP versus the traditional R-CHOP regimen. Most of them are still recruiting patients; we need time to know whether there is a group where another standard of care may change R-CHOP.
Recent molecular subtypes of diffuse large B-cell lymphoma and proposed targeted therapy.

Schmitz et al. 98
Chapuy et al. 99
BCR, B-cell receptor.
Conclusion
The DLBCL landscape is heterogeneous. Immunochemotherapy R-CHOP has been a standard of care for two decades and cures approximately 70% of cases. Dose intensification fails to improve survival, whereas dose reduction in the elderly population is still under study. Using rituximab biosimilars in patients living in resource-limited settings could have a positive impact on healthcare costs. Adding new drugs to R-CHOP is also under study, as well as matching genetic alterations to treatments.
Supplemental Material
sj-pdf-1-tah-10.1177_2040620721989579 – Supplemental material for Rituximab in combination with cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) in diffuse large B-cell lymphoma
Supplemental material, sj-pdf-1-tah-10.1177_2040620721989579 for Rituximab in combination with cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) in diffuse large B-cell lymphoma by Myrna Candelaria and Alfonso Dueñas-Gonzalez in Therapeutic Advances in Hematology
Footnotes
Conflict of interest statement
The author(s) declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.