
Abstract
Background
Stroke is a leading cause of hospitalisation, disability, and death in Singapore. The healthcare system’s rehabilitative care model has seen ongoing evolution in response to changing patient needs and healthcare financing demands. Changi General Hospital (CGH) and St Andrew’s Community Hospital (SACH) collaborated on an integrated subacute stroke ward (SSW) in 2019 to optimise the transfer of stroke patients to the subacute rehabilitation setting.
Objective
To evaluate the outcomes of the integrated SSW.
Methods
This was a retrospective study. Anonymised data was used to evaluate functional, financial, and length-of-stay (LOS) outcomes.
Results
There were 71 patients in the control group (historical cohort) and 226 patients in the SSW cohort. Both groups were demographically, medically, and functionally similar except for a higher proportion of lacunar infarcts (LACI) in the SSW group. Although functional scores by Modified Barthel Index (MBI) were similar on discharge, the total LOS fell significantly (20 days) for the SSW group, with significant improvements in median rehabilitation efficiency (19.6 vs 10.9) but not median rehabilitation effectiveness (35.3 vs 31.0). Subgroup analysis revealed no impact from the disproportionate number of LACIs. Gross bill size, when corrected for inflation, was significantly lower across the combined hospitalisation ($31,270 vs $40,005).
Conclusions
This collaboration achieved savings in healthcare expenditure and LOS without compromising functional outcomes. The community hospital is a potent bridge for care transition and integrated services such as the SSW can optimise the rehabilitation journey for patients with stroke. Innovation in care provision can help to address the ever-changing challenges of healthcare.
Keywords
Introduction
Singapore’s traditional healthcare system was primarily structured to address the acute phase of Illness. 1 This acute-centric model of care is less robust in supporting the healthcare and rehabilitation needs of patients beyond the acute episode due to the lack of collaboration and integration with the community sector. To address this gap, the Singapore government rolled out the Regional Healthcare System (RHS) to allow each cluster of acute, subacute, and chronic healthcare providers to work collaboratively in delivering patient care that spans across the entire health spectrum.1,2 Other initiatives included establishing national health care records (National Electronic Health Record),3,4 evolutions in healthcare system financing (moving from fee-for-service where patients are charged per utilisation of service regardless of the quality of care, to value-based care where bundled payments and capitation funding models are based on efficiency, high-quality care, good patient outcomes and experiences),5–8 and harmonisation of the rehabilitation journey with outcome tracking through the National One-Rehab Framework. 9 These were envisioned to improve right-siting of patients to the care settings appropriate to their needs and at the lowest necessary cost, increase patients’ access to the expanded scope of community services, and encourage respective healthcare clusters to provide cost-effective, data-driven quality healthcare.
Post-acute rehabilitation in Singapore
Before the piloting of the National One-Rehab Framework in 2021, the post-acute hospital-based rehabilitation care journey for in-flight patients with rehabilitation needs has been institution- and cluster-dependent, with patients being transferred to either the inpatient rehabilitation unit of the acute hospital, or to one of the multiple community hospitals in Singapore. Some patients with higher-acuity specialist needs and a slower tempo of recovery could even be cared for sequentially in both. Community hospitals are local convalescence-rehabilitation facilities providing a range of healthcare facilities and resources that usually do not include emergency or acute inpatient care, intensive care, or major surgery but very commonly include inpatient rehabilitation for older people.1,10 Care models for community hospitals vary across countries and even within Singapore, with differences in service delivery, staffing, rehabilitation efficiency and outcomes.11,12 Up to the time of the setting up of the stroke subacute ward in 2019, stroke patients were not cohorted in a specialised ward in the community hospitals. Patients in the community hospitals were mainly cared for by family medicine physicians. The National One-Rehab Framework was intended to better-define and standardise right-siting for rehabilitation, as well as improve outcome measurements and goal setting across the nation. The One-Rehab framework suggested complex care be sited in acute inpatient units and others in the community hospital. There was no guidelines on the cross-over of expertise.
The CGH-SACH model
Changi General Hospital (CGH) is an acute general hospital in the east of Singapore. Our inpatient rehabilitation unit cared for 600 stroke patients in 2021. As the fourth leading cause of death in Singapore and among the top ten causes of hospitalisation in our greying population,13,14 patients with stroke experience significant morbidity and have significant rehabilitation needs. Transferred as early as the 2nd or 3rd day post stroke, these patients undergo medical stabilisation and concurrent inpatient rehabilitation whilst awaiting the completion of investigations. Most were discharged directly from our unit, leaving approximately 30% who required a longer period of rehabilitation and were referred to the community hospital setting. Prior to the set-up of the stroke subacute ward (SSW), patients have been traditionally admitted to general wards with mix of conditions within SACH.
St Andrew’s Community Hospital (SACH) is a 298-bed community hospital that was established and administered by a charitable organisation but is co-located with CGH within the same healthcare campus.
In 2019, SACH invited the CGH Rehabilitation Medicine department to collaborate in the setting up of the SSW. This was supported by literature suggesting that specialised stroke rehabilitation reduces mortality in patients with severe strokes and improves functional outcomes in those with moderate strokes when compared to non-specialized standard care. 15 Patients with more severe strokes experience reduced mortality; those with moderate strokes experience improved functional outcomes. The purpose of this collaboration was to improve stroke rehabilitation outcomes by setting up a SSW, allowing a direct and seamless transfer of patients from the acute hospital to the community hospital with fewer administrative delays. This was also an effort to integrate care between the acute and the community hospital with the initiation of the bundled care payment financing model. 6
A CGH rehabilitation physician would oversee the medical care of patients admitted to the SSW on a part-time basis, and work with a full-time medical officer to manage the care of stroke patients. The nurses and allied health staff would be SACH employees. The SSW would be sited in an integrated building shared by both organisations. The CGH – SACH model of rehabilitation would incorporate intensive inpatient rehabilitation and use of technology in the early post-stroke period. Under the National One-Rehab Framework stroke pilot, our collaboration was approved to run as a comparative stroke rehabilitation model. 16 Whilst One-Rehab provides guidance on providing rehabilitation to stroke patients in either the acute hospital or community hospital facility up to 30 days, stroke patients stay in the acute inpatient unit in CGH for a shorter period of time. Instead, if they require a longer period of rehabilitation, they would be transferred to the SSW.
System changes and integration
Multiple meetings were held between the staff of 2 organizations, i.e., CGH Rehabilitation Medicine Chief, Consultant, Clinical Services, Finance, Medical Social Services and SACH Medical, Nursing, Allied Health, Human Resources, Finance, Medical Social Services and Business Office. Multiple workflows had to be discussed and set up, comprising referral, transfer to the subacute ward, transfer back to the acute setting due to medical deterioration, collapse and resuscitation and rapid response team coverage (known locally as the Medical Emergency Team - MET).
The SACH nursing team visited the CGH Inpatient Rehabilitation unit to better understand nursing practices. New initiatives were started, including a walking program to assist stroke patients in the bathroom, in favour of previous commodes or bedpans. The occupational therapists worked on a new set of outcome measures, a fall risk reduction program, a ward-based ADL (activities of daily living) enhancement program and purchase of a H-MAN robotic device (Articares Pte Ltd) for upper limb training. The physiotherapists and therapy assistants conducted adjunct robotic therapy utilising the Andago V2.0 (Hocoma AG, Volketswil, Switzerland) device. The doctors increased the frequency of multidisciplinary meetings from fortnightly to weekly and began providing ultrasound-guided interventions such as botulinum toxin injections for spasticity, as well as injections for musculoskeletal conditions associated with stroke. Specialized stroke rehabilitation care provided by physicians , nursing and allied health members was novel in the community hospital setting.
Referrals to the community hospital were made through a national electronic platform at that time known as the Integrated Referral Management System (IRMS), which required multiple documentary inputs from the different members of the care team. We instead proposed the use of a secured end-to-end texting platform, TigerConnect (TigerConnect Inc) for referrals. As the consultant in charge of the SSW would be from CGH and hence able to review the patient on our hospital’s electronic medical records, the clearance process could be safely truncated, allowing for next-day and even same-day transfers. The proposal to set-up SSW was reviewed for governance and approved by our hospital’s Medical Board.
The SSW commenced operations in October 2019 and an audit was conducted on the patients admitted between Oct 2019 and June 2021. The main purposes of the audit was to assess the functional outcomes, length of stay and the healthcare costs.
Methods
The aim of this study was to evaluate the outcomes of the integrated subacute stroke ward, namely in patient functional outcomes, length of stay and healthcare expenditure as compared with the previous model of care.
Study design and patient population
This retrospective study involved anonymised patient clinical data that was independently extracted by the medical officers working in both units. The baseline data was a convenient sample as it was previously used for another audit. The 2016 data was not yet electronic. Rotating medical officers were trained and supervised by consultants and were unrelated to the study. Data on bed utilization and bill were extracted from electronic medical records and patient billing system. The SACH IT and business office team assisted in data extraction. These are routine data required for national reporting. Extraction methods are standardized and robust.
Two cohorts were included in this study. 1. Stroke rehabilitation patients discharged from SACH between January and June 2016 (control group). These patients were transferred from the CGH Rehabilitation Medicine unit. 2. The patients discharged from the SSW between October 2019 and June 2021 (SSW group).
There were 71 patients in the control group and 226 patients in the SSW cohort. The periods of 2017 and 2018 were not considered in the baseline analysis due to multiple workflow changes in those years. Missing data was deleted pair-wise (i.e., admission and discharge) and no efforts were made to impute missing values.
Outcome measures
We assessed 3 main clusters of outcome measures - functional, financial and length of stay (LOS). Functional outcome measures were the Modified Barthel Index (MBI) and its derivative impact indices - functional gain (FG), rehabilitation efficiency and rehabilitation effectiveness.
The MBI is an established rehabilitation assessment tool for the activity domain with scores ranging from 0 to 100, which is used across community hospitals in Singapore.17,18 The MBI assesses ten ADLs, including personal hygiene, bathing, feeding, toileting, stair climbing, dressing, bladder control, bowel control, ambulation, and transfers. FG is the difference between discharge and admission MBI scores.
Rehabilitation efficiency is the rate of functional recovery during rehabilitation (scaled up to a month for readability), and is calculated as
Rehabilitation effectiveness is defined as the percentage of potential functional improvement achieved with consideration to the ceiling of the functional scale (100 for the MBI), and is calculated as
Financial outcome measures
Hospitalisation cost data was extracted from the CGH and SACH hospital financial databases. Cost analysis was performed from the healthcare provider perspective, which includes direct medical costs incurred during each hospitalisation before the application of government subsidies and insurance claims. Direct medical costs included ward charges, radiology and laboratory fees, physician and specialist consultation fees, medications, consumables, emergency services fees, rehabilitation therapy fees, and other miscellaneous charges.
The data for cost calculations was collected by the bottom-up (micro-costing) method, 20 and all cost data are provided in Singapore Dollars (SGD). All costs for CGH patients were inflated to 2021 Singapore dollars (SGD) for equivalent comparison. The inflation factor was utilised for ward charges and the consumer price index (CPI) for healthcare costing in public health institutions was applied for all other categories. As SACH belongs to a charitable organisation and is autonomous, the inflation factor provided by SACH Finance was applied for costs incurred during the community hospital phase. Direct nonmedical costs such as out-of-pocket expenditures by patients for the purchase of assistive technology and mobility devices, and those related to loss of work productivity, were not included in this study.
The costs of both the control and SSW groups were compared using the direct cost approach and calculated on a per episode basis. Each episode refers to the acute hospital admission which is followed by the community hospital admission. The per-episode costs are summed across the entire LOS across both hospitals.
Statistical analysis
Descriptive statistics were used to tabulate the costs and demographics of the patients from the two cohorts. Numerical data were presented as mean and standard deviation (SD) or median and interquartile range (IQR). Continuous data were analyzed using t-test or Mann-Whitney U test, depending on the distribution of the data. Pearson’s chi-squared test was used to analyze categorical variables. To account for the different sample sizes and potential confounders, multiple linear regression analysis was performed to determine the significant predictors of the total direct medical costs (Supplemental Table 1a) and length of stay (Supplemental Table 1b). Logarithmic transformation was undertaken for total direct medical costs and LOS to reduce skewness, minimize the number of outliers, and improve the normality, linearity, and homoscedasticity of residuals. For a variable to be included in the multiple regression analysis, its F statistic on univariate analysis had to be significant at p < 0.05. The criterion for retention of a variable in the model was p < 0.15.
Subgroup analysis was conducted to assess the impact of the higher proportion of lacunar infarcts (LACIs) in the SSW group. To ensure a more homogeneous comparison between the control and SSW cohorts, hemorrhagic stroke cases were excluded from the analysis (Supplemental Table 2). This involved stratified analysis and adjusted regression models to evaluate whether the disproportionate number of LACIs influenced the outcomes (Supplemental Table 3). Sensitivity analyses were performed to ensure the robustness of our findings. We re-analyzed the data using non-parametric tests and adjusted for potential confounders using multivariate regression models. The results were consistent across these various methods, confirming the reliability of our initial findings.
All tests were two-tailed, and statistical significance was set at p < 0.05. All statistical analyses were conducted using Stata version 16 (StataCorp LP, 173 College Station, TX, USA).
Results
Functional outcomes
Comparison of baseline demographics characteristics, functional assessments, and healthcare utilisation between pre and post cohorts.
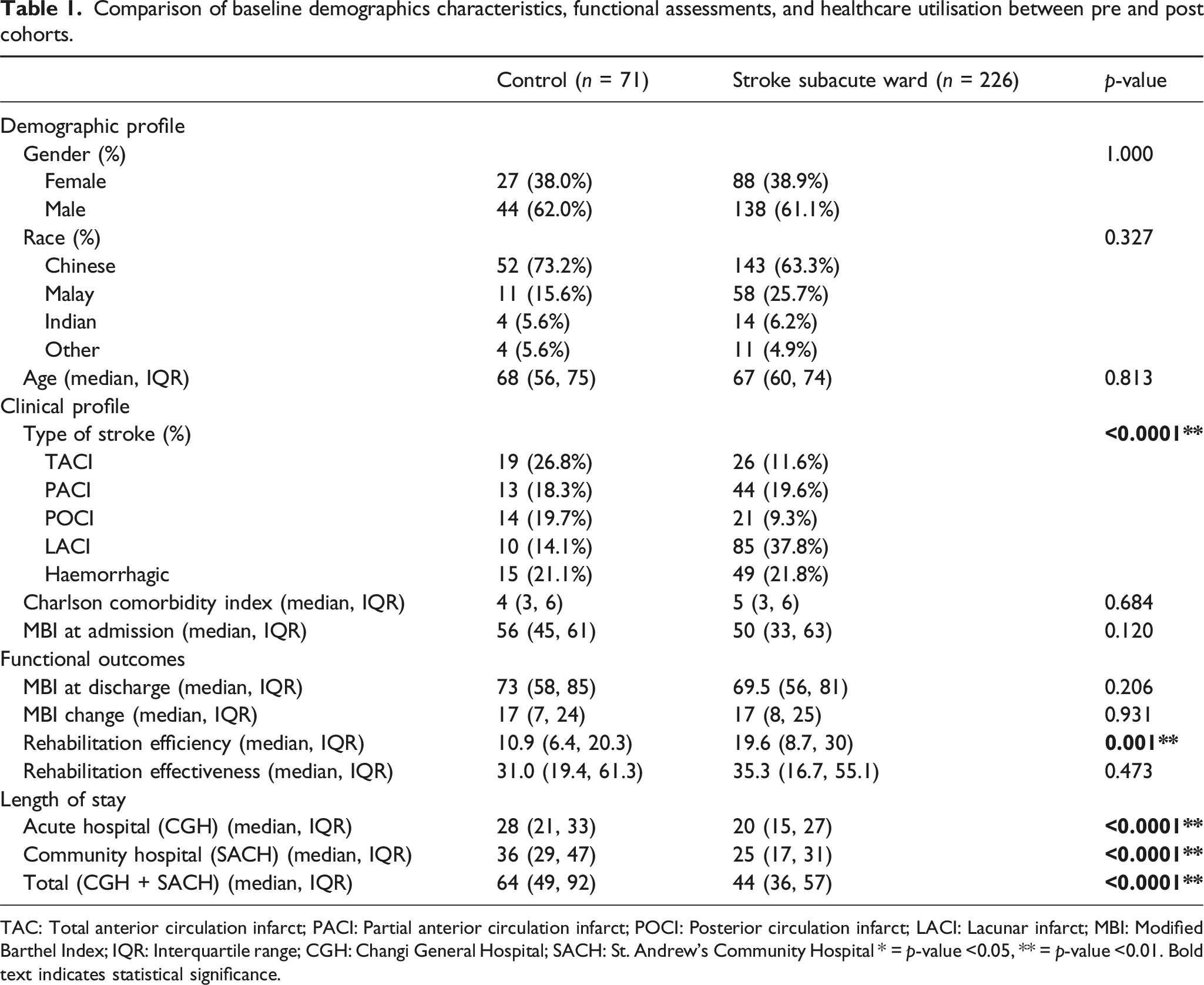
TAC: Total anterior circulation infarct; PACI: Partial anterior circulation infarct; POCI: Posterior circulation infarct; LACI: Lacunar infarct; MBI: Modified Barthel Index; IQR: Interquartile range; CGH: Changi General Hospital; SACH: St. Andrew’s Community Hospital * = p-value <0.05, ** = p-value <0.01. Bold text indicates statistical significance.
There was a significant reduction in the LOS in the community hospital, from a median of 36 (29, 47) to 25 (17, 31) days (p < 0.0001). The LOS in the acute hospital was also reduced from 28 (21, 33) to 20 (15, 27) days (p < 0.0001). There was a total reduction of 20 days in the LOS (p < 0.001) across the whole continuum of care.
Baseline clinical profile and outcome measures by stroke subtype.

TACI: Total anterior circulation infarct; PACI: Partial anterior circulation infarct; POCI: Posterior circulation infarct; LACI: Lacunar infarct; MBI: Modified Barthel Index, * = p-value <0.05, ** = p-value <0.01. Bold text indicates statistical significance.
Outcomes of financial analysis
Comparison of per-episode costs.

CGH: Changi General Hospital; SACH: St. Andrew’s Community Hospital; IQR: Interquartile range; MRI: Magnetic resonance imaging, * = p-value <0.05, ** = p-value <0.01. All costs are reported in Singapore Dollars (S$). Bold text indicates statistical significance.
For SACH, the per-episode total gross bill size was significantly reduced from $20,504 to $13,716 (p < 0.0001), with significant reductions in inpatient treatment, bed charges, and laboratory charges.
The per-episode gross bill size for the entire continuum of care decreased from $40,005 to $31,270, which was statistically significant (p = 0.001).
Discussion
The economic burden of stroke has direct, indirect, and intangible components, with direct cost accounting for 70% of the total, 21 largely determined by the LOS. There have been changes to the systematic approach and funding mechanism of healthcare in Singapore over the past years, with the introduction of Value-based stroke care followed by bundled payments. Bundled payment is also known as episode-based payment, 22 and this can be more complex than the historical fee-for-service reimbursement system (known as diagnostic-related group - DRG). 23 With bundled payment, the funding body makes one lump-sum payment for a package of services provided by multiple providers for a defined episode of care, 24 including inpatient, community hospital, outpatient, and community services. Innovations that have succeeded in lowering the costs of healthcare delivery include improving proper medication prescribing, medication adherence, moving care to lower cost settings and system-wide process improvements. 25 The SSW was the culmination of deliberate engagements between CGH and SACH in a bid to tackle this problem. Having the work processes in place for the SSW laid the foundation to pilot stroke rehabilitation for the One Rehabilitation Framework subsequently. One Rehabilitation Framework seeks to standardise rehabilitation, lower cost and improve patients’ access. Our stakeholders collaborated to pre-emptively implement changes that would result in better outcomes, improve access and lower costs.
Through this collaboration, there have been reductions in healthcare expenditure through shorter LOS and cost savings without compromising functional outcomes. The increased efficiency in care is multifactorial and can be attributed to a change in the referral system, as well as in the model of care. Studies have shown that integrated stroke services can reduce costs. 26 Although CGH is a public healthcare institution and SACH is a private hospital operated by a charity, efforts were made for integration, one of which was the adoption of the same electronic medical record that CGH was using as part of the Singapore Health Services cluster. Sharing a common electronic medical record platform between both institutions facilitate direct access exchange of clinical information critical for referral clearance and patient care. Other forms of integration included joint governance meetings and the availability of specialist inputs from CGH.
Factors Associated with Improved Outcomes: a) Subacute Stroke Ward (SSW) versus General Rehabilitation Ward: SSW was staffed by nurses and therapists trained in stroke rehabilitation care. The historical cohort received care in general rehabilitation wards. The SSW operates with a higher nurse-to-patient ratio (subacute subvented ward) compared to a standard rehabilitation ward. This facilitates activities such as ambulation to the bathroom, reducing reliance on commodes and bedpans. Therapist staffing ratios are comparable between the SSW and rehabilitation wards.
Notably, the 2016 cohort was offered lower limb robotic therapy utilizing a device shared by different wards. Subsequently, new upper and lower limb robotic devices were specifically purchased for the SSW after consultation and cross-training with the CGH team. A patient guided suspension device, Andago®
27
was purchased to increase exercise dosage in the lower limb. A Cochrane review found that patients who received RAGT combined with physiotherapy were more likely to achieve independent walking than those who received physiotherapy alone.
28
The specificity, amount, and intensity of locomotor training determine ambulatory outcomes.
29
Upper limb robotics work on the same principles of repetitive practice.
30
The device purchased was H-man® which involved the patient in upper limb exercises through gamification.
31
As patients would have received robotic therapy in the acute hospital, receiving it in the SSW provides a continuity of treatment. b) Multidisciplinary Care led by a Rehabilitation Physician: The Rehabilitation Physician makes daily clinical rounds and leads weekly multidisciplinary meetings. This model of care facilitates earlier diagnosis and management of stroke complications (e.g., pain syndrome, aphasia, spasticity). The availability of rehabilitation specialist input ensures effective discharge planning and timely transition to outpatient rehabilitation. The historical cohort received care coordinated by a Family Physician with multidisciplinary meetings held bi-weekly during their community hospital stay. c) Streamlined Referral Process: The SSW benefited from a streamlined referral process with defined escalation protocols. A shared electronic medical record platform between institutions facilitated efficient exchange of clinical information for referral clearance and patient care. The historical cohort relied on the national IRMS, which though comprehensive, was time-consuming and involved duplicate data entry for the referring institution
In our audit, there were savings in both institutions for the treatment cost and bed cost due to the reduced length of stay. The increased cost of laboratory investigations could be due to the need to complete the work-up for aetiology and other medical issues thoroughly before sending the patient to the SSW. Service cost at CGH increased in the SSW cohort and could be due to the increased intensity of therapy as additional exercise groups were implemented in 2019. This was likely contributed by the use of robotics as well. At SACH, bed and treatment charges were significantly reduced, reflecting the reduced LOS. The cost of laboratory investigations had fallen significantly in the community hospital phase, suggesting that patients were more stable with fewer medical complications arising from this initiative.
Local studies suggest that factors associated with functional improvement in the community hospital setting include a younger age, a higher admission MBI, and a musculoskeletal diagnosis. 18 A diagnosis of stroke reduces the odds of functional improvement 32 and medical complications and functional dependence were correlated with a longer stay. 33 Correlation analysis revealed a similar trend in our patients for admission MBI and healthcare expenditure, with a lower admission MBI correlated with higher LOS and healthcare expenditure (Supplemental Tables). Compared with the historical functional outcomes for stroke patients in community hospitals, 18 the rehabilitation efficiency in both cohorts was higher. However, these studies18,32,33 were carried out in different time periods. It has been previously proven by a study in Hong Kong that, 12 functional outcomes in stroke rehabilitation can vary between different community hospitals within the same country. In a previous local study, trade-offs between rehabilitation efficiency and effectiveness was discussed. 34 It was found that when the length of stay increased, the rehabilitation effectiveness (potential achieved) increased but efficiency will decrease. In our study, although the length of stay decreased, both the rehabilitation efficiency and effectiveness were higher in the SSW cohort as compared with this historical national study. As previously detailed, several factors contributed to the enhanced outcomes observed in the SSW. The improved rehabilitation efficiency and effectiveness are likely attributable to these factors.
In a study by a London-based hospital found that early inpatient discharge to community-based rehabilitation was unlikely to result in overall healthcare savings, but could release capacity for an expansion in stroke caseload. 35 The community hospital is a bridge for the continuity of rehabilitation in the community, such as home-based or centre-based therapy services in our local context. Stroke is a heterogeneous disease, and patients can have complex rehabilitation needs. As such, directly discharging patients to home from the acute hospital can raise concerns regarding the lack of transitional care plans. 36
Due to the higher throughput of patients, the institutions’ capacity to handle more patients with other rehabilitation diagnoses also increases and may lead to higher access to equitable care.
Limitations
This study ended with community hospital discharge, and no further data were collected at the 6-month or 1-year time points to assess longer term functional outcomes. Mortality rates were not captured for comparison due to the short follow-up period and setting of the study. Functional outcomes were not further categorised by severity due to the relatively small number. The design of the SSW is unique, and the outcomes may not be readily generalisable. The actual inflation of services in the acute hospital other than ward charges was applied using the consumer price index provided by the health ministry, which could not be itemised.
Conclusions
Funding mechanisms and healthcare changes are inevitable, and negotiation of the waves of change often requires openness and integration of care between different healthcare providers. The setting up of the SSW achieved savings in healthcare expenditure and LOS without compromising functional outcomes. The community hospital is a potent bridge for care transition and integrated services such as the SSW can optimise the rehabilitation journey for patients with stroke. Innovation in care provision can help to address the ever-changing challenges of healthcare. Further work could include qualitative research surrounding the satisfaction of both patients and healthcare providers on integrated services.
Supplemental Material
Supplemental Material - An integrated subacute stroke ward within a community hospital increases rehabilitation efficiency and reduces healthcare expenditure
Supplemental Material for An integrated subacute stroke ward within a community hospital increases rehabilitation efficiency and reduces healthcare expenditure by San San Tay, Teck Kheng Edward Goh, Mon Hnin Tun, Edmund Jin Rui Neo and Onn Kei Angel in Proceedings of Singapore Healthcare
Footnotes
Acknowledgments
The authors thank the CEOs of CGH and SACH for their support in this collaboration and study, the finance departments of CGH and SACH, Dr Kwok Kah Meng, and Dr Mark Tan, CGH CTRU for their support.
Author contributions
Tay S.S. conceptualised, obtained de-identified data, wrote first draft and reviewed manuscript. Neo J.R.E. performed data analysis and reviewed manuscript. Tun M.N. performed data analysis. Lee O.K.A. and Goh T.K.E. reviewed and approved of final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.