
Abstract
Background
Primary care staff do not provide consistent education on musculoskeletal pain management to patients in accordance with the recommendations of clinical practice guidelines. We have developed a concise online learning program to bridge this gap.
Objectives
To investigate (1) the effectiveness of 1-hour musculoskeletal pain neurophysiology education program conducted by a physiotherapist on primary care staff; (2) the correlation between demographic factors of staff and the interdisciplinary learning performances.
Methods
We piloted a multicenter single-blind prospective study on sixty-four staff from the pharmacy department in eight public primary care clinics. Participants in the intervention group attended the 1-hour online program compared to a control group. The Neurophysiology of Pain Questionnaire (NPQ) to assess learning and the 10-point Likert scale program evaluation form to assess learning reaction of participants after the program were used.
Results
The participants reacted positively to the online learning program. The intervention group significantly improved in their musculoskeletal pain knowledge by a greater mean NPQ score difference 2.39 (p < 0.001) compared with the control group. There were poor correlations between the demographic factors and their learning.
Conclusion
The pilot study shows that primary care staff may still utilize a biomedical approach in managing musculoskeletal pain. The improvement in knowledge demonstrates that short online programs could be a valuable part of interdisciplinary education in primary care because it is easily accessible by healthcare professionals and can benefit other healthcare staff regardless of their background.
Keywords
Impact Statement
What the article adds to the current literature? - Primary care staff may still utilize biomedical approach toward the management of musculoskeletal pain despite biopsychosocial approach is recommended. What new knowledge is added by this study? - Online lecture on musculoskeletal pain can effectively nudge healthcare professionals toward embracing biopsychosocial thinking. -Simple online education program can benefit healthcare staff regardless of their training background. - Pain neuroscience relating specifically to nerve functions requires more in-depth teaching beyond brief online program.
Introduction
Musculoskeletal pain is the most common cause of severe long-term pain and physical disability. It is a health condition that poses huge economic burdens around the world. 1 In Singapore, chronic pain affects at least 8.7% of the population, and musculoskeletal conditions are a major cause of chronic pain. 2 Musculoskeletal pain is amongst the leading reasons for people seeking medical attention in local primary care, accounting for 6–28% of principal diagnoses. 3
Managing pain in primary care has been challenging due to the complex interplay of biopsychosocial factors.4,5 To manage musculoskeletal pain effectively, current guidelines recommend that healthcare professionals provide consistent pain education to patients including relevant information about their medical condition, an updated prognosis, discussions about the role of psychosocial factors on their pain, and their proposed treatment plan addressing biopsychosocial factors. 6 This approach, based on a modern understanding of pain biology, encourages and empowers patients to engage in self-management. 6 In keeping with this approach, it has been shown that patients hope to receive clear, consistent, and individualized information about their pain. 7 However, primary care staff commonly fail to adhere to these recommendations and still practice with a biomedical orientation.8,9
Primary care pharmacists and pharmacy technicians frequently attend to patients with musculoskeletal pain. They are an integral part of the healthcare team that manages patients with musculoskeletal pain along with doctors, nurses, and physiotherapists. They counsel patients on the proper and appropriate use of pain medications in their daily practice. Pain medications make up a significant 20% of the daily prescriptions that are dispensed in SingHealth Polyclinics in Singapore. This is similar to the situation in the USA, where it has been reported that 22% of primary care visits are for pain management. 10 Therefore, it is imperative that patients prescribed with pain medications are provided with accurate and appropriate information about their pain conditions to empower them to administer the medications in a proper manner. Patients have reported receiving conflicting information relating to their pain from different staff, for example, one staff may advise total avoidance of movements, whereas another may advocate allowance of graduated movements. 11 Inconsistency in information provided may be due to inadequate pain science education in the undergraduate training courses of healthcare professionals. 12 One of the aims of this study is to investigate whether this knowledge gap exists in Singapore.
Healthcare providers have a significant and long-lasting influence in shaping the attitudes and beliefs of patients. 13 This presents a need for improving the musculoskeletal pain science knowledge in our primary care staff to ensure that patients are provided with consistent information on pain management, as recommended by clinical practice guidelines. In view of this need, we have developed an education program, which can be easily accessed virtually by all healthcare professionals providing care to patients with musculoskeletal pain.
In tandem, we designed a prospective study to evaluate the effectiveness of the program on staff from the pharmacy department as a pilot study. We also aimed to investigate whether there is any correlation between demographic factors of staff and their learning performances.
This is the first musculoskeletal pain education program developed in our institution. It is a simple intervention designed to be easily implementable in any healthcare setting to enhance the level of pain neuroscience knowledge amongst staff. If proven effective, it can easily be adopted by other healthcare institutions, thereby enhancing the practice of pain management.
Methods
Design
This was a multicenter single-blind prospective study of the musculoskeletal pain neuroscience knowledge amongst primary care staff. The Intervention group participants received an online education program and compared to a Control group. The Neurophysiology of Pain Questionnaire (NPQ) was used to assess learning before and after the program. The 10-point Likert scale evaluation form was used to assess the learning reaction of the participants. There were no changes in protocol. This study was reported according to the CONSORT guidelines. 14
Participants
The study participants were frontline staff in the pharmacy department who regularly provide healthcare to patients. The prospective study was conducted in eight SingHealth primary care clinics. These clinics serve the majority of population in the eastern, southern, and north-eastern part of Singapore. Staff participation was entirely voluntary, and only anonymized data was collected to ensure confidentiality. Ethics approval was exempted by SingHealth Centralised Institutional Review Board. Data collection occurred in October 2020. Using an assumed effect size of 50%, the study required at least 14 participants in each arm to test the effectiveness of the musculoskeletal pain program at a statistical power of 80% and alpha cutoff of 5%.
Interventions
The education program was developed by a multidisciplinary team. The content was based on the current understanding of pain neuroscience according to relevant textbooks.15,16 The key information included mechanisms of peripheral sensitization, neuropathic pain, central sensitization, and differences between biomedical model and biopsychosocial model, as well as MSK pain management in primary care. The program was delivered in a 1-hour online lecture for only one session. No pre- and post-lecture reading materials were provided. The program was presented by a primary care physiotherapist via an online lecture. Although the presenter was not blinded to the NPQ items, the validity of the study was not compromised as the online program had been developed independently of the NPQ and hence was not designed to facilitate achievement of high NPQ scores by attendees of the program. This approach is consistent with other studies.12,17
Outcomes
We adopted Kirkpatrick’s Levels 1 (reaction) and 2 (learning) evaluation model. 18 We assessed the reactions of participants who attended the program using a self-developed program evaluation form. They were asked whether the program was interesting, easy to understand, useful to their work, and helped them gain new knowledge and understand musculoskeletal pain better. They were also asked to rate on a Likert scale of 1–10, where 1 depicted “Strongly Disagree” and 10 depicted “Strongly Agree”. To assess the participants’ learning, we used the English version of the NPQ before and after the online program. The order of NPQ items was randomly shuffled pre- and post-program. Participants were also asked to report the age, gender, number of years working in pharmacy, and job designation.
The Neurophysiology of Pain Questionnaire (NPQ)
The original NPQ was a 19-item questionnaire designed to assess how an individual conceptualizes pain. 12 It was then refined to a shorter version of 12-item questionnaire. 19 The NPQ is widely used amongst healthcare professionals, undergraduate medical and allied health students, as well as patients.12,17,20–22 Each NPQ item has three response options: True, False, and Undecided. The NPQ uses the number-correct scoring method. 1 point is awarded for each correct response. A score of 0 is attributed to incorrect responses and those marked as “Undecided”. Participants are advised to utilize the Undecided option and avoid lucky guesses. As a straight True–False format will force participants to guess, the NPQ developers provided the “Undecided” option. They contend that although guessing may still exist, the inclusion of an ‘‘Undecided’’ option allows for the identification of gaps in knowledge, while incorrect responses allow for the identification of mistaken beliefs. 19 The maximum total score is 12.
Blinding and Randomization
Randomization was done in a concealed manner. Data collection forms were printed on equal number of Blue- and Yellow-colored paper. The research team then shuffled and randomly distributed the colored forms to all staff. The research team members who were assigned to distribute the forms were blinded to the purpose of the colors. The participants did not know the purpose of the colors; hence, they were blind to which group they were allocated to. They were instructed to complete the demographic data form and pre-program NPQ before the program started. They were asked to complete the post-program NPQ and program evaluation form immediately after the 1-hour lecture. Although all were invited to attend the program, participants who did not attend the lecture were free to read up on this topic of their own free will after completing the pre-program NPQ. They were asked to complete the post-program NPQ after 1 hour. All participants were informed that the purpose of collecting the data was to compare participants who attended and did not attend the program; as such, they were blind to the primary interest of the study.
The principal researchers were not blinded from the purpose of using colored paper. Yellow was used for the Intervention arm, whereas Blue was used for the Control arm. Participants who attended the online program and completed the Yellow forms were classified as the Intervention group, while those who did not attend the program and completed the Blue forms were classified as Control group. Responses by participants who received the Blue forms but attended the program, as well as those who received the Yellow forms but did not attend the program, were excluded from analysis of results. Hence, the statistical analysis was not undertaken blindly.
Statistical Analysis
Demographic characteristics and learning reactions of the participants were analyzed using descriptive statistics. The Student unpaired t-test was used to test the homogeneity between Intervention and Control groups, as well as to determine whether the program was an effective intervention tool to improve participants’ understanding of musculoskeletal pain by comparison between the Intervention and Control groups. Student paired t-test was used to examine the intragroup changes of NPQ scores of the Intervention and Control arms.
Pearson’s correlation test was used to assess the correlations between the demographic factors of participants (age and number of years working) and changes in NPQ score after the program. The Chi-square or Fisher exact test was used to analyze categorical variables such as whether the demographic factors (gender and seniority in job designation) associated with the changes in NPQ score after the program. A Pearson’s correlation coefficient level of >0.8 is depicted as very strong, 0.6–0.8 as strong, 0.3–0.5 as fair, and <0.3 as poor. All the statistical analyses were performed using SPSS (Version 25.0). p-Values of less than 0.05 will be considered statistically significant.
Results
Baseline characteristics and NPQ scores (pre- and post-program) of Intervention and Control groups.

Student unpaired t-test was used to compare to differences of age (years), the average number of years working in pharmacy, and pre–post program NPQ scores between the Intervention and Control groups. p< 0.05 is considered statistically significant.

Study flow diagram.
Intervention group participants’ reactions (n = 36).

Means, SDs, 95% Confidence Intervals, and p-values for the NPQ score difference in Intervention and Control groups.

Student paired t-test was used to compare to mean differences of NPQ scores pre- and post-program. p < 0.05 is considered statistically significant.
Pre- and post-Program Means, SDs, 95% Confidence Intervals, and p-values for each NPQ item score difference in Intervention group (n = 36).
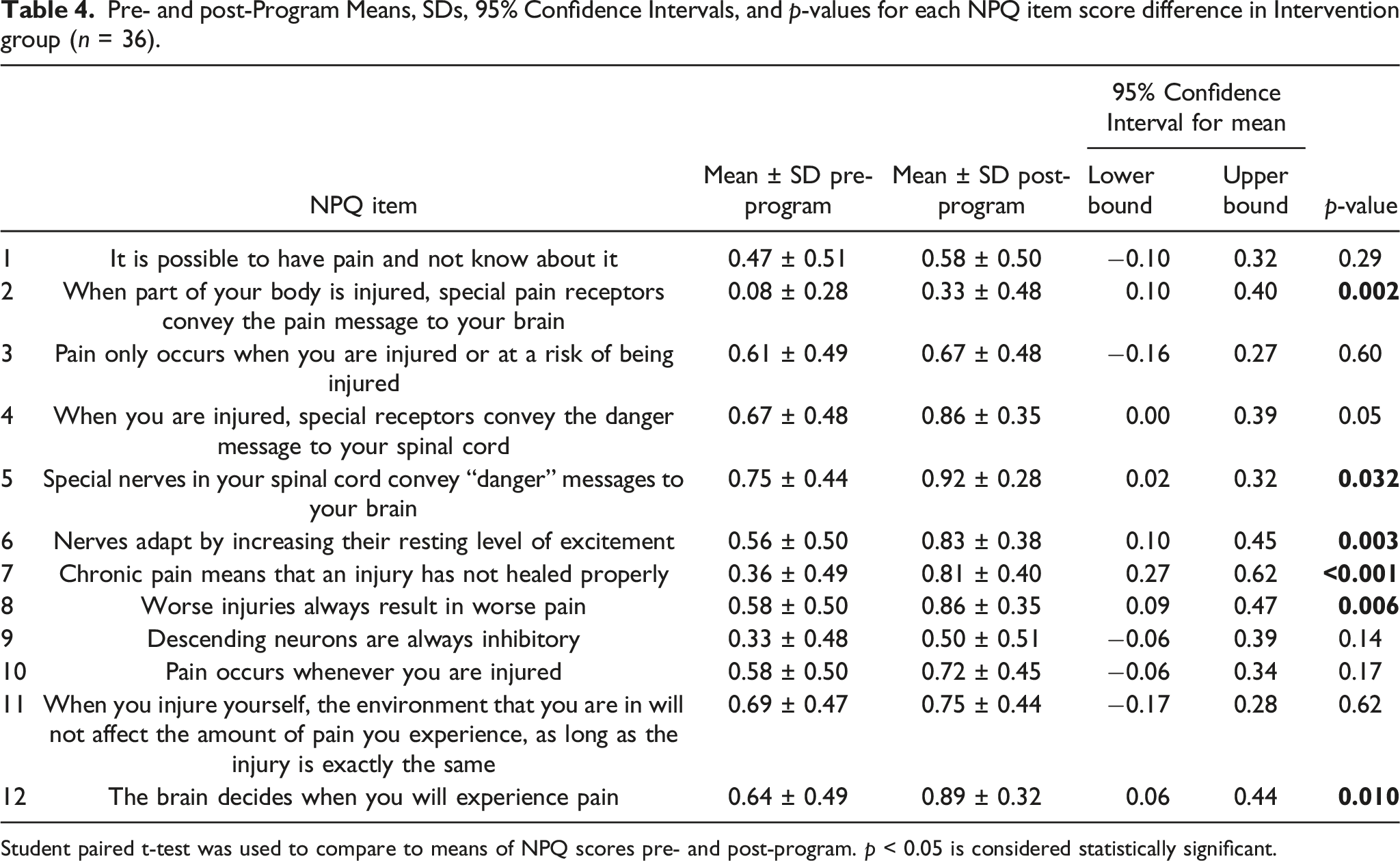
Student paired t-test was used to compare to means of NPQ scores pre- and post-program. p < 0.05 is considered statistically significant.
Items 2, 9, and 7 were among the questions for which the research participants scored poorly before the program, with only 8%, 33%, and 36% of the Intervention group participants having selected the correct answers, respectively. Items 5, 11, and 4 were among the questions for which the research participants scored relatively better before the program, with 75%, 69%, and 67% of the Intervention group participants, respectively, giving the correct answers. Although item 2 showed significant change (p = 0.002) post-program, the score remained the lowest—only 33% of the Intervention group participants answered it correctly post-program. It was the only question for which more than half of the Intervention group participants had answered wrongly after the program. On the other hand, item 7, for which the research participants also answered poorly before the program, achieved the most significant change (mean difference 0.44 ± 0.50), with 81% of participants answering correctly post-intervention.
Lastly, we analyzed the demographic factors versus the participants’ learning. There were poor correlations between the age (p = 0.40) or the number of years working in pharmacy (p = 0.69) and the NPQ score improvement. Also, there were no associations between gender (p = 0.26) or the seniority in job designation (p = 0.18) and the improvement in NPQ scores.
Discussion
This study demonstrates that an online interdisciplinary education program can effectively increase the musculoskeletal pain neuroscience knowledge of healthcare staff in primary care. In addition, we also found that staff demographic factors did not affect their learning.
Comparison with Existing Literature
Our baseline NPQ score (52.8%) implies that primary care staff may still be practicing with a biomedical orientation. This score is comparable with the original study by Moseley which used the original 19-point NPQ. 12 In Moseley’s study, the multidisciplinary healthcare professionals who did not receive specific training in pain neuroscience scored 55% on average. 12 Our subgroup analysis on pharmacists, however, revealed a mean baseline NPQ score of 65.8%. This finding resonates with the findings of Louw et al., who studied baseline knowledge of pain neuroscience among pharmacists and found a mean score of 67.7%. 17
Our study showed significant improvement of 37.8% in NPQ scores post-intervention. Moseley’s study showed that the healthcare professionals improved by 23% after an educational intervention. 12 In a study by Louw et al., the pharmacists improved their knowledge of pain by 17.0%. 17 The lower percentage improvements reported by Moseley and Louw et al. could be due to their higher baseline scores. In our study, we noticed that our participants improved particularly well for some questions such as “Special nerves in your spinal cord convey ‘danger’ messages to your brain,” “Chronic pain means that an injury hasn’t healed properly,” and “The brain decides when you will experience pain”. This indicated that our online learning program had successfully nudged the learners toward embracing biopsychosocial thinking. This is important because it suggests that the learners had started to conceptualize pain as a marker of the perceived need to protect body tissue, rather than as a marker of tissue damage. 24 With this improved understanding of pain neuroscience, the primary healthcare staff who had participated in our online learning program may now be able to better engage with their patients on the subject of pain management and will be in a better position to provide them with more accurate information about their pain. Accurate reconceptualization of pain in patients has been shown to improve pain ratings, dysfunctions, fear-avoidance, and pain catastrophization, disability, and healthcare utilization. 25
Despite statistically significant improvements for the item “When part of your body is injured, special pain receptors convey the pain message to your brain,” fewer than half of the Intervention group answered this question correctly after the program. This may reflect a common misconception about the differences between “nociception” and “pain,” which Wall and McMahon described as an “unfortunate trivialization” perpetuated by inaccuracies in various textbooks. 26 Along with the item “Descending neurons are always inhibitory,” the participants seemed to perform poorly in the questions that required deeper understanding about the neurophysiology. Thus, 1 hour of teaching might be insufficient to allow the participants to grasp and master these concepts. By inference, competence at answering questions relating specifically to nerve functions would require an improvement in the level of neuroscience knowledge which would exceed enlightened pain beliefs and attitudes. 19
Clinical implications
These findings highlight an opportunity to enhance the training curriculum across disciplines to provide specific coverage of pain neuroscience given the growing evidence pointing to the benefits of accurate understanding of pain neurophysiology, which can potentially translate into improved patient care in the form of better musculoskeletal pain management. 15
Another noteworthy finding from this study is that effective online learning is not limited by demographic factors. Age, number of years working in pharmacy, seniority, and job designation did not affect the participants’ ability to gain new knowledge in musculoskeletal pain via online learning. Online lectures can be as effective as face-to-face learning in improving the knowledge and skills of healthcare professionals. 27 For example, Louw et al. demonstrated that live presentation was not superior to virtual classroom. 17 Our current finding further supports the feasibility of use of technology for delivering education, particularly in the midst of the current ongoing COVID-19 pandemic that has abruptly changed and disrupted the conventional methods of conducting education in healthcare. 28
Limitations
Our study has limitations which should be noted. Firstly, our participants were staff from pharmacy department in primary care. It may not be conclusively generalizable to staff from other departments or institutions. Second, using NPQ, we assessed only the “knowledge” (knows) and “competence” (knows how) components of Miller’s pyramid of learning model. 29 It is not known if the knowledge is transferable into “performance” (shows how) or ‘action’ (does). Third, to our knowledge, it has not been conclusively demonstrated that an NPQ score improvement would necessarily translate into a clinically significant improvement or a positive impact on patient care. Fourth was a methodological limitation. Convenience sampling resulted in a high number of dropouts despite our team’s innovative randomization method to improve the study rigor. A randomized controlled trial with an alternative education program or a sham program for the Control group would have been more methodologically robust. Notwithstanding, it has been cited that a Control group in educational intervention study is in fact unnecessary. 30 We decided to include staff who did not attend the program to enable comparison between groups. Knowles suggested that adult learners are motivated to self-explore the topic. 31 In this context, 1 hour may simply not be sufficient for the Control group to learn about pain neuroscience. Lastly, we did not conduct a long-term follow-up. We argue that knowledge retention could be affected by many intrinsic and extrinsic factors. 32 Hence, a long-term follow-up may not necessarily reflect the effectiveness of the interdisciplinary education program. One study, however, showed that the knowledge retention decreased over time but clinicians retained a positive clinical perspective in managing musculoskeletal pain. 17
Additional research is recommended to evaluate the effectiveness of the program on other healthcare professionals with a bigger sample size as an extension of this pilot study. Further research can also include direct observation of staff communicating with patients, as well as tracking of patients’ clinical outcome measures and satisfaction to explore the translation of knowledge on clinical care in primary care setting.
Conclusion
This study found that primary care staff may still be practicing with a biomedical orientation. Although the 1-hour online program could not adequately address the pain neuroscience knowledge gap relating specifically to nerve functions, this brief program has, in short term, increased knowledge of pain neuroscience amongst the primary care staff, and nudged them toward embracing biopsychosocial thinking. Hence, it could potentially facilitate better communication between healthcare professionals and patients about musculoskeletal pain, in keeping with an accurate understanding of pain has shown to improve clinical outcomes. Furthermore, our study supports the feasibility of use of technology for delivering education. This simple interdisciplinary program can be extended to more healthcare professionals as it is easily accessible and can benefit staff regardless of their background, although further studies are needed to confirm this.
Footnotes
Acknowledgments
We thank Mr Tim Cocks, Dr Mark Catley, and Professor Lorimer Moseley for providing helpful advice. Also, we would like to thank the SingHealth Polyclinics pharmacy team for facilitating the study.
Authors’ Contributions
KS and S researched the literature, and together with BQ, WP, KH, and SM conceived the study. KS, S, KH, and SM developed the educational program, and KS conducted the online lecture. WP and AWY contributed in the participant recruitment. BQ was involved in gaining ethical approval and performed data analysis. KS wrote the first draft of the manuscript. WP and AWY guided the development of this manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The development of the interdisciplinary education program received an Academic Medicine Education Institute (AM.EI), Duke-NUS Grant [Project No.: 2011].
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are available from repository (Figshare.com, ![]() ).
).
Ethical Approval
Ethics approval was exempted by SingHealth Centralised Institutional Review Board (CIRB Reference: 2020/2855).
Informed Consent
Verbal informed consent was obtained from all subjects before the study. Written informed consent was not obtained because only anonymized data was collected.
Trial Registration
Not applicable because this study did not involve patient-level outcome measures or community participants.