
Abstract
Giant cell arteritis is a granulomatous vasculitis of large and medium sized arteries manifesting as temporal arteritis and/or polymyalgia rheumatica. The histological assessment of temporal artery biopsies is frequently encountered in anatomical pathology and has important diagnostic consequences in patients clinically suspected of having giant cell arteritis. We present an intriguing case of giant cell arteritis associated with a Basal cell carcinoma and discuss the ongoing controversy pertaining to the association of giant cell arteritis/polymyalgia rheumatica with malignancy.
Introduction
Giant cell arteritis (GCA) is a systemic granulomatous vasculitis of large and medium sized arteries manifested either as a local temporal or cranial artertis (TA) or as polymyalgia rheumatica (PMR), an entity characterized by pain and stiffness of the shoulder and hip girdles or proximal extremities.1–3 The clinical features of TA usually include localized pain, often accompanied by jaw claudication; delay of appropriate treatment for TA carries a risk of ophthalmological and neurological complications.1–3 Notably, not all cases of GCA manifest with both TA and PMR; indeed, most cases of GCA manifest as PMR and many cases of TA do not present with other rheumatologic symptoms. 4 Interestingly, whilst some authors have noted an association between PMR and malignancy,5,6 recent studies have questioned the association between histologically confirmed GCA (i.e. cases of TA) and malignancy.7–10 We present an intriguing case of basal cell carcinoma identified in the same biopsy specimen as GCA.
Case Report
An eighty three year old male presented to his primary care physician with a left temporal non-traumatic, ulcerating lesion. In the three months prior to his presentation, he had also noted periodic intense unilateral headaches, vague symptoms reminiscent of jaw claudication as well as increasing proximal muscle pain in his upper limbs. The patient did not, however, note any vision changes or neurologic symptoms. The skin lesion to his left temple was clinically consistent with a basal cell carcinoma and he was subsequently referred to a plastic surgeon for surgical resection. In the interim, to investigate his headaches and other symptoms, the patient's family doctor requested a magnetic resonance image of his brain, which noted only age-related changes. Excision of the left temple lesion revealed an ulcerating basal cell carcinoma (Figure 1), clear of the surgical margins of resection. In addition, a portion of presumed temporal artery noted at the periphery of the primary lesion showed mural-based granulomatous inflammation associated with fibrinoid necrosis obliterating the internal and external arterial elastic laminae (Figure 2). The case was diagnosed as left temple basal cell carcinoma with concomitant giant cell arteritis. The patient received immediate steroid therapy and is well after 2 years of follow-up.
Low-power photomicrograph demonstrating basal cell carcinoma component (top left) with underlying giant-cell arteritis (bottom right) (Hematoxylin and Eosin, 20×).
A) Basal cell carcinoma (Hematoxylin and Eosin, 40×); B) giant-cell arteritis (Hematoxylin and Eosin, 100×); C) giant-cell arteritis (Elastic Van-Gieson, 100×).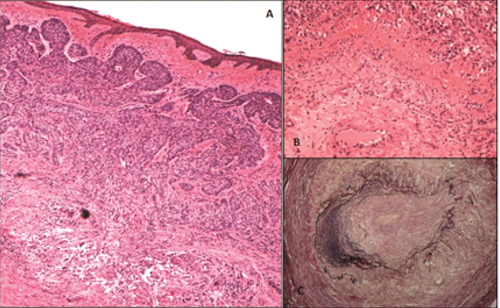
Discussion
GCA is a systemic granulomatous arteritis and may involve large and medium sized arteries from the aortic arch to the scalp. 1 Giant cell arteritis is a descriptive histologic diagnosis for a spectrum of rheumatologic entities with similar histological features. 2 We were able to note only one other such instance of a reported concurrent basal cell carcinoma with underlying giant cell arteritis; in the former case, however, high clinical suspicion of temporal arteritis was the primary indication for biopsy and the overlying basal cell carcinoma was not ulcerated. 11 A review of the English language literature notes a number of individual case reports and case series of GCA occurring in association with a malignancy. GCA has been identified in association with tongue squamous cell carcinoma. 12 A report of an invasive ductal carcinoma of the breast with concomitant breast-limited GCA was also noted. 13 In a study of 35,918 patients hospitalized for treatment of GCA (either diagnosed with PMR or TA), 3941 patients developed subsequent cancer; the authors noted that this translated to a 19% increased incidence of cancer in patients with GCA relative to controls with a notable increased risk of skin cancer and acute myeloid leukemia. 6 In another study of 271 patients diagnosed with GCA by Liozon et al., subsequent malignancy was noted in 20 patients. 14 In this study, the reported average time from diagnosis of GCA to detection of malignancy was 3.5 years and the malignant diagnoses were also predominantly hematolymphoid (45% of cases), though cancers of the gastrointestinal tract were also noted. 14 This study led the authors to suggest that some malignancies may act as precipitants of TA.
In contrast, a number of other studies have disputed the claims of an association between GCA and malignancy. Hill el al studied 226 cases of biopsy-proven GCA and noted that only 31 cases were diagnosed with cancer subsequent to their diagnosis of GCA; they concluded no increased risk for malignancy in subjects with biopsy-proven GCA relative to the general population. 10 In another study, Gonzales-Gay reviewed the medical records of 255 patients with biopsy-proven GCA and noted only a slight increased incidence of cancer in this cohort, without any evidence of worsened cancer-related mortality. 7 Finally, Kermani et al. performed a population-based case–control study including 204 GCA cases and 407 controls and noted that GCA patients had no overall increased incidence of cancer, and comparable mortality rates due to cancer relative to the control group. 8
GCA is believed to be immunologically mediated.1,2 Some malignancies have been noted to cause systemic immune dysregulation. 15 These observations may account for the contradictions noted pertaining to the correlation between GCA and cancer. In particular, as Stern argues, 16 both cancer and GCA can produce similar a myalgic clinical picture; clinical bias, therefore, may erroneously draw associations between GCA and malignancy. It should be noted, however, that both malignancies and GCA are diseases showing a predilection for older age groups and thus, 17 despite the contradictory data regarding a possible association between GCA and malignancies, it is incumbent on the surgical pathologist to diligently examine all histologic sections in either context to ensure that the other entity is not present concomitantly. Failure to identify GCA in a biopsy to examine a lesion suspicious for malignancy, or vice versa, can put the patient at a significant risk of improper management.18–20