
Abstract
Background
The roles of physiotherapy in Intensive Care Unit (ICU) have significantly developed from the traditional management of respiratory conditions to early rehabilitation and mobilisation of patients on mechanical ventilation. Surveys of United Kingdom, Australia and regional ICU physiotherapy practice have been published but there are no local data sets. This study aims to report the physiotherapy practices across the adult ICUs of Singapore.
Methods
Twenty-nine item questionnaire was mailed to 90 physiotherapists working in 15 adult ICUs across restructured and private hospitals in Singapore. Data sets were summarised from the returned questionnaires. This includes identifying common physiotherapy techniques and exercise prescription protocols for both mechanically and non-mechanically ventilated patients in the ICU.
Results
A total of 63 (70%) questionnaires were returned. The most used physiotherapy interventions were airway secretion clearance, techniques to improve lung ventilation and mobilisation out of bed. Positioning was most used respiratory technique (60/61, 98%). Sitting on the edge of bed is the most preferred physical activity for ICU patients (43/44, 98%). Exercise was routinely prescribed (50/61, 83%) although only a minority (8/50, 16%) have established exercise prescription protocols. For mechanically ventilated patients, active/active assisted exercises were most used (40/44, 91%). 12% of ICU use either Chelsea Critical Care Physical Assessment Tool or the Functional Status Score for the Intensive Care Unit as routine outcome measures.
Conclusion
Airway clearance was stated as the most used physiotherapy technique. Exercise is routinely prescribed in ICU. Validated outcome measures are only used by few.
Keywords
Introduction
The involvement of physiotherapy in the ICU has been longstanding. Physiotherapy treatments in ICU include mobilisation, positioning, percussion, vibration, manual hyperventilation, suctioning, coughing, inspiratory muscle training and bed and breathing exercises. 1 These interventions can be classified as chest physiotherapy or mobilisation therapy. 2 There is evidence that chest physiotherapy assists in the re-expansion of atelectatic lung, 3 improves aeration of the dorsal lung region, 4 improves secretion clearance and increased static compliance 5 and reduces the incidence of ventilator-associated pneumonia. 6 In patients with prolonged ICU stay (>3 days), early mobilisation therapy is recommended to prevent and manage neuromuscular complications. 7 A systematic review by Tipping et al. 8 found that early mobilisation in the ICU improved muscle strength and independent mobility, and lowered mortality and hospital readmission rate, up to 6 months follow-up.
In recent times, the ICU physiotherapy practices have been reported from USA, 9 Australia, 10 UK 11 and Europe. 12 One commonality of these national surveys is that the frequency and types of intervention varied depending on hospitals types and patient diagnosis. The specific practices of physiotherapy, level of autonomy differed between the clinicians, their clinical settings and various countries.9,10 Uniquely, in these surveys, there was no consistent outcome measure used for patients’ assessment and progress monitoring.
In Singapore, there are 671 Intensive Care Unit (ICU) beds for a population of 5.7 million. 13 As a cosmopolitan country that is highly interconnected with other parts of the world, Singapore receives professionals from all over the world come to the city state to seek job opportunities. 14 In addition to locally trained physiotherapists, physiotherapists in Singapore come from Australia and New Zealand, Ireland, United Kingdom and neighbouring countries such as Malaysia. 15 Due to different schools of thought and cultures in the various countries, this may result in varying practices among physiotherapists in Singapore. Considering the emerging ICU physiotherapy practices and increasing number of ICU beds in Singapore, it is timely to conduct a survey of ICU physiotherapy practices in Singapore. To date, there is no reported data describing the physiotherapy practices in the ICUs of Singapore. This survey serves to ascertain the current and common physiotherapy practice patterns in the adult ICUs of hospitals in Singapore.
Methodology
Aims and Objectives
This study aims to explore the various physiotherapy practice patterns across the adult ICUs of hospitals in Singapore. The objectives of this adult ICU study are to establish 1) Local critical care Physiotherapy referral criteria; 2) Training and competencies for new physiotherapists working in ICU; 3) The types and prevalence of physiotherapy techniques employed in ICU; 4) Factors used for exercise prescription and 5) Outcome measures used in critical care physiotherapy.
Research Design
A cross-sectional survey study design. Hard copy postal questionnaire was chosen because the practice of internet separation in restructured hospitals in Singapore has precluded workstations access to electronic survey through the Internet. The questionnaire composed of 29 open and close-ended questions organised in four sections: hospital information, physiotherapist information, physiotherapy management (Rehab and respiratory specific techniques) and exercise prescription.
Ethics Approval
Ethics approval was obtained from the Singapore Institute of Technology Internal Review Board on 2 May 2019 (project number 2019092).
Construction of Questionnaire
Our questionnaire was adopted and modified from Skinner et al. 10 A senior principal physiotherapist and a principal physiotherapist practicing in Singapore ICUs adapted the questionnaire to Singapore context (version 1). The version 1 questionnaire was subsequently reviewed by six other physiotherapists with minimal 10 years of ICU working experience in Singapore. Version 2 questionnaire incorporated the changes suggested by the reviewers. Thereafter, a public health nurse practitioner, who had no relation to the field of physiotherapy, was consulted to attain the face validity for the questionnaire. 16
Distribution of Questionnaires
Email invitations to participate in this study were sent to Head of physiotherapy department or service lead of critical care physiotherapy of all hospitals with ICU facility. A physiotherapist was nominated as the point of contact to ascertain the number of physiotherapists working in his/her ICUs and assist with distribution and collection of questionnaires. We aimed to survey physiotherapists currently practicing in ICU on weekdays. Physiotherapists who provided only weekend or ad-hoc on-call ICU coverage were excluded. Based on this, 90 questionnaires were distributed to the respective ICUs in May 2019.
The questionnaire package consisted of three items: a cover letter to explain the purpose of the study (Supplemental Appendix II), the questionnaire (Supplemental Appendix III) and a prepaid return envelope. Two follow-up email reminders (at one-week and three-week after the initial mail) were sent to the point-of contact physiotherapists, to request the response and return of the questionnaires to encourage higher response rates (Malone et al., 2015). Additional questionnaire packages were provided on request. No incentive was provided for the completion of the survey, and consent was implied by the return of a completed questionnaire. 17
Data Collection and Analysis
Data sets extracted from the returned questionnaires were stored and organised on Microsoft Excel and analysed using Stata 15 statistical package. Most data sets were nominal or ordinal. Where respondents were asked to rank items in order of importance, with 1 being the most important, mean ranks were calculated. For several questions, respondents were asked to select as many options as applied, thus resulting in a cumulative percentage of more than 100 for several questions.
Results
Out of 17 ICUs in Singapore, eight restructured hospital ICUs and seven private hospital ICUs (88%) participated in the study. Two hospitals did not respond to the invitation. Sixty-three questionnaires were returned with a response rate of 70%. After excluding 2 questionnaires that described the practice of paediatric ICU, the data sets of 61 questionnaires were used for this study.
Participants Demographic Data sets.

aRespondents chose more than one option.
Physiotherapy Referral Criteria
Blanket referral (48/61, 79%) was the most common process, followed by referral by attending team (29/61, 48%) and referral by protocol (9/61, 15%). Some respondents ticked two categories, so percentage does not add up to 100%.
Orientation and Competency Check
37 (61%) respondents stated the presence of ICU physiotherapy competency check, while 9 (15%) of them explained that the development of this check was underway. A compulsory orientation programme was in place in the majority (46/61, 75%), with on the job training being the most common mode of orientation (51/61, 84%).
Physiotherapy Management in Intensive Care Units
Figure 1 shows most utilised physiotherapy interventions. Most utilised physiotherapy interventions in ICU (n = 61).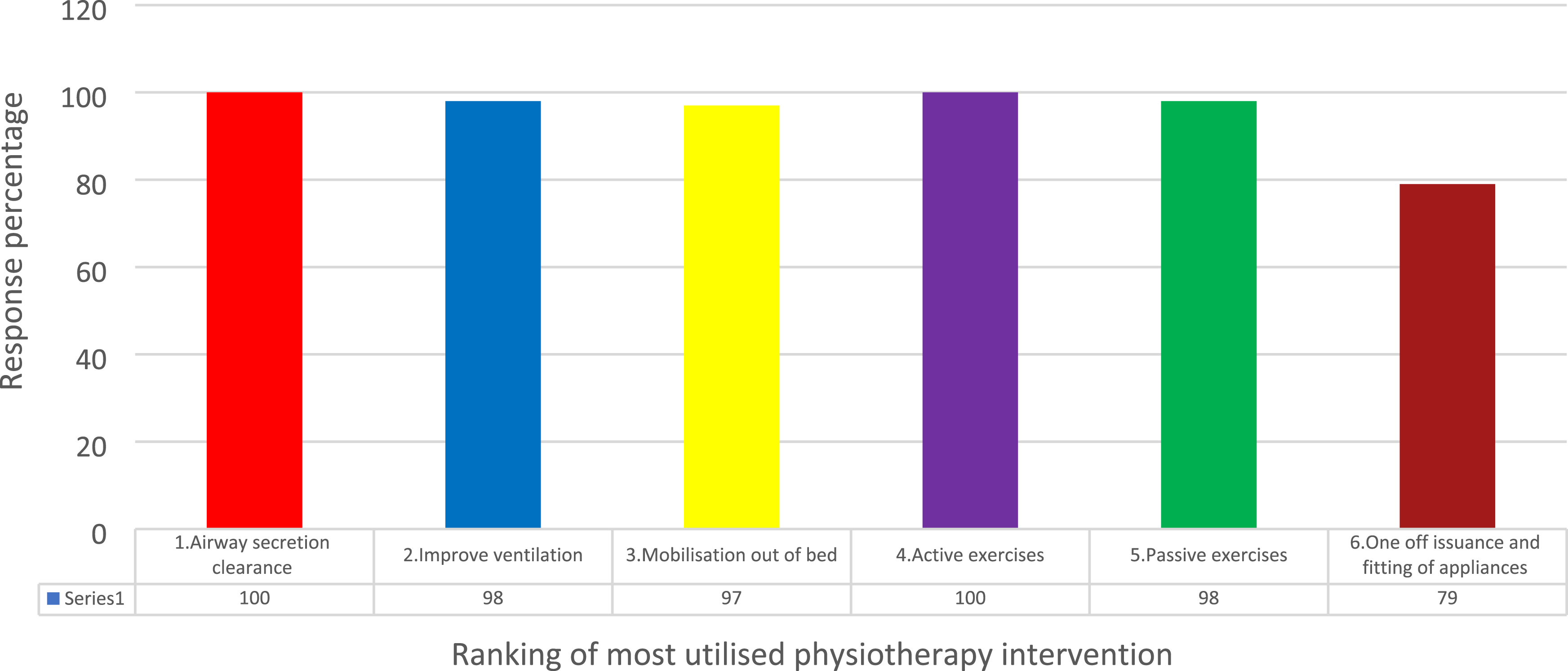
Respiratory Management in Intensive Care Units
Figure 2 shows exclusive ranking of most utilised respiratory management techniques. Most utilised respiratory management techniques in ICU (n = 61).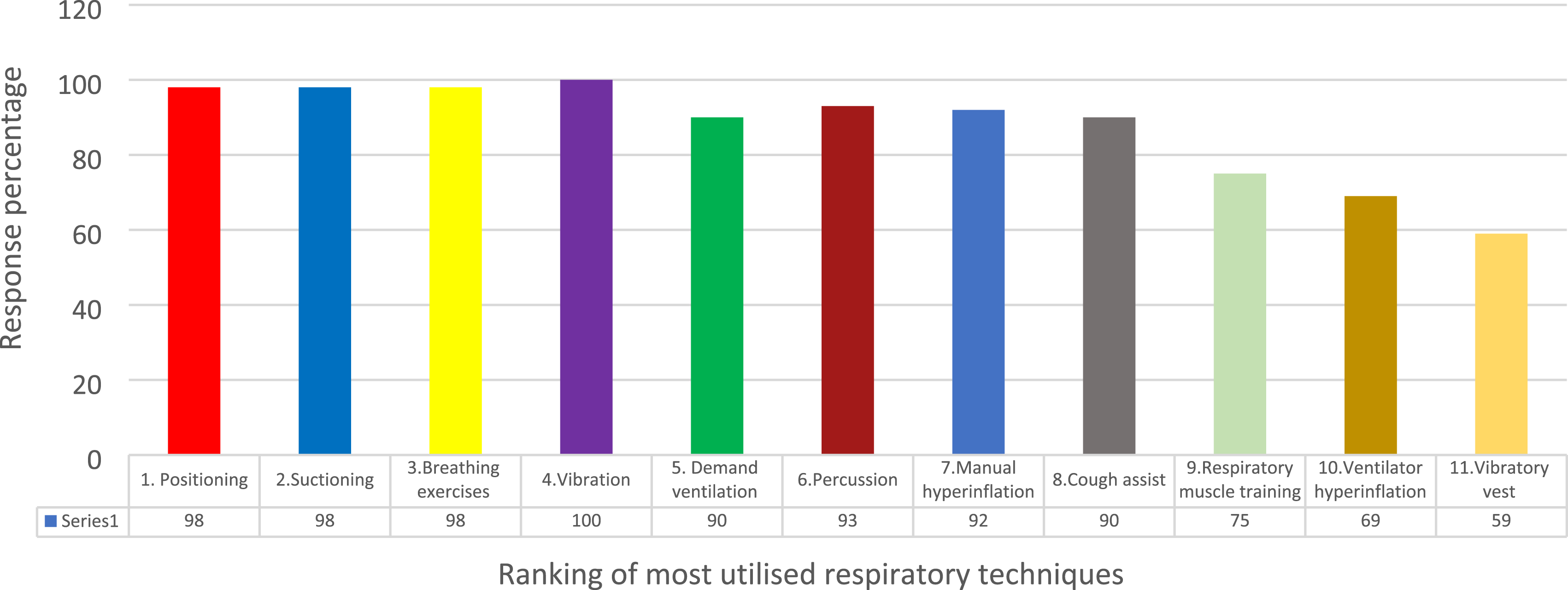
Exercise Prescription in Intensive Care Units
50/61 (83%) respondents prescribed exercise in ICU. Majority reported the absence of an exercise prescription protocol in the ICUs of their hospitals (42/50, 84%). 74% prescribed exercise for every ICU patient (37/50), while 38% (19/50) and 30% (15/50) of them considered the prescription of exercise for debilitated and long-stay patients, respectively. All the respondents attributed the responsibility of executing the exercise programme to the physiotherapists. 60% (30/50) stated that patients should carry out the exercise programme. 54% and 52% of respondents involved the families and caregivers (27/50) and therapist assistant (26/50) in the exercise programme. While majority (41/50, 82%) reported the frequency of exercise sessions to be once daily, some reported twice daily session (10/50, 20%). A small percentage of respondents reported exercises to be conducted more than twice daily (1/50, 2%) and even hourly (3/50, 6%) for patients.
The types of exercises prescribed for patients in the ICU are ranked in Figure 3. Type of exercise prescribed exercise activity in ICU (n = 44*) *Six responses were excluded as they did not rank their responses.
Contraindications to Exercise in Intensive Care Units
Circumstances when exercise would be contra-indicated include the need for inotropic support (20/50 (40%)), the diagnosis of acute respiratory distress syndrome (ARDS) (18/50 (36%)), ongoing continuous veno-venous hemofiltration (CVVH) or continuous veno-venous hemodiafiltration (CVVHDF) (15/50, 30%), the presence of Swan-Ganz catheter (15/50, 30%), being sedated (12/50, 24%), confused (9/50, 18%), had a femoral vascular catheter in situ (7/50, 14%), high ventilator settings with fraction of inspired oxygen ratio 0.6 and above (26/50, 52%) and positive end expiratory pressure of more than 10 cm H20 (27/50, 54%), abnormal laboratory results such as low haemoglobin levels less than 7.0 g/dL (21/50, 42%) and elevated troponin levels (8/50, 16%). One (2%) respondent identified the presence of mechanical ventilation as a contraindication to exercise.
Factors Used for Exercise Prescription, Progression and Monitoring in Intensive Care Units
Respondents were invited to select, out of 12 potential factors, parameters that would influence their exercise prescription, progression and monitoring in the ICU. The data sets are summarised in Figure 1. Heart rate was chosen by most as a factor that prescribes, progresses and monitors exercise response (Figure 4). Selected factors to determine patient’s initial exercise parameters, patient’s ability to progress exercise, and to monitor patient’s response to exercise. Spo2-Pulse oximeter saturation, RR-Respiratory rate, HR-Heart Rate, BP-Blood Pressure, ABG-Arterial Blood Gas.
Use of Outcome Measures in Intensive Care Units
Nineteen out of 50 physiotherapists (38%) used specific outcome measures to monitor exercise therapy in critical care setting. 12% use objective means such as SpO2 and Borg Scale while 10% used functional tests such as 5 times sit-to-stand. Standardised outcome measures such as Chelsea Critical Care Physical Assessment Tool and the Functional Status Score for the Intensive Care Unit (FSS-ICU) were used by 8% (4/50) and 4% (2/50) of respondent, respectively.
Exercise Prescription for Mechanically Ventilated Patients in Intensive Care Units
Forty-nine respondents completed this section. More than three-quarters would alter the exercises prescribed for patients on mechanical ventilation (37/49, 76%). The aims of exercise for mechanically ventilated patients are to increase endurance (45/49, 92%), function (42/49, 86%), strength (40/49, 82%) and range of motion (23/49, 47%).
The commonly prescribed exercises for mechanically ventilated patients are ranked in Figure 5. The highest ranked physical activity were active/active assisted exercises and sit on edge of bed. Most prescribed exercise activities in mechanically ventilated patients (n = 44).
Mobility Team for Mechanically Ventilated Patients in Intensive Care Units
Mobility team is present in 28% (14/50) of ICU. The physiotherapist and registered nurse were core members of ICU mobility team (14/14, 100%), while therapy assistant (12/14, 86%), respiratory therapist (10/14, 71%) and doctor (8/14, 57%) were also part of the team. Enrolled nurse (5/14, 36%) and occupational therapist (1/14, 7%) were less commonly involved.
Discussion
Our study achieved a response rate of 70% (63/90 questionnaires). This was comparable to similar postal ICU questionnaire study in Australia 10 and United Kingdom. 11 Our high response rate could be attributed to measures such as pre-notification to potential participants, follow-up with contact personnel at the respective hospitals and provision of stamped return envelopes. 18 Given the high response rate, our results are likely to be representative of the physiotherapy practices in Singapore’s ICUs. Our data sets suggest that Singapore ICU physiotherapists practice with good level of autonomy as 79% (48/61) practice blanket referral model where physiotherapists screen ICU cases and decide on physiotherapy service. All respondents ranked secretion clearance technique as the most used technique, similar to the findings in Brazilian survey study. 19 The preference for conventional chest physiotherapy was even more evident in a Nepal ICU study 20 where 54% of respondents prioritise the use of chest physiotherapy (53.8%) over therapeutic exercise (3.8%). Such preference for conventional chest physiotherapy might be attributed to its longstanding traditional use. 21 Despite the strong evidence supporting the benefits of ICU mobilisation,1,8 mobilisation out of bed was ranked the third commonly used physiotherapy intervention in the ICU, behind airway secretion clearance and improving ventilation.
The present study revealed 2 key findings about respiratory management techniques employed by critical care physiotherapists. Firstly, positioning is the most used respiratory technique. This is similar to findings by Skinner et al. 22 Secondly, despite having good evidence supporting its efficacy in weaning,23–25 respiratory muscle training was not frequently used in Singapore ICUs. Similar findings were found in Turkey. 2 Hence, we recommend that local ICUs should incorporate IMT training in their competency checklist.
Despite the lack of an exercise protocol in ICUs, most respondents (83%) prescribed exercise routinely. This is slightly lower than the 94% of Australia physiotherapists who prescribed exercise routinely at a frequency of once to twice daily. 10 The most common forms of prescribed physical activity were sit on edge of bed, active exercises and sit-to-stand, which concur with the survey study by Skinner et al. 10 Eleven participants (25%) stated that they use portable mini treadmill for their patients. The factors considered for the prescription and progression of exercise, as well as the monitoring of exercise response, were similar to the study by Skinner et al. 10 This included both objective measures such as heart rate, oxygen saturation, respiratory rate and blood pressure, as well as subjective measures such as the pain and fatigue reported by patients.
All respondents attributed the responsibility of leading the exercise programmes to physiotherapists (100%), with majority incorporating the patient (60%), and the family (54%) in the exercise programme. Only 18% of respondents involved nurses in exercise programmes, as compared to the 55% reported by Skinner et al. 10 This difference in the role of nurses and their contribution towards the exercise programme might be due to the difference in the roles and responsibilities of the nurses locally. All respondents reported routine exercise prescription for mechanically ventilated patients (100%) Our results were in line with the recommendations by Li et al. 26 that exercise was safe and effective for the rehabilitation of mechanically ventilated patients in the ICU.
Despite current research evidence supporting the effectiveness of a mobility team for the early mobilisation of patients in the ICU, 27 most respondents reported the absence of such a mobility team in their respective ICUs (72%). This might be due to lack of knowledge about the need for a mobility team. Instead, the common practice in the ICUs of Singapore is that of physiotherapists recruiting the personnel required for the mobilisation of mechanically ventilated patients on an ad-hoc basis. ICUs in Singapore should evaluate its clinical workforce and form a mobility team to support the routine practice of safe and effective mobilisation of mechanically ventilated patients. The presence of inotropes, diagnosis of ARDS, ongoing CVVH or CVVHDF, indwelling femoral catheter, as well as sedation and confusion among patients as contraindications to exercise. This was similar between the current study and study by Skinner et al. 10 Surprisingly, both studies had respondents that identified the presence of a mechanical ventilator as a contraindication to exercise (2% for current study; 5% for. 10
However, differences were noted when results of the study were compared against current research evidence and recommendations. While escalating inotropes was regarded as an absolute contraindication to exercise, 28 the patient’s reduced level of awareness and consciousness, presence of indwelling lines and attachments were regarded as relative contraindications. This disparity might be due to the limitation of the current study in the lack of distinction between absolute and relative contraindications. Furthermore, while recommendations exist, respondents might remain more conservative in their management of patients in the ICU. Few Singapore physiotherapists use standardised outcome measures for patients in the ICU (12%). Our value is much lesser in comparison to other studies (21% for 11 ; 34% for. 10 The use of standardised and validated outcome measures should be encouraged among physiotherapists in the ICUs of hospitals in Singapore.
Limitations
There are several potential limitations to the current study. The inability to obtain a mailing list of all physiotherapists working in the Singapore’s ICUs may have skewed the responses of this study. This is because questionnaire packages were posted out based on the estimated number of ICU physiotherapists working in the respective hospitals, as noted by the contact personnel at each hospital. Thus, there was uncertainty whether the questionnaire had reached out to all physiotherapists in Singapore’s critical care setting. Secondly, it was not possible to compare the results of all respondents for some questions of ranking nature in entirety as some answers were given as ticking of options rather than ranking of options. Thus, responses that were wrongly represented could not be considered for data analysis. Thirdly, the study consisted of questions that required physiotherapists to select the relevant options based on their practice in the ICU. This may not be specific unlike in the provision of case scenario questions which would enable respondents to indicate their treatment preferences in a particular clinical situation. Lastly, there exists the risk of respondent fatigue, 29 especially with a considerably longer questionnaire, which might lead to less accurate responses.
Conclusion
Amongst all the available physiotherapy management techniques, conventional airway clearance techniques remain the most used treatment for patients in the ICU. Positioning is the common respiratory technique used. Majority of physiotherapists were reported to have prescribed exercise routinely for both spontaneously breathing and mechanically ventilated patients, although no exercise protocol has yet been established. Presently, a combination of subjective and objective measures is being used to guide the prescription and progression of exercise, as well as for the monitoring of patients’ response to exercise.
Furthermore, the use of validated ICU outcome measures should be encouraged to allow for a more objective evaluation of patients in the ICU. Finally, the formation of a mobility team for the early mobilisation of mechanically ventilated patients, and the involvement of family members in the rehabilitation of patients in the ICU should be considered, to enhance the effects of exercise on patients.
Supplemental Material
sj-pdf-1-psh-10.1177_20101058211068589 – Supplemental Material for Physiotherapy Practice Pattern in the Adult Intensive Care Units of Singapore – A Multi-Centre Survey
Supplemental Material, sj-pdf-1-psh-10.1177_20101058211068589 for Physiotherapy Practice Pattern in the Adult Intensive Care Units of Singapore – A Multi-Centre Survey by Gabriel Wai Mun Ou, Marcus Jun Hui Ng, Cindy Li Whye Ng, Hwee Kuan Ong, Balachandran Jayachandran and Vimal Palanichamy in Proceedings of Singapore Healthcare
Footnotes
Author Contributions
Hwee Kuan Ong, Balachandran Jayachandran and Vimal Palanichamy researched literature, conceived the study drafted the questionnaire.
Cindy Li Whye Ng, Gabriel Wai Mun Ou, Marcus Jun Hui Ng and Vimal Palanichamy were involved in protocol development.
Gabriel Wai Mun Ou and Marcus Jun Hui Ng gaining ethical approval, patient recruitment, data analysis and wrote the first draft of the manuscript.
All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval (include full name of committee approving the research and if available mention reference number of that approval) Ethical approval for this study was obtained from Singapore Institute of Technology review board 2019092.
Informed Consent
Informed consent was not sought for the present study because *Implied consultant as it is a survey*.
Availability of Data
The datasets generated and/or analysed during the current study are available from corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.