
Abstract
Background
As the global population ages, the prevalence of dementia increases, and the need for healthcare services increases. Healthcare workers should possess necessary knowledge and appropriate attitudes to care for dementia patients.
Objectives
There is a lack of studies of dementia knowledge and attitudes of healthcare workers in post-acute and intermediate care settings. Our study aims to address this gap and evaluate factors associated with dementia knowledge and attitudes in community hospitals.
Methods
Eligible healthcare workers from three community hospitals in Singapore were invited to fill in anonymous, self-administered questionnaires consisting of sociodemographic, work or training-related, assessment of self-competence factors together with Dementia Knowledge Assessment Scale (DKAS) and Approaches to Dementia Questionnaire (ADQ). Univariate analysis followed by multiple linear regression was conducted to determine the association between covariates with DKAS and ADQ scores.
Results
A total of 500 responses were obtained, giving a response rate of 60.2%. Mean DKAS and ADQ scores were 27.8 and 68.4 respectively. Multiple linear regression revealed better dementia knowledge was associated with occupation, highest education level, having attended a dementia training course, experience in caring for dementia patients and self-assessment of dementia knowledge. More positive attitudes towards dementia care were associated with occupation, time spent providing dementia care and self-assessment of attitude towards dementia care.
Conclusion
Healthcare workers in community hospitals exhibit positive attitudes towards providing dementia care but have a lower level of dementia knowledge compared to other study populations. Modifiable factors can be targeted to improve dementia knowledge and attitudes amongst healthcare workers.
Introduction
Due to increased life expectancy and declining birth rates around the world, the prevalence of aging population is up-trending. 1 In 2015, the proportion of the population in most developed countries aged 60 years or older was approximately 10 to 24%; by 2050, it is estimated that this proportion will increase to 20 to 30%. 2 As this occurs, public health issues such as dementia come to the forefront.
Dementia is a neurodegenerative syndrome that leads to a decline in cognitive function beyond what is expected from normal aging. In 2022, approximately 55 million people globally have dementia. 3 It is estimated that the number of people with dementia globally may potentially rise to 152.8 million by 2050. 4
Dementia is one of the main causes of dependence of care and disability in the elderly around the world. 5 By World Health Organization’s Global Health Estimates, dementia is the 25th leading cause of disability adjusted life years (DALYs) at 28.3 million DALYs. 6 In 2020, the estimated annual global cost of dementia was over US$1 trillion and this figure is expected to double by 2030. 7
In 2019, the year before the COVID pandemic, the rate of admission to Singapore hospitals in the 65 & above age group was 345.3 per 1000 resident population and 26.8 per 1000 resident population in the acute and community hospitals respectively. 8 During the pandemic, there was decreased healthcare utilization by patients with chronic disease. 9 The pandemic has also adversely affected the health of patients with dementia – increased risk of contracting COVID with subsequent increased risk of hospitalization 10 ; worsening baseline behavioural and psychological symptoms of dementia (BPSD). 11 This may potentially lead to poor chronic disease control for all patients and the spillover effect of increased hospital admission rates post pandemic. As such, hospitals play a crucial role in providing care for patients with dementia and healthcare workers are at the forefront of providing this care.
In Singapore, community hospitals play an important role in the healthcare ecosystem – focusing on intermediate care. The role of the community hospital is to provide patients with ongoing hospital based care, meet their rehabilitation needs and support their transition back to the home and community. 12 Some of the community hospitals also provide specialized services such as dementia care, palliative care, and complex wound care. 12 The multidisciplinary teams in community hospitals comprise of doctors, nurses, allied health professionals and nursing care support staff.
Current literature indicates that negative attitudes and stigmatization towards dementia can have adverse effects on patients, leading to poorer quality of life and outcomes. 13 Poor level of knowledge and negative attitude towards dementia patients among healthcare workers can lead to caregivers receiving inadequate information on care of the patient as well as increased caregiver stress. 14 Therefore, it is important healthcare workers in community hospitals possess the necessary knowledge and appropriate attitude to provide quality care and support for dementia patients as they may be admitted for many weeks.
To date, studies on dementia knowledge and attitudes have focused on nursing students, 15 medical students, 16 tertiary hospital healthcare workers in China and Ireland,17,18 general practitioners from Germany 19 and other community sector healthcare workers from Australia and China.20,21 There is a lack of studies on dementia knowledge and attitudes of healthcare workers in the post-acute and intermediate care settings. To address this knowledge gap, we conducted a cross-sectional study to assess the level of, as well as evaluate the factors associated with, dementia knowledge and attitudes towards dementia care of healthcare workers in community hospitals. Our study also aims to test the reliability of the Dementia Knowledge Assessment Scale (DKAS) and Approaches to Dementia Questionnaire (ADQ) in Singapore healthcare workers, which hadn’t been validated in previous studies. This was done to ensure these tools could accurately measure dementia knowledge and attitudes among healthcare workers in Singapore community hospitals.
Methods
Measures
Outcomes of interest
Dementia knowledge was assessed using the 25-item DKAS. Items were scored on a five-point Likert scale with true and false statements about dementia: 2 points for answering ‘true’ to a true statement or ‘false’ to a false statement; score 1 point for answering ‘probably true’ to a true statement or ‘probably false’ to a false statement; and score 0 points if you do not meet the criteria above or answered, ‘I don’t know.’ 22 DKAS has a score ranging from 0 to 50. Higher DKAS scores reflect better dementia knowledge. DKAS covers four subscales about dementia: Causes & Characteristics, Communication & Behaviour, Care Considerations, and Risks & Health Promotion. DKAS has been validated in healthcare workers from different countries but not specifically in Singapore. Cronbach’s alpha for DKAS is 0.85. 22 Permission to use DKAS was given by the original authors.
Attitudes towards dementia care was assessed using the 19-item ADQ. Items were scored on a five-point Likert scale that ranges from ‘strongly disagree’ to ‘strongly agree.’ 23 ADQ has a score ranging from 19 to 95. Higher ADQ scores reflect more positive attitudes towards people with dementia. ADQ comprises of two domains: Hope – reflection of pessimism or optimism about the abilities of people with dementia, and Person-Centered – reflection of the extent to which people have a person-centered understanding of dementia. ADQ has been validated in healthcare workers from the United Kingdom with a Cronbach’s alpha of 0.83. 23 Permission to use ADQ was given by the original authors.
Independent variables
The selection of independent variables for this study was based on previous studies that investigated factors associated with dementia knowledge and attitudes towards dementia care amongst healthcare professionals.16–20 These variables are classified into three broad categories: namely sociodemographic, work or training related and self-assessment of competence factors.
Sociodemographic factors included age, gender, occupation, highest educational level and having a family member with dementia. Work or training related factors included working experience in healthcare, having attended a dementia training course, experience in caring for patients with dementia and time spent providing dementia care. Self-assessment of competence factors included dementia knowledge, level of confidence towards providing dementia care and attitude towards providing dementia care.
Study design and population
A pilot was undertaken to assess the reliability of DKAS and ADQ in the Singapore healthcare setting. To assess the content and face validity of DKAS and ADQ, two of the study team members assessed the relevance and comprehensiveness of the questions independently. We then purposively sampled 24 healthcare workers in three community hospitals in Singapore who participated in cognitive debriefing interviews. 24 Based on these interviews, no modifications were required. Participants had to complete the questionnaires on two separate occasions, 2 weeks apart. 25 Written informed consent was obtained from all pilot participants.
After the pilot, we conducted a multi-centre, cross-sectional study in the three community hospitals. We surveyed physicians, nurses, nursing care assistants, rehabilitation therapists, therapy assistants, pharmacists, dietitians, and medical social workers. Only English-speaking healthcare workers, who were 21 years and above, with direct patient contact during their daily work were invited to participate in the study. Healthcare workers who were on leave during the entire period of data collection and those who participated in the pilot were excluded.
Anonymous self-administered questionnaires were distributed to medical, nursing, and allied health leads, who in turn disseminated the surveys to their respective team members. Participants were given the period from 29th July 2022 to 31st August 2022 to complete the survey and were instructed to return the completed forms to sealed opaque boxes located in the wards or offices. Completion of the questionnaires was voluntary. Consent was implied if participants returned a response.
Sample size calculation
We performed a sample size calculation using the finite population sampling formula. With a 95% confidence level and 5% margin of error from a sampling frame of 830 staff and addressing a potential 40% rate 26 of non-response or incomplete data in the questionnaire, a minimum sample size of 439 participants was required.
Data analysis
All analyses were performed using SPSS version 26. Data from the pilot was used to test for internal consistency and test-retest reliability. Results obtained after the pilot, were summarized using descriptive statistics: frequency, mean, standard deviation, coefficients and 95% confidence intervals where applicable. Student t test and Analysis of Variance (ANOVA) were used for univariate analysis as both outcome measures (DKAS and ADQ scores) were parametric. Variables that had significant associations with DKAS or ADQ scores, as well as other variables that were suggested to be important in the literature were included in multiple linear regression analysis. The strength of the associations is presented as coefficients together with a 95% confidence interval. A p-value of <.05 was considered statistically significant.
Results
Pilot – internal consistency and test-retest reliability
The Cronbach’s alpha for the DKAS and ADQ were 0.81 and 0.80 respectively. The intra-class coefficients for the DKAS and ADQ were 0.73 and 0.65 respectively.
Self-administered questionnaire - participants’ characteristics
Baseline characteristics of study participants (N = 500), DKAS and ADQ scores.
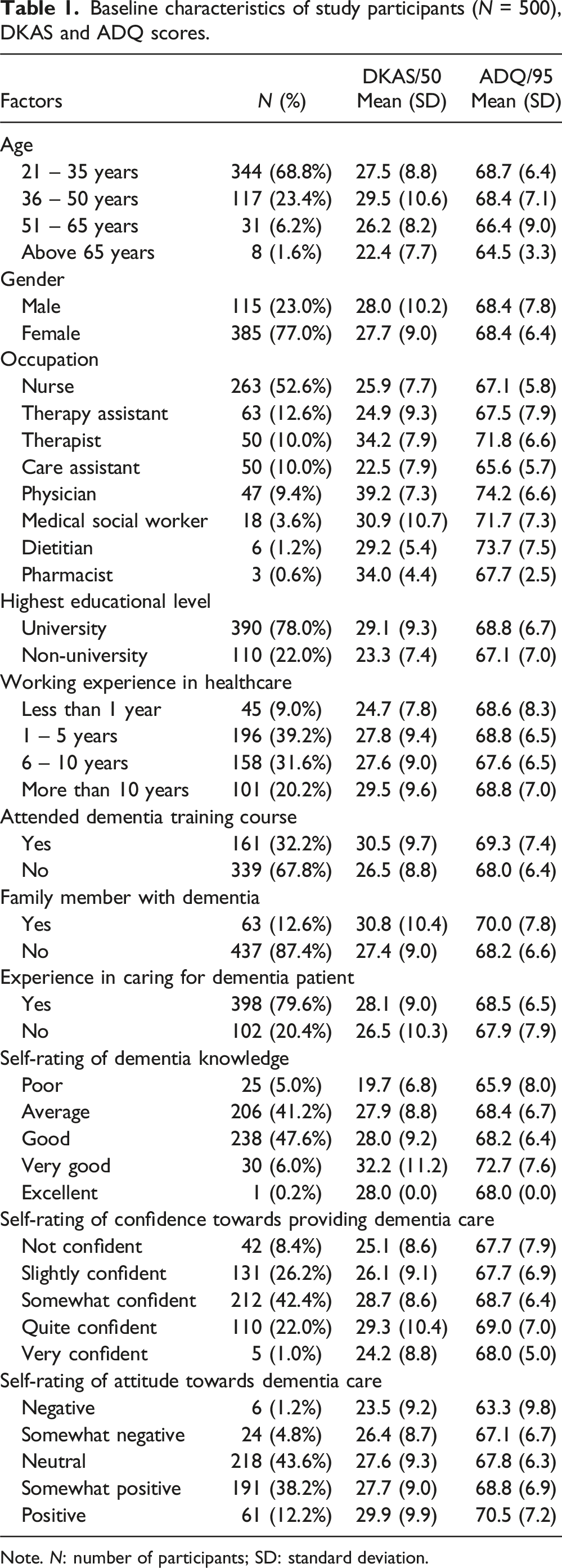
Note. N: number of participants; SD: standard deviation.
Dementia knowledge
Descriptives
The DKAS scores are reported in Table 1. The mean DKAS score of the participants is 27.8 ± 9.3 out of 50. Physicians, therapists, pharmacists, and medical social workers have higher DKAS scores compared to the other professions. Higher DKAS scores are observed in participants who have a family member with dementia, graduated from university or previously attended a dementia training course.
DKAS subscale scores of study participants.

Note. SD: standard deviation.
Association between independent variables and dementia knowledge
Univariate analysis between covariates and DKAS score.

Note. B: unstandardized coefficient; 95% CI: 95% confidence interval; Ref.: reference.
Multiple linear regression of covariates and DKAS score.

Note. Ref.: reference; regression statistics: Adjusted R2 = 0.31, F (19,480) = 12.51, p <.001.
Attitudes towards dementia care
Descriptives
The ADQ scores are reported in Table 1. The mean ADQ score of the participants is 68.4 ± 6.8 out of 95. Physicians, dietitians, therapists, and medical social workers have higher ADQ scores compared to the others. Interestingly, having a family member with dementia or having experience in caring for patients with dementia does not translate to a higher ADQ score.
ADQ subscale scores of study participants.

Note. SD: standard deviation.
Association between independent variables and attitude towards dementia care
Univariate analysis between covariates and ADQ score.

Note. B: unstandardized coefficient; 95% CI: 95% confidence interval; Ref.: reference.
Multiple linear regression of covariates and ADQ score.

Note. Ref.: reference; regression statistics: adjusted R2 = 0.17, F (13,486) = 8.74, p <.001.
Discussion
For our pilot, the reported Cronbach’s alpha of 0.81 (DKAS) and 0.80 (ADQ) are comparable to the original studies (DKAS: 0.85, 22 ADQ: 0.83 23 ). The reported intra-class coefficients of 0.73 (DKAS) and 0.65 (ADQ) demonstrate moderate reliability 27 but are slightly lower compared to the original studies (DKAS: 0.80, 28 ADQ: 0.70 23 ). The difference in intra-class coefficient scores between our pilot and other studies could possibly be due to the small sample size in the pilot. Overall, the pilot results indicate that DKAS and ADQ are suitable to be used to measure dementia knowledge and attitudes in Singapore healthcare workers.
Overall, our study demonstrates community hospital healthcare workers have a lower level of dementia knowledge compared to previous studies.21,22 Despite having a lower level of dementia knowledge, they exhibit positive attitude towards providing dementia care.
Community hospital healthcare workers’ knowledge of dementia
Our community hospital healthcare workers have a mean DKAS score of 27.8 out of 50. This is a lower score compared to other research findings in various settings, namely the Australian health workforce from hospitals, aged care facilities, community service providers (mean DKAS score: 44.9 out of 54 – using an earlier version of the DKAS) 21 and healthcare workers from different countries participating in an online dementia education course (mean DKAS scores prior to completing the online course: ranging from 36.9 to 37.9 out of 50). 22
More specifically, our community hospital staff scored lower in the Causes & Characteristics, Communication & Behaviours and Care Considerations subscales and higher in the Risks & Health Promotion subscale compared to the international cohort of healthcare workers. 22 One particular reason for the higher Risks & Health Promotion subscale score could be related to Singapore’s ‘Healthy Living Master Plan’ which focuses on creating awareness for healthy living amongst the population, 29 with initiatives such as the National Step Challenge™ which encourages people to engage in more physical activity. 30 Particularly, our community hospital staff scored less than 50% in the Communication & Behaviours and Care Considerations subscales. This could be explained due to operational requirements: During the cross-sectional study, one of the community hospitals involved in the study functioned as a COVID-19 pandemic hospital – providing care for COVID-19 patients; The other two community hospitals involved in the study have one dementia ward each. The resultant reduced clinical exposure to patients with dementia could have contributed to the lower DKAS subscale scores. Additionally, our study found positive associations between staff with experience in caring for dementia patients and DKAS scores.
Interestingly, physicians, therapists and medical social workers were found to be significantly associated with higher DKAS scores. These professions also scored higher in the Communication & Behaviours and Care Considerations subscales compared to the rest. This is possibly due to the type of training they underwent during their undergraduate years and the quality of clinical exposure to patients with dementia – physicians conducting comprehensive geriatric assessments 31 ; therapists conducting therapy sessions; medical social workers spending time to understand the life story of their dementia patients. Our study result adds information to the existing literature on the impact of profession on dementia knowledge: other studies that focused on doctors and nurses 17 or did not find any significant difference in dementia knowledge levels amongst different professions (medical, nursing, allied health). 21
Our study also found that staff who have better self-reported dementia knowledge or completed university qualifications have a higher DKAS score compared to others, which is similar to the findings in the Australian health workforce study. 21 This shows the link between educational achievement and knowledge. Another significant positive association is staff who attended dementia training scored higher DKAS scores. This is similar to the findings in other studies16,32 and highlights the importance of dementia specific training on dementia knowledge, which could consequently improve dementia care standards. 14
Community hospital healthcare workers’ attitudes towards dementia care
Our community hospital healthcare workers exhibit a positive attitude towards providing dementia care, with a mean ADQ score of 68.4 out of 95. This score is comparable to other research findings, such as Irish acute hospitals (mean ADQ score: 70.6), 18 Korean acute hospitals (mean ADQ score: 71.4) 33 and Norwegian nursing homes and hospital-based geriatric ward (mean ADQ score: 70.4). 34 Our study found a generally higher Person-Centered subscale which is similar with previous research.18,33,34
Certain professions such as therapists, medical social workers, dietitians, and physicians were found to be significantly associated with higher ADQ scores. This result could be related to the training for each profession as well as each professions’ clinical exposure to dementia patients. Our study result adds information to the literature on the impact of profession on attitudes towards dementia care: most studies did not report any significant associations between professions and dementia attitudes.
An interesting predictor of attitudes towards dementia care in our study is the self-assessment of attitudes towards dementia care – positive self-assessment is associated with higher ADQ scores. This result can possibly be explained by the theory of planned behaviour which states that perceived behavioural control (how much a person believes that he/she can perform a certain behaviour) affects the outcome of the actual behaviour. 35 Previous research findings have demonstrated negative attitude towards dementia patients among healthcare workers can lead to increased caregiver stress due to not receiving appropriate support. 14 This can potentially affect the level of care that the dementia patient receives, potentially leading to poor care outcomes.
In our study, time spent providing dementia care is positively associated with higher ADQ scores, which is similar to the findings documented in a United Kingdom study. 36 This is different from the findings of a study conducted in caregivers of people with dementia, which found that increased time spent with a person with dementia led to increased caregiver burden and stress. 37 The difference in results could be explained by the differing roles of the healthcare worker (providing care during working hours whilst the dementia patient is admitted in hospital) versus the caregiver (providing care to their person with dementia up to 24 h per day, 7 days per week).
Strengths and limitations
To our knowledge, this is the first study conducted to validate the use of DKAS and ADQ in Singapore healthcare workers. It is also the first study in community hospitals assessing staffs’ dementia knowledge and attitude towards providing dementia care and provides valuable insights into the potential predictors that influence dementia knowledge and attitudes.
However, some limitations were identified in this study. In our pilot, participants were purposively sampled which may have introduced selection bias. The 2-week interval might introduce bias due to participants remembering their initial responses or experiencing changes in their knowledge or attitudes within that short period.
In our main study phase, the cross-sectional design limits the ability to establish causality between the predictive factors and dementia knowledge or attitudes. Additionally, as a self-administered survey, it was prone to self-reporting bias, where participants might have referred to external sources while completing the questionnaire, potentially inflating the mean scores. Even though the response rate is 60.2%, there could be potential non-response bias, where the survey results don’t fully represent the views or experiences of the entire target population. Also, the study was conducted in only three community hospitals in Singapore, limiting the generalizability of the findings.
Conclusion and implications
DKAS and ADQ are suitable outcome measures to assess dementia knowledge and attitudes in Singapore healthcare workers. This study contributes to the knowledge of the levels of dementia knowledge and attitudes towards dementia care among healthcare workers in community hospitals. It also adds to the understanding of the factors associated with dementia knowledge and attitudes towards dementia care.
Modifiable factors can be targeted to improve dementia knowledge and attitudes amongst healthcare workers. Based on the study findings, one strategy is to conduct dementia training for all healthcare workers in the community hospitals, not only those that work in the dementia ward. As the different healthcare professions in the community hospitals have differing levels of dementia knowledge, further needs analysis can be conducted to identify their knowledge gaps and lead to creation of education material tailored to the different needs.
Another strategy is to allow for healthcare workers to be given opportunities to gain experience and spend more time managing patients with dementia. Organization leaders in the community hospitals play an important role in building a positive culture towards care of dementia patients, providing adequate support to staff in managing patients with dementia.
Footnotes
Acknowledgements
The authors would like to acknowledge the study participants who generously shared their time and insights.
Author contributions
WH was the principal investigator, conducted the literature review, designed the methodology, conducted the pilot phase and survey phase at one of the study sites, conducted all data analyses and prepared the manuscript. JHL conducted the literature review, conducted the pilot, was the site investigator of one of the study sites and reviewed the draft manuscript. GGWY was one of two reviewers who assessed the DKAS and ADQ for content and face validity, was the site investigator of one of the study sites and reviewed the draft manuscript. CQHC was one of two reviewers who assessed the DKAS and ADQ for content and face validity and reviewed the draft manuscript. LLL provided expert advice for the study design and edited the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.