
Abstract
Benign fibro-osseous lesions are a diverse range of entities that have distinct clinical and radiographic features. They can occur as solitary lesions or concomitant with other pathologies as hybrid lesions. Fibrous dysplasia (FD) accompanied by central giant cell granuloma (CGCG), peripheral giant cell granuloma (PGCG) or peripheral ossifying fibroma (POF) as hybrid lesions, is reported very rarely in the literature. Although we were unable to find any reports of FD with PGCG as a hybrid lesion. Fibro-osseous lesions have certain histopathological features in common with PGCG including multinucleated giant cells. Here we report a 28 year old female with a painless, slow growing and pedunculated swelling of the maxilla for 18 months. Differential diagnosis consisted of FD, cemento-ossifying fibroma (COF), chondrosarcoma and probable PGCG considering radiographic and clinical investigations. Histopathologic findings revealed PGCG and FD as a hybrid lesion. The combination of PGCG and FD has not been reported in the literature so far.
Introduction
Peripheral giant cell granuloma (PGCG) is an intraoral, non-neoplastic developmental tumor-like lesion that is usually identified in gingiva or alveolar mucosa anterior to the molar region and moderately more frequently in the lower jaw. 1 This lobular, site specific and painless lesion can arise from periosteum or periodontal ligament (PDL). Females are affected predominantly and it can occur in a wide age range. 2
The ethiology of PGCG has not been clarified precisely yet, probably it is a reactive lesion which is caused by different irritating factors such as foreign bodies, calculus accumulation, residual cement and etc.
Foreign bodies can be crowns and dental implants. Our patient in this paper has natural dentation without any crowns or implants. The probable pathogenesis of PGCG associated with our case was accumulation of palque/calculus.
The diagnostic hallmark of giant cell granulomas, either peripheral or central, is the presence of multinucleated giant cells (MGC) in fibrotic stroma. The source of these MGCs could be phagocytes, foreign body cells or osteoclasts, even though studies have shown osteoclasts are more commonly the source. 3
Benign fibro-osseous lesions such as FD are a heterogenous number of bone anomalies that are described as hamartomatous formation of cellular fibrovascular connective tissue in medullary bone with varying amount of irregular, weakly calcified bone or cementum. Peak incidence of FD is the second decade of life and they occur unilaterally and mostly in the maxilla. The most challenging issue with FD is regrowth of the lesion after reshaping. 4
Hybrid lesions are referred to those lesions that have distinct features from different pathologies in one lesion concomitantly. In the literature, co-occurrence of CGCG with fibro-osseous lesions such as FD, COF, cemento-osseous dysplasia and Paget’s disease has been reported. 5 In the other hand, co-existence of PGCG only with peripheral ossifying fibroma (POF) have been reported in a few cases till now. 6 However, coincidence of PGCG and FD in one lesion has not been identified yet. In this paper, we report a hybrid lesion constituted of FD-PGCG in a 28 years old female to discuss clinical, radiographic and histopathological aspects.
Different surgical techniques are appraoched to treat FD and PGCG. Since then the exact diagnosis of these lesions is of crucial in order to avoid surgical under/overtreatment. PGCG lesions must be resected totally under local anesthesia or general anesthesia with extensive curretage of base of the lseion to avoid relapse. Despite of PGCG, FD lesions are being treated mainly surgical or non surgical. For stable or quiscent FD, observation and monitoring, use of bisphophonates, has been offered. However surgical approaches in problematic or symptomatic patients, comprises conservative or extensive shaving can be done.
Case report
A 28 year old female was referred to the department of oral and maxillofacial surgery of Tehran university of medical sciences with a slowly expansible right maxillary swelling encompassing the canine to tuberosity from 18 months ago.
Pre-op investigations
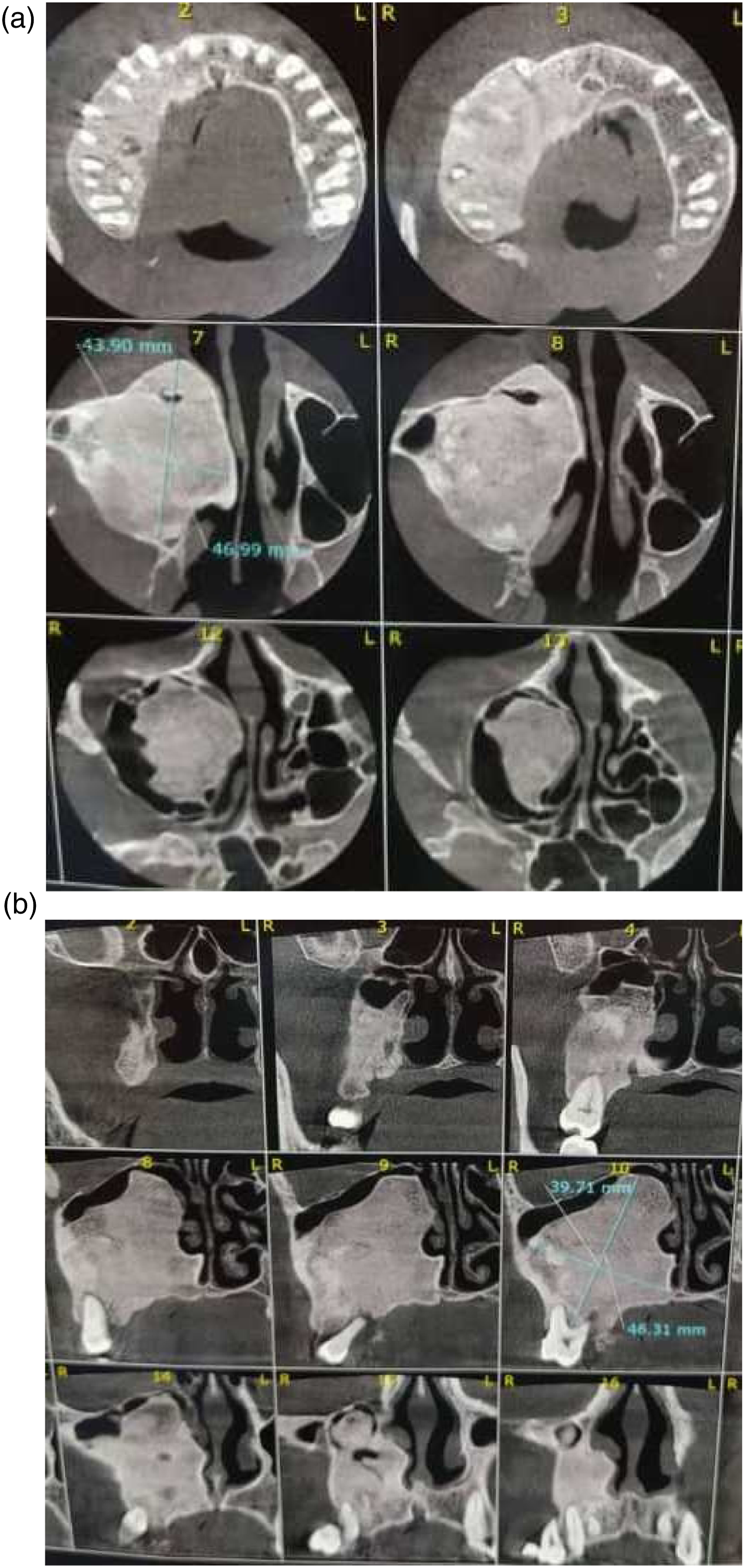
1. Intraoral examination revealed a fragile, pedunculated, red-white enlargement measuring approximately 3*4 cm in diameter. The lesion extended from upper right canine to tuberosity, from hard palate medially to buccal vestibule laterally. We identified the lesion to be firm on palpation, covered by pseudomembrane with some areas of superficial ulceration. This well-defined, exophytic, lobular mass was painless except for interference with occlusion or mastication. Moreover, other than scab in some areas, obliteration of the buccal vestibule, dental luxation in the involved area, no other pathological condition was found in intraoral examinations (Figure 1). 2. On extraoral investigation, there was noticeable bony hard malar swelling and obstruction of right nasal airway. However, no neurosensory disturbances and no lymphadenopathy was present. 3. Panoramic findings exhibited ill-defined radiopaque area in right maxilla with varying degrees of opacification and nearly ground glass appearance. Partial Root resorption and PDL widening of upper right molars and premolars was obvious (Figure 2). 4. CT scan was carried out and radiographic survey confirmed the well-defined expansile radiopaque lesion which was extended to the floor of the nose, right lateral nasal wall, right lateral wall of zygoma and right maxillary antrum (Figure 3). Based on clinical and radiographic characteristics differential diagnosis included FD, COF, chondrosarcoma and PGCG. 5. An incisional biopsy was performed under local anesthesia and the specimen was sent for histopathological analysis. Microscopic findings showed a lesion which was partially covered by stratified squamous epithelial and composed of large number multinucleated osteoclast-like giant cells and mineralized tissue formation scattered within a fibroblastic and cellular vascular stroma including many plump spindle cells (Figure 4). Foci of hemorrhage hemosiderin deposition and fibrinoleukocytic exudate were also noted. No necrosis was identified. The diagnosis of hybrid PGCG and FD was established. Clinical view of the lesion/clinical features showed an exophytic ulcerated large mass in the area of maxillary tuberosity extended to hard palate. Panoramic view of the lesion. Panoramic view showed an ill-defined radiopaque lesion in right posterior site of the maxilla extended to interradicular areas of the regional teeth. (a) Axial view of CT scan. They showed extension of the lesion to the floor of the nose, right lateral nasal wall, right maxillary antrum. (b) Sagittal view of CT scan. They showed extension of the lesion to the floor of the nose, right lateral nasal wall, right maxillary antrum. Macroscopic and microscopic view of the lesion. (a) Gross view of the lesion. (b) Mature lamellar bone trabecular with loose vascular connective tissue. (c) Proliferation of MNGs admixed with plump mesenchymal cells in hemorrhagic background.



Surgical approach
Following definitive diagnosis and preoperative work-up, informed consent was obtained from the patient. In the operation room, under general anesthesia nasotracheal intubation was carried out and then fixed by sutures to the membranous septum and columella. After prep and draping 2% lidocaine with1:100,000 epinephrine was injected into the right maxillary vestibular mucosa. The soft tissue, pedunculated, intraoral mass was totally resected to base of the lesion, using a scalpel. Hemostasis was achieved by the electrocautery. The ipsilateral premolars and molars were extracted.
Access to the right maxillary buttress and lateral wall of zygoma was achieved by flap elevation from canine to the tuberosity with anterior releasing in the mesial of the canine. By means of osteotomes some areas of bony expansion from lateral wall of zygoma and lateral nasal wall were removed and the remaining bony lesion was reshaped in order to improve esthetic and breathing. Following ensuring the hemostasis of surgical field, the irrigation of surgical field with copious serum was done. Intraoral incision was sutured with 4-0 vicryle.
According to permanent histopathological report, the neoplastic tissue was composed of lobulated sheets of multinucleated osteoclast-like giant cells in fibrotic stroma containimg multiple foci of fresh hemorrhage, aggregations of mgc, new bone formation, macrophages and some foci of granulation tissue formation. The stroma was cellular and fibroblastic with presence of many plump spindle cells. The diagnosis was PGCG and FD.
Follow up
No evidence of reccurrence and oroantral communication was found after 1 year of close follow up. However the recall sessions of the patient will be continued due to highly likelihood overgrowth of FD. In spite of many efforts to satistfy the patient with taking the 1-year follow-up imaging or photographs, we were not successful.
Discussion
As a result of the ambiguous behavior of fibro-osseous lesions, differential diagnosis is challenging. Patient history, clinical, radiographic and histopathologic features of these lesions must be considered for definitive diagnosis.
Approximately 84% of hybrid cases occur in mandible, specifically in posterior region with female predilection. Although in this paper, the hybrid lesion was present in the maxilla. Incidence age of hybrid lesions differs from 5 to 68 years old with mean age of 31 years old. 7 Our patient was 28 years old, although in previous studies hybrid lesions were observed in older patients.
According to clinical and physical evaluation, PGCG, POF, pyogenic granoluma, peripheral odontogenic fibroma can be considered as differential diagnosis. PGCG appears as a firm, soft, bright, pedunculated or sessile nodule with various sizes. The growth of PGCG can be stimulated by repeated trauma and rarely it affects the underlying bone. 2
FD is a well-defined, intrabony lesion with ground glass radiographic appearance. It is mainly composed of irregularly shaped bony trabeculae described as Chinese letter pattern. These bony trabeculae lacks osteoblastic border and are organised in the fibrous stroma, occupied with giant cells and erythrocytes. 4
The diagnostic challange was to describe the exact origin of the lesion whether it is a case of central lesion with overlying soft tissue involvement or an intrinsically peripheral lesion involving underlying bony structures. The combined histopathologic and radiographic features of both lesions was postulated to be reminiscent of hybrid lesion of FD and PGCG.
In hybrid lesions comprising of giant cell tumors associated with FD or other fibro-osseous lesions, it has been declared that these giant cells may show a reaction to stromal change in the original tumor. This stromal change could stimulate osteoblasts, who can activate osteoclast-giant cell type through paracrine mechanism.5,8
Recently it has been demonstrated that mgc in CGCG and PGCG have some similarities to osteoclasts like presence of acid phosphatase and osteoclast-specific cellular antigens. 9 Bo Liu et al. have concluded that osteoclast-like MGCs in these lesions arise from the fusion of mononuclear component that are osteoclast precursors. 3
A case report by Dmitry Jose et al. presented a 35 year old female with NF1 and painless extraosseous purplish-red soft nodule in the anterior mandibular region. Radiographic investigations revealed large mixed lesion, predominantly radiodense compatible with florid cement-osseous dysplasia. Their case fulfilled the diagnostic criteria for NF1 who had florid cemento-osseous dysplasia associated with PGCG unlike our case with no medical history. 10
Ramesh et al. reported a case of 57 year old female with a hybrid lesion that showed both features of PGCG and POFs in maxilla. Alveolar bone was not involved by the lesion and no calcified bone or cementum was present. 11 However, in our patient there was a massive radiopaque lesion with extensive involvement of right maxilla, nasal floor as well as right lateral nasal wall.
There is also a report of PGCG with distinct area of osseous formation along with stromal area, reminiscent of POFs in the posterior mandible of 44 year old man. 12 In addition, another case of PGCG combined with POFs as a hybrid lesion described by Mayara et al. in the left mandibular alveolar mucosa of a 31 year old female. 6 The capacity of bone tissue formation, either mature bone, osteoid or amorphous calcifications within the PGCG, has been demonstrated in different studies. 13 It is not yet defined whether PGCG with POFs is a true hybrid lesion, concurrency of two different entity or simply the ability of PGCG for bone tissue formation.
In our literature review, the first case of hybrid lesion of adenomatoid odontogenic tumor and odontoma was reported in a 18-year old boy in 1951. 14 All case reports of hybrid lesions containing a similar feature of GCG and mineralized components were CGCG except for three cases in addition to the present case report. To the best of our knowledge, this is the first report of hybrid lesion of PGCG and FD.
In general, there are three theories regarding the origin of hybrid lesions. The first theory describes “collision tumor” characterized by synchronized occurrence of both lesions. The second theory is primary occurrence of a true neoplasm followed by formation of the second lesion due to the production of some growth factors and chemokines by the initial lesion. The third theory proposes that after occurrence of the primary lesion, external stimuli including tissue trauma induce the formation of the second lesion. 15 It seems that in our case, PGCG evolved as a reactive lesion due to chronic trauma to the gingiva in the area with bony expansio.
In our case, the hybrid lesion was treated by surgical resection of the soft tissue tumor with elimination of the whole base of the lesion and bone reshaping. Removal of irritation source of the lesion and extensive clearing of the base of the lesion is crucial to prevent recurrence. Rate of recurrence of PGCG ranges from 5 to 11%. 2 In the present case, recontouring of the bony expansions was performed to improve esthetic and function of the patient.
Regarding the importance of the exact diagnosis followed by proper treatment plan of this kind of lesion, is the longterm follow-up of FD becuase of facial disfigurement and functional issues due to its occurrence.
Conclusion
We report a case of hybrid lesion that has both features of FD and PGCG for the first time. In order to be able to treat these lesions adequately and properly, the precise diagnosis is of the utmost importance. Misdiagnosis in hybrid pathologic lesions happens as a result of considering predominant features of one lesion by surgeons and pathologists and it can lead the clinician to unwilling mismanagement of patients. Therefore, all cases of rare hybrid lesions should be reported to achieve comprehensive understanding of interrelationship between lesions better.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient.