
Abstract
Aim
The aim of this study was to describe the patients’ perception regarding their experiences of ward rounds during hospitalisation.
Background
Ward round facilitates many activities during hospitalisation, most importantly serving as a communication channel between patients and physicians for shared decision-making and information exchange. The quality of ward rounds can affect patients’ satisfaction levels and their eventual health outcomes.
Method
A cross-sectional study using questionnaires was conducted to examine the organisation, structure and delivery of ward rounds among 527 adult inpatients and/or caregivers of paediatric patients. Patient satisfaction levels were calculated by aggregating individual ratings, which were then evaluated based on gender, age group and ward type. Statistical analyses were evaluated using One-way Anova test, with statistical significance considered at p ≤ 0.05, which was evaluated based on gender, age group and ward type.
Results
Majority of patients found the ward rounds’ duration (86.6%) and timing (88.4%) suitable. Poor patient satisfaction was related to not informing patient or family on plans for discharge, provide necessary information on test and procedures and giving opportunities to raise questions or concerns. Patient satisfaction was associated with age groups (p < 0.001, n2 = 0.069) and ward types (p = 0.001, n2 = 0.031). 58% of patients expressed a preference for nurse participation during ward rounds.
Conclusion
Whilst the organisational and structural aspects were satisfactory, the conduct of ward rounds requires enhancement. The disparate experiences across patient age groups and ward types highlight a need for more homogenized care delivery. Healthcare providers and administrators should prioritise understanding patient preferences and values, whilst fostering health literacy to optimise patient outcomes.
Implications for nursing management
The findings suggest that patients prefer the presence of nurses during ward rounds. Further research can potentiate and evaluate strategies on nurses’ role and participation during ward rounds.
Keywords
Existing literature (what is known)
- Ward round is a quintessential activity allowing the interdisciplinary team to review and formulate patient’s treatment plan. - It serves as an important platform for patients to communicate with the team and be actively involved in their own care. - The available literature is mostly focused on fulfilling pertinent outcomes during ward rounds, with limited quantitative data on patient’s satisfaction and experience.
Clinical impact (what is new)
- First quantitative study evaluating patient experience and satisfaction of ward rounds conducted in several Singapore hospitals - Majority of patients preferred their families and ward nurses to be present during ward rounds. - Caregivers for patients above 50 years old and patients in lower ward classes were least satisfied with ward rounds - There is a lack of awareness among patients on when the ward rounds will be conducted and what to expect of ward rounds - Findings show that the conduct of ward rounds requires further improvement in helping patients to understand and be involved in their treatment
Clinical implications
- Helps healthcare professionals in understanding what patients value and how to improve patient-healthcare professional interaction - Shared decision making with patients and family members can improve patient care and satisfaction - Nursing’s role and active participation during ward rounds needs to be ameliorated
Introduction
Ward rounds is the cornerstone of all activities during patients’ hospitalization. 1 It provides patients with an opportunity to discuss their symptoms, progress, and concerns with their healthcare providers.1,2 Ward rounds may also facilitate multi-disciplinary communication and involvement in patient care, 2 while allowing physicians to conduct clinical examinations on their patients, review treatment options and formulate discharge plans.3–5 Furthermore, it also serves as a platform for shared decision making and exchange of information amongst the healthcare team, patients and their families. 5 Shared decision making can be described as firstly, the patient or caregiver being provided with accurate information, following which the patient or caregiver can use this information to actively communicate their goals and participate in their treatment decisions. 5 It has been reported that patients’ expressed appreciation and enhanced well-being when they are actively involved in their care, thereby facilitating the knowledge of their own medical condition and eventual adherence to treatment. 5
The Ministry of Health (MOH, Singapore) conducted a Patient Experience Survey in the year 2018 and 2019 to measure inpatient experience among public healthcare institutions. Based on the results and the secondary analysis of inpatient feedback from Singhealth institutions, the pertinent aspects highlighted were patient’s satisfaction and experience related to ward rounds.
Background
Multiple guidelines and expert opinions on systematically reviewing patients, maximising learning,6,7 patient outcomes8,9 and being time-efficient8,9 on ward rounds are available. However, there is minimal literature available on patient satisfaction and experience within the expert guidelines. Most studies exploring both patients’ and healthcare professionals’ experiences7,10–13 to ward rounds are qualitative in nature.
Patients’ satisfaction with ward rounds
Patient satisfaction related to ward rounds are often primarily focused on empathy, communication and patient involvement. Showing empathy and care by physicians taking time to listen was found to be one of the most important factors. 5 Two-way communication that allows for clarifications and discussions on further treatment plans allows for patient involvement. These factors were found to be most important across literature. 5
The duration of ward rounds is a major influencing factor in patient satisfaction during hospitalisation. Inadequate time allocated to ward rounds was associated with poorer patient-perceived quality of care. This was subsequently found to be associated with lowest levels of patient satisfaction when compared to the associated environment, service and frequency in relation to ward rounds. 14 A study assessing the duration of ward rounds revealed that the average time spent per patient was only 12 min, 4 which may be insufficient if it was meant to cover the conduct of clinical examinations, education and patient-physician communication.
Patients’ participation and experience in ward rounds
Participation of patients in the management of their own care is imperative, but this requires patients to understand healthcare processes. Ward rounds provide opportunities for the team to discuss with the patient and their families on their medical management to improve health literacy. 15 This allows for improved communication and better comprehension, supporting shared management which ultimately can promote patient involvement. 15
Physicians should avoid the use of medical terminology during ward rounds, as hearing unfamiliar medical terms can potentially make patients increasingly anxious about their condition. 16 Clear understanding of information with regards to patients’ own diagnostic, management and treatment processes is important in the successful navigation of their treatment journey.17,18 Patients are incapable of undertaking the necessary actions for their health or make appropriate health choices if they do not understand health information. Similarly, patients are less likely to participate in the management of their care due to lack of comprehension. In addition to minimising the usage of medical terminology, patients’ health literacy can be further improved when they are given a platform or opportunity to clarify and ask questions. Redley et al. (2009) observed that patients were invited for questions in just 43% of 113 ward rounds, while technical medical terms were used in more than 60%. Patient care preference and shared decision making were only elicited in 6.7% and 23% of ward rounds respectively.
The presence of other patients in multi-bedded wards can also pose as an obstacle in patient communication. Privacy has been shown to be highly valued by patients, and they are more likely to share information when confidentiality can be maintained 15 or placed in a single-bedded ward. 3 In addition, overpopulated ward rounds can be intimidating for patients due to the presence of several medical students or junior doctors. 3 This may require physicians to return for an individual bedside discussion and explanation. 1 It is apparent that the lack of privacy can be detrimental to patients’ well-being and self-perceived quality of care.
Limitations in current literature
Whilst numerous guidelines and expert recommendations exist for conducting systematic, educational and time-efficient ward rounds, there remains a notable gap in literature regarding patient satisfaction and experience. The available evidence primarily comprises of qualitative studies examining the perspectives of both patients and healthcare professionals, with limited quantitative research in this domain. Existing literature are primarily based in countries of western culture. Patients’ experiences of ward rounds can differ considerably, especially given the cultural differences in ways of expression and healthcare professional-patient relationships. Individual factors such as upbringing, mindset, and education level can also influence a patient’s perception of their ward round experience. 14 Singapore has a diverse population with four resident ethnicities. As such, the impact of cultural values and health-related practices must be considered when looking into the local patients’ experiences of ward round. The language spoken by the healthcare provider and non-English speaking elderly may differ as well. With the approaching silver tsunami, it is crucial to acknowledge potential cultural and language barriers that can impact hospital-based activities such as ward rounds. Current literature also focuses more on the qualitative aspect of patients’ experience in ward rounds.11–13 Such data may not be generalisable to the local population, especially given the cultural values, practices and language differences. As such, this study aimed to better capture, understand, and describe a larger population of patients’ perception on ward rounds in Singapore hospitals. Results of this study will help to inform future ward round practices aimed at improving patient experience.
Aim
This study aimed to examine patients’ or their caregivers (for paediatric patients) experience of ward rounds during hospitalisation.
Design
Methods
Study design
A cross-sectional study was conducted across five healthcare facilities in Singapore to allow heterogeneity within a general cohort. The five facilities consist of a tertiary hospital, two general hospitals, one specialised hospital for women and children, and one cardiac specialty care centre with inpatient facilities. A cohort of 527 adult inpatients (N= 477, 90.5%) and caregivers (N= 50, 9.5%) were surveyed in the month of September 2021. Convenience sampling was adopted with the following inclusion criteria: inpatients admitted for at least a day and have experienced a ward round. Patients who are illiterate or suffer from cognitive impairment were excluded. The study followed the STROBE guideline for reporting cross-sectional studies.
Data collection
A questionnaire was developed to quantify and examine patients’ experiences of ward rounds in an acute inpatient context. The questionnaire was designed from pertinent aspects based off The Ministry of Health Patient Experience Survey and from literature review, focusing on the following aspects: the organization, structure and conduct of ward rounds. The questionnaire was assessed for face validity by a panel consisting of chief nurses and senior physicians.
Data collection took place in the month of September 2021. The questionnaire consisted of 17 close-ended questions categorised into three domains. The questions elicited responses to timing, predictability, and duration of word rounds (domain 1—4 questions), satisfaction with the conduct, language used, opportunity for questions (domain 2—11 questions) and preferences for ward round members composition (domain 3—3 questions). The questionnaire was self-administered or facilitated by ward nurses (for patients who preferred to complete the survey verbally), and was made available in English, Mandarin and Malay languages. Patients or their caregivers (for paediatrics) can choose to answer a paper copy survey form or via an online digital platform.
Data analysis
Descriptive statistics were used to summarise the data. Questions related to satisfaction on structure and conduct of ward rounds were allocated values from 0 to 5 (Don’t know = 0, Poor = 1, Fair = 2, Good = 3, Very good = 4, Excellent = 5). The values were summed to obtain each patients’ level of satisfaction in terms of their ward round experience. Statistical analyses were conducted using Statistical Package for the Social Sciences version 26 (IBM, Chicago, IL). Descriptive statistics was used to compare satisfaction scores in relation to demographic data. Comparison between each patient related categories such as gender, age and ward types, in relation to patients’ level of satisfaction was evaluated using one-way Anova. Statistical significance was considered at p ≤ 0.05.
Results
Patient characteristics
One- way Anova test comparing patient satisfaction score across patient demographics.

*significant when p < 0.05.
0.01 ≤ n2 ≥ 0.06: small to medium effect where satisfaction score was affected by the ward type.
n2 ≥ 0.06: medium effect where satisfaction score was affected by the age group.
Timing, predictability and duration of ward round
Patient/Caregiver feedback on ward rounds duration, timing and predictability.
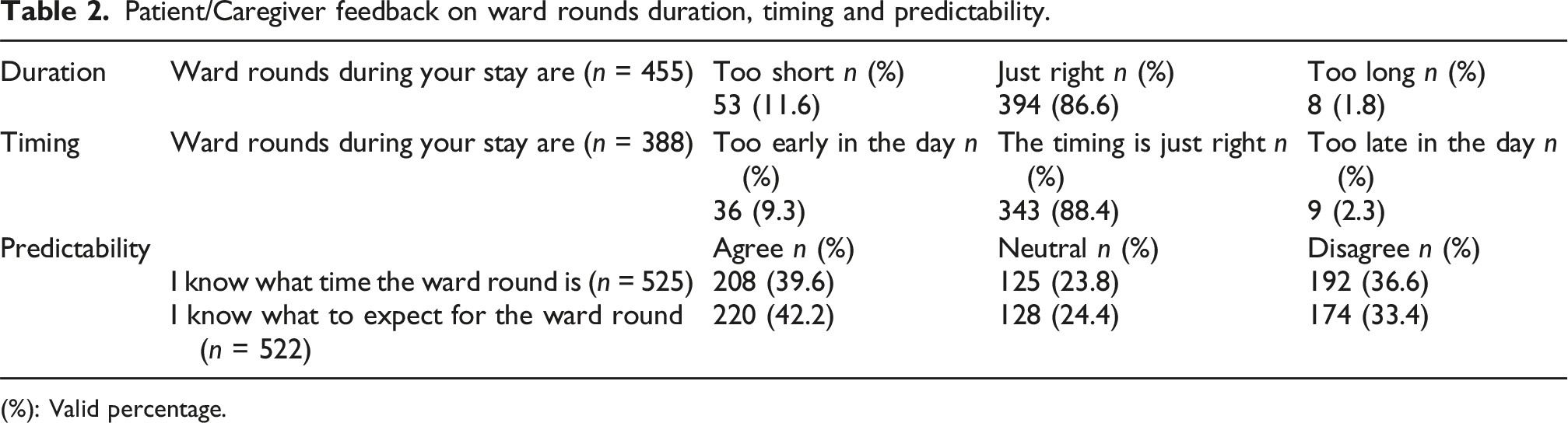
(%): Valid percentage.
Level of satisfaction
Satisfaction levels of Patient/Caregiver on ward rounds.

(%): Valid percentage.
Age group was statistically associated with satisfaction of ward rounds (F = 19.42, p < 0.001, n2 = 0.069). Patients above 50 were less satisfied as compared to patients of the younger age group or their caregivers (who answered on behalf of their children aged 16 and below). The satisfaction scores were highest among caregivers for patients between 0 and 16 years old, followed by ages 17 to 50, and lastly above 50 years old (Refer to Table 1).
Ward types was also related with a significant difference in satisfaction scores, where the satisfaction scores were the highest among A1, followed by B1, with B2 and C class types being comparable (p = 0.001, n2 = 0.031) (Refer to Table 1).
Patient preference on who should be present during ward rounds
Patient/Caregiver preference on who should be present during ward rounds.

(%): Valid percentage.
Discussion
Ward rounds is an integral part of patient care in the hospitals, not only to enable clinical examinations and provide medical care, but also to facilitate patient engagement. It has been well-documented that a better engaged patient experience can improve health outcomes and consume less healthcare resources.18,19 Hence it is important to first evaluate patients’ experiences during ward rounds, in order to inform ward round practices.
In our current study, we evaluated multiple domains of ward rounds, including organisation, structure, and conduct. Majority of responses to the organisation of ward rounds were positive, as most patients felt that the duration and timing of ward rounds were appropriate. However, a third of the patients surveyed did not know when and what to expect of ward rounds. The lack of knowledge of when ward rounds will be conducted can be an unpleasant experience when the medical team unexpectedly shows up. 20 In addition, patients may not have considered beforehand with regards to what they would like to ask or clarify. Patients not knowing when to expect ward rounds suggest that the rounds are conducted at variable timings from one day to another, which can be frustrating for them. 5 In terms of the structure and conduct of ward rounds, patients were most dissatisfied with poor communication of discharge and treatment plans, followed by the lack of opportunity to ask questions. Poor satisfaction levels could be related to insufficient information being provided, which is further exacerbated when patients are not invited to have their questions or concerns addressed by their physician. This can be inferred as patients wanting to be more actively involved in their treatment plans. Lateef (2011) 21 described that such unmet expectations of patients can lead to disappointment and anger, but such negative emotions can be avoided if patients know what to anticipate. Patient- centred ward rounds allows patient participation to be organised into the rounds, providing them with the opportunity to be an active participant and speak with the medical team. 22 Cultivating such a participatory environment by inviting patients to collaborate in the treatment planning process can also cultivate a sense of respect and empowerment through active patient engagement. 2
Based on demographical information, patient satisfaction scoring was found to be influenced by age and ward types. In terms of age, the results revealed that patient satisfaction is significantly poorer in elderly patients aged 50 and above. This could have been a result of age-related discrimination. The concept of ageism in healthcare is not new and can occur in many aspects of healthcare processes, including information exchange and decision-making. 23 Physicians may subconsciously reduce information given or time spent with elderly patients as old age is associated with diminished status and stubbornness. 24 Older adults are generally thought to be difficult and cantankerous. 25 In addition, they are perceived to not communicate much, which can implicate disease management and health outcomes. 24 These may be the contributing reasons as to why physicians are less likely to involve elderly patients in decision-making processes, and why physicians tend to be less accommodating with these patients. 26 It is crucial to acknowledge the difference between abstaining from decision making, and not being informed of treatment plans. While some patients have the intentions to plainly accept the recommendations of their physicians to avoid influencing their care, it does not negate the need to inform patients about their disease and treatment plans. 5
Expectedly, patient satisfaction is also poorer for lower ward classes. Patients staying in higher ward classes (A1) were reportedly more satisfied with their ward round experience as compared to their counterparts in the lower ward classes. This could be explained by several reasons. Being the only patient in the room may heighten their sense of being valued as the patient has the entire medical team to themselves. Our findings are consistent with literature reporting that during ward rounds the communication was longer and more engaging in single-bedded rooms.5,27 In contrast, ward B2 and C can contain between 5 to 6 patients in a room. All the common facilities are shared between patients, which may have predisposed patients to discomfort and eventual dissatisfaction. There is little to no privacy in such multi-bedded rooms as closed curtains are not soundproof. Although visual privacy can be ensured by completely drawn curtains, auditory privacy is arbitrary and depends on proximity of others, ambient noise level, speaking volume and construction of the physical environment.28,29 Barlas et al. (2001) cited that the lack of privacy resulted in five percent of patients withholding details of their medical history or refusing physical examinations. Literature suggests that compared to individual rooms with walls, patients within curtained areas believed that they could be overheard, and that their personal information is being listened to by others. 28 While there are individual treatment rooms in certain wards, these rooms are often use for medical procedures, or to provide a quiet and comfortable environment for bereavement. Another issue with multi-bedded cohort rooms is that patients may feel like they are ‘just one of the cases’ when the doctors move from bed to bed. 5 Patients may also feel disgruntled if they perceive the medical team to spend more time with other patients than themselves.
More than half of the patients preferred having the involvement of nurses during ward rounds. From the results, it is apparent that the presence of nurses were preferred as compared to even family members. Nurses play a crucial role in all aspects of patient’s care, which makes them important patient advocates. 30 This may be the reason as to why patients prefer the presence of nurses, in addition to patients relying on nurses to understand relevant information about their care. 30 As such, the active participation of nurses during ward rounds is indispensable, and often required for inter-disciplinary communication and development of care plans. 30 This can boost patients’ confidence to not only actively participate in ward rounds, but to provide assurance of the care received.2,30 With differing ward round timings and competing time sensitive nursing tasks, it is important that nurses prioritise their tasks such that participating in ward rounds becomes a norm. 30 In a local study, nurse-led ward rounds revealed that nurses actively organised clinical tasks according to the ward round timings. 31 While the exact ward round timing for the different disciplines may not be known to the nurses prior, this unintended staggering of ward rounds can provide nurses with pockets of time to plan tasks around.
Understanding what patients expect is crucial for the improvement of patient satisfaction and delivery of high-quality healthcare. The importance of being given adequate information, including clinical, disease management or prognostic information, is repeatedly mentioned in literature.21,32 Patients generally value clear explanations of their diagnosis or treatment, being shown care and compassion by their healthcare providers, and being listened to. Berhane and Enquselassie (2016) similarly highlighted that patients place their emphasis on diagnosis, information, listening and understanding.
Limitations
One of the main limitation of this study is the use of convenience sampling. Convenience sampling was employed for this study as the data collection was conducted within a limited data collection period of one month. As such, the results may not be generalisable to the general population of patients admitted to Singhealth institutions. 33 The use of convenience sampling and limited data collection period may have potentially affected the difference in sample numbers seen across the participant demographics. As such, while the results do have significant values with small to moderate effect size, the interpretation of these values must be done with caution. The questionnaire tool was developed for this study, and only face validation was conducted. Having also done feasibility testing, reliability testing and pilot testing the survey questions with patient volunteers would have established the tool’s validity. 34
Implications for nursing management
Ward rounds are an established core activity where patient care decisions are made. It has been long established that a well-organised multi-disciplinary team including nurses should be involved in ward rounds. The perceived importance by patients in the need for nurses’ presence further emphasizes what is already recommended by current literature. With increasing workload, concurrent competing ward activities and differing or fragmented ward rounds, there is a need to rethink and evaluate the nurse’s role and feasibility of participation during ward rounds. Nursing administrators plays a pivotal role as this often requires a concerted change that can call for reallocating nursing time and resources within individual wards to bring forth an organisational cultural change. Further research into evaluating practical strategies that promote participation will be beneficial.11,35–37
Conclusion
Our study found that the overall feedback on ward round organisation and structure were positive. However, further improvement is required with regards to the conduct of ward rounds, specifically the opportunity for patients to ask questions and the type of information provided to patients. The varying experiences between patients of different life stages and ward types should be noted and bridged where possible. Understanding what is valued by patients and providing them with necessary information can facilitate patients’ health literacy and improve health outcomes. Healthcare providers need to learn what is experienced and valued by patients to not only improve patient care and satisfaction, but to also create meaning at work.
Footnotes
Acknowledgements
We would like to acknowledge and thank Chief Nurse Png Gek Kheng from Changi General Hospital, Chief Nurse Wong Sook Thow from KK Women’s & Children’s Hospital and Chief Nurse Amy Tay from National Heart Centre, Singapore for their immense support throughout this study.
Ethical considerations
This study was conducted as part of service evaluation and adopted an anonymous survey approach, hence fulfilling the criteria for exemption by SingHealth Centralised Institutional Review Board, Singapore (ref: SHS-RSH-CIRB-4211 Version 4 dated 9 Feb 2020).
Consent to participate
By completing and submitting the survey, informed consent was implied from the participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Research data and materials supporting the study are not publicly available but can be accessed upon reasonable request by contacting the corresponding author.