
Abstract
Background
Medication errors (MEs) can lead to adverse effects and mortality, especially in older adults, due to physiological changes and accumulated multi-morbidities associated with ageing. Hence, interventions to reduce MEs among older adults are important and examining their effects will provide us with the impetus to improve upon current local measures to further reduce MEs.
Objectives
To review the effectiveness of the interventions that have been implemented locally to reduce MEs.
Methods
Using chosen keywords, searches were conducted in Pubmed and Google scholar. Based on their abstract, relevant articles were chosen from all retrieved articles that were published in English. Relevant online resources and other journal articles referenced in the chosen articles were also referenced in writing this narrative review.
Results and Conclusion
Although MEs occur globally, studies examining the prevalence of MEs within Asia are lacking and the impact of various local interventions to reduce MEs is also poorly understood. Electronic prescribing, a national electronic health records repository, education in geriatric pharmacotherapy, a more centralised pharmacist’s role and the use of prescribing assessment tools are local interventions whose effectiveness in reducing MEs are supported, instead, by overseas studies examining such similar interventions. Locally, more studies are needed to examine the effectiveness of interventions in reducing MEs in various settings.
Introduction
A medication error (ME) is defined as a failure in the treatment process that leads to, or has the potential to lead to, harm to the patient. Often preventable, MEs can occur anywhere along the medication use process which includes prescription, transcription, dispensation, or administration while in the control of the healthcare professional, patient or consumer.1,2 These errors can lead to drug-drug interactions (DDIs), drug-disease interactions, adverse drugs events (ADEs) and inappropriate dosing in older patients. MEs in older adults, 65 years and above, can have a significant clinical impact on them, especially when these errors are undetected. 3
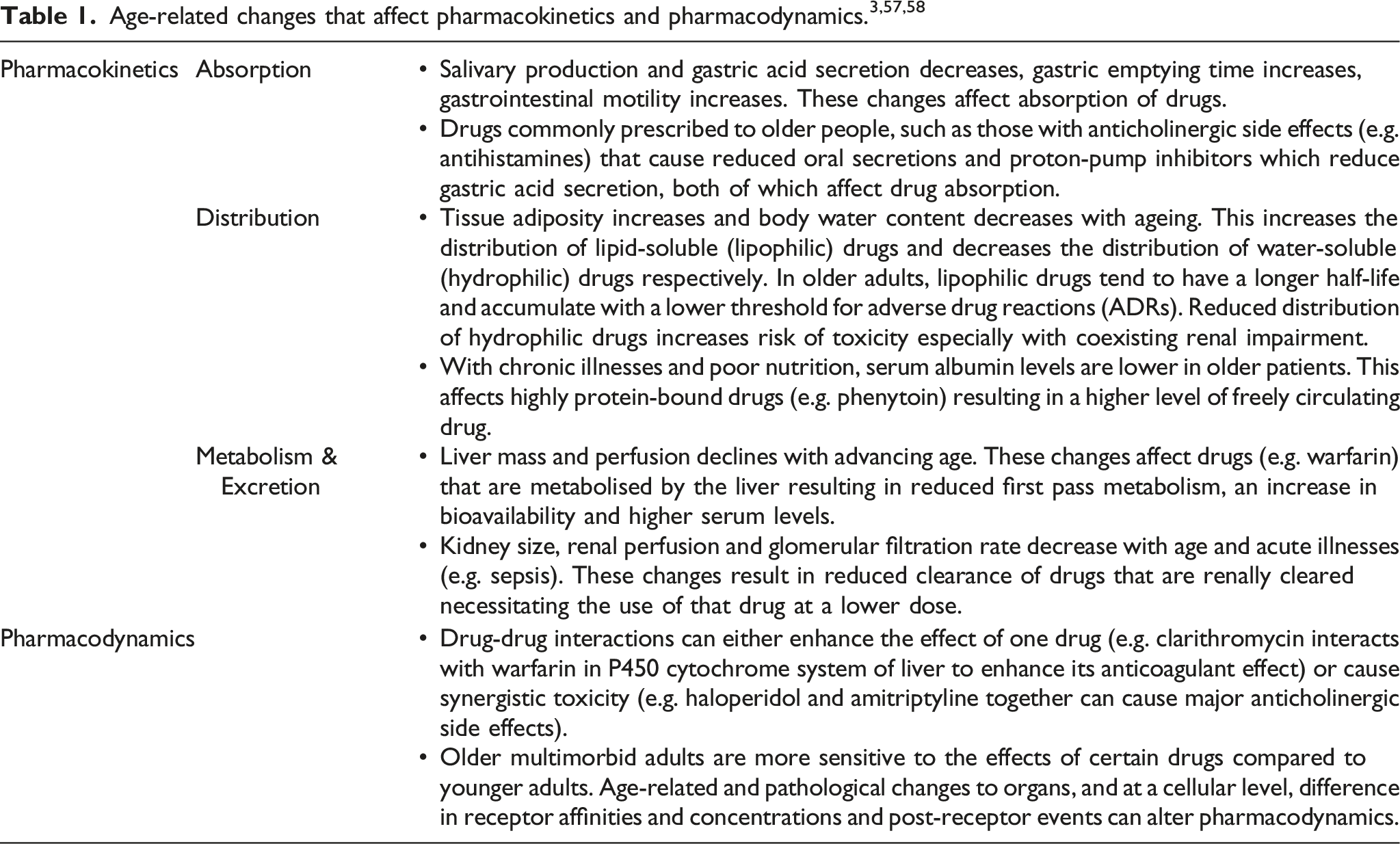
With ageing, important physiological changes occur that affect pharmacokinetics (absorption, distribution, metabolism and excretion of the drug) and pharmacodynamics (the effect the drug has on the body). Along with multiple pre-existing comorbidities, reduced physiological reserves and functional impairment, older patients are more susceptible to and affected by MEs.
Apart from the harm or potential harm inflicted on older patients, MEs also contribute to the higher economic burden on healthcare systems. A 2017 systematic review showed that MEs contribute to a country’s economic burden, with the cost of an ME during hospitalization ranging from EUR 17.6 to EUR 6432.16. 4 The United States (U.S.) spends more than $40 billion per year on patients who have been affected by MEs and the global cost of MEs constitutes almost 1% of the total global health expenditure. 5
Although MEs pose a worldwide healthcare problem, most studies on it have been performed mainly in developed countries in North America and Europe, and such studies are lacking in Southeast Asia (SEA). 6 In Singapore, there have been several interventions to reduce MEs, but quantitative studies examining the effectiveness of these interventions here are lacking. Hence, we had to extrapolate the findings of studies examining the impact of similar interventions to reduce MEs in overseas healthcare systems to our local context.
For this narrative review we will be addressing some of the common risk factors for MEs in the older population and examining local data on MEs. We will also be reviewing the interventions that have been implemented to reduce MEs locally and examine their effectiveness based on similar overseas interventions. Along with future propositions, this review endeavours to provide useful and pertinent information that will trigger future local studies to better understand the effectiveness of locally implemented interventions in reducing MEs among the older population.
Factors contributing to medication errors (MEs)
MEs resulting in ADEs occur commonly in older adults but there has been limited data, overseas, pertaining to self-reported ADEs in elderly community-dwelling or outpatient clinic populations.7,8 Also, overseas ME rates are reported differently. 9 With the exception of polypharmacy, factors contributing to MEs are still poorly understood owing to limited data, particularly on self-reported ADEs, and the variability in the data reported.
Polypharmacy
Multimorbidity, defined as two or more chronic medical conditions, results in polypharmacy which is often defined as the long-term use of five or more prescribed drugs daily. 10 Although polypharmacy may be indicated for the management of multiple medical conditions, the risk of inappropriate prescribing also inevitably rises from this.11,12 Older people with several medical conditions requiring multiple medications are therefore at risk of or subject to MEs. As much as 30% of hospital admission in older adults are related to drugs, half of which are preventable.13,14 Polypharmacy increases the probability of DDIs, drug-disease interactions and ADEs.15,16 One epidemiological study estimated the risk to be around 38% for four drugs and 82% for seven drugs or more. 17 A 2021 study carried out in Spanish primary healthcare centres on multi-treated (with five or more drugs) elderly patients between the ages of 65–74 with multimorbidity (three or more chronic disease) showed that half of the patients had at least one DDI in their prescriptions. 18 In Hong Kong where polypharmacy afflicts 77.8% of older patients, 30%–59% of patients have been found to be taking at least one inappropriate medication. 19
In Singapore’s rapidly ageing population, where the number of citizens aged 65 and above is expected to more than double from 440,000 to 900,000 by 2030, the number of older patients with multiple medical conditions will inevitably escalate. 20 Associated with this, polypharmacy will be a significant problem among our older patients, bringing with it MEs. A 2004 local study at nursing homes warned of this problem in its report of polypharmacy being seen in 58.6% of the 454 elderly residents with 70% of them receiving inappropriate medications. 21
Potentially inappropriate medications (PIMs) common in the geriatric population
In geriatric medicine, the difference between what is appropriate and inappropriate medication can be ambiguous and often decisions made are complicated by there being a lack of evidence in older patients. 22 Older patients often end up taking medications in the absence of evidence about their efficacy and safety in older age groups which would then make the drug a PIM or are denied potentially effective treatments because medications are untried in their age group. 23 In the latter scenario, the denial of a potentially effective medication can unintentionally contribute to the mortality and morbidity of the older patient.
Poor health literacy resulting in poor compliance
Most often what contributes to a ME on the part of the patient is not the patient’s intentional disregard of medication instructions but a poor understanding of the changes made or even a failure to notice medication changes. Unintentional non-adherence to medications were found in up to half of the patients following a hospital discharge. 24 Older patients were found to be at risk of this behaviour in one study. 25 Another study found that 14% of older patients with non-adherence were re-hospitalised at 30 days following initial hospital discharge. 24 One particular group of patients at high risk of suffering the effects of medication non-adherence include those with depression and impaired cognition as they possess a poor comprehension of medication-related information. 26 Another similarly at-risk group consists of patients who receive multiple medications or complicated regimens. 26 Older patients with multiple medical conditions requiring multiple medications form a majority of the latter group.
Factors contributing to medication errors vary according to practices of health systems
The rates of MEs and their contributing factors are circumstantial as they depend on the medication delivery process of the health system. A 20-weeks prospective study conducted in a geriatric ward of a public teaching hospital in Bali, Indonesia, showed that MEs occurred at every stage of the medication delivery process with administration errors being the most frequent (59%). 9 In this hospital, nurses are the primary healthcare professionals responsible for medication administration and its documentation in the ward. Their high workloads may have contributed to the high frequency of administration and transcription errors. 9 Plausibly, electronic prescribing system would provide a comprehensive solution but the cost involved in implementation and maintenance and the need for sufficient computer literacy to effectively utilise the system made it a less viable solution. 9
In addition to the aforementioned, other system-dependent factors include multiple prescribing physicians involved in the care of a single patient, lack of continuity of care and the low availability of clinical pharmacy services. 27
Local studies and what we learnt from them
While there have been several interventions across various institutions, there has been a paucity of quantitative studies examining the efficacy of these interventions in reducing MEs in Singapore.
A retrospective clinical record review of 150 elderly patients in a local tertiary care hospital was done to estimate the number of medication discrepancies (addition, omission or duplication of medications, and/or a change in dosage, frequency or formulation of medication) between preadmission and discharge medication lists. A total of 279 medication discrepancies were identified, of which 42 were unintentional medication discrepancies (35 were related to omission/addition of a medication and seven were related to a change in medication dosage/frequency). The authors concluded that unintentional medication discrepancies are a common occurrence at hospital discharge. Notably, discharge summaries often do not have adequate information on the reasons for medication changes. 28
Case notes review was conducted among 454 residents in the geriatric age group residing in three randomly selected local nursing homes. Polypharmacy and inappropriate medication use were seen in 266 (58.6%) and 318 (70.0%) residents, respectively. There was significant association between polypharmacy and inappropriate medication use. The most common medication-related problems were significant potential for adverse drug reactions (n = 281) and drug interactions (n = 141). The authors concluded that the prevalence of polypharmacy and inappropriate medication use is high in Singapore nursing homes and suggested that a multidisciplinary approach involving geriatricians, nursing home physicians, nurses and pharmacists may potentially reduce polypharmacy and inappropriate medication use in Singapore’s nursing homes. 21
At one of the local tertiary care hospitals, a multidisciplinary team consisting of professionals trained in geriatric care (a geriatrician, specialist registrar, geriatric advanced practice nurse and board-certified geriatric pharmacist) adopted interventions for frailty within the hospital’s Accident and Emergency (A&E) department and reported a success rate of up to 81.4% in preventing acute hospital admissions in older adults, with no compromise in health outcomes. 29 The authors acknowledged the important role of the geriatric pharmacist in minimising potentially avoidable acute admissions due to MEs. 30
A retrospective prevalence study analysed the pharmacotherapy-related problems highlighted by pharmacists in three local nursing homes and the rate of acceptance of pharmacists’ recommendations. A total of 392 pharmacotherapy problems were identified and 236 (60.2%) recommendations were accepted. The authors concluded that the provision of pharmaceutical care to nursing home residents resulted in improved medication safety and quality of care. 31
In a prospective case series, eligible patients were recruited from a local tertiary hospital and referred to their preferred community pharmacy for medication reconciliation, review and counselling. Among the 32 participants who completed the study, 63 drug-related problems (DRPs) were identified from 379 medications reviewed, and 60 (95.2%) were resolved by the community pharmacists. Drug interactions (n = 11, 17.5%) were one of the most common DRPs. In this model, community pharmacists played an important role in identifying and resolving DRPs by providing patients with medication reconciliation and review services from a more convenient neighbourhood location. 32
Liew et al. conducted a systematic review with meta-analysis to pool the adverse outcomes of potentially inappropriate prescribing (PIP) in primary care. Although PIP did not affect mortality, it was significantly associated with other outcomes, including emergency room visits, ADEs, functional decline, health-related quality of life and hospitalizations. This meta-analysis provides consolidated evidence on the wide-ranging impact of PIP among older persons in primary care. 33
Effectiveness of interventions relevant to Singapore
Even though several interventions have been implemented within Singapore’s health system to reduce MEs, local data pertaining to the efficacy of these interventions is lacking. Looking at how overseas models similar to our local interventions have fared may provide us with an idea of their effectiveness in reducing MEs.
Computer physician order entry (CPOE) systems
The wider use of electronic prescribing has been long recommended for the purpose of reducing MEs. Since the early 1990s, electronic prescribing has evolved into the CPOE system which refers to a variety of computer-based systems for ordering medications and automating the medication ordering process. 34 The CPOE system can range from offering no decision support (provision of a selection of drugs from a list, information on available doses and costs, access to drug monographs), limited decision support (provision of evidence-based patient-specific recommendations of a drug, dosing, frequency) or advanced decision support (provision of at least some drug-allergy contraindications, drug-drug interactions, drug-laboratory, or other patient-specific alerts). 34 Locally, we utilise the advanced form of the CPOE system. A systematic review by Ammenwerth et al. 34 to determine the effects of electronic prescribing showed that the CPOE system is a useful intervention for reducing the risk of MEs and ADEs, especially the advanced CPOE system within the hospital setting. Of the 25 studies that analysed the effects on ME rate, 23 showed a significant relative risk reduction of 13%–99%. However, another earlier systematic review concluded that the heterogeneity of research designs, information systems, patient settings and outcome measures preclude a definitive conclusion on CPOE being an effective intervention and recommended further testing of the CPOE system in diverse settings to examine its true potential. 35
Qualitative studies have shown some of the unintended negative effects of CPOE systems particularly, on doctor-nurse communications and collaborations. 36 CPOE systems have produced an asynchronous working relationship between doctors and nurses resulting in excessive documentation with a lack of verbal communication or visibility of each other’s actions leading to MEs. Electronic prescribing also runs the risk of replacing clinical judgement pertaining to simplification of medication regimens, appropriate drug choices and relevant indications. The development of a systematic approach to patient-centred care particularly for the frail, elderly patient where several factors have to be considered before deciding to start on a particular drug (i.e. warfarin) may also be negatively affected with the utilisation of an electronic prescribing system. 16
National electronics health records (NEHR) 1 repository
The NEHR system has facilitated the reconciliation of medications especially for our rapidly ageing population of older adults who are being managed for multiple medical conditions with several medications by various healthcare providers. Having a centralised national repository of medical records allows for various medical practitioners to be informed of the medications that have been used to manage a particular condition potentially avoiding polypharmacy or even a prescribing cascade. A prescribing cascade occurs when ADEs are mistaken as a new medical condition which leads to the addition of new drugs to treat the ADE. 38 This in turn places patients at risk of experiencing additional ADEs from the unnecessary treatment. Overall, it seems intuitive that having a centralised electronic system is beneficial as authorised healthcare professionals can access valuable longitudinal information pertaining to the healthcare of an older adult. Understandably, in much larger and infrastructurally varied populations elsewhere, having a centralised electronic health records system similar to NEHR with studies to examine its effect on MEs may prove challenging. This may explain the lack of qualitative and quantitative studies overseas to examine the effects of having a centralised medical health records system.
Pharmacist-centred intervention
Globally, it has been shown that pharmacists can prescribe safely but despite this the longstanding practice, in most healthcare settings, has been to let the physician play the central role in prescribing. 39 In Australia, recent studies have shown that pharmacist-led interventions which include a partnered doctor-pharmacist prescribing have not only produced lower rates of medication errors but a reduced length of hospital stay (4.7 versus 4.2 days with p < 0.001) which in turn will lead to reduced healthcare costs. 40 In another Australian geriatric service, a collaborative pharmacist-led prescribing model for discharge prescriptions had fewer patients with MEs than the usual prescribing model in both handwritten and digital prescriptions. 41
Another similar model wherein pharmacists utilise a common electronic health record to access latest information on patient demographics, medication history and laboratory values allowing them to detect medication discrepancies, perform medication reconciliation and advice on potential DDIs, drug-disease interactions and ADEs has proven to help lower MEs and reduce polypharmacy in older patients. 42 Also, by checking medication compliance, providing counselling, identifying the patient’s difficulties, and communicating this valuable information to clinicians who can make appropriate modifications to the medication regimen, pharmacists further augment the positive effects of centralising their role. This sort of patient-centred care will be beneficial for the older vulnerable patient.
The input of clinical pharmacists has also been shown to reduce MEs in acute hospitals, at time of discharge and in intensive care settings. 43 Therefore, making the pharmacist’s role more central, especially in settings attended frequently by older multimorbid adults where they face a higher chance of getting their prescriptions altered, makes this a potentially effective intervention. 3 The A&E department is one such setting.
Education and training as an intervention
Although advanced practice nurses and pharmacists locally have taken on bigger prescribing responsibilities, majority of the prescribing is still performed by doctors who receive training for prescribing only in medical schools. In UK, this training is perceived to be inadequate by both students and junior doctors. 44 A randomised control trial to study the impact of a structured online geriatric prescribing-education program on junior hospital doctors showed that doctors who received the online education performed better in a subsequent assessment of their geriatric prescribing knowledge compared to those who did not. 45 Whether this translated to an application of the knowledge resulting in fewer MEs was not determined. Nevertheless, this intervention was low-cost, reproducible, and user-friendly, as evidenced by the low drop-out rate of doctors in the trial’s intervention arm. 3 Also, training should extend to post-graduate years beyond the first post-graduate year of practice.
Use of prescribing assessment tools – Beers criteria and STOPP/START criteria
Apart from education, the utilisation of elder-specific prescribing quality assessment tools has helped facilitate the decision-making process when it comes to prescribing medications to the older patients appropriately. There are several elder-specific prescribing tools. One of the best-known tools, the Beers criteria, first published in 1991, with its sixth version published in 2019 and endorsed by American Geriatric Society (AGS), is commonly used by geriatricians. 46 In recent years the STOPP/START criteria have emerged as an alternative to the Beers criteria after it was first published in 2008 and purposed for use in routine clinical practice. 47 STOPP criteria are designed to detect PIMs and START criteria places emphasis on medication omissions in which potentially beneficial medications for the older person are not prescribed. One study showed that the STOPP/START criteria applied once within 48 hours of acute hospital admission of older adults significantly improved the level of appropriate medication use in this group which was maintained for 6 months post-discharge. 47 Another trial by Frankenthal et al. 48 showed that routine application of the STOPP/START criteria in nursing homes for older adults significantly reduced polypharmacy, monthly drug costs and the incidence of falls. When used by the multidisciplinary geriatric medical team for acutely ill hospitalised elderly patients, the STOPP/START criteria helped reduce the number of patients taking PIMs compared to control patients receiving standard pharmaceutical care (19.3% versus 39.7%). 49
Essentially, several clinical trials have shown the use of prescribing tools on older persons to yield clinical benefits but the applicability of these studies is limited by their single centre, small scale and inevitably single blind designs. 3
Propositions for the future
In view of the global demographic shift due to a rapidly ageing population, with data showing multimorbid older patients being vulnerable to MEs, it is important that medical students and doctors receive appropriate training particularly in geriatric medicine and geriatric pharmacotherapy, regardless of their eventual career path. 3 Similar to physicians, clinical pharmacists would also benefit from structured training in geriatric medicine and geriatric pharmacotherapy both at an undergraduate and postgraduate level. Through online didactic teaching, relevant geriatric pharmacotherapy knowledge can be acquired conveniently. An example of an online teaching resource is the UK-based Prescribing Safety Assessment. 50 Such an online assessment could be modelled to suit our local context and healthcare system.
Another area of technological application to reduce MEs is that of artificial intelligence (AI). By reviewing medical records and medication information, AI algorithms can identify as well as predict potential MEs. 51 Potential application includes identifying drug overdose, duplication order, and timing of medications with counteracting effects.
While technology has helped augment efforts to reduce MEs, it should not compromise on a personalised approach encompassing effective communication, exchange and clinical reasoning. When attending geriatric ward rounds, a pharmacist gains both insight into the geriatrician’s perspective and rationale of prescription patterns, as well as patients’ multiple comorbidities. By reviewing patients’ medication list on the spot, a pharmacist also provides immediate feedback, reducing prescription errors and educating the medical team on safe prescription practices. A multi-disciplinary team approach involving the doctor, pharmacist and in addition, the nurse, will ultimately benefit the patient, in terms of improving MEs, as each plays an inter-dependent role in the pharmacotherapy process.
MEs are not only made by healthcare providers but by patients as well. Hence, minimising MEs should focus also on the patient-related factors, one of which is health literacy. With better understanding of their health condition and medication history, older patients would be in a better position to take an active role in patient-centred shared decision-making discussions with their doctors and pharmacists. 52
Training of older adults in self-administration of medications (SAM) whilst inpatient could help reduce MEs. A pilot program of SAM implemented within a local inpatient rehabilitation unit where patients were trained and assessed in SAM showed good patient safety outcomes in terms of safe SAM post-discharge through educational empowerment and identification of patient-related factors. 53
With the glaring lack of local studies, it is important to recognise that having adequately powered high quality trials to assess the effects of interventions to reduce MEs locally is important in developing them further. Based on the findings of these studies, changes can be made to the pharmacotherapy process that could potentially lead to further minimisation of MEs. For example, qualitative studies would be useful to address doctors’ and patients’ perceived barriers to pharmacotherapy optimisation and future trials could also focus on specific drug classes (e.g. benzodiazepines) relevant to the older adult or even specific types of ADEs such as drugs that predispose to falls.54,55 Furthermore, future trials could also be carried out in clinic, community and nursing home settings to widen the applicability of their findings.
Medical error reporting (MER) systems in each institution provide another means by which MEs can be reduced. Through reporting MEs, we can learn about the failures in the pharmacotherapy process that led to the ME and perform root cause analyses. 6 Often the reluctance in reporting MEs is due to the additional administrative work involved and perceived repercussions such as fear of legal consequences, disciplinary action, loss of credibility and public embarrassment. 6 A simplified non-punitive MER system that advocates the participation of pharmacists and all other healthcare professionals should instead be implemented. 56
Conclusion
Medications, if utilised wrongly, may pose a significant threat to the provision of safe and effective healthcare especially in a growing population of vulnerable older adults in whom the effects of MEs can be dire. Several studies have shown MEs to be common in this group. Additionally, MEs further contribute to burgeoning healthcare costs associated with an ageing population and potentially lessens the public trust placed on the local healthcare system.
Although a global problem, studies pertaining to MEs are mostly sited in developed western countries with a limited number of such studies being carried in SEA. Singapore, too, lacks in studies on MEs but has implemented several interventions over the years to reduce MEs. However, the effect of these interventions on MEs, especially among older patients, has yet to be adequately examined. With this lack, we can only gauge their effectiveness based on overseas studies examining the efficacy of similar interventions elsewhere.
MEs should be regarded as a result of the issues within a healthcare system rather than as a result of an individual's or team’s failure. In an advanced healthcare system like ours, it becomes essential to identify system-based factors that contribute both directly and indirectly to MEs. Hence identifying MEs and proactively reporting them provides a useful resource or database to analyse and learn from. Also, studies looking at the impact of interventions to reduce MEs, particularly qualitative ones, are important to examine the process and make further changes to improve the end result of minimising MEs.
It is hoped that this review will highlight the need to actively evaluate the effectiveness of our various local interventions in reducing MEs for the purpose of further optimising them to cope with our rapidly ageing population.
Footnotes
Author contributions
All authors have contributed significantly, an!d agree with the content of this review article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.