
Abstract
Introduction
Poisoning contributes to significant morbidity and mortality worldwide, 1 and is the leading cause of injury and death for patients aged 1-44 in the US. 2 In 2021, more than 2.8 million calls were made to the Poison control centres in the US. 3 Poison centres have been shown to reduce healthcare costs from timely and effective poison management information. 4
Locally, a study in 2009 showed that poisonings comprise 1% of Emergency department (ED) attendances, with a 30% admission rate. 5 A study from the previous Drug and Poison Information centre 6 showed cost-benefit by reducing unnecessary hospitalizations.
Singhealth is a healthcare cluster consisting of 4 general hospitals (1 paediatric and 3 adult with EDs which see paediatric patients) with a total of 4699 beds and a total ED attendance of 522910 for the financial year of 2019/2020. 7 Of the 3 adult EDs, one has an Emergency Department Observation Unit (EDOU) protocol that provides psychiatric care to admitted poisoning patients during the study period.
A 24-h, hospital physician-initiated toxicology teleconsultation service was started in Changi General Hospital in 2014, 8 with toxicology fellows taking first line calls and toxicologists providing supervisory consultation. Most of the cases were consulted via phone while some of the cases were seen in person by the toxicology team members. The service expanded to include all the institutions of Singhealth in May 2019. The epidemiology and outcome of poisoning cases referred to the service over a 2-year period from inception (May 2019 to April 2021) are described here.
Methods
A retrospective audit review was performed on all patients referred to the Singhealth Cluster Toxicology service from May 2019 to April 2021. The consultation records of the toxicology service are kept in a central secure database. Information from these records as well as relevant hospital records are accessed, and the required data extracted. Records were excluded if they are duplicates, have missing identifiers, are incomplete or are information enquiry calls without patient data.
Patient demographics, exposure patterns, clinical presentation, interventions received, and outcomes were examined and presented. The Poisoning Severity Score (PSS)9,10 was used to determine the severity of poisoning, with 0 = asymptomatic, 1 = mild, 2 = moderate, 3 = severe and 4 = fatality. This is assessed at the initial consultation with the service (initial PSS), with the maximum severity for the poisoning episode determined when the patient is discharged (maximum PSS).
The likelihood of exposure to poisoning agents is based on the case presentation, on a scale of 1-4 with 4 = definite exposure (supported by laboratory or other investigations), 3 = probable exposure, 2 = possible exposure (other causes were equally likely) and 1 = unlikely due to poisoning exposure (other causes being more likely). The cases were abstracted onto a password-protected excel file and the de-identified data analysed. Information about resource use: EDOU, ward Length of Stay (LOS), High Dependency (HD) and Intensive Care Unit (ICU) utilisation was obtained. Cases placed on extracorporeal membrane oxygenation (ECMO) and fatalities were also reviewed for causation. The relative contributions of poisoning to the fatality were determined using the relative contribution to fatality (RCF) scale that is used in the American Association of Poison Control Centres annual reports. This is determined by 2 senior clinicians after review of records and the final score obtained by consensus. All data was entered directly into a standardised Microsoft Excel (Microsoft, Redmond, WA. USA) spreadsheet. Descriptive data is presented, while categorical data is presented as percentage frequencies, and continuous data is presented as medians with interquartile ranges (IQRs). No statistical analysis was performed. This study was approved by the Singhealth Institutional Review Board with a waiver of consent.
Results
A total of 974 records were available for the period May 2019 to April 2021. 63 records were excluded after chart review and 911 records were analysed. (Figure 1). Across the 2 study years, there were 406 cases from May 2019 to Apr 2020, and 505 cases from May 2020 to Apr 2021. The ED referred 87.2% of patients, followed by the EDOU and the inpatient wards (5.7% each). There were 28 recorded instances of a second call made during the same patient journey. Of note, 62.3% of all calls were made after office hours (5pm to 8am). Most consults came from the adult hospitals (98.6%) with 1.4% from the paediatric hospital. Review of records.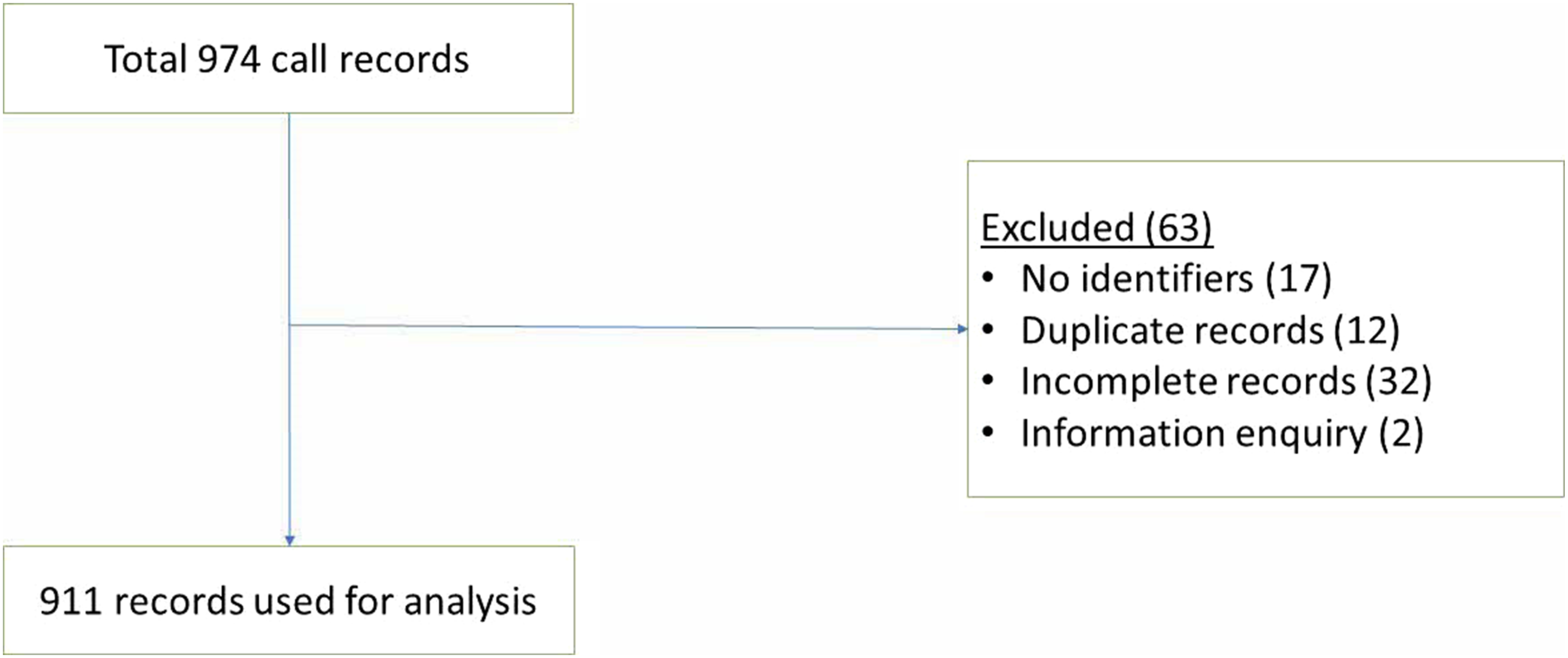
Figure 2 shows the demographics of referred patients. 462 (50.7%) were male. The age group from 20 to 29 was the largest at 29.9%. The cohort ranged from 1 to 97 years old with a median of 32 years (IQR 22-48). Population Demographics. Line denotes proportion of Males in each age group.
Most of the patients attended the ED via ambulance (55.0%) and 84.3% were self-referred, without a prior primary care consult. 5.9% of the patients came to hospital within 1h of poisoning, 43.8% within 4 h and 76.7% within the first 24h, while 4.7% came to hospital after 24h of poisoning. The rest of the cohort had an unknown timing of exposure or had repeated exposures.
Oral was the most common route of exposure (81.7%), followed by dermal (7.8%) and inhalational (5.0%).
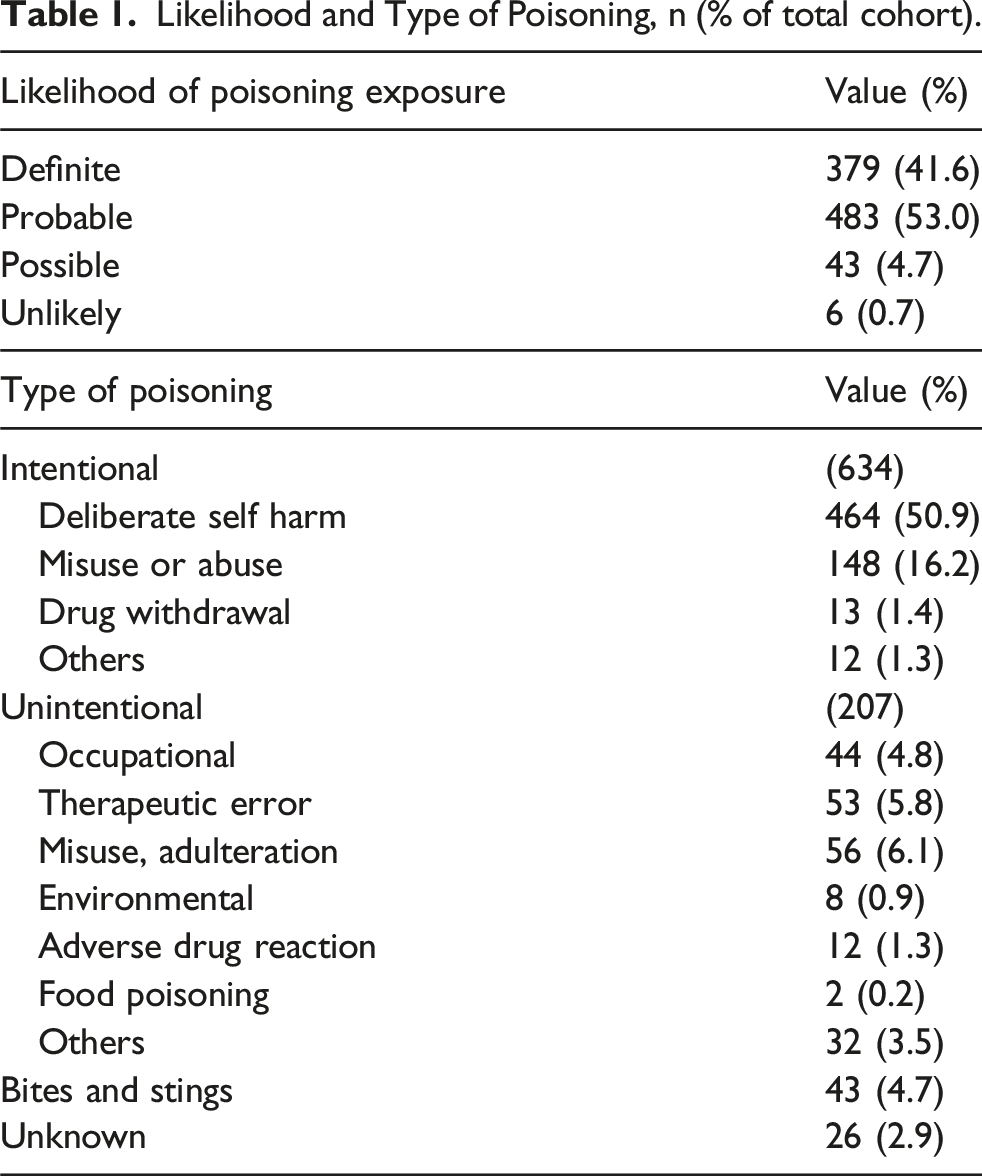
Likelihood and Type of Poisoning, n (% of total cohort).
Most patients (57.1%) were exposed to 1 poison, 20.1% by 2 poisons, and 19.8% by 3 or more poisons. The 3 commonest classes of poisons were analgesics (20.4%), sedatives (19.2%) and antidepressants (9.1%). Figure 3 shows the distribution of poisoning classes. Poison by class.
Changes in poison severity score throughout patient journey.

The most common symptom complaint related to the nervous system (44.1%), followed by gastrointestinal (21.4%) and cardiovascular (8.2%) symptoms.
Interventions given to patient.

Disposition of patients from the ED.

Admitted patients stayed a median of 3 days (IQR 2-6, Range: 1-86). Patients who were admitted to HD/ICU spent a median of 2 days in the respective critical care areas. (IQR 1-3.5, 1-17), with a median total hospital LOS of 5 days (IQR 3-10.5, 1-62)
Subgroup analysis of critical cases (patients admitted to HD or ICU)
The toxicology service was consulted for 153 critically ill cases (140 patients admitted to HD or ICU from the ED, and 13 patients that deteriorated from GW and EDOU), accounting for 16.8% of calls. 58.8% of the patients were male, with a median age of 41 (IQR 27-52.5). 85.7% of consults was from the ED, with 61.7 % occurring after office hours. Most patients were brought in by ambulance and self-referred (66.9%). The majority (68.8%) was for intentional poisoning, made up mostly of deliberate self-harm (62.3%) and drug abuse (30.2%). Most were exposed orally (83.8%) and 43.5% were exposed to one poison only.
Analgesics and sedatives were the commonest poisons involved followed by cardiac medications and antidepressants. Initial PSS was 3 for most cases (50.6%). The nervous and cardiovascular systems were the most commonly involved.
50 patients were intubated (32.6%) in this group, and 17 patients received activated charcoal. Enhanced elimination was started on 8.5% (11 cases of Haemodialysis, 3 cases of urine alkalinization and 1 case of multidose activated charcoal), while 54.3% received antidotes. 17.7% had inotropic support & 3 cases received ECMO.
Use of ECMO for poisoning
Three poisoning cases received treatment with ECMO. One had received VV-ECMO for severe pneumonia that was unrelated to toxic exposure (Fatality case 9)
The latter 2 cases described below involved poisoning with cardiotoxins, resulting in refractory shock despite conventional treatment. Both patients made full recoveries.
The first case was a 44-year-old woman with an overdose of amlodipine, fluoxetine and zopiclone, presenting in refractory vasoplegic shock about 5 h later, despite treatment with fluids, calcium, high dose insulin euglycemic therapy (HIET), vasopressors and methylene blue. ECMO was instituted at about 18 h post ingestion with albumin haemodialysis and therapeutic plasma exchange for extracorporeal toxin removal. ECMO was explanted after 60 h.
The second was a 66-year-old male with a history of ischaemic heart disease who ingested amlodipine and quetiapine 12 h prior to presentation at the ED, presenting with a mixed cardiogenic and vasoplegic shock (Left ventricular ejection fraction (LVEF) 45%) which was refractory to resuscitation with fluids, calcium, vasopressors, HIET and methylene blue. ECMO was initiated followed by therapeutic plasma exchange and albumin dialysis. ECMO was explanted after 53 h.
Deaths
A total of 9 patients died in this cohort, 1 at the end of initial consultation in the ED and 8 during hospital admission. They are presented below with their RCF scale.
Case 1/undoubtedly responsible: A 25-year-old woman sustained a cardiac arrest while abusing inhaled ethyl chloride. She had a return of spontaneous circulation after resuscitation but passed away from cerebral hypoxic ischaemic injury 5 days later.
Case 2/undoubtedly responsible: A 46-year-old man who presented with altered sensorium, hyperthermia, and hypotension was admitted to the ICU and died after 4 h. Blood toxicology revealed an olanzapine level of 380 ng/ml (therapeutic level:20-40 ng/ml).
Case 3/undoubtedly responsible: A 41-year-old man found with altered sensorium after using methamphetamine and gamma hydroxybutyrate. He survived a cardiac arrest from ventricular fibrillation but died the next day. Blood toxicology revealed the presence of amphetamines.
Case 4/contributory: A 45-year-old man with a history of previous nitrazepam use was admitted for cardiogenic shock to the ICU and died after 1 day. Toxicology tests revealed the presence of nitrazepam in the blood and urine.
Case 5/unknown: A 76-year-old woman with extensive medical history was referred for raised digoxin levels presenting with lethargy. Digoxin was omitted with down trending of levels, but the patient died from other causes 40 days later.
Case 6/unknown: An 81-year-old woman on regular digoxin presented in cardiac arrest after being treated for a UTI. She was found to be acidotic, hyperkalaemic and died in the ED.
Case 7/clearly not responsible: A 58-year-old man who was referred for advice after larger than normal amounts of silver nitrate were used for wound cauterisation. The patient subsequently passed away 2 months later from pneumonia.
Case 8/clearly not responsible: A 61-year-old female with metastatic lung cancer who was suspected to have been administered an alleged inadvertent overdose of subcutaneous fentanyl. The overdose was clarified to have not happened upon investigation.
Case 9/clearly not responsible: A 35-year-old man who was being treated for adult respiratory distress syndrome from pneumonia who went onto veno-venous ECMO, and a consult was made to identify a possible toxicological cause of his severe lactic acidosis. None was found. He passed away after 13 days of hospital care.
Discussion
Rate of consults
Our study of 911 cases in the first 2 years of a cluster wide teleconsultation-based toxicology service is the largest study locally. During this period, the ED attendance for the 3 adult hospitals was 691682 while that for the Pediatric hospital was 243448. The number of consults/ED attendances works out to be about 911/935130 = 0.097% of the total ED attendance. Considering only the 3 adult EDs, the rate of consults was 898/691682 = 0.13%. This is lower compared to a previous single-centre adult ED study which reported a rate of about 0.2%. 8
Consultation of cases is physician dependent and hence our data does not reflect all the poisoning cases that attended the ED. The number of consults from the pediatric hospital is very low, probably reflecting the publicity of the service to the pediatric hospital and the internal process of managing poisoning in that hospital. 11 As the service just started in May 2019, the number of referrals picked up with publicity and recognition of the service, with an increase in consults in the second year of service by 24%.
Overall, this consult rate is lower than the poisoning rate of 0.94% in the 2001 study 5 which attempted to capture the total number of poisoning cases. Another local study 12 from another hospital reported 0.4% from toxic exposures for their ED cohort. Our data suggests that about 1 in 3 to 7 cases would have been referred to the service if the poisoning rate had remained constant. Besides publicity and awareness of the resource, the consult rate is also dependent on physician experience, preferences, department policy and protocols. Further study may clarify this phenomenon.
Poisoning epidemiology
The commonest group in our cohort was 20-29 years of age, followed by 30-39 and 12-29 years. This is comparable to previous studies5,8,12 and continues to show how poisoning affects the financially active members of our society.
Slightly more than half of our patients came by ambulance and more than 80% are self-referred. reflecting the health-seeking behaviour of poisoned patients: they tend to go to the hospital as the first point of healthcare contact and would more likely come by ambulance. About half the cohort sought help at the ED within 4 h of exposure, which continues to present opportunities for early risk assessment and intervention.
Route of exposure continued to be predominantly oral, similar to previous studies.
Most patients were intentional poisonings, mostly due to deliberate self-harm and drug abuse, highlighting a problem for which harm prevention (improved psychiatric care, less toxic psychiatric medications, and more extensive support programs for abuse) can help to tackle. The epidemiology in our study is similar to other developed countries. 3
Similar to previous studies, the commonest class was analgesics, sedatives and antidepressants, with similar rates of nervous, gastrointestinal and cardiovascular symptoms. 8
Overall, most of the patients have a low PSS of 0 and 1 (67%). However, the number of patients with PSS of 3 increased compared to the previous study from 3 to 13%. 8 This could suggest that consults are made for higher acuity cases where the need is greater. A small number of patients deteriorated during their journey. This is not unexpected in view of continued absorption of poison with delayed effects. This reinforces the need for appropriate disposition of patients so that adequate monitoring and treatment can be instituted.
Disposition of cases
In our cohort, 27.4% of patients were admitted to the EDOU of which most patients (88%) were admitted for less than 23h.
For self-harm, engaging psychiatric resources early in EDOU can reduce the need for admission to access such care. EDOU has been shown to reduce inpatient admission and cost.13,14 The poisoned patient represents a group which, barring the most critical patients, require short periods of hospitalization.
Of the patients admitted to the ward directly, 12.2% were admitted for 1 day, and 20.0% were admitted for 2 days. In our experience, most patients recover clinically within 72 h and there is a potential to reduce LOS with concurrent psychiatric assessment. Also, the use of EDOU was only common in one of the hospitals in our cluster, which had poisoning protocols employing a multidisciplinary approach, allowing the delivery of critical care, toxicological resource, psychiatric assessment, and medical social work support within 23 h for suitable patients. This data suggests that there is room for improvement in setting up more service-integrated EDOUs, which can manage patients who only require a short period of hospitalization, to reduce inpatient bed demand.13-19.
HD/ICU
A small number of patients required HD/ICU therapy, which include respiratory, cardiovascular and dialysis support (for renal support and toxin removal) which points to the low morbidity of this cohort. This number is higher (16.6% compared with 8.9%) than the study done 4 years prior. 8 Another previous local study (>20 years ago), reported 50 patients admitted to the ICU at a hospital over 3 years (17 case per year). 20 Our cohort had 50 patients (25 per year) who were admitted to the ICU, but is based on the population attending 3 adult general hospitals. A separate analysis of these patients suggested a slightly older cohort and no other significant differences with the main cohort.
Fatality
Fatality was low in our 2-years cohort at 0.99%. This is comparable to another local poison study at 1.7%. 8 The Hong Kong Poison Centres also reported a fatality rate around 1%. 21
Benefits of toxicology service
Most calls (62.3%) were made after office hours, a period of reduced senior staffing in hospitals. This illustrates how a 24-h toxicology phone consult service is a valuable resource for the management of poisoned patients, who often require prompt assessment and prognostication, experienced management from senior healthcare staff, expedient treatment including antidote use and employment of hospital resources to provide supportive care and extracorporeal toxin removal. Continuity of care was also provided for 28 cases for which a second call was recorded. Moreover, antidotes, decontamination, enhanced elimination are not commonly used, and clinicians may not be familiar with their use. In our cohort, 16.4% of patients needed higher acuity care and these patients needed more interventions. Previous studies have showed that toxicology service was helpful for inpatient management.15–19 The toxicology service can also serve a surveillance function for occupational health issues, medication error, drug of abuse patterns and poisonings from malicious/deliberate intent with risk to public health. The service could work closely with stakeholders to introduce measures to improve medication safety and better protect workers and the public.
The Singhealth cluster is one of the 3 healthcare clusters in Singapore, with a total A&E attendance about 368 983 7 patients in 2019 which is about (368983/1080982) = 34% of the national A&E attendance in 2019. 22 Extrapolating from our poisoning consult rate of 0.13%, the total workload for a nationwide toxicology consult service yearly could come up to 1400 cases (116 cases a month) with about 235 cases (19 cases a month) admitted to HD/ICU and 13 fatalities (or 1 case a month). This is lower than the data from Hong Kong Poison Centre where 2100 cases consulted the poison centre a year 21 but it is still a substantial number. The need for a national level poison consultation service to cater to the management of poisoned patients should be considered for cost effectiveness and efficacy in healthcare management in future planning.
Limitations
Consultation with the cluster toxicology call service is physician dependent, hence the data captured on poisoning load is an underestimate of the total burden of poisoning cases in the hospital cluster, representing the real-world practice in the institutions.
Only hospital-based physicians are supported by this service; hence this study does not include unreferred community poisoning cases.
As this is primarily a phone consult service with limited onsite patient reviews, the assessment, management and accuracy of data captured are dependent on the primary treating physicians.
A limitation about LOS in our study is that it includes the LOS attributed to psychiatric treatment. Therefore, the overall LOS may not be reflective of LOS required just for poison management.
Conclusion
Poisoned patients constitute a unique part of our patient cohort, with characteristic presentations and prognoses which can be improved with early recognition and institution of appropriate measures. Our study offers insights to patient characteristics, behaviour and opportunities for intervention that would better serve this cohort. Periodical audit reviews of data collected can inform future planning efforts for resource allocation and efficient utilisation of hospital beds.
Footnotes
Ethical considerations
This study was approved by the SHS Institutional Review Board with a waiver of consent: 2021-2794.
Consent to participate
This study was approved by the SHS Institutional Review Board with a waiver of consent: 2021-2794.
Author contributions
KKK wrote the first draft, RP and THH reviewed the manuscript, performed data abstraction and analysis, GA, AK, MRP, NMW, IH, TBP and GO performed data abstraction.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are available from the corresponding author.