
Abstract
Background
Patients with advanced cancer have poor quality of life and high utilisation of acute healthcare services. Early access to palliative care has been shown to improve quality of life as well as reduce acute healthcare utilisation and costs.
Objectives
To determine the prevalence and timing of hospital-based specialist palliative care reviews for patients with advanced cancer known to National Cancer Centre Singapore. We also explored the association between specialist palliative care review and place of death.
Methods
A retrospective study of patients with Stage 4 cancer who died in a 2-year period from 1 January 2016 to 31 December 2017 (regardless of their date of diagnosis) and who received treatment in National Cancer Centre Singapore (NCCS).
Results
A total of 2572 patients were included, of which 1226 (47.7%) had at least one inpatient or outpatient specialist palliative care consultation. Those who had their first specialist palliative care review 30 days or less before death had a 2.01 (95% CI 1.62 to 2.49, p < 0.001) increased odds of hospital death while those who had the first hospital-based palliative care review more than 30 days before death a 0.76 (95% CI 0.62 to 0.93, p = 0.009) reduced odds of hospital death.
Conclusions
Our study found inadequate and late access to specialist palliative care among advanced cancer patients. Furthermore, late access to specialist palliative care was associated with hospital death. There is an urgent need to improve access to specialist palliative care in order to improve patient outcomes.
Introduction
Advanced cancer patients have poor quality of life and high utilisation of acute healthcare services. Specialist palliative care improves quality of life of patients with advanced cancers and their caregivers, as well as reduces acute healthcare utilisation and costs by these patients.1-10 Patients who have access to specialist palliative care may also be able to spend their last days at home, if that is their preferred place of death. In a Death Attitudes Survey conducted in 2014, 77% of Singaporeans expressed their wish to die at home. 11 However, majority of deaths in Singapore still occur in hospitals – out of 21,446 deaths in 2019, 13,340 (62.2%) occurred in hospitals and only 4913 (22.9%) occurred at home. 12 There is a paucity of local data on the association of access to specialist palliative care and place of death.13-15
Both the American Society for Clinical Oncology (ASCO) and the European Society for Medical Oncology (ESMO) recommend that all advanced cancer patients should receive dedicated supportive and palliative care from the time of diagnosis. 16,17 Yet international data suggests that specialist palliative care is delivered to a minority of advanced cancer patients and very late in the illness trajectory in the period just before death.18,19 With the ageing population in Singapore and increasing risk of cancer with increasing age, the number of people being diagnosed and living with cancer is set to rise. 20 This translates to an escalating need for specialist palliative care services. Although there have been efforts to increase the service capacity, the extent to which advanced cancer patients have access to timely specialist palliative care is largely unknown.
The aim of this retrospective mortality cohort study was to determine the prevalence and timing of specialist palliative care review by the hospital-based team for advanced cancer patients, and explore the sociodemographic and clinical factors associated with whether or not a person received specialist palliative care. As death occurring in hospital is generally recognized as an undesirable outcome, we also explored the association between receipt of specialist palliative care and place of death, adjusted for known factors associated with death occurring in hospital instead of home or inpatient hospice.13-15
Methods
This was a retrospective study of all patients with Stage 4 solid organ malignancies who died in a 2-year period from 1 January 2016 to 31 December 2017 (regardless of their date of diagnosis) and who received treatment in National Cancer Center Singapore (NCCS). Ethical approval and waiver of informed consent for this study was obtained from the Singhealth Centralised Institutional Review Board (CIRB Ref: 2018/2324).
Demographic characteristics, clinical characteristics and hospital-based specialist palliative care services utilization (both inpatient and outpatient clinic consultation) were extracted from an existing database of patients in NCCS. Patients’ date of death, cause of death and place of death were obtained from Singapore Registry of Births and Deaths.
Continuous variables were summarized using median and range. Categorical variables were summarized using frequencies and percentages. Demographics, clinical characteristics and end-of-life outcomes were compared between patients who were referred to specialist palliative care services and patients who were not referred to specialist palliative care services using the Wilcoxon rank-sum test (for continuous variables), chi-squared test (for categorical variables) or Fisher’s exact test (for categorical variables with at least one expected cell count of less than 5). Univariable and multivariable logistic regression analyses were performed to identify factors associated with hospital or non-hospital death. A 2-sided p-value of less than 0.05 was taken was statistically significant. All analyses were performed in Stata 16.0 (StataCorp, College Station, Texas, USA).
Results
A total of 2823 patients met the inclusion criteria, of which 251 (8.9%) patients were excluded due to missing demographic or diagnosis data (diagnosis date or staging). Therefore, a total of 2572 patients were included in the analysis. Forty-six patients had 2 diagnoses of different Stage 4 cancers in the dataset. For these patients, the later diagnosis was used. One patient had 2 diagnoses of Stage 4 breast and lower gastrointestinal cancers with the same diagnosis date. This patient was categorized as having ‘Multiple’ primary sites.
Of the 2572 included patients, 1226 (47.7%) had at least one inpatient or outpatient specialist palliative care consultation. The median time from first specialist palliative review to death was 29 days (IQR: 8–93 days). The place of death was missing for 36 patients. Of the remaining 1190 patients, 680 died in hospital and 510 had a non-hospital death. There was a significant difference in the time from first review to death by location of death (hospital death: median 16.5 days IQR 4–67 days vs non-hospital death: median 49 days IQR 21–123 days, p < 0.001).
Demographics and clinical characteristics.

Note: p-value for pay class excludes ‘Missing’ observations. p-value for primary cancer site excludes ‘Multiple’ and ‘Unknown’ categories.
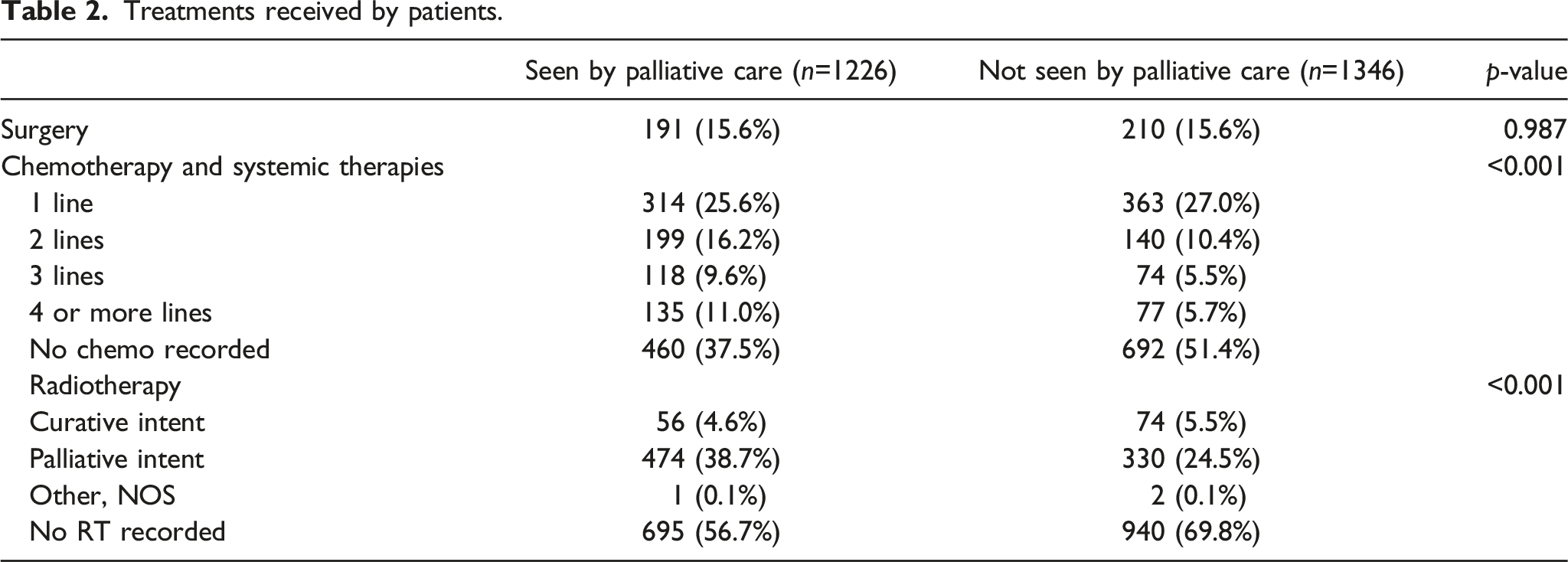
Treatments received by patients.
Association between specialist palliative care review and hospital death.

aAfter adjustment for age, gender, race, pay class and primary cancer site.
Discussion
The main findings of this study were that 47.7% of all advanced cancer patients received any form of hospital-based specialist palliative care before death. Those who received earlier specialist palliative care input, with the first palliative care review more than 30 days before death, were less likely to die in hospital.
Even though international guidelines recommend that all advanced cancer patients should receive specialist palliative care from the time of diagnosis, published studies report a much lower percentage of 5–11% of patients who are referred to specialist palliative care services. The higher referral rate of 47.7% in our study sample may be attributed at least in part to the close working relationship between oncologists and specialist palliative care clinicians, with the specialist palliative care service being co-located within the cancer centre. Nonetheless, less than half of the advanced cancer patients in our study received specialist palliative care; furthermore, those who did received specialist palliative care support very late in their illness trajectory. This highlights a gap in care that needs to be addressed urgently.21,22
One possible reason for inadequate and late access to specialist palliative care is that existing care models are resource-intensive and consequently have limited capacity to provide care for large number of cancer patients. 23 Innovative models of care need to be developed, evaluated and implemented, in order to feasibly upscale services and extend the reach of specialist palliative care.24,25 For example, there could be novel ways of integration between oncologists and specialist palliative care providers to utilise limited resources more efficiently and deliver more coordinated palliative care support to advanced cancer patients.26-29 This may involve oncologists providing generalist palliative care for those without complex needs who may not require specialist palliative care.30,31
The second main reason for delayed access to specialist palliative care is the dependence on the referring practices of primary oncologists which vary widely – some refer all patients with advanced cancer while others refer only in the terminal phase of life.32-34 Furthermore, primary oncologists may be reluctant to refer due to stigma or misperceptions of the role of specialist palliative care, leading some centres to consider rebranding themselves as ‘supportive care’ instead of ‘palliative care’. 34-36 Education among oncologists may also increase awareness of the potential benefits of early specialist palliative care involvement in patients with advanced cancer; strategies to build trust and collaboration may also increase the willingness of oncologists to refer patients to specialist palliative care services.26,36-39 Systematic screening or standardized referral criteria may also be used to increase specialist palliative care referrals for advanced cancer patients with unmet palliative care needs.36,40-44
In our study population, we found that being a private patient was associated with higher access to specialist palliative care. It could be that there is higher awareness of palliative care among the more socially and materially affluent, leading to higher utilization of specialist palliative care services.45,46 Further studies to explore the awareness and perceptions of palliative care among the local Singaporeans population may help build a better understanding of how these factors affect access to specialist palliative care. It is perhaps surprising that cancer site was not associated with receipt of specialist palliative care, as some cancer types may carry higher physical and psychological morbidity. However, as this is a mortality cohort with just over half of the patients receiving specialist palliative care 30 days or less before death, there is probably more similarity than difference in palliative care needs across cancer types in the last weeks of life.
When comparing those who received versus did not receive specialist palliative care, more patients among those who received specialist palliative care had also received chemotherapy. The reasons for this observation are unknown. It is possible that those who had chemotherapy had more treatment toxicity that required specialist palliative care review. Furthermore, these patients who had advanced disease and yet were still on chemotherapy could also be navigating between the goals of life prolongation versus quality of life, and more likely to face more complex decision making that could benefit from specialist palliative care support.
Another key finding from our study was that the timing of first specialist palliative care review was associated with place of death, where earlier timing of specialist palliative care is associated with reduced incidence of death occurring in hospital. This may be related to a longer time available to address physical and psychosocial issues that may have otherwise triggered an acute hospital admission in the last days of life prior to death. This finding is congruent with a growing body of evidence that earlier timing of specialist palliative care involvement improves patient outcomes.2-5,47 In the inpatient hospital setting, earlier specialist palliative care review by hospital-based teams is associated with better quality of life and reduced health care cost.10,48,49 In a prospective cohort study of advanced cancer inpatients receiving care from hospital palliative care teams, earlier consultation was associated with a larger effect on cost of hospital stay. 10
Study limitations
A limitation of our study was that we were unable to capture receipt of community hospice services. Some patients may be directly referred by the primary oncologist for home hospice services in the community, without review by the hospital-based specialist palliative care team; however, our clinical experience is that this would occur only in a small number of patients. Another limitation is that we were unable to measure the provision of generalist palliative care by the primary oncologist. However, most patients who require specialist palliative care are formally referred and would have been accounted for. Also, we were not able to extract data on symptoms, function or psychosocial factors that may have influenced the referral rates to specialist palliative care services.
In conclusion, our study found inadequate and late access to specialist palliative care among advanced cancer patients. Furthermore, late access to specialist palliative care was associated with hospital death. There is an urgent need to improve access to specialist palliative care in order to improve patient outcomes, perhaps through the development, evaluation and implementation of innovative models of care to feasibly increase the capacity of specialist palliative care services. Further studies could explore other quality measures of end-of-life care such as the occurrence and documentation of advance care planning conversations; documentation of ‘do not resuscitate’ orders; aggressiveness of end-of-life as indicated by chemotherapy or ICU admissions in the last weeks of life.
Footnotes
Acknowledgements
We would like to thank Audrey Koh for assistance with data extraction.
Author contributions
GMY obtained funding for this research project. CL was conducted data analysis. All authors contributed to the study design and data interpretation, critically reviewed and revised the manuscript, approved the final manuscript for submission, and participated sufficiently to take responsibility for the content of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the SingHealth RHS PULSES Centre Grant (CGFeb18S01)
Informed consent
This study was granted waiver of informed consent by the SingHealth Centralised Institutional Review Board.
Ethical approval
Ethical approval for this study was obtained from the Singhealth Centralised Institutional Review Board (CIRB Ref: 2018/2324).
Data availability
The datasets generated and analysed during the current study are available from the corresponding author.