
Abstract
Isolated mediastinal lymphadenopathy represents a common diagnostic dilemma whereby morphological analysis of tissue specimens are frequently needed to ascertain the diagnosis. Cryobiopsy by linear endobronchial ultrasound (EBUS) guidance had recently been described in literature. We described a multimodality biopsy approach of a case of isolated tuberculous mediastinal lymphadenitis in which we employed the 22-gauge transbronchial aspiration needle, mini-forceps and a flexible cryoprobe sequentially. We aim to highlight the novel technique of linear EBUS guided cryobiopsy in acquiring superior histological specimen from mediastinal lymphadenopathy for diagnosis purposes. We also compared the histopathological quality of the specimens acquired from these three different biopsy modalities.
Keywords
Introduction
Isolated mediastinal lymphadenopathy represents a common diagnostic dilemma whereby morphological analysis of tissue specimens are frequently needed to ascertain the diagnosis. 1 Linear endobronchial ultrasound (EBUS) is a minimally invasive procedure in lung cancer staging but its diagnostic performance for rare or benign conditions can be less satisfactory when confined to cytological specimens from needle aspiration (EBUS/TBNA).2,3 Various tissue biopsy tools guided by linear EBUS have been described in the literature which includes the mini-forceps (EBUS/TBFB) and more recently, the use of cryoprobe (EBUS/TBCB).4–6 In this article, we describe a multimodality linear EBUS biopsy approach of a case of tuberculous mediastinal lymphadenitis who presented as isolated mediastinal lymphadenopathy.
Case Report
A seventeen-year-old man presented with a one-month history of non-productive cough and exertional dyspnea. Physical examination showed no lymphadenopathy and hepatosplenomegaly. His blood investigations were unremarkable. Sputum smears were negative for acid-fast bacilli and did not grow any pathogen. Chest radiograph showed widening of the right paratracheal stripe and an obliterated aorto-pulmonary window which was further confirmed by a computed tomography (CT) thorax which showed multiple para-tracheal mediastinal lymphadenopathies, with the largest at the subcarinal region measuring 5.2 × 1.9 cm.
Under total intravenous anaesthesia, flexile bronchoscopy and linear EBUS was performed through the rigid tracheal tube. There were no significant findings on airway examination. On linear EBUS systematic assessment, there were multiple mediastinal lymphadenopathies at station 4R, station 7 and 4L. The target lymph node at station 7 (subcarinal) measured 28.3 mm on short axis was sampled using a 22-gauge EchoTip Procore HD-EBUS needle (Cook Medical, Bloomington, IN, USA). A total of 4 separate aspirations were performed with fanning method and 10 cm H20 suction. The rapid onsite cytology evaluation (ROSE) of the aspiration samples revealed only lymphocytes with no pathognomonic diagnostic features. Subsequent biopsies using a mini-forceps (EBUS/TBFB) were attempted using a 1 mm miniature forceps after undiagnostic ROSE. The mini-forceps were inserted through the working channel of the echobronchoscope, then directed into the lymph node under EBUS guidance through the previous needle puncture hole. The lymph node was biopsied twice which only yielded small amount of fragmented tissues. Hence, a novel 1.1 mm miniature flexible cryoprobe (ERBE, Medizintechnik, Tübingen, Germany) was explored. The cryoprobe was inserted through the working channel of the echobronchoscope and entered into the target lymph node through the same mucosal defect. The cryoprobe was activated for 7 s as per described in literature 6 and the sample was retrieved by pulling out the echo-bronchoscope and cryoprobe en-bloc from the airway. Retrieval process was smooth despite mild resistance felt during the initial extraction, no bleeding was encountered. The cryo procedure was then repeated with 5 s activation without significant resistance felt during retrieval process. The specimens were thawed in normal saline and fixed in formalin immediately. Patient was extubated well with no pneumothorax or pneumomediastinum.
Results from EBUS/TBNA showed aggregates of epitheloid histiocytes with multinucleated giant cells in a background of necrotic material. Acid-fast bacilli were seen but was negative for GeneXpert MTB/RIF (Cepheid Sunnyvale, CA, United States) and Mycobacterium tuberculosis culture. Microscopically, the sample from EBUS/TBFB shown multiple fragmented necrotic tissues with crushed histiocytes. On the other hand, EBUS/TBCB retrieved two specimens measured 5 × 4 × 3 mm and 5 × 4 × 4 mm respectively. Numerous necrotizing granulomas were demonstrated from these. The qualitative analysis of the three specimens from pathological perspective was presented in Figure 1. Based on the results, there was a high degree of certainty for tuberculous mediastinal lymphadenitis. Anti-tuberculous treatment (isoniazid, rifampicin, ethambutol and pyrazinamide) was commenced with favorable treatment response during follow up. EBUS/TBNA from EchoTip Procore 22G: The entire length of the needle was visible sonographically, cell block showed aggregates of epitheloid histiocytes with multinucleated giant cells in a background of necrotic material (×20 magnification, Hematoxylin & Eosin Stain). EBUS/TBFB from SpyBite mini-forceps: The jaw of the forceps was echogenic once fully opened; microscopically, multiple fragmented tissues with crushed histiocytes were seen (×100 magnification, Hematoxylin & Eosin Stain). EBUS/TBCB from 1.1 mm cryoprobe: The tip of the cryoprobe appears more echogenic compared to the shaft of the probe. Histopathological analysis confirmed necrotizing granulomatous inflammation, evidenced by presence of epithelioid granulomas with Langhan’s giant cells in a background of necrotic tissue (×100 magnification, Hematoxylin & Eosin Stain).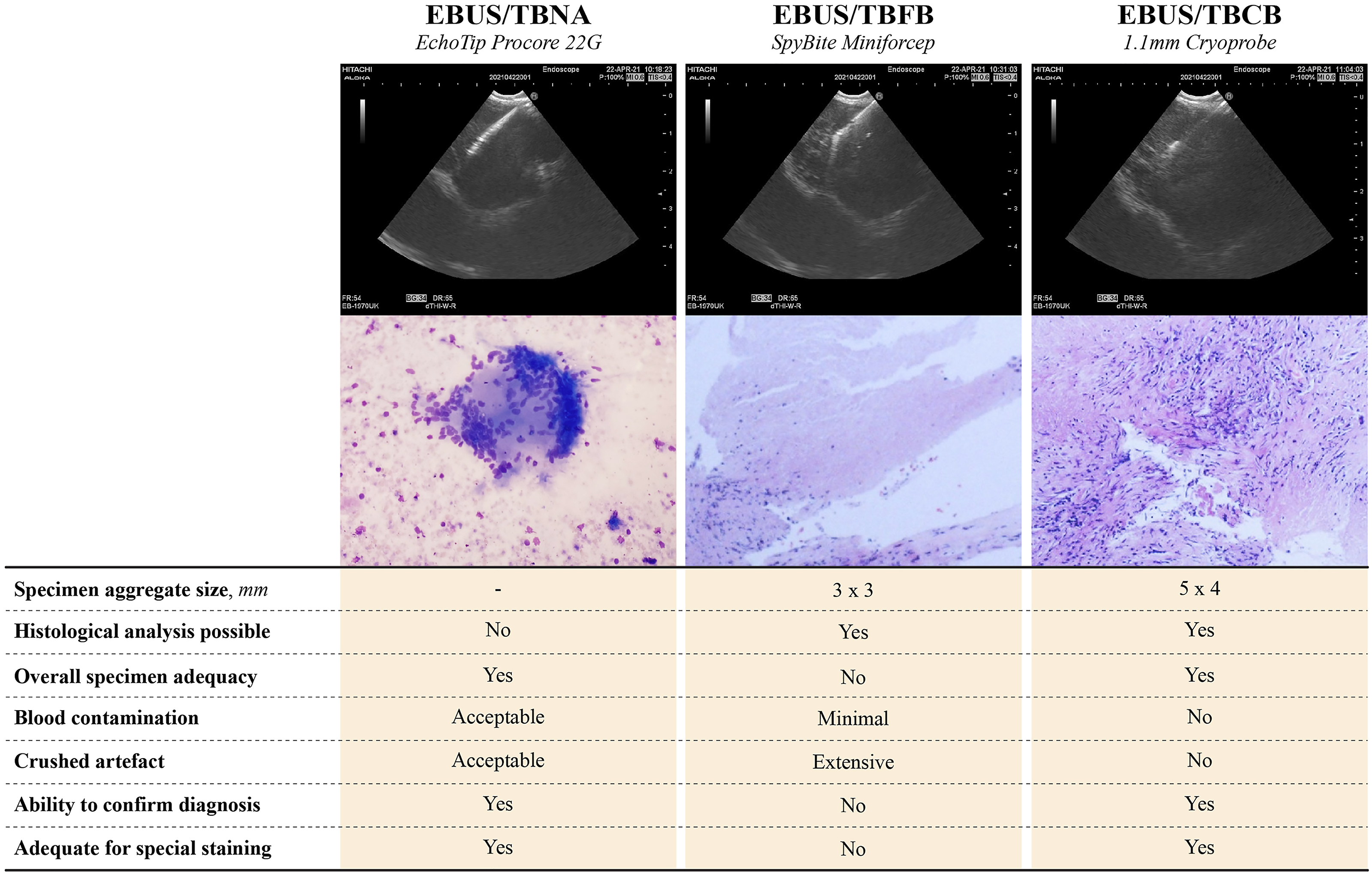
Discussion
In tuberculous cervical lymphadenitis, the diagnosis can only be ascertained in two third of cases after fine needle aspiration (FNA) while excisional biopsy successfully established the diagnosis in all cases. 7 Assuming both FNA methods (FNA for cervical lymphadenopathy and FNA via EBUS/TBNA for mediastinal lymphadenopathy) have similar fundamental principles, a certain amount of mediastinal tuberculous lymphadenitis would require histological analysis for diagnosis. A recent randomized control trial had demonstrated the safety and feasibility of EBUS/TBCB in the diagnosis of mediastinal and hilar lymphadenopathy, especially in the diagnosis of rare tumours and benign diseases. 6 Diagnosis of tuberculous mediastinal and hilar lymphadenitis via EBUS/TBCB had been reported in literature, we further strengthened its role by demonstrating its superiority among three different biopsy modalities. 6
Although EBUS/TBFB is a promising novel technique in acquiring tissue from mediastinal lymph node for histological analysis,4,5 the specimen quality from EBUS/TBFB frequently hinder its clinical usage due to significant crushed artefacts from our observation. In animal study, the endoscopic forceps size is inversely proportionate to more crushed artifacts. 8 Crush artefacts are apparent in EBUS/TBFB due to the small forceps jaws even when fully opened. Furthermore, in lymph nodes with dense consistency, forceps may not open easily to allow effective biopsy, thus further limiting its clinical use. Therefore, the “cryo-adhesion” biopsy principle of cryoprobe can be a more appropriate alternative compared to EBUS/TBNA and TBFB as demonstrated.
However, we have identified a few challenges in utilizing EBUS/TBCB. First, using the TBNA needle with fanning method, the operator is able to sample multiple different areas of the lymph nodes during the agitation movement which may provide a more representative sample. In comparison, although histological samples can be obtained through EBUS/TBFB and TBCB, the samples are obtained from the same region within the lymph node. This potentially affects the diagnostic yield based on the understanding of intra-lymph node heterogeneity when a non-representative region is sampled. 9 The use of ultrasonographic elastography or further advanced imaging to guide the biopsy region may improve this tissue sampling method in the future. Second, the insertion of the cryoprobe can be challenging and should only be handled by trained operators. In previous study, high frequency cautery needle knife was used to create a mucosal defect to facilitate cryoprobe insertion. 6 However, in a smaller case series, the cryoprobe was successfully inserted into the target lymph node without additional procedure as demonstrated in this case. 10 Finally, further study is needed to assess the feasibility and viability of tissue obtained from EBUS/TBCB for microbiological analysis; as well as the potential risk of disseminating a localized tuberculous infection, etc.
Conclusion
EBUS/TBCB is an exciting novel and promising interventional technique which allows clinicians to examine mediastinal lymphadenopathy histologically via a minimally invasive procedure, an important step in the diagnosis of isolated mediastinal lymphadenopathy.
Footnotes
Author Contributions
SSK and CIS initiated the idea for case reporting.
SSK, MZN and JAAR performed the procedure.
SSK and CIS prepared the final copy of the manuscript.
SSK, MZN and JAAR were involved in the overall patient management.
KWN analysed the pathological specimens and provided insight on the pathological perspective in this manuscript.
JAAR supervised the whole management process and reviewed the final manuscript.
All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.