
Abstract
Background
Patient safety is of paramount importance in healthcare delivery. This is especially so in the high-risk and complex environment of the operating theatre.
Objectives
The purpose of this narrative review is to illustrate the risks that patients are exposed to in the operating theatre and the measures in place to mitigate preventable harn, including the nationwide Ensure Safer Systems programme.
Methods
A literature search was conducted utilising sources such as PubMed, Scopus, Cochrane Library, Google Scholar and Web of Science between 2010 and 2024. ‘Patient safety’, ‘surgical safety’, ‘operating theatre’, ‘operating room’ and ‘systems approach’ were combined using Boolean operators. Selected guidelines and position statements from professional medical societies and government websites were also reviewed.
Results
This narrative review is informed by the analysis of qualitative and quantitative articles from the literature review. While there are numerous interventions addressing patient safety, many of these efforts target specific harms. In order to make a significant impact, it is crucial to adopt a systems approach that underpins these initiatives. Although the Ensure Safer Systems programme is a hospital-wide initiative, its scrutiny and oversight of operating theatre processes enhances patient safety in the operating theatre.
Conclusions
The establishment of a safety system comprising strong leadership commitment, safety culture and robust process improvement is vital to achieving sustained improvement in patient safety.
Introduction
The guiding principle of “primum non nocere” in medicine has been strengthened by the development of the field of patient safety. The impetus for this was largely due to the publication of the report To Err is Human by the United States Institute of Medicine (IOM), which revealed how almost 100,000 people die from medical errors alone each year. 1 More importantly, it identified challenges that needed to be tackled, such as an over-emphasis on individual accountability, insufficient attention to systemic factors and a fragmented approach to patient safety. This has galvanised the development of patient safety into a discipline, driving an increase in research, funding and interventions to address medical errors. 2
Given that a significant portion of patient care occurs within the operating theatre (OT), ensuring patient safety in this high-risk environment is paramount. The OT presents unique challenges, as it involves multi-disciplinary teams, complex procedures, technological integration, and human factors that must work seamlessly to prevent errors. The aim of this narrative review is to illustrate the risks that patients’ are exposed to in the OT, the factors that may contribute to these risks, and the measures in place to mitigate preventable risks. It also explores the Ensure Safer Systems (ESS) programme and its adoption as a systems-based approach in improving patient safety. Given the breadth and complexity of this topic, a narrative review approach was chosen. It is hoped that this information will be useful to non-OT healthcare practitioners as well, eventually translating to greater public awareness of this aspect of healthcare.
Critical patient safety processes in the OT
Ensuring patient safety in the OT requires multiple issues to be addressed even before the patient arrives there. This includes obtaining informed consent for both surgery and anaesthesia, achieving appropriate fasting duration, reviewing the patient’s medical issues, medications and investigations, and obtaining necessary blood products if required. Concurrently, the OT has to be ready with the appropriate equipment, medical implants, and healthcare workers of different skill sets that are specific to that particular surgery. Perhaps unbeknownst to the public, these medical and nursing staff are credentialed by the healthcare organisation (and the Ministry of Health (MOH) Singapore through their respective medical and nursing boards) so that patients are cared for by qualified professionals.
On arrival to the OT reception area, another series of checks are performed. This includes patient verification with two patient identifiers, confirming and annotating the surgical site, and verifying allergies and fasting status. Additional precaution is required for patients with limited capacity or reduced consciousness.
A team huddle is conducted to ensure that every member is cognizant of the exact surgery being performed, anticipated complications, estimated duration, special equipment and implants required, antibiotic prophylaxis and need for blood products. This is also an opportunity for any team member to clarify uncertainties or raise concerns regarding any aspect of patient care. 3
After induction of anaesthesia, a final time-out is performed just prior to skin incision. This pause serves as the final confirmation by the surgical team that the correct patient is present for the correct surgery, on the correct site, using correct equipment and imaging, and where required, that prophylactic antibiotics have been administered. 4 Although the process can be laborious, one can appreciate that despite all the checks ensuring the correct operative site, a simple mistake such as placing the sterile drape over the wrong eye or a tourniquet on the wrong limb may still result in a wrong site surgery. Hence this final pause allows for a final check before surgical incision.
Under anaesthesia, appropriate continuous monitoring of the patient’s physiological parameters is performed, adhering to safety guidelines from international anaesthesia societies. 5 This may include blood pressure, heart rate, oxygen saturation, electrocardiography, gas concentrations, processed electroencephalography, neuromuscular monitoring and temperature as required. These monitors incorporate alarm systems to alert the anaesthetist to any deviations from normal physiology while keeping the patient appropriately anaesthetised.
At the completion of the surgery, a sign-out process verifies the actual procedure performed, identifies any complications encountered, ensures all surgical items have been accounted for, verifies that specimens obtained are correctly labelled and dispatched, and establishes a clear post-operative plan. 3
History and evolution of patient safety in the OT
The concept of the OT first emerged in the late 18th century, primarily as a space for the demonstration and teaching of surgical techniques. 6 Hence, the early OTs featured large amphitheatre-style theatres with a stage-like setup for colleagues and students to observe surgery from tiered seating, albeit with poor infection control. 6
The 19th century marked a transformative period, with the introduction of ether and chloroform in 1846. This enabled longer and more complex surgeries to be performed, but also introduced new challenges such as airway management and the risk of overdose. 7 Concurrently, Louis Pasteur’s germ theory of disease laid the groundwork for the development of aseptic techniques. 8 This led to a slew of aseptic techniques in this century, including the use of anti-septics in surgery, sterilisation of surgical instruments, use of surgical gloves, and a growing emphasis on hand hygiene - all of which remain foundational elements of modern infection control.9,10
The early to mid-20th century was marked by significant advancements in both anaesthesia and surgery that improved patient safety. The development of safer anaesthetic agents such as cyclopropane and halothane, along with the introduction of endotracheal intubation and monitoring equipment, enhanced intraoperative care. 11 Additionally, the establishment of intensive care units and post-anaesthesia care units revolutionised post-operative monitoring and management. 12 The discovery and widespread use of penicillin and other antibiotics substantially reduced post-operative infections. 13 Finally, the advent of minimally invasive surgical techniques further reduced surgical trauma, infection rates, and recovery times, collectively enhancing patient safety. 14
The late 20th century marked the formalisation of patient safety as a discipline. Organisations dedicated to the improvement of perioperative patient safety, such as the Anesthesia Patient Safety Foundation (APSF), were established. Intraoperative monitoring became more stringent, with the American Society of Anesthesiologists (ASA) setting minimum monitoring requirements for patients under anaesthesia. The ASA also pioneered the first large scale audit of adverse events in the OT with its Closed Claims Project database. 15 Perhaps most influentially, the Institute of Medicine’s (IOM) landmark report, To Err is Human, highlighted the staggering number of preventable deaths caused by medical errors, and advocated for a systems-based approach to patient safety, including within the OT. 1
In the 21st century, patient safety has continued to evolve through a systems-based approach and technological advancements. The introduction of the World Health Organization’s Surgical Safety Checklist has been associated with significant reductions in surgical complications and mortality. 3 Increasing emphasis has also been placed on human factors and non-technical skills such as teamwork and communication. 2 The digital transformation of healthcare, characterised by the adoption of electronic medical records (EMR) and real-time data analytics, has enhanced the auditing of clinical practice and enabled more effective monitoring of patient safety metrics. 16
Methodology
Data sources and search strategy
To identify relevant literature on patient safety in the operating theatre, a search was conducted across multiple databases including PubMed, Scopus, Cochrane Library, Google Scholar, and Web of Science from 2010 to 2024, although seminal papers were also included where relevant. The keywords used were: patient safety, surgical safety, anaesthesia/anesthesia safety, operating theatre, operating room, and systems approach. Boolean operators were used to refine the results.
In addition to peer-reviewed literature, selected guidelines and position statements from professional medical societies and government health authorities were also reviewed, including the WHO, the Association of Anaesthetists (AoA), the Australian and New Zealand College of Anaesthetists (ANZCA), and MOH.
Study selection and screening
Titles and abstracts were independently screened by two authors. Full-text review was performed to assess relevance to the review topic, with discrepancies resolved by consensus discussion. Inclusion criteria included peer-reviewed studies, systematic reviews, and clinical guidelines published in English that discussed safety interventions, errors and risks management in the operating theatre. Studies were excluded if they focused primarily on non-operative settings or lacked specific relevance to perioperative patient safety. Reference lists of selected articles were manually screened to identify additional studies that could be relevant.
Information extraction and synthesis
A narrative synthesis of the data was conducted, with findings organised into key thematic areas to provide a comprehensive understanding of the topic. These included risks to patients in the OT, factors contributing to these risks, mitigation strategies, and systems-level initiatives such as the ESS programme.
Results
Risks to patients in the OT
Risks to patients in the operating theatre.
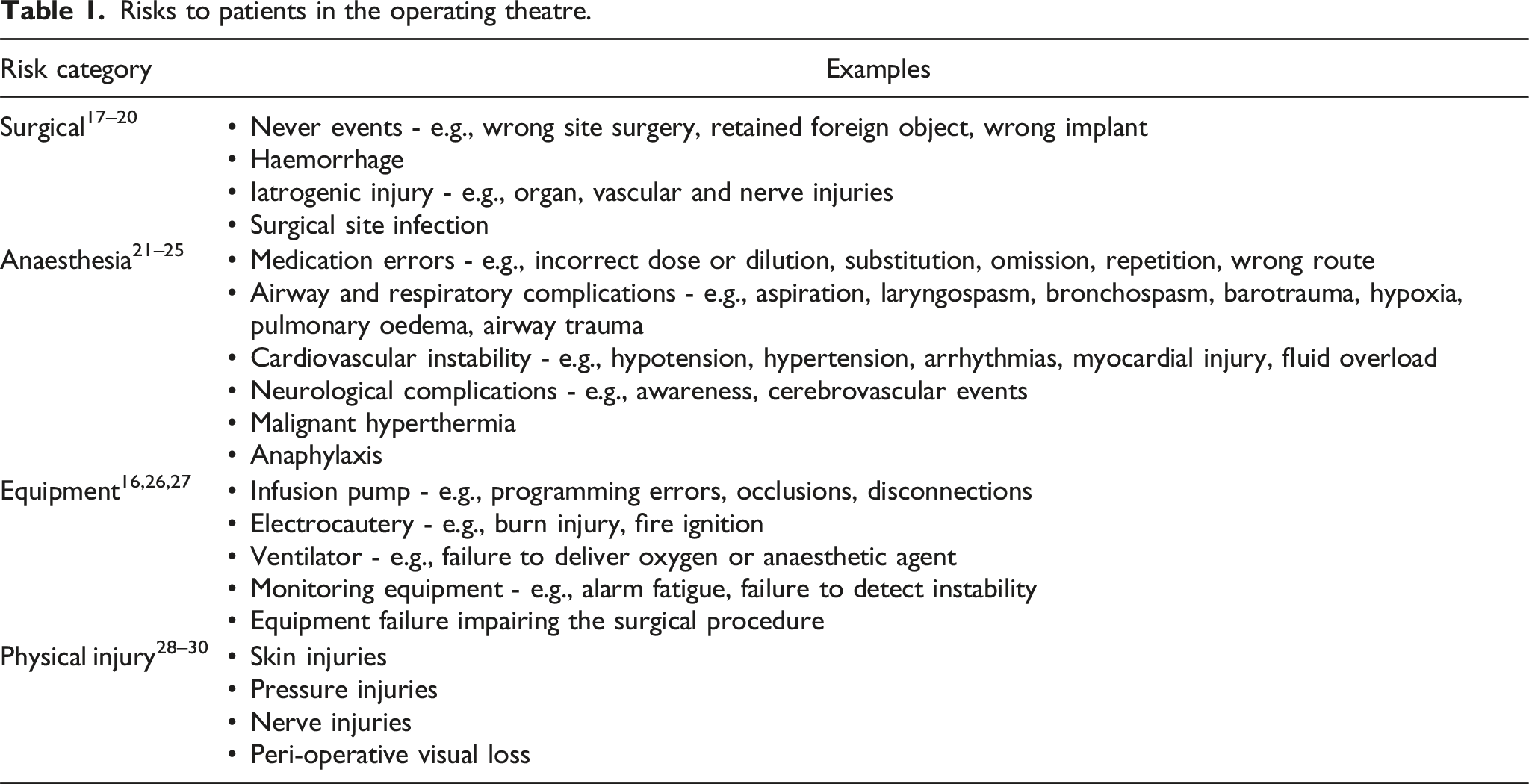
Surgical risks
Never events
The term ‘never events’ was first introduced by the National Quality Forum in 2001. It refers to medical errors with serious consequences for the patient that are entirely preventable and should never occur. Hence, such events are also regarded as sentinel events by the Joint Commission International (JCI), as they can be indicative of significant safety problems in the organisation. 17 Additionally, they can incur considerable financial and medicolegal costs for the institution.
It is estimated that never events occur at a rate of 1 in 12,000 to 22,000 procedures.17–20 This includes operating on the wrong patient or procedure (35%), performing the procedure or regional anaesthesia block on the wrong side or site of the patient (30%), having a retained foreign object (28%), and using a wrong implant (7%). 20 Retained foreign objects are usually surgical items such as sponges, gauzes, needles and guidewires that can be inadvertently left inside the patient at the completion of a procedure, potentially requiring additional procedures to extricate these foreign bodies. 18
Anaesthesia risks
Perioperative medication errors
Medication administration in the OT is unique as it bypasses the usual safety checks in place, such as pharmacists, nurses and electronic clinical decision tools. Instead, a single clinician may be solely responsible for everything from medication verification, preparation, administration, documentation and monitoring. Consequently, it is not surprising that perioperative medication errors continue to account for one of the most common critical incidents in anaesthesia. 21 The most common medication errors were incorrect dose (29%), substitution (28%), omission (7%), repetition (5%) and incorrect drug (5%), which includes the inadvertent administration of a drug to which the patient has a known allergy. 22
Incorrect drug administration due to misreading of vials or syringe swaps remains a pertinent problem with potentially life-threatening consequences, such as the inadvertent administration of a muscle relaxant instead of a sedative to an awake patient. 23 Medication mishaps also include extravasation errors during infusions of fluid or medication. Not only does the administered medication fail to be delivered, the inadvertent subcutaneous administration of the medication may also potentially cause significant tissue injury. 21
Equipment and physical injury risks
Equipment such as infusion pumps for drug delivery may be wrongly programmed or accidentally disconnected, resulting in failure of drug delivery to the patient. 21 This is particularly significant if it involves vasoactive agents or anaesthetic agents that render anaesthesia. Electrocautery equipment can also cause thermal injuries to the patient with improper grounding pad placement, and may even ignite OT fires when used near flammable materials such as alcohol-based antiseptic solutions. 27
Improper positioning and inadequate protection measures can lead to significant physical injuries such as skin and pressure injuries, nerve injuries and even perioperative visual loss.28,29 There have also been reports of patients falling off the operating table due to inadequate securing of the patient with safety straps. 30
Factors contributing to patient risks
The unique OT environment is potentially hazardous for several reasons. Patients eventually lose capacity to look out for themselves under anaesthesia. The highly specialised members that make up the OT team have different job scopes and may not always appreciate the challenges of one another. A single OT list may also have different surgical teams treating different patients, which requires even more vigilance by healthcare staff. Additionally, the constant pressure to deliver efficiency in a high-stakes environment can compromise patient safety in the OT. A systematic review of in-hospital adverse events found that the majority of such events (41%) occurred in the OT, as compared to only 26% in the ward setting. 31
Factors contributing to patient risks in the OT and their mitigation strategies.

Distractions
Distractions and interruptions to the OT team have been found to occur as frequently as 11 to 12 times every hour. 37 These include phone calls, social conversations, alarms, and the constant traffic of people entering and leaving the OT. Such high frequency of disruptions can result in impaired team communication and concentration, lapses in monitoring, delayed responses to deteriorations in the patient’s condition, and contribute to errors in medication administration or procedural steps. 35
Communication failure
Communication failure remains one of the most common causes of medical errors, especially in the multidisciplinary environment of the operating theatre.31,32,34–36 Communication failures can arise from inappropriate timing, incomplete information, absence of key personnel, and unresolved issues. 32 Each of these lapses can disrupt team cohesion, delay critical decisions, and increase the likelihood of preventable errors, ultimately compromising patient safety.
Understaffing
Having adequate and competent medical staff is fundamental to quality care, with evidence that both the quality and quantity of staff improve patient safety. 38 This problem was recently exacerbated by the coronavirus disease, with an increased number of public healthcare workers resigning during the pandemic, leading to an increased workload for the remaining healthcare workers. 39 While new medical staff can be hired, the high turnover translates to reduced experience and familiarity regarding specific workflows, procedures, and protocols that are critical for maintaining patient safety in the OT environment.
Fatigue and burnout
The pressure of working in a high-stakes environment such as the OT places healthcare workers at a higher risk of fatigue and burnout. This is often aggravated by other factors including understaffing problems, increased night shifts and administrative responsibilities. Fatigue and burnout have been associated with reduced cognitive function and situational awareness, poorer communication and teamwork, and decreased compliance with safety protocols. 40 Consequently, this leads to an increased incidence of medical errors and undermines patient safety.
Mitigation strategies addressing contributory factors
The mitigation strategies outlined in Table 2 can be applied to enhance overall patient safety in the OT, as outlined below. They include specific strategies that have also been recommended by several society guidelines, including the AoA, ANZCA, and the APSF.63,66,72
Human factors
Ensuring that OT personnel are adequately trained and assessed is critical to minimising errors in decision-making, procedural execution, and crisis response. Simulation training that focuses on managing crisis situations, such as an unexpected difficult airway, anaphylaxis, or intraoperative haemorrhage, is crucial in improving clinical decision-making under pressure.41,42 Physical and mental exhaustion, which contribute substantially to errors in the OT, can be mitigated through duty hour restrictions, access to mental health support services, and cultivating a supportive workplace culture.40,41,43,73
Task factors
Pre-operative briefings align team members on patient risks and ensure that emergency resources such as blood products or surgical equipment for contingencies are readily available. 45 Crisis manuals with visual aids illustrating the correct dose, preparation and administration of critical medications (e.g., adrenaline, dantrolene and intralipid) are readily available in the OT. The use of pre-packed emergency kits (e.g., front-of-neck access kits and malignant hyperthermia box) further streamlines crisis management. 47
Technology factors
User-centered design of equipment such as ventilators and infusion pumps can avoid overly complex interfaces that may lead to errors.49–51 Additionally, having a trial period with end-user feedback prior to equipment procurement is equally important. To address system fragmentation, integrated EMR systems enable comprehensive access to a patient’s medical history, a consolidated medication administration record, and intraoperative events. This reduces the risk of missed or duplicate interventions such as prophylactic antibiotic administration. 16 Routine equipment maintenance and pre-operative safety checks identify potential failures pre-emptively, while backup equipment and protocols allow for continuity in the event of failure.
Team factors
Communication failure in the OT accounts for a large proportion of surgical errors, delays in care, and compromised patient outcomes.34–36 Pre-operative team huddles and checklists, such as during the pre-operative sign in, reduce adverse outcomes such as never events, and ensure timely administration of critical interventions such as antibiotics.3,74 Training staff in the use of communication tools and structured handover frameworks ensure concise communication of patient information, particularly during the transfer of patient care from one anaesthesia team to another, or when patients are transferred from the ward to the OT and vice versa.53–56
Supervision factors
Clear supervisory responsibilities with feedback mechanisms and performance reviews enhances oversight, which supports a training environment that is safe for both patients and trainees in the OT.57,60 Additionally, leadership and mentoring training equip supervisors with the necessary skills to guide, support, and empower their trainees.58,59
Environmental factors
During critical phases of surgery such as timeout and induction, distractions are minimised by limiting non-essential conversations and noise.61,65 Surgical instruments, and consumables are arranged in an ergonomic and logical manner to facilitate easy access. 64 Medication trays in the anaesthesia workstation also incorporate color-coded labeling and clear differentiation of look-alike vials to prevent errors.63,66
Organisational factors
An anonymous and non-punitive reporting system increases the reporting rates of errors and near-misses, which help identify latent safety threats in the OT.68,69 The leadership must also demonstrate a visible commitment to safety by supporting quality improvement initiatives and engaging stakeholders. 58 In addition, the well-being of staff must be ensured by providing adequate training, fostering a supportive work culture, and a balanced workload to prevent fatigue and burnout.70,71
Discussion
One and a half decades after the report by the IOM, the National Patient Safety Foundation (NPSF) assessed the progress that had been made on patient safety. 75 It found that a broader approach to patient safety initiatives led to greater success, prompting their advocacy for a systems approach to patient safety that underpins other improvement initiatives. This was in contrast to the traditional clinician-centered approach to patient safety, where the individual clinician was often held solely responsible for any errors or harm befalling the patient.69,76 This approach detracts from addressing the underlying systemic factors that may have predisposed to the error, leaving the system and other healthcare colleagues susceptible to similar errors in the future.
A systems approach to patient safety
A systems approach involves identifying error-prone elements of the environment and addressing them by optimising work processes, guided by human factors. 77 This approach has a longstanding and well-documented history of success in various high-risk industries, including aviation and nuclear power. 78 The benefit of a systems approach is illustrated by Heinrich’s safety pyramid. 79 In the healthcare context, it suggests that for every serious reportable event, there are many more adverse events with minor injuries, and a significantly larger number of near-misses and unsafe acts. Hence, adopting a systems approach to errors addresses the entire pyramid, in contrast to a clinician-centered approach which merely targets the apex.
Surgical Safety Checklist
One of the most well-known initiatives utilising a systems approach to reduce the incidence of adverse events in the OT is the surgical safety checklist. Introduced in 2008 by the WHO, it aims to improve patient safety by facilitating better communication and teamwork within the OT. 80 Its practical characteristics have driven its widespread adoption, which include being relatively inexpensive, ease of implementation and adaptability to the local context. Importantly, implementation of the surgical safety checklist has been associated with a reduction in perioperative mortality and complications. 3 The mechanism for this is likely multi-factorial, including a formal pause for briefings, improved safety attitudes, enhanced team communication and better adherence to critical tasks such as verification of the right patient, surgery and site. 81
Systems approach with the ensure safer systems program
In 2021, MOH implemented ESS, a 5-year programme which was jointly developed by MOH, JCI, and the Joint Commission Center for Transforming Healthcare. ESS is based on JCI standards but adapted to the local Singapore context, with the aim of achieving a state of high reliability with the goal of zero harm events of any kind.
82
This is achieved by incorporating the three pillars of the ESS into the healthcare organisation: leadership commitment, a strong safety culture and robust process improvement.
58
(Figure 1) The Ensure Safer System’s framework for achieving high reliability in healthcare.
Leadership
Building a safer and sustainable system requires full leadership commitment towards the goal of zero patient harm. Such a goal translates into an organisational ethos of always striving to improve the current level of safety, with the success of all subsequent changes contingent upon this. Clearly defined safety goals are incorporated into organisational objectives and are well-communicated. There are regular reviews of safety systems, reports on safety improvement initiatives and leadership walkabouts of the OT environment. Walkabouts have been shown to identify latent errors not picked up through conventional methods of error detection such as incident reports. 83 Examples include identifying hazardous layouts of the workplace, look-alike ampoules before a medication error occurs, or inadequate resuscitative equipment in remote OT environments around the hospital.
Leadership commitment extends to resource allocation that supports patient safety efforts such as staffing, equipment and training, ensuring that safety initiatives are not only implemented but sustainable over time. 84 Additionally, resources are also provided for quality improvement initiatives and root cause analysis of errors, as these help to drive the adoption of best practices throughout the OT. By investing in these areas, the leadership demonstrates a tangible commitment to fostering a safe and supportive environment for both patients and healthcare providers.
Safety culture
A safety culture permeates the safety ecosystem and is defined by the conglomerate of attitudes, values and beliefs held by an organisation’s members in relation to patient safety. 85 This influences the behaviours and priorities of healthcare workers when executing their job responsibilities, and may lead to improved error reporting, reduced adverse events and thus, better patient outcomes.
To encourage the accurate reporting of errors in the OT, any reporting is done anonymously and without fear of reprisal or punitive behaviour. 68 Additionally, the reporting of near misses is encouraged, as it provides a valuable opportunity to identify situations where a potential error could have occurred but was averted, and to address the underlying systemic factors to prevent similar incidents in future.69,70 When trust, reporting and improvement function effectively, these three elements of a safety culture support high reliability within the OT. 58
Other interventions that have been shown to promote a safety culture include team training to improve communication and mutual support. 68 This is important because of workplace hierarchy, which remains ingrained in medicine. 52 The unequal power relationship between trainees and consultants or scrub nurses and surgeons can lead to a fear of raising concerns, the suppression of which is at the expense of patient safety. Examples of such concerns may include discrepancies in the surgical consent and site marking, or ensuring that all members of the team stop what they are doing to actively participate in the team huddle, time-out and sign-out processes.
Locally, initiatives that have been implemented to tackle this include the TeamSPEAK programme, which empowers OT staff to speak up on safety issues through respectful and assertive communication strategies. 86 This was adapted from the Team Strategies and Tools to Enhance Performance and Patient Safety programme, which aims to improve teamwork through its four components of communication, team leadership, situation monitoring and mutual support. 53
Robust process improvement
The third key component of ESS is robust process improvement, which aims to streamline workflows, reduce errors and improve overall patient care.58,82 This is achieved by applying a structured problem-solving approach to identify root causes of issues in the workplace, and introducing solutions backed by data. This can be seen with initiation of quality improvement projects, morbidity and mortality reviews, and root cause analyses (RCA) of errors.
Quality improvement projects involve a multi-disciplinary team of stakeholders working towards a common goal with measurable outcomes. 87 Problems are analysed to their root causes and prioritized using a Pareto chart. Solutions are brainstormed and categorised based on impact and feasibility, then tested and evaluated with a run chart. Successful solutions are scaled up and integrated into workflows for sustainable change. This has been applied to improve a variety of OT processes, including reducing surgical site infections, medication errors, enhancing efficiency, and increasing patient satisfaction.
RCA and morbidity and mortality reviews are conducted regularly at both department and institutional levels. Quality Assurance Committees (QAC) identify systemic factors and implement corrective measures to enhance safety, with the impact of these changes monitored closely to ensure effectiveness. For serious reportable events such as never or sentinel events, dedicated QACs conduct RCAs and report their findings to the MOH. 88 Progress reports regarding the implementation status of recommendations are also reviewed by the hospital and MOH regularly to ensure effective implementation.
ESS journey
Prior to the implementation of ESS, Singapore’s healthcare institutions primarily pursued external accreditation, most notably from JCI.
89
While JCI is one of the most recognised benchmarks for patient safety and quality standards, it was largely externally driven and periodic in nature. ESS builds upon this foundation by introducing a more dynamic, locally-led approach that emphasises continuous improvement, real-time monitoring, and proactive risk mitigation. The five key areas that ESS aims to transform and enhance are detailed below.
89
(1) From compliance with standards to a culture of continuous improvement Previously, compliance to predefined accreditation standards could inadvertently foster complacency once targets were met. ESS shifts this focus towards a commitment and culture of perpetual safety and quality improvement. (2) From high-stakes, episodic assessments to continuous formative assessments JCI accreditation assessments were conducted periodically, with the potential for standards to lapse between evaluation periods. ESS replaces this with continuous formative assessments, ensuring that patient safety and healthcare quality are perpetually monitored and improved. (3) From reliance on external experts to being conducted by local leaders Prior to ESS, local healthcare institutions relied on external evaluators to evaluate their safety standards. Conversely, ESS empowers local leaders, trained and coached by JCI consultants, to independently assess and cultivate a safety culture that is tailored to their specific institutional context. (4) From manual data collection and analysis to a digital platform Previously, data collection was manual and resource-intensive, limiting real-time insights into patient safety issues. In contrast, ESS employs an integrated digital platform (Tracers with Accreditation Manager Plus) that automates data capture, analysis, and reporting. This digital integration allows hospitals to proactively identify and address safety concerns promptly. (5) From the goal of JCI Gold Seal to one of “Zero Harm” Before ESS, obtaining the JCI Gold Seal, while prestigious, was often perceived as an endpoint of patient safety efforts, potentially limiting continued improvement beyond accreditation. ESS redefines this approach by adopting the more ambitious and enduring goal of eliminating preventable patient harm. This encourages sustained vigilance and continuous improvement of patient safety practices.
Challenges and lessons from ESS implementation
The implementation of the ESS program in Singapore’s healthcare institutions presented several challenges with lessons learnt during this transformative process. Firstly, transitioning from a compliance-based approach to a culture of continuous improvement required a significant shift in mindset. 89 Many healthcare professionals were accustomed to meeting predefined accreditation standards, and fostering a mindset of ongoing, proactive safety enhancement required training and engagement. Secondly, encouraging open communication and collaboration across multiple levels of the healthcare organisation was another key challenge that was vital for the successful adoption of ESS. 89 Finally, upgrading infrastructure and integrating information technology systems to support ESS initiatives required overcoming logistical and technical barriers.
Despite these challenges, several valuable lessons emerged from the ESS implementation. 89 Strong leadership and commitment from each hospital’s executive leaders were crucial in ensuring sustained engagement across all levels of staff. Effective change management strategies were vital in helping staff navigate the transition, with structured training and resources mitigating resistance to new processes. Stakeholder engagement and collaboration proved instrumental in fostering a sense of ownership. Lastly, encouraging ground-up initiatives empowered healthcare institutions to develop localised solutions tailored to their specific challenges, resulting in more targeted and sustainable improvements. On the ground level, translatable improvements to patient safety as a result of one ESS survey included improvements in patient checklists and surgical site-markings, safer monitoring standards for patients undergoing procedural sedation, and better storage organisation of high-risk drugs in the OT.
Limitations and future directions of ESS
Despite its multiple benefits, the ESS has several limitations. Continuous formative assessments and improvement, while ideal, can lead to assessment fatigue, initiative overload, and burnout among healthcare staff. Rapid changes in protocols and safety initiatives can make it difficult to keep up with evolving standards, potentially leading to confusion, inconsistent adherence and disengagement. Another limitation is the amount of resources required to drive ESS, with significant manpower and financial support required for digital integration and process improvement initiatives. Hence, it may not be easily adopted by institutions operating with resource constraints and staffing shortages.
Artificial intelligence (AI) is emerging as a valuable asset in many areas of healthcare. There are many applications of AI relevant to ESS, including enhanced data analytics, risk detection, automation, and real-time clinical decision support systems, ultimately improving efficiency and patient safety around the OT and hospital. 16 Hence, incorporating AI into ESS will drive greater transformation in the healthcare system, delivering efficiency and high reliability.
Implications for practice
The findings of this review highlight the importance of a systems-based approach to patient safety in the OT, underpinned by leadership commitment, safety culture and process improvement. Focusing solely on human behaviour tends to yield only short-term improvements. In contrast, adopting a systemic approach that involves tackling contributory factors across multiple levels strengthens defenses, reduces latent vulnerabilities, and creates an environment that enhances human performance. 32 Ultimately, this achieves a more sustainable, effective, and comprehensive improvement in patient safety.
Strengths and limitations
A key strength of this review is its broad scope, which integrates historical developments, risk factors, mitigation strategies, and systemic safety initiatives, including the ESS programme. The findings were also synthesised from diverse sources, including peer-reviewed literature, institutional guidelines, and international safety frameworks in order to provide a holistic understanding of patient safety in the OT.
This review only covered studies published in the English language, which may miss relevant literature published in other languages. Also, while ESS is grounded in evidence-based safety principles, it remains in its early stages of implementation. locally While it is evident from personal communications that institutional awareness about patient safety has significantly increased since the introduction of ESS, there is currently limited data regarding its long-term effectiveness in improving patient safety and clinical outcomes. Ongoing evaluations and longitudinal studies will be necessary to assess its sustained impact and refine its strategies.
Conclusion
Patient safety should be of paramount importance to every healthcare worker, particularly in the OT where patients are at their most vulnerable. Due to human fallibility, individual vigilance is often insufficient at preventing errors in the complex environment of the OT. Instead, a broader systems approach that underpins improvement initiatives is necessary. Critical components of such a system should include resolute leadership commitment, a strong safety culture and robust process improvement. Only by doing so can a sustained improvement in patient safety be achieved.
Footnotes
Author contributions
All authors contributed equally to the conception, research, and writing of this manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript. All authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.