
Abstract
Leprosy, or Hansen’s disease, is a chronic granulomatous infection caused by Mycobacterium leprae, with a broad spectrum of clinical and histopathological manifestations. Histological examination plays a pivotal role in accurately diagnosing its various subtypes. Elastophagocytosis (phagocytosis of elastic fibers by giant cells) is typically associated with annular elastolytic giant cell granuloma and other granulomatous conditions but has rarely been reported in leprosy. We report the case of an 85-year-old male who presented with a solitary, slowly enlarging annular plaque on the trunk. The lesion was asymptomatic and exhibited mild sensory loss without peripheral nerve involvement. Histopathological analysis of the skin biopsy showed granulomatous inflammation with Langhans-type giant cells and a striking feature of elastophagocytosis. Fite-Faraco staining confirmed the presence of acid-fast bacilli, establishing the diagnosis of borderline tuberculoid leprosy. The patient was treated with multibacillary multidrug therapy and demonstrated complete lesion resolution.
Keywords
Introduction
Leprosy is a chronic infectious disease with ancient origins, continuing to affect millions globally and remaining a significant public health concern. Despite considerable advancements in medical, histological, immunological, and pathological understanding, the disease remains prevalent in many regions. Hansen’s disease (leprosy) is caused by Mycobacterium leprae, an obligate intracellular bacterium that primarily targets macrophages and Schwann cells. Histopathological analysis of skin and nerve biopsies plays a crucial role in confirming the diagnosis and classifying the disease into subtypes, which includes – tuberculoid (TT), borderline tuberculoid (BT), borderline, borderline lepromatous (BL), and lepromatous leprosy (LL). 1 Although each subtype displays distinct histological patterns, atypical features may complicate the diagnostic process. We report a rare case of elastophagocytosis – an uncommon histological finding in a patient with BT Hansen’s disease. To our knowledge, elastophagocytosis in the BT subtype has not been previously described, making this case a novel contribution to the literature.
Elastophagocytosis, the process of engulfment and degradation of elastic fibers by histiocytes and multinucleated giant cells, is a characteristic feature of annular elastolytic giant cell granuloma (AEGCG). 2 This phenomenon has also been observed in a spectrum of other cutaneous conditions, including inflammatory dermatoses, cutaneous malignancies, infectious diseases (e.g. leprosy, tuberculosis, fungal infections), and as a reaction to certain medications. 2 Although rare, elastophagocytosis has been previously documented in the BL and LL subtypes of Hansen’s disease. 3
Case report
An 85-year-old male presented with a gradually enlarging, asymptomatic, annular erythematous plaque persisting for 6 months. The patient appeared healthy, with no systemic symptoms such as fever, weight loss, or fatigue. On cutaneous examination, a well-demarcated lesion measuring 10 × 7 cm was noted on the lateral aspect of the right trunk. The plaque displayed an indurated border with central clearing (Figure 1). Sensory examination revealed mild hypoesthesia over the lesion, although there was no detectable thickening of cutaneous or peripheral nerves on palpation. Examination of the rest of the neuromuscular systems was unremarkable. The patient reported no history of chronic illness, previous surgeries, or drug allergies and denied smoking or alcohol use.

A well-demarcated lesion measuring 10 × 7 cm on the lateral aspect of the right trunk with an indurated border and central clearing.
Based on the clinical presentation, three possible differential diagnoses were made, which include BT Hansen’s disease, AEGCG, and sarcoidosis. To narrow down the diagnosis, a slit-skin smear for acid-fast bacilli (AFB) and a tuberculin skin test for Mycobacterium tuberculosis were performed, both yielding negative results. Additional investigations revealed normal serum angiotensin-converting enzyme (ACE) levels, and chest radiography showed no abnormalities, effectively excluding sarcoidosis.
Histopathological examination of the skin biopsy revealed hyperkeratosis, focal brownish pigment deposition, increased basal melanocyte activity, scattered melanophages, and minimal pericapillary inflammation. The dermis exhibited diffuse granulomatous inflammation with collections of epithelioid histiocytes, Langhans-type giant cells, and a dense infiltrate of lymphocytes and plasma cells (Figure 2). Importantly, occasional multinucleated giant cells demonstrated engulfed elastic fibers, a phenomenon consistent with elastophagocytosis (Figure 3). This histological finding is more typical of AEGCG, adding complexity to the diagnostic assessment. No features of vasculitis, atypia, malignancy, or caseous necrosis were identified. Given the overlapping clinical and histopathological features suggestive of both BT Hansen’s disease and AEGCG, Fite-Faraco staining was performed. This revealed the presence of AFB, thereby confirming BT Hansen’s disease as the underlying etiology (Figure 4).

Histopathological features of the skin lesion.
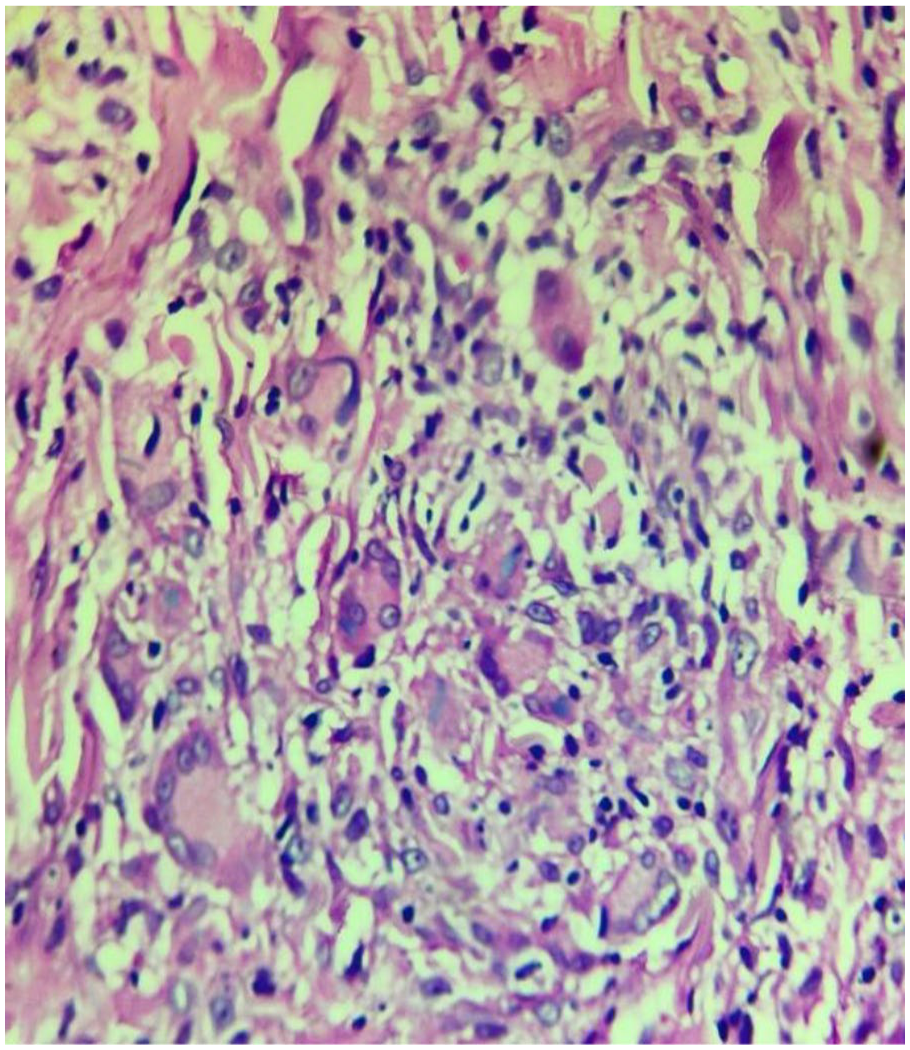
Elastophagocytosis observed within granulomatous inflammation.
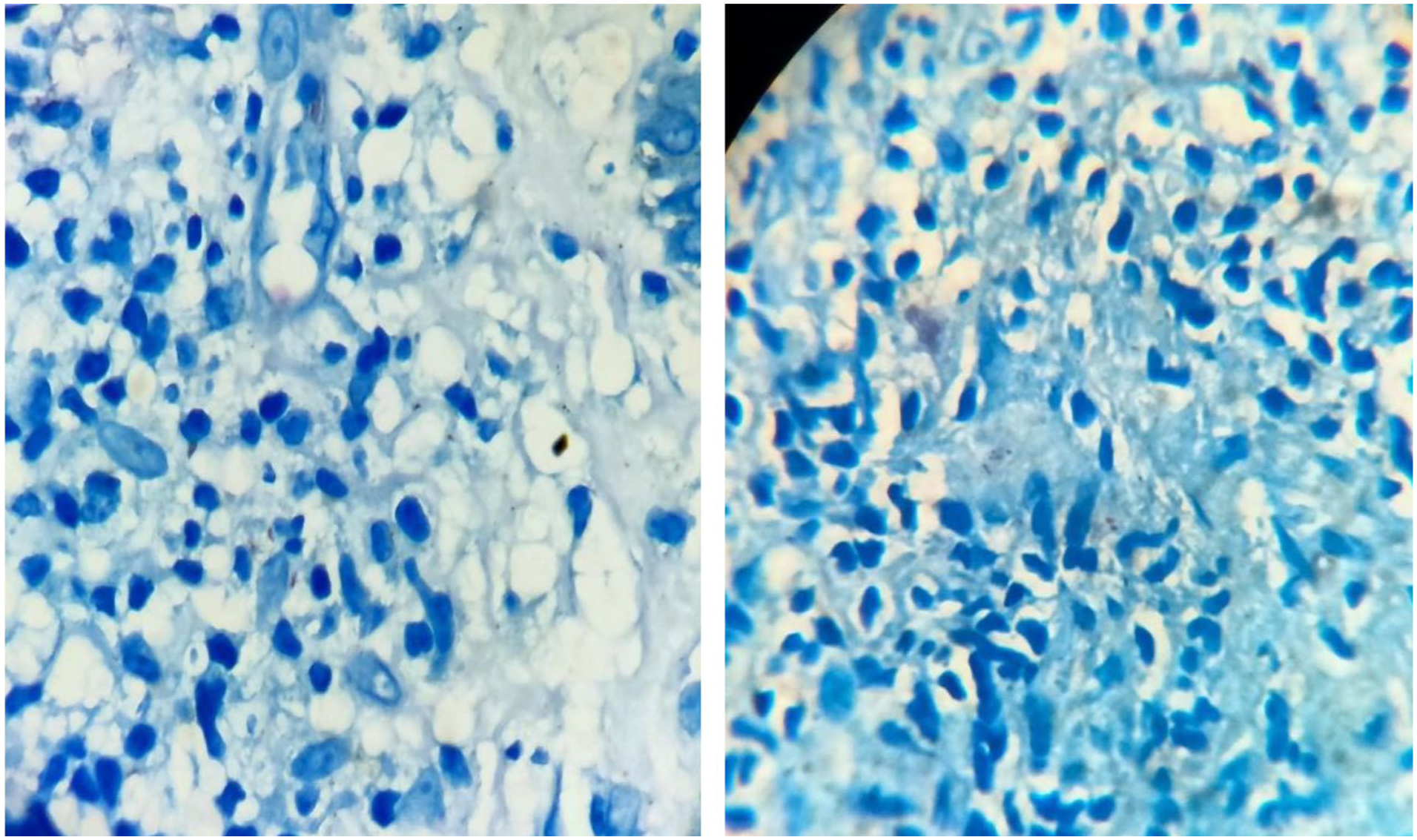
Detection of Mycobacterium leprae by Fite-Faraco staining.
The patient was initiated on the standard multibacillary multi-drug therapy (MB-MDT) regimen, which comprised Rifampicin 600 mg administered once monthly under supervision, Clofazimine 300 mg once monthly (supervised) along with a daily self-administered dose of 50 mg, and Dapsone 100 mg taken daily on a self-administered basis. The patient demonstrated a favorable response to therapy, with complete resolution of the lesion by the end of the 12-month treatment course (Figure 5). Notably, this case represents the first documented instance of elastophagocytosis in the BT subtype of leprosy. The unusual histopathological finding posed a significant diagnostic challenge, highlighting the need for careful correlation between clinical, histological, and microbiological data in cases of suspected Hansen’s disease.

Clinical resolution of the lesion following MB-MDT.
Discussion
BT leprosy is the most common and extensively studied subtype within the leprosy spectrum. Clinically, skin lesions in BT leprosy subtypes resemblance to those seen in the tuberculoid (TT) form but tend to be more numerous and variable in presentation. This variability is thought to result from an enhanced cell-mediated immune response against Mycobacterium leprae, which characterizes the borderline forms of the disease.1,2 Elastophagocytosis refers to the phagocytosis of elastic fibers by histiocytes and multinucleated giant cells, visible under light microscopy. 2 Although the exact pathogenesis remains unclear, elastase, a proteolytic enzyme, is believed to play a central role in mediating this process. The interaction between elastase and elastin is thought to be governed by electrostatic forces. 2 Several mechanisms have been proposed to explain elastolysis, including defective synthesis of elastic tissue, elastase release from inflammatory cells, diminished serum copper levels, and immune-mediated reactions.3,4 It remains uncertain whether inflammation serves as the primary trigger for elastophagocytosis or emerges as a secondary phenomenon. However, evidence suggests that inflammation may be a prerequisite for the initiation of elastolytic activity. 4 Alterations in elastic fibers, both qualitative and quantitative could result from inherited disorders or be acquired through physiological aging and pathological processes.
Elastophagocytosis is particularly characteristic of localized elastolytic disorders, such as AEGCG, actinic granuloma, granulomatous slack skin, and other elastolytic dermatoses like mid-dermal and papillary dermal elastolysis.2,5,6 Granulomatous infections and inflammatory dermatoses have also been associated with elastophagocytosis, likely due to the ability of neutrophils and certain pathogens to stimulate elastase release, thereby degrading elastic fibers. 2 An inconsistent presence of elastophagocytosis has been noted in conditions such as granuloma annulare, lichen sclerosus, sarcoidosis, granulomatous mycosis fungoides, and atypical fibroxanthoma. Less frequently, it is observed in a wide range of cutaneous diseases, including necrobiotic xanthogranuloma, Sweet’s syndrome, morphea, anetoderma, acquired cutis laxa, pseudoxanthoma elasticum, linear elastosis, dermatofibroma, basal cell carcinoma, keratoacanthoma, and eruptive vellus hair cysts. Certain infections, such as cutaneous leishmaniasis, blastomycosis, and LL, have also been reported to exhibit elastophagocytosis.2–4
BT Hansen’s disease must be differentiated from other granulomatous skin disorders, notably sarcoidosis and AEGCG (Table 1). Sarcoidosis is typically associated with systemic manifestations such as bilateral hilar lymphadenopathy visible on chest radiography, elevated serum ACE levels, and a lack of AFB. In the present case, the normal chest X-ray, normal ACE levels, and positive identification of AFB effectively rule out sarcoidosis as a potential diagnosis. 7 Previous studies have documented elastophagocytosis in BL and LL.3,8 However, to the best of our knowledge, this is the first reported instance of elastophagocytosis in borderline BT leprosy. In this case, skin biopsy revealed lympho-epithelioid granulomas with occasional Langhans-type giant cells, findings consistent with BT Hansen’s disease. 9 While elastophagocytosis is a hallmark histological feature of AEGCG,10,11 its occurrence in leprosy, particularly along the tuberculoid spectrum, is exceedingly rare. The annular morphology with central clearing, combined with the histological evidence of elastophagocytosis, initially suggested a diagnosis of AEGCG. However, the Fite-Faraco stain demonstrated the presence of AFB, a finding absent in AEGCG, thus confirming BT Hansen’s disease as the definitive diagnosis. The central clearing observed in the annular lesion may be attributed to elastolytic activity by multinucleated giant cells, histiocytes, and Langhans cells within the non-caseating granulomas of BT Hansen’s disease. The indurated border likely reflects the peripheral expansion of the granulomatous inflammatory response. The coexistence of positive AFB staining with elastophagocytosis in a patient diagnosed with BT leprosy is an unusual and previously unreported finding, adding a novel dimension to the histopathological spectrum of the disease.
Differential diagnosis of BT Hansen’s disease.

AEGCG: Annular elastolytic giant cell granuloma: AFB: Acid-fast bacilli; ACE: Angiotensin-converting enzyme.
Conclusion
This case highlights a rare and previously unreported histopathological finding of elastophagocytosis BT Hansen’s disease, confirmed by the presence of AFB on Fite-Faraco staining. While elastophagocytosis is typically characteristic of AEGCG, its occurrence in BT leprosy presents a diagnostic challenge due to overlapping clinical and histological features. The identification of AFB, although uncommon in BT leprosy, was pivotal in establishing the correct diagnosis. This emphasizes the importance of comprehensive histopathological evaluation and the use of special stains in cases with atypical presentations. Clinicians and pathologists should remain vigilant for such unusual overlaps, as timely and accurate diagnosis is essential for guiding appropriate treatment strategies.
Footnotes
Acknowledgements
Special thanks to Squad Medicine and Research (SMR) for their guidance and help in publication.
Ethical considerations
In our university, ethics approval was not required for case reports and case series.
Consent to publication
Written informed consent was obtained from the patient for the research and the publication.
Authors contributions
Raj M – Approved final draft, Conceptualization, Idea, Supervision, Writing draft.
Thomas V – Approved final draft, Conceptualization, Idea, Supervision, Writing draft.
Anand KRG – Resources, Revision of draft and approved final draft, Writing draft.
Suvvari TK – Approved final draft, Formal analysis, resources, Writing draft and revision of draft.
Barne HS & Bauskar RS – Approved final draft, Visualization, Writing draft and revision of draft.
Singh T – Formal analysis, Idea, Project administration, Revision of draft and approved final draft, Writing draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.