
Abstract
Introduction
This case of misoprostol-induced coronary vasospasm demonstrates the rare but potentially serious cardiac-related adverse events which arose from the use of misoprostol in a young healthy adult with no past cardiac history of note.
Case Presentation
A 37-year-old female with a history of idiopathic vasculitis but no known cardiovascular risk factors was administered misoprostol vaginally for an elective outpatient hysteroscopy. She developed typical cardiac symptoms of severe chest pain and her initial electrocardiogram demonstrated changes mimicking an anterolateral ST-elevation myocardial infarction. Fortunately, her symptoms resolved shortly before her presentation to the Emergency Department, and her cardiac troponin levels were within normal limits. She underwent further workup during her inpatient stay in a Cardiology ward which revealed no evidence of coronary artery disease, and she was discharged with the rare diagnosis of misoprostol-induced coronary vasospasm.
Discussion and Conclusion
This case illustrates the importance of physician awareness to patients who present with cardiac symptoms following misoprostol administration. We recommend that misoprostol be administered with caution in patients with vasculitis or traditional cardiovascular risk factors and that these high-risk patients should be counselled for the potential of rare but serious cardiac-related adverse events arising from coronary vasospasm.
Introduction
Misoprostol is a commonly used drug in obstetrics and gynaecology for induction of labour, for medical termination of pregnancy, 1 and for cervical priming to decrease cervical tone prior to routine hysteroscopy. 2 It has been extensively researched and is generally considered safe and well-tolerated, with the most common side effects being gastrointestinal in nature such as nausea, vomiting, abdominal cramps, diarrhoea and fever. This case report describes a rare case of coronary artery vasospasm following administration of vaginal misoprostol.
Case details
A 37-year-old female with a history of idiopathic vasculitis not requiring any chronic medications but otherwise no known cardiovascular risk factors (including personal or family history of ischemic heart disease) was planned for elective hysteroscopy under general anaesthesia for evaluation of heavy menstrual bleeding.
This patient had a history of panniculitis with multiple nodules on her bilateral lower limb, which was later demonstrated by skin biopsy and autoimmune tests to be ANCA-negative vasculitis with granulomatosis. She was treated with pentoxyphylline and prednisolone but these were stopped when her symptoms improved and she was not on any chronic medications for the past year prior to the current episode.
Her elective hysteroscopy was to be performed in an operating theatre with facilities for maintaining general anaesthesia. The patient did not have any significant complaints of chest or abdominal, or pelvic pain prior to the administration of the misoprostol. She was asymptomatic and well and her vital signs were stable. She had misoprostol 400 mcg inserted per vaginally by the physician 2 hours prior to her scheduled hysteroscopy time for cervical priming.
Fifteen minutes after insertion, she developed sudden acute-onset severe chest pain with a reported pain score of 10/10. This chest pain was described as crushing, central, with radiation to bilateral shoulders and associated with dyspnoea and diaphoresis. An electrocardiogram (ECG) performed immediately captured ST elevations in the anterolateral leads, and new T wave inversions and ST depressions in the reciprocal inferior leads (Figure 1), mimicking an anterolateral ST-elevation myocardial infarction. 1st ECG performed demonstrating significant ST elevations in anterolateral leads and reciprocal changes in inferior leads following misoprostol insertion.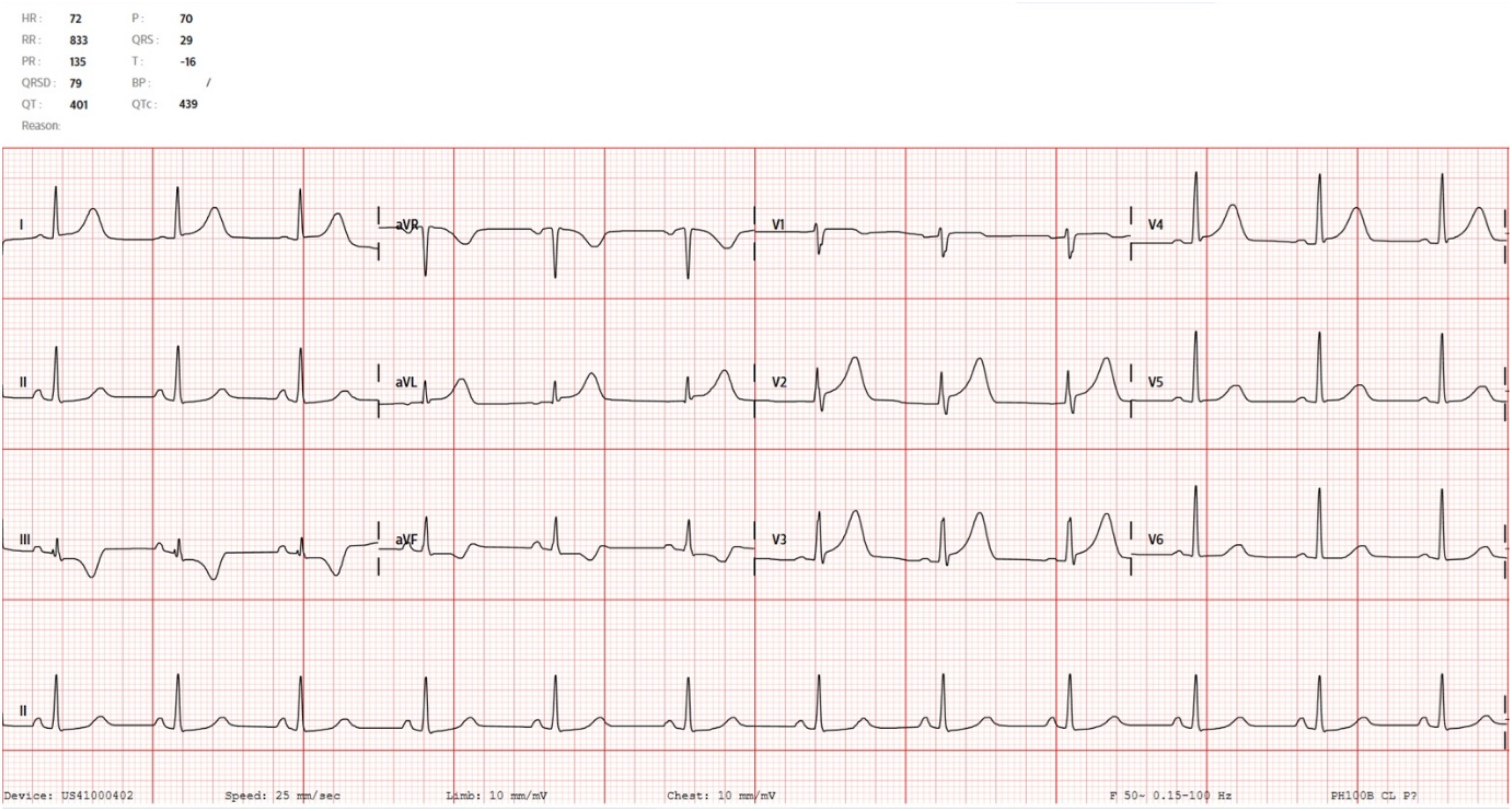
Interestingly, these ECG changes fulfil the European Society of Cardiology/American College of Cardiology Foundation/American Heart Association/World Heart Federation (ESC/ACCF/AHA/WHF) Task Force Universal definition of Myocardial Infarction (“new ST elevation at the J-point in V2-3 ≥ 1.5 mm in females or of at least 1 mm in two contiguous leads except for V2-3”) 3 and therefore also fulfil the institutional criteria for direct activation of the coronary catheterization lab.
A 2nd ECG (Figure 2) done 5 minutes after the initial ECG (Figure 1) showed resolution of the ST changes. She reported relief of her chest pain symptoms 10 mins after the initial ECG was done. She was referred urgently to the emergency department (ED) for further evaluation, and the vaginal misoprostol was removed. Initial investigations at the ED revealed normal high- sensitive troponin (20 ng/L; reference value: <30 ng/L), which was taken approximately 1 hour after the onset of her chest pain symptoms. Her eosinophil level was marginally elevated at 6.1% (reference range 0%–6%). Her chest x-ray was normal. Cardiology was consulted and the patient was admitted to Cardiology for monitoring. Serial ECG done when patient reported relief of chest pain.
The patient underwent further cardiac workup in the Cardiology ward, which included serial cardiac troponin levels at the 7th and 14th hour mark, which were normal. She also underwent a formal transthoracic echocardiogram which showed left ventricular ejection fraction of 62% and did not detect any regional wall motion abnormalities. A computed tomography coronary angiogram performed the following day also likewise revealed no evidence of coronary artery disease with a calcium score of 0. She was eventually discharged 4 days later with the rare diagnosis of misoprostol-induced coronary vasospasm.
Discussion
Vasospastic angina was first described in 1959 when Prinzmetal reported 32 cases of non-exertional chest pain. The classic diagnostic criterion described requires normal coronary angiography with vasospastic response on provocation. 4 Various mechanistic explanations have been proposed, including excessive catecholamine surge, endothelial cell dysfunction, smooth muscle hypercontractility and inflammation arising from increased oxidative stress but no definitive answer has been found. 4 Vasospastic angina most frequently occurs in young females with no significant cardiovascular risk factors otherwise, although drugs such as vasoconstrictor agents and sympathomimetics have been listed as suspected precipitants. These drugs range widely from illicit substance use (e.g. cocaine, marijuana, butanes, amphetamines) to over-the-counter medications, chemotherapy agents and even antibiotics. 5
Drug characteristics of misoprostol
Misoprostol is a synthetic E1 prostaglandin with a wide range of uses that is frequently used to soften the cervix for induction of labour or medical termination of pregnancy. In the non-pregnant patient, it is also used decrease cervical resistance prior to hysteroscopy to reduce the risks of complications arising from cervical dilation such as cervical laceration or perforation. 6 Its uterotonic effects have also been used to control postpartum haemorrhage. Its most common side effects include diarrhoea, abdominal cramps, nausea and vomiting due to its primary effect on the gastrointestinal mucosa as a prostaglandin E1 analogue, but systemic effects like hyperthermia, vertigo and syncope have been rarely reported at therapeutic doses. 7
Misoprostol can be administered via a variety of routes – oral, sublingual, buccal, vaginal and rectal – which in turn affects bioavailability. Amongst these routes, the highest peak plasma drug concentration is achieved via sublingual administration, whereas per vaginal administration with water results in the most prolonged duration of elevated plasma drug concentration. 8 Aronsson et al. (2007) examined serum levels of misoprostol following drug administration and demonstrated a rapid increase to near peak plasma concentration within the first 30 minutes, and this may be further hastened if the drug was delivered vaginally onto a moist mucosa surface. 9 Vaginal administration is also associated with decreased gastrointestinal side effects and increased effects on the reproductive tract, reaching peak plasma concentration in one to 2 hours, 10 then declining slowly. Of note, misoprostol has a short half-life of an hour and undergoes rapid de-esterification during absorption. Misoprostol is primarily metabolized in the liver and its active metabolite, misoprostol acid, is renally eliminated. 11 Serum toxicology levels are therefore unlikely to be helpful in such cases because misoprostol is usually undetectable in plasma.
As Prostaglandin E analogues such as misoprostol have both vasoconstrictor and vasodilatory properties, it is hypothesized that misoprostol exhibits a dose-dependent effect to elevate norepinephrine levels. This rapid increase in norepinephrine levels may provoke coronary artery vasospasm to cause clinically significant vasoconstriction, giving rise to cardiac ischemia which can manifest as typical anginal pain, hypertensive crisis 12 or even cardiovascular collapse in extreme cases. 13 In addition, Kaur et al. highlighted a 52-year-old female who demonstrated features of Takutsubo cardiomyopathy following successful resuscitation from misoprostol-induced cardiac arrest, 14 which suggested that there could be a currently unexplored association between coronary vasospasm and Takutsubo cardiomyopathy.
Current evidence on misoprostol-induced cardiac ischemia.
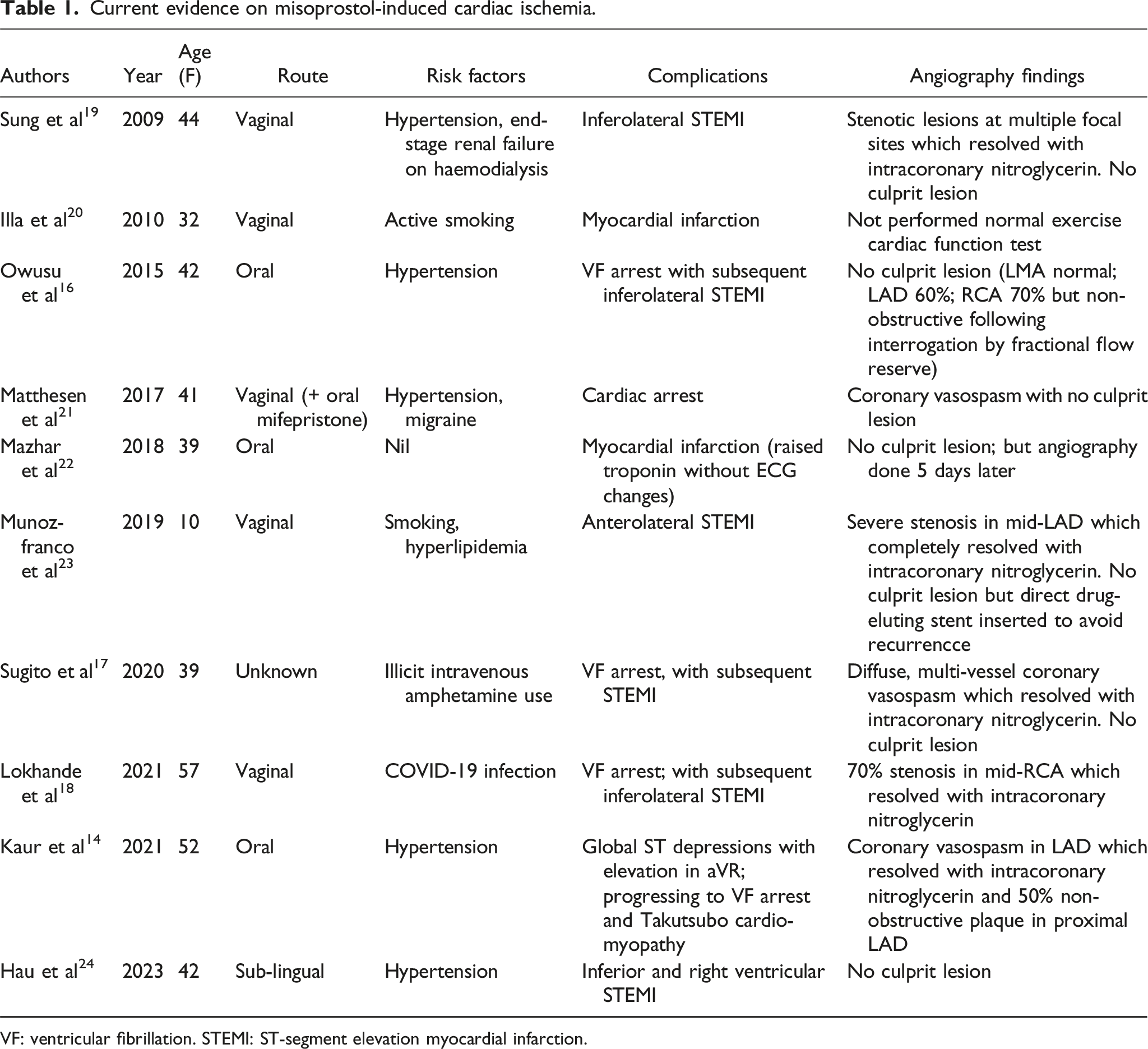
VF: ventricular fibrillation. STEMI: ST-segment elevation myocardial infarction.
Vasculitis and coronary vasospasm
Eosinophilic granulomatosis is a small and medium vasculitis with an incidence of around 0.9 per million population – it is a difficult and rare diagnosis as it presents with varying features that may occur in distinct episodes over a long period of time. 15 In these patients, the features they present with may differ depending on their ANCA (anti-neutrophil cytoplasmic antibody) status: ANCA-negative patients tend to have cardiac and lung involvement due to eosinophilia, whereas ANCA-positive patients may present with more typical features of small vessel vasculitis such as mononeuritis, purpura or glomerulonephritis. 15 As this patient is ANCA-negative, she would therefore be at higher risk for cardiac complications such as vasospastic angina.
Management of misoprostol-induced coronary vasospasm
All patients who present with severe cardiac symptoms such as chest pain, accompanied with significant ECG changes, should still be evaluated as per Advanced Cardiac Life Support protocol as it may be difficult to determine a specific cardiac event. Hence, all patients should be managed in a high-acuity resuscitation area with trained medical staff, availability of resuscitation and cardiac drugs and airway equipment. Treatment is largely supportive in most cases as symptoms typically subside after a period of expectant management. However, if patients report persistent or worsening chest pain, accompanied with refractory ECG changes, the patient should be stabilized and given adequate analgesia such as intravenous morphine, assess to determine if they fulfil criteria for activation of their institution’s cardiac catheterization, and seek an urgent consult with the cardiology specialists.
However, intra-arterial, intracoronary or intravenous nitroglycerin remain distinct therapeutic options for the management of severe refractory vasospasm, in particular those leading to cardiac arrest. Owusu et al. reported successful resuscitation from ventricular fibrillation arrest using nitroglycerin, 16 while Kaur et al. likewise described coronary angiography confirmation of misoprostol-induced coronary artery spasm that responded to nitroglycerin administration. 14 Sugito et al 17 and Lokhande et al 18 also described management of coronary vasospasm with nitroglycerin and oral calcium channel blockers. This is noteworthy because using nitroglycerin as a vasodilator for the management of cardiac arrest is counterintuitive given its potential to worsen hypotension and runs contrary to the standard Advanced Cardiac Life Support algorithm.
Conclusion
The use of misoprostol to facilitate hysteroscopy usually leads to relatively mild side effects. This case adds to the limited literature on misoprostol-induced cardiac complications and illustrates that otherwise young and healthy patients with underlying vasculitis rather than traditional cardiovascular risk factors like hypertension or hyperlipidemia may also be predisposed to misoprostol-induced vasospasm. The risk of cardiac and lung involvement may be elevated in patients with known ANCA-negative vasculitis.
We recommend that misoprostol be administered with caution in these patients and that high-risk patients (including those with traditional cardiovascular risk factors) should be counselled for the potential of rare but serious cardiac-related adverse events arising from coronary vasospasm. In addition, nitroglycerin should be considered for vasodilation in cases of misoprostol-induced coronary vasopasm leading to severe cardiac ischaemia or cardiac arrest for such cases, despite not being part of the standard Advanced Cardiac Life Support algorithm.
Footnotes
Author Contributions
ZT and MN drafted the initial manuscript. Both contributed equally to the writing of this manuscript. SL provided critical input from her gynecological expertise in the case analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.