
Abstract
Background
Chronic insomnia disorder, a condition associated with frequent and persistent difficulty in initiating or maintaining sleep, is one of the most common reasons for patients consulting general practitioners and psychiatrists in Singapore.
Objectives
The landscape for managing chronic insomnia disorder is constantly changing but a clear, updated guidance for its management is lacking.
Methods
This guidance document provides guidance and recommendation for the diagnosis, assessment, and management of chronic insomnia disorder in Singapore based on a review of the current clinical practice guidelines and recent evidence including findings specific to Singapore.
Results and Conclusion
This document further summarises the properties and safety profiles of various pharmacological agents and provides guidance for their use across patient profiles. Lastly, this document provides recommendations from a panel of 5 clinicians with expertise in treating patients with sleep disorders.
Introduction
Insomnia is a common sleep disorder which poses a major public health concern worldwide. 1 Over time, the nosology of insomnia has varied across the three major classification systems (International Classification of Sleep Disorders [ICSD], International Classification of Diseases [ICD] and Diagnostic and Statistical Manual of Mental Disorders (5th Edition) [DSM]), but has slowly evolved to be almost identical.2–5 Clinical diagnosis of insomnia is based on patient complaints such as difficulty falling asleep or maintaining sleep or simply unrefreshing sleep resulting in daytime dysfunction, impairment of daily activities and quality-of-life (QoL) despite a suitable sleep environment and sleep hygiene practices. It is generally classified according to its chronicity: chronic (persistent) insomnia is most commonly defined as a disturbance in sleep which occurs at least 3 times/week for 3 months or longer while short-term (episodic) insomnia is defined by the same criteria, but for periods <3 months.3,5–7
It is estimated that 30–50% of the population suffer from occasional short-term insomnia and at least 5–15% of adults develop chronic insomnia disorder.6–12 The rates vary depending on the populations studied. For example, significantly higher rates have been reported in older individuals and in patients with medical and/or psychiatric comorbidities, and it is more frequently diagnosed in females.7,8,13,14
With the demands posed by a modern lifestyle and work-related pressures, there is evidence that sleep disorders are becoming a common reason for medical consultation. In terms of disease burden, insomnia is associated with numerous detrimental effects on functional status, health/well-being, and QoL.8,15,16 This is reflected in increased rates of work absenteeism, occupational/motor vehicle accidents, depression and alcoholism and, as such, it places a substantial economic burden on society [for reviews see references 6,8].6,8 More recent data indicate a higher prevalence of insomnia in some European countries and this has been paralleled by the greater use of hypnotic medicines. 6
In the Singapore Mental Health Study, the prevalence of insomnia-related sleep disturbances among patients with lifetime and 12-month major depressive disorder was 90.9% and 91.4%, respectively. 17 Previous studies found that 42.5% of workers reported poor sleep quality. 18 Poor sleep quality occurred in 54.3% of patients aged >65 years with at least one cardiometabolic risk factor treated in primary care 19 and 13.7% of adults aged ≥60 years reported having at least one sleep problem in the previous month. 13 Among people with mental illnesses, poor sleep quality was reported in 27.6%, 20 insomnia disorder in 31.8% 21 and clinical insomnia in 22.6%. 22
Treatment guidelines for chronic insomnia disorder are evolving globally with modification of classification systems, greater awareness of the risk-benefits of conventional hypnotic medications and the introduction of new therapeutic approaches. However, clear guidance is still lacking and, in light of this, our goal was to review recent changes as they apply to Singapore and to develop updated recommendations to assist local physicians in the management of patients presenting with chronic insomnia disorder.
Methods
This guidance document is based upon 3 stages of development, following the Research and Development/University of California Los Angeles (RAND/UCLA) consensus method. 23 Stage 1 involved a review of the literature focused on the management of insomnia included in current evidence-based clinical practice guidelines such as from the European Sleep Research Society, 6 the American Academy of Sleep Medicine.7,8 Stage 2 involved the inclusion of findings specific to Singapore based on a search of PubMed from 1/1/2010 to 30/6/2023 using the terms “insomnia” and “Singapore” and augmented by references known to the authors. Stage 3 involved the final recommendations from an advisory panel of 5 clinicians with expertise in the management of patients with sleep disorders which is based on a structured methodology comprising: development of a questionnaire relating to management of chronic insomnia based upon the literature (Supplemental Table 1), determination of key issues arising from the questionnaire based on on-line feedback from the advisory panel, a meeting of the panel to discuss and finalise recommendations based on the best available evidence and clinical judgement.
Guidance and recommendations: literature review
Diagnosis and assessment of insomnia
Chronic insomnia disorder is a common psychiatric condition which primary care physicians often overlook. This may be due to time constraints associated with the lengthy consultation times required to exclude many differential diagnoses.7,24–26 European guidelines propose that clinical assessment should include:
6
• Clinical interview (evaluation of the current sleep-wake behaviour; sleep history; somatic and mental disorders; physical evaluation; use of sleep questionnaires/diaries and others) • Actively ascertain use of medications, alcohol, caffeine, nicotine and illegal drugs • Sleep diaries/actigraphy to determine irregular sleep-wake patterns or circadian rhythm disorder • Polysomnography is recommended when other sleep disorders occur or are suspected (e.g., periodic limb movement disorder, sleep apnoea, narcolepsy, treatment-resistant insomnia, or insomnia in occupational high-risk groups).
DSM-5 (2013) removed the distinction between primary insomnia and insomnia-related comorbidities. 5 Instead, a revised category, insomnia disorder, was introduced which is also used in the third version of ICSD. 3 There is also evidence that insomnia is a risk factor for psychiatric disorders such as major depression, anxiety, suicide ideation and substance abuse, and vice versa.27–30 Furthermore, cross-sectional studies have reported an association between insomnia and co-morbid medical conditions (e.g., cardiovascular, pulmonary, gastrointestinal, and many other disorders).1,31
Management of chronic insomnia disorder
Sleep hygiene
Treatment of chronic insomnia disorder should be initiated with a full understanding of the sleep problem and good sleep hygiene should include a conducive sleeping environment, regular routine for rising and retiring, avoiding caffeine, nicotine and alcohol before bedtime, reducing screen time before bedtime, reducing daytime napping and practising relaxation techniques. 32
Sleep hygiene practices should be personalised to take into consideration negative emotions that can impact sleep, and incorporating behavioural changes and a commitment to planned actions for successful implementation. 32 Before therapy is instituted, most patients are asked to maintain a sleep diary and complete a sleep-specific questionnaire to help provide a clearer picture of the degree of sleep disturbance. This will help facilitate an accurate diagnosis and the development of a tailored treatment strategy. 12
Cognitive behaviour therapy for insomnia (CBT-I)
CBT-I is a multicomponent intervention which incorporates 3 main components; cognitive control therapy, stimulus control and sleep restriction therapy (with or without relaxation therapy). 33 The access to CBT-I is challenging for a variety of reasons including lack of availability, long waiting list, insufficient numbers of train psychologists and lack of medical insurance coverage for CBT-I.26,34–38 There is evidence from randomised controlled trials (RCTs), as reported in a meta-analysis of 33 studies, that using digital techniques (computer, smart phone and other devices) to support CBT-I produces greater improvement in insomnia severity index during follow-up (≤6 months). 38
A brief survey completed by 239 physicians in 2 large tertiary hospitals in the US (both having well-established sleep laboratories) reported that they saw an average of 121 patients/month (15 with insomnia), but only a mean ± SD of 1.5 ± 4.9 were referred for treatment with CBT alone. 39 This was also reflected in an expert assessment of non-pharmacological treatment of insomnia in Japan, with the highest levels of recommendation for treatment approach (in descending order) being: sleep hygiene education, relaxation therapy, stimulus control, sleep restriction therapy, and finally CBT. 37 The authors note that it is difficult to recommend in the Japanese clinical setting due to the lack of adequate resources.
Pharmacological treatments

Updated treatment recommendations for sleep disorders from a collaboration of the Section of Addiction Psychiatry of the College of Psychiatrists and the National Addictions Management Service, Singapore. 42

The evidence relating to the comparative effectiveness of drugs prescribed for adults with chronic insomnia disorder was the focus of a systematic review/network meta-analysis involving 148 articles, 153 clinical trials and 46,412 participants. 43 Compared with placebo, total sleep time was significantly improved with non-benzodiazepines, antidepressants, and DORAs. In addition, sleep onset latency was significantly shortened with non-benzodiazepines and melatonin receptor agonists. Non-benzodiazepines also significantly decreased wake time after sleep onset. 43 DORAs are a newer class of FDA-approved medicines indicated for the treatment of insomnia characterised by difficulties with both sleep onset and sleep maintenance. In another systematic review/network meta-analysis (69 studies and 17,319 participants), DORAs were found to be superior to “Z-drugs” with respect to wake time after sleep onset and sleep efficiency, and better than melatonin receptor agonists for sleep latency, wake time after sleep onset and sleep efficiency. 44 Melatonin receptor agonists appeared to be beneficial for patients with sleep-onset insomnia and were well tolerated. 44 A systematic review of clinical trials with hydroxyzine, which is used off-label, in adults with insomnia reported mixed findings and the authors suggested that it may be useful short-term option in patients not responding or not tolerating previous therapy. 45 A systematic review of gabapentinoids (pregabalin and gabapentin; off-label) found minimal evidence for sleep benefits in insomnia, 46 although in patients with comorbid pain, partial seizures, restless leg syndrome or alcohol use disorder improvements in sleep were observed. 7 Quetiapine is an antipsychotic drug used off-label to treat insomnia and a systematic review of 21 clinical trials demonstrated that it produced benefits including increased total sleep time and better sleep quality compared with placebo. 47
Key clinical trials with lemborexant.

AEs, adverse events; AIS, Athens Insomnia Scale; CGI-I, clinical global impression improvement scale; CI, confidence interval; DB, double-blind; DFS, daytime functioning score; ISI, insomnia severity index; LEM, lemborexant; m, months; MC, multicentre; n, NIGHT; PC, placebo-controlled; PG, parallel groups; PL, placebo; PSG, polysomnography; R, randomised; sSOL, subjective sleep onset latency; sTST, subjective total sleep time; sWASO, subjective wakefulness after sleep onset; TEAEs, treatment-emergent adverse effects; ZOL, zolpidem.
The favourable improvements in sleep parameters produced by lemborexant in controlled clinical trials has been noted in several evidence-based systematic reviews/network meta-analyses.43,44,56 In one which included 170 trials, 36 interventions and 47,950 participants, and representing some of the highest clinical best-evidence available, eszopiclone and lemborexant were considered to have the best overall profiles in terms of efficacy, patient acceptability and tolerability. 56 However, the authors added the caveats that eszopiclone may cause ‘substantial adverse events’ while the safety data on lemborexant were currently “inconclusive” based on the criteria established in the meta-analysis. 56
Management of patients with comorbidities
Compared with individuals not suffering insomnia, patients with chronic insomnia reported a higher prevalence of comorbid medical conditions such as chronic pain (50 vs 18%), hypertension (43 vs 19%), gastrointestinal disorders (34 vs 9%), breathing difficulties (25 vs 6%), heart disease (22 vs 10%), urinary problems (20 vs 10%), diabetes (13 vs 5%), cancer (9 vs 4%) and neurological disorders (7 vs 1%). 1 Furthermore, patients with chronic pain, hypertension, gastrointestinal disorders, breathing difficulties, heart disease, urinary problems, cancer and neurological disorders were more likely to have insomnia than individuals without these disorders. Interestingly, insomnia exhibits a bidirectional association with psychiatric illnesses such as depression, anxiety, bipolar disorder, schizophrenia and post-traumatic stress disorder and is often included as a symptom of these conditions.14,26,57 Indeed, Freeman and colleagues reported a ubiquitous level of sleep disturbances in individuals with psychiatric disorders reflecting an overlap in genetic, neurobiological, psychological and environmental causes. 14 They also noted that disrupted sleep might accentuate mental health problems as a result of negative effects, hyperarousal, emotional dysregulation and that treating insomnia should help reduce the severity of psychiatric symptoms.
In Singapore, a study of local residents (n = 6126) found that 27.6% reported poor sleep quality and individuals with comorbid mental health problems (adjusted OR 14.11, 95%CI 6.52 – 30.54; p < .01) and multiple medical comorbidities (1.63, 95%CI 1.24 – 2.15; p < .001) were significantly more likely to report poorer sleep compared with healthy controls. 20 Individual studies have found a high prevalence (>90%) of insomnia in patients with major depressive disorders 24 and those with first episode psychosis. 58 In the latter study, 62.9% reported poor sleep quality and this rate was higher than that for patients with chronic schizophrenia receiving antipsychotics. In other studies, poor sleep quality was reported in elderly Singaporean with nocturia 19 and pain. 59
Various studies have evaluated drug treatments for insomnia in patients with comorbid conditions. In a study evaluating insomnia and mood stability in patients with euthymic bipolar disorder, patients who received ramelteon were less likely to experience bipolar disorder relapse. However, improvements in sleep were not statistically significant. 60 Another study examining treatment-resistant insomnia in patients with bipolar disorder reported inconsistent efficacy results. A small increase in objective total sleep time was observed with suvorexant during the randomized phase but not during the open-label phase of the study. 61 In patients with comorbid major depressive disorder and insomnia, the combination of zolpidem and escitalopram significantly improved various sleep parameters compared to escitalopram alone. 62 For patients with alcohol dependence and comorbid insomnia, gabapentin significantly delayed the onset of heavy drinking compared although without differential effect on sleep. 63
Re-evaluation and follow-up
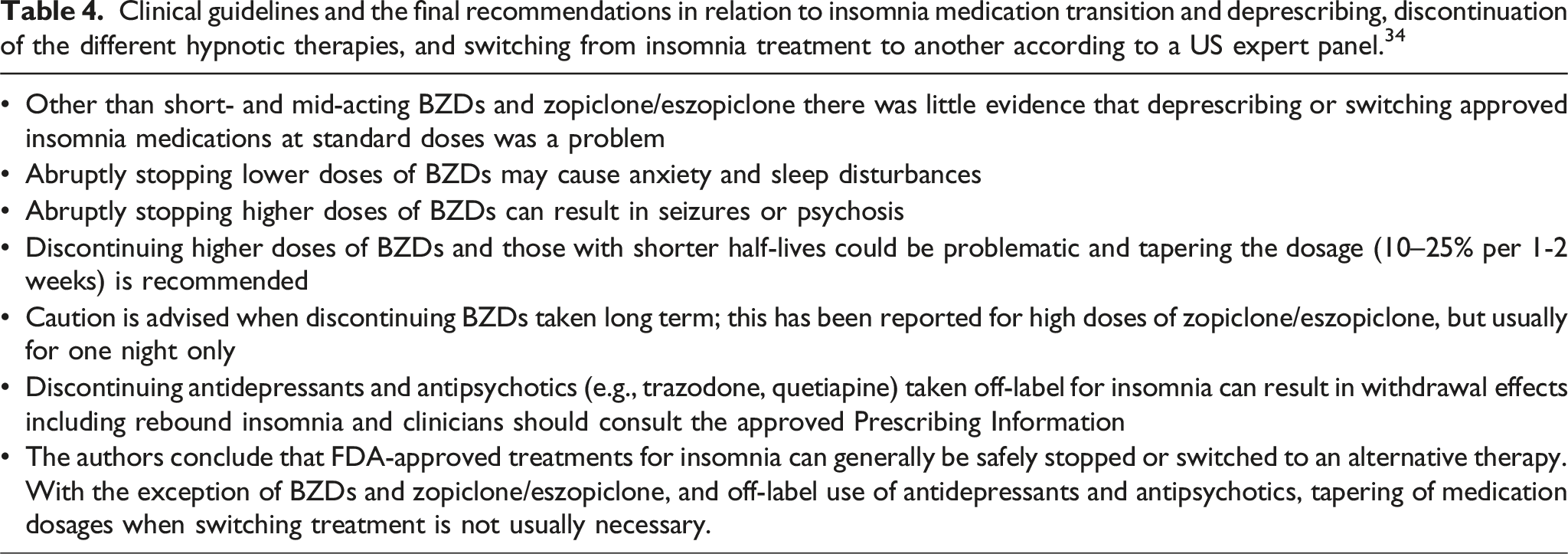
Determination of the most effective treatment for persons with chronic insomnia disorder is based on clinical judgement taking into consideration patient preference, comorbidities and access to available therapies. CBT-I is included in most clinical practice guidelines but, as noted previously, it is not always readily available or effective, and many patients request pharmacotherapy. 8 Pharmacotherapy can have diverse effects in terms of sleep benefits as well as their safety/tolerability, and such treatment is generally only recommended for short-term use (2-4 weeks in Singapore). 42 This poses a problem for many patients with chronic insomnia necessitating long-term treatment.12,34 Furthermore, some classes of hypnotics used in the management of chronic insomnia tend to lose their effectiveness over time which is an additional challenge for physicians. 34 This is compounded by the fact that patients may respond differently to treatment, both in terms of efficacy and/or safety, and multiple trials may be needed to ascertain optimum treatment. Possible problems associated with changing treatments for insomnia (depending on which drugs are involved) include rebound insomnia with exacerbation of symptoms, withdrawal syndrome, impact on the perception of efficacy for future treatments and, in rare instances, precipitation of seizures. 34 Clinicians note that currently little guidance is available for the safest and most effective way to switch between different hypnotic agents and, as a result, physicians should exercise sound clinical judgement based on current best evidence, clinical experience, prior patient responses to treatments, patient preferences and potential adverse effects. 34
Clinical guidelines and the final recommendations in relation to insomnia medication transition and deprescribing, discontinuation of the different hypnotic therapies, and switching from insomnia treatment to another according to a US expert panel. 34
Referral to relevant specialists
In practice, insomnia is treated in primary care; however, there are occasions when referral to a sleep specialist or psychiatrist would be appropriate:
24
➢ Patients with insomnia resistant to treatment (notably high-dose/long-term BZDs) ➢ Patients with other sleep disorders such as obstructive sleep apnoea or restless leg syndrome ➢ Patients with other disorders which are moderate-to-severe, proving difficult-to-treat such as chronic pain, psychiatric diseases, narcolepsy, circadian rhythm disorders, etc. ➢ Patients non-compliant with professional advice.
Guidance and recommendations: Singapore expert panel
Management of people with chronic insomnia is undergoing continual refinement within current guidelines. 6 In the absence of rigorous controlled clinical trials for many therapies, a number of gaps in our understanding of which treatments are optimal to guide a personalised approach to the management of chronic insomnia. 7 This is overlaid by changes in therapeutic approach driven by continued emphasis of sleep hygiene and non-pharmacological options (especially CBT-I), appropriate use of traditional therapies (e.g., BZDs) and introduction of newer treatment options (notably the DORAs). Thus, from the outset it should be acknowledged that there are wide differences regarding the pharmacological management of chronic insomnia, recognising differences in guideline recommendations and availability of certain medications.
In light of these developments and differences, the goal of this guidance report is to determine current treatment practices in Singapore based on findings from a pre-meeting online survey (Supplemental Files 1). This was followed by a panel meeting to discuss the latest evidence pertaining to the care of people with chronic insomnia and to formulate recommendations for optimal pharmacological approaches when sleep hygiene/behavioural techniques alone are insufficient; including positioning of the recently approved DORA lemborexant in the treatment algorithm of chronic insomnia disorder, based on the current available evidence and clinical experience.
The spectrum of patients presenting to family physicians and sleep medicine specialists/psychiatrists for insomnia disorders is very broad; ranging from newly diagnosed individuals to patients with an array of medical and psychiatric comorbidities.
For newly diagnosed patients with chronic insomnia disorder, the panel recommend the following: • Most guidelines do not provide recommendations about ‘treatment of choice’ and this is partly explained by the absence of published clinical best evidence (controlled clinical trials).
7
Consequently, prescribing decisions are usually based on patient profile, physician experience with the effectiveness of the chosen therapy, and cost. • Three main classes of drugs should be considered in the first instance and these include antihistamines
45
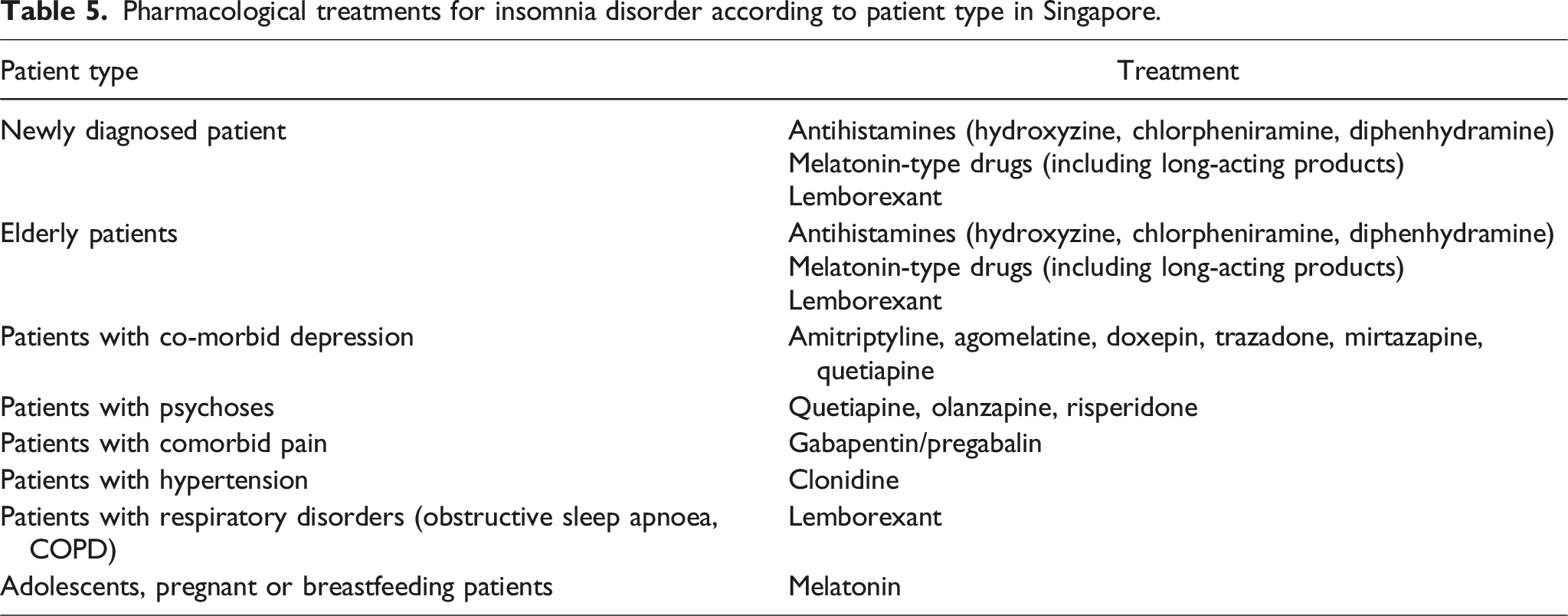
(e.g., hydroxyzine, chlorpheniramine, diphenhydramine), melatonin and DORAs (e.g., lemborexant) (Table 5). The panel notes that although antihistamines are not indicated locally for the treatment of insomnia and may be associated with significant side effects (e.g., anticholinergic effects), and the level of evidence for melatonin may be weak, these agents may be useful depending on the clinical context. • In primary care, BZDs and “Z-hypnotics” are efficacious in the short-term management of acute insomnia.
54
However, they should not be used as first-line options for the longer-term management of patients with chronic insomnia disorder, because of safety concerns and potential addictive properties.41,56 Longer-term use in patients with chronic insomnia disorder should be under the care of a psychiatrist / sleep specialist. • In the presence of comorbidities clinical judgement is needed to decide whether the chronic insomnia disorder or comorbidity is treated first, or whether they are treated simultaneously. Pharmacological treatments for insomnia disorder according to patient type in Singapore.
Elderly patients have a higher prevalence of chronic insomnia disorder than younger adults and recommendations for treatment include: • Evaluate the awareness, previous experience and response to sleep hygiene practices. • When pharmacological options are required, preferred choices include melatonin, an antihistamine (carefully monitoring for possible anticholinergic effects) and lemborexant which have been shown to be effective in older patients.45,50,64 As reported above, the panel notes that although antihistamines are not indicated locally for treatment of insomnia and may be associated with significant side effects (e.g. anticholinergic effects), and the level of evidence for melatonin may be weak, these agents may be useful depending on the clinical context. • Avoid or reduce the use of BZDs, if possible, because of adverse effects profile.
It is important to note that the recommendations for the off-label use of antihistamines in adults, especially elderly patients, relies on the rich clinical experience of the panel, given the weak level of evidence supporting the use of antihistamines for chronic insomnia disorder and significant side effects associated with their use. 45
The panel acknowledge the limited evidence available for currently approved hypnotics in special populations including adolescents, patients who are pregnant or breastfeeding. • When pharmacological options are required, melatonin can be considered as it has the most available evidence.
65
Melatonin is useful in delayed sleep-wake phase disorder in adolescents.
66
• When pharmacological options are required in pregnant or breastfeeding patients with insomnia, considerations should be taken on the safety of drug exposure of drugs to the fetus and breastfeeding infant.
67
Given the limited evidence available, melatonin may be considered for patients who are pregnant or breastfeeding.
Most frequent responses (≥50% of specialists) to pre-meeting survey questionnaire regarding the most important factors for clinicians to consider when treating insomnia disorder in specific patient groups, and considerations when changing treatment.

When to refer patients to specialist care needs to be considered on a case-by-case basis and it can be challenging to manage chronic insomnia disorder in primary care. This can be a result of factors such as comorbidities (both medical and psychiatric), the length of time needed to ascertain such contributing factors, and determination of an accurate diagnosis and providing detailed follow-up. A combined approach involving the patient, primary care physician and psychiatrist/sleep medicine specialist would be ideal.
Conclusions
Management of patients with chronic insomnia disorder is evolving both in terms of how it is defined and how it is treated. Sleep hygiene is often tried in the first instance, but may not be effective longer term. CBT-I has been shown to be effective, but a lack of psychologists trained in CBT-I and long waiting times limits its usefulness. There is a long list of alternative agents available to help manage chronic insomnia disorder (including antidepressants, antihistamines, antipsychotics, gabapentinoids and melatonin analogs, most of which are off-label) and help reduce the long-term use of BZDs. Furthermore, the development, and introduction of a new class of treatments, the DORAs, is a step forward. Lemborexant has recently been approved for use in Singapore, and findings in pivotal clinical trials and evidence-based systematic reviews have been published.
Supplemental Material
Supplemental Material - Pharmacological management of chronic insomnia disorder in Singapore: Recommendations from an expert panel
Supplemental Material for Pharmacological management of chronic insomnia disorder in Singapore: Recommendations from an expert panel by Roger Ho, Chau Sian Lim, Phern Chern Tor, Cyrus Su Hui Ho, Jason Wui Chi Pang and Beng Yeong Ng in Proceedings of Singapore Healthcare.
Footnotes
Acknowledgments
The final review was based upon discussions at a panel meeting involving 5 clinicians with expertise in treating patients with sleep disorders, and was funded by Eisai (Singapore) Pte. Ltd. The authors thank Dr Steve Clissold (Content Ed Net, Singapore) for preparation of a draft manuscript in line with Good Publishing Practice guidelines and under the guidance of Dr Roger Ho.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RCMH—honoraria (Eisai, Lundbeck, Pfizer), consulting or advisory role (Eisai, Mitsubishi, Takeda), travel (Pfizer), and stock or stock options (Pfizer). CSL—honoraria (Eisai, Lundbeck, Civil Aviation Authority of Singapore, Nanyang Polytechnic), grants (Boehringer Ingelheim), travel (Johnson & Johnson), Advocacy groups (Singapore Association of Mental Health, National Council of Problem Gambling) and Advisory Board (Eisai, DKSH Singapore, Lundbeck, Mitsubishi Tanabe Pharma). JWCP—honoraria (AstraZeneca, Eisai, GlaxoSmithKline, Pfizer), BYN—honoraria (Eisai (Singapore), Eisai (Asia, Latin America) and HI-Eisai Phillipines). All other authors declared no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Eisai (Singapore) Pte. Ltd.
Author contributions
All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Trial registration
Not applicable.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.