
Abstract
Objective:
This study examines current practices, experiences, beliefs, concerns regarding negative outcomes and confidence of non-pain specialty anaesthetists regarding prescribing opioids to chronic pain patients.
Design:
An electronic cross-sectional survey was conducted by physicians from the Division of Anaesthesiology, excluding pain specialists, at the Singapore General Hospital.
Methods:
An online survey was conducted, investigating: (a) sociodemographic and practice characteristics; (b) current opioid prescribing practices; (c) experiences and beliefs towards prescribing opioid analgesics for chronic non-malignant pain; (d) confidence and comfort when prescribing opioids; and (e) educational and training needs in chronic pain management.
Results:
A total of 123 anaesthetists (80.9%) responded to the survey. It was noted that only 38.2% of respondents were comfortable managing patients with chronic pain. The majority (86.2%) felt that anaesthetists should be the primary doctors in the management of postoperative pain in chronic pain patients, and 61% believed that chronic pain trained specialist anaesthetists should be responsible; 92.7% of respondents agreed that patients who are educated about their pain tend to do better. Most importantly, 96.7% of respondents feel that they will benefit from more education regarding pain management in chronic pain patients.
Conclusions:
The majority of non-pain specialist anaesthetists recognise the importance of education regarding pain management for non-malignant chronic pain patients. Many feel that they are not confident in managing these patients and will benefit from continuing medical education and self-assessment courses to improve their confidence. These results could be used to enrich current pain management courses.
Introduction
Pain, especially chronic pain (pain lasting more than 3 months), is a multidimensional and individual experience, comprising complex mechanisms contributing to its pathophysiology. Patients who have chronic pain are often difficult to treat as a result of biopsychosocial factors. The lack of appropriate regulations on opioid prescription may mean that many of them are on chronic opioid therapy. The prevalence of chronic pain may be more than we think, it has been estimated that approximately 20% of people are affected by this condition worldwide.1,2 A local study found that the prevalence of chronic pain was 8.7%. 3 In the UK it has been reported that chronic pain exists in up to 46% of the population. 4
Opioids play an important role in acute and cancer pain management but the risk–benefit ratio is not as clear in patients with chronic non-cancer pain. Increasing opioid use resulted in opioid epidemics worldwide, with 1000 deaths per month in the USA. As such, many physicians are hesitant with opioid use, paradoxically undertreating pain at times. Locally, where regulated opioids are very restricted, those without regulatory control have been seen to be abused experientially. 5 It is hence even more imperative that physicians have good knowledge and confidence in the management and titration of opioid doses to avoid problems of tolerance, dependence and addiction.6,7 One study performed within the primary care sector reported that approximately 60% of physicians did not feel confident in managing chronic pain patients. 8 Another study showed that a high confidence level in their opioid prescribing skills was associated with willingness to prescribe opioids to chronic pain patients, resulting in increased patient satisfaction levels. Some studies have also shown that provider confidence improved when there were standardised practices to guide opioid prescription.9–11
Managing patients with chronic pain can be challenging, and as anaesthetists pain management in the perioperative setting is part of what we do on a daily basis. However, not all anaesthetists are trained pain specialists even though most pain specialists have their basic specialty training in anaesthesiology. Our day to day management of perioperative pain in surgical patients makes it necessary for pain management to be part of a core topic during anaesthesiology residency training. Thus far, studies have been carried out to assess if family physicians, junior doctors and physician nurses were confident in prescribing opioids in the management of chronic non-cancer pain. However, current practice, beliefs and attitudes in anaesthetists towards this subject have yet to be examined. This survey was part of a larger research project designed to develop and evaluate the pain curriculum in a residency programme. The first phase of this research was to conduct a needs analysis survey and we also aimed to examine the current practice, experience, beliefs and apprehensions regarding negative outcomes and confidence of anaesthetists (who are non-pain specialists) when prescribing opioid analgesics for the chronic pain patient.
Methodology
Survey design
The survey questions were based on questionnaires in previously published research about physician attitudes and practices and were adapted to the perioperative setting in which our study participants work.12,13 The questions were pretested on 10 anaesthetists in the department through the same online survey platform as the final iteration, and minor edits were made to correct grammatical errors and provide improved clarity in question phrasing.
Setting and participants
All 152 anaesthetists, except those with subspecialty accreditation in pain management, in the Division of Anaesthesiology at Singapore General Hospital and Sengkang General Hospital, Singapore, were invited to participate in an anonymous web-based survey from 3 to 31 August 2020. The participants ranged from medical officers not in a training programme, anaesthesia residents in all 3 years of training, senior residents, resident physicians, associate consultants and consultants to senior consultants. The doctors provide a range of anaesthetic, perioperative and pain management services to patients of all ages in the largest tertiary hospital in Singapore, with comprehensive multidisciplinary care and extensive academic involvement and training.
The survey questionnaire was conducted via Form.sg, which is a government-run data-encrypted secure online platform.
An email invitation was sent out, which included a description of the study and a link to the web-based questionnaire. A total of three reminder emails were subsequently sent out one week apart. This study was approved by the local ethics review board (CIRB 2020/2708).
Data collection and measures
Outcome measures: Respondents completed survey items addressing their: (a) sociodemographic and practice characteristics; (b) confidence and comfort when prescribing opioid analgesics; (c) opinions and attitudes about chronic pain management; (d) perceived profile of chronic pain patients in their practice; and (e) further education needs.
Questions were adapted from previously published questionnaires that assessed general pain knowledge and doctors’ attitudes towards the treatment of chronic pain. The majority of questions utilised a 5-point Likert scale (1 = ‘strongly disagree’; 5 = ‘strongly agree’). The final iteration of the survey contained 38 questions and required approximately 10 minutes to complete.
Analysis
We grouped the respondents into juniors (medical officers, residents, senior residents and resident physicians) and seniors who are accredited on the specialist register (associate consultants, consultants and senior consultants) to explore if junior doctors had significantly different responses from senior doctors. Due to sparse counts in the two extreme categories ‘strongly disagree’ and ‘strongly agree’, we collapsed ‘strongly disagree’ and ‘disagree’ together into one category as ‘disagree’, and similarly ‘strongly agree’ with ‘agree’ into another category as ‘agree’. Chi-square test results were obtained to assess the statistical association between the respondents’ attitudes towards the set of questions and their seniority, and Fisher’s exact test was used when some of the expected cell counts in the contingency table were smaller than 5. The analysis was run using R 4.0.3.
Results
Respondent demographics
From the 152 anaesthetists who were sent the questionnaire, 123 (80.9%) responded (see Table 1). Respondents’ age ranged from 25 to 66 years (mean 42.79 years). The number of years in practice ranged from one to 35 years, with a mean of 11.1 years in practice. Male anaesthetists represented 48% of the respondent population. Sixty-five (52.8%) respondents were accredited senior anaesthetists on the specialist register (including associate consultants, consultants and senior consultants), 58 (47.2%) were junior doctors in the department (including residents in early training and medical officers who were not in a training programme at that point).
Respondent demographics.

Comfort and confidence in care of chronic pain patients
Only 38.2% of respondents somewhat or strongly agreed with the statement of ‘I feel comfortable managing pain issues for patients with chronic pain’ whereas 39.9% somewhat or strongly disagreed (see Table 2). Senior and junior doctors were divided on their responses to this: while 57% of senior doctors agreed with this statement, 55% of junior doctors disagreed with it. In fact, only 17% of junior doctors endorsed this statement (χ2 (2, N=123)=20.70; P<0.001).
Physician comfort and confidence.
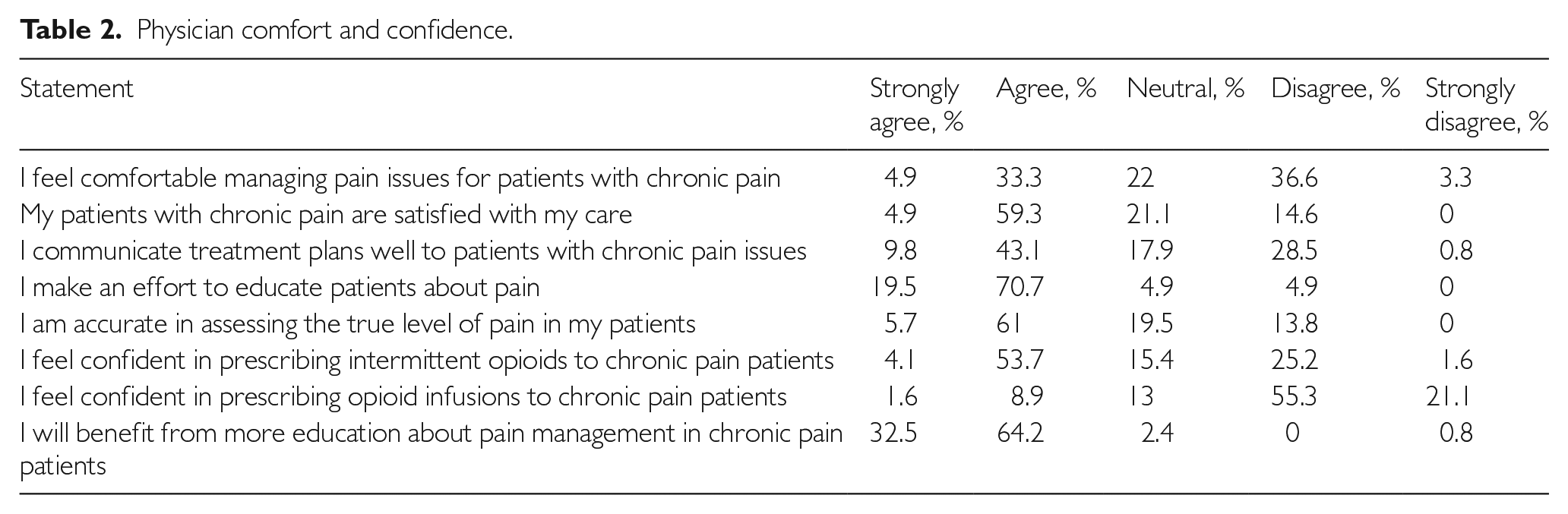
Some 66.7% somewhat or strongly agreed that they are accurate in assessing the true level of pain.
However, 59.3% agreed and 4.9% strongly agreed that their patients with chronic pain were satisfied with their care. An overwhelming 90.2% of respondents agreed that they make an effort to educate patients about pain, but only half of respondents (52.9%) agreed that they communicate treatment plans well to patients with chronic pain issues. Opinions were clearly divided among the junior doctors: 45% disagreed with the statement and 43% agreed with it. While senior doctors were more inclined towards agreement with this statement (62%), it is worth noting that 23% of them chose to be neutral on this matter (χ2 (2, N=123)=13.13; P=0.001).
Some 57.8% felt confident prescribing intermittent opioids to chronic pain patients, but only 10.5% felt likewise in prescribing opioid infusions. There was nearly unanimous disagreement with the statement ‘I feel confident in prescribing opioid infusions’ among junior doctors (93%) while only 62% senior doctors expressed outright disagreement, another 22% were neutral, and only 16% endorsed the statement unequivocally (χ2 (2, N=123)=16.97; P<0.001).
Attitudes and beliefs
Most respondents (94.3%) felt sympathy for patients with chronic pain issues (see Table 3); 52.9% of respondents enjoy taking care of their patients with chronic pain issues and 58.5% of respondents find satisfaction in caring for patients with chronic pain issues. Some 86.2% of respondents indicated that they strongly or somewhat agreed that anaesthetists should be the primary doctor in the management of postoperative pain in chronic pain patients. The term ‘anaesthetist’ in the prior statement refers to all anaesthetists including pain specialists, who in the local context, are anaesthetists who have undergone further subspecialty training in pain; 47.2% of respondents agreed that patients get relief after referral to the chronic pain team while 41.5% strongly agreed.
Attitudes and beliefs.

While 61% believed chronic pain specialists should be responsible for the postoperative pain management in chronic pain patients, 35% believe it should be via a team approach (see Table 4).
Who do you think should be responsible for postoperative pain management in patients with chronic pain.

Some 64.2% of respondents felt that patients with chronic pain issues take more time to manage. The majority of both senior and junior doctors agreed that chronic pain patients take up more of their time, but there were significantly more juniors (86%) than seniors (66%) who felt this way (χ2 (2, N=123)=6.79; P=0.03).
Perception of chronic pain patients
A vast majority (97.6%) somewhat or strongly agreed that patients with chronic pain have more pain postoperatively (see Table 5). Some 92.7% somewhat or strongly agreed with the statement that ‘patients who are well educated about their pain tend to do better’.
Perception of chronic pain patients.

While 82.9% agreed that the majority of their patients with chronic pain issues are not drug seekers, 36.6% agreed that chronic pain patients exaggerate their pain; and 70% believed that chronic pain patients requesting stronger narcotics are honest about their pain requirements.
Some 74.8% felt that patients with chronic pain are sorry to bother them about their pain, while 79.7% agreed that patients with chronic pain tend to have underlying psychiatric problems. Some 39.9% believed that narcotics cause dependency among their patients with chronic pain issues, 87% believed that ethnic groups vary in their expression of pain and 78.8% found there are racial differences in pain relief seeking behaviour. Some 42.3% agreed that women tend to have worse cases of pain.
Responses to the question of what chronic pain patients want are presented in Table 6.
Physician impression of what chronic pain patients want.

Opioid preference
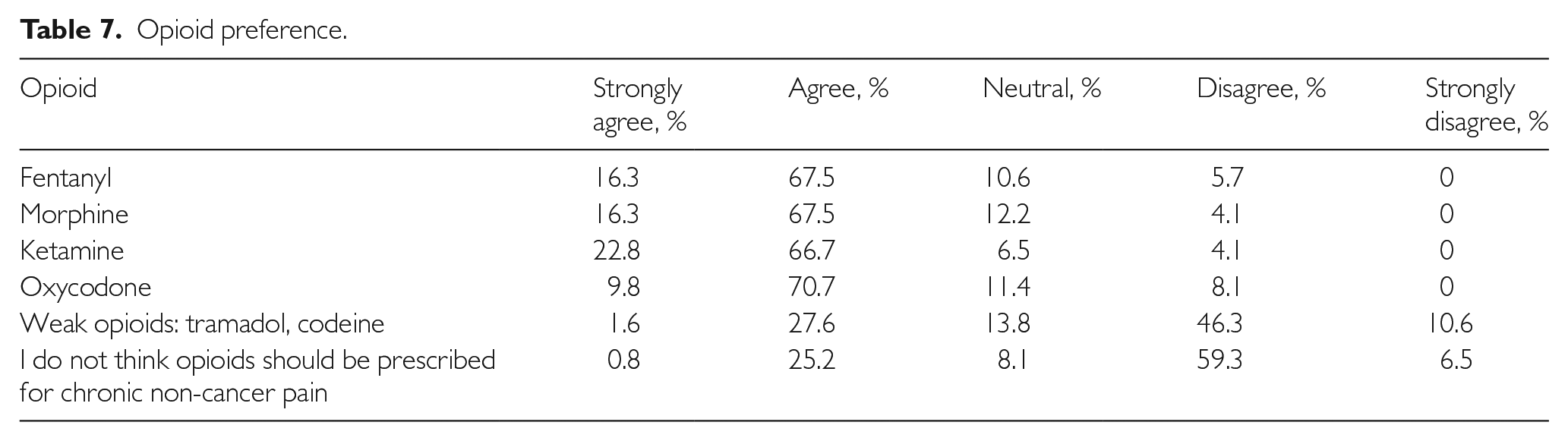
Most respondents believed that strong opioids such as fentanyl, morphine and oxycodone are useful in the management of postoperative pain in chronic pain patients and 89.5% agreed that ketamine is useful. In contrast, only 29.2% agreed that weak opioids such as tramadol and codeine are useful in this context (see Table 7).
Opioid preference.
Education and training
An overwhelming 96.7% of respondents agreed that they will benefit from more education about pain management in chronic pain patients (see Table 8). Some 87.8% felt that continuing medical education courses and 79.7% felt that self-assessment courses will be most helpful to them to improve the management of patients with chronic pain. Integrated blended learning involving self-assessments and interactive feedback courses appear to be the most preferred for further pain education.
The following will help me in managing patients with complex pain.

A summary of comparisons between seniors and juniors reported is shown in Table 9.
Chi-square analyses to examine differences between seniors and juniors.

Discussion
Pain management is an examinable topic in our current anaesthesiology trainee curriculum; however, despite the structured objectives at present in the local curriculum, there has been a lack of emphasis on the perioperative pain management of the chronic pain patient. This lack of emphasis is evident in our study when we found that only 38.2% of anaesthetists agreed that they were comfortable in managing pain issues for patients with chronic pain. While this finding is consistent with much of the medical literature regarding provider confidence in opioid prescribing, 13 we expected a higher confidence in anaesthetists who are well versed in administering opioids during the perioperative period. In addition, the junior anaesthetists surveyed were less comfortable than the seniors and fewer agreed that they communicate treatment plans well to these patients. Several reasons could have contributed to the low confidence. During the course of anaesthesiology training, rotation to chronic pain clinics is often a brief exposure, and complex pain patients are often referred to the few chronic pain specialists within the anaesthesiology department. The training of each anaesthesiology resident is therefore often dependent on chance encounters with this patient group in their course of work, and this experience would be built on, and this gradual increase in confidence over time may explain the difference between seniors and juniors. Examination questions on opioids in chronic pain patients are often predictable, and thus trainees would naturally place more time and energy on other aspects of their anaesthesiology study. There is also a general concern on the risk of opioid dependence and addiction in patients with chronic pain, and hence many would prefer to leave the opioid prescribing to pain specialists.
Traditionally, the anaesthetist is thought to take on the responsibility of managing the patient peri-operatively, and this includes preoperative optimisation of the patient for surgery, intraoperative management of the patient under anaesthesia and postoperative pain control. It was therefore very surprising that only 3.3% of the participants felt that managing postoperative pain lies with the anaesthetists in charge of the case. The results reflect the consequences of the early division of the anaesthesiology specialty into different subspecialties, including pain management and critical care. Chronic pain patients are an extremely heterogeneous group, and infrequent and episodic exposures may not significantly improve comfort levels in the general anaesthetist. This is also reflected in the high proportion who felt that a subspecialist in pain should be responsible for the postoperative pain management of chronic pain patients instead of the anaesthetist in charge of the case during the surgery. Some 61% felt that the pain specialist should look after postoperative pain in chronic pain patients. In fact the majority (88.7%) agreed that patients get relief after referral to the chronic pain team. For the past decade in our institution, there has been an efficient referral system in place to allow the transition of care of chronic pain patients to pain specialists. Early involvement of the chronic pain specialist even in the preoperative period for complex pain patients has allowed appropriate titration of opioid dosages in the opioid-dependent patient and the prevention of opioid withdrawal, thus improving patient care.
Frantsve and Kerns highlighted the importance of communication in chronic pain management in the context of shared medical decision making. 14 It is encouraging that 90.2% of respondents agreed that they make an effort to educate patients about pain, and accordingly more than 90% also agree that patients who are well educated about pain tend to do better.
We found that most respondents (66.7%) agreed that they are accurate in assessing the true level of pain in patients. This could possibly be attributed to most of these patients being attended to in the postanaesthesia care unit, whereby the leading strategy in assessing pain is not what the patient reports, but rather behavioural observation, facial expression and vital signs, as reported in the previous literature. 15
The majority of anaesthetists are confident in prescribing intermittent opioids to chronic pain patients, and this is unsurprising as this is often the first line treatment of postoperative pain in the recovery room. It stands to reason that the majority believe that opioids should be prescribed to patients with chronic non-cancer pain. However, it is noteworthy that the same level of confidence does not extend to the prescription of opioid infusions in chronic pain patients. In our survey, we did not include intravenous patient-controlled analgesia (IV-PCA) as part of the definition of opioid infusions. Compared to conventional opioid infusions, IV-PCA as a form of pain relief has demonstrated superiority in both safety and efficacy and allows the easier individualisation of therapy in postsurgical patients.16,17 Hence, IV-PCA is often the mainstay of postoperative analgesia in patients undergoing major surgery, and most anaesthetists would be familiar in its use and prescription. However, this comfort level may not extrapolate to the group of opioid-tolerant, complex pain patients, in whom a fine balance between the need for effective pain control, the prevention of opioid withdrawal and avoiding increased opioid dependence needs to be considered.
There is evidence that situational and work-contextual factors affect the clinician’s judgement of pain. High levels of work activity affect pain assessment and are associated with decreased response to patients’ pain cues. 18 The majority of survey respondents agreed that patients with chronic pain issues take more time to manage, and many junior staff felt that this work took them away from their other clinical duties. However, this is mitigated by the high number who report joy and satisfaction in the care of, as well as feeling sympathy (94.3%) for these patients.
A clinician’s perception of the patient and the patient’s personality affect the clinician’s feelings and views towards the patient. 19 It is heartening that 82.9% agree that the majority of their patients with chronic pain issues are not drug seekers, 70% agree that these patients are honest about their pain requirements and 74.8% agree that these patients are sorry to bother them about their pain. This is also consistent with the high number of respondents who report feeling sympathy for these patients.
We found that the majority of respondents agree that there is an ethnic difference in pain expression as well as pain relief-seeking behaviour. Ethnic differences in pain responses have been associated with mu-opioid receptor (OPRM) polymorphism. 20 It has been found that stoicism can be a consequence of socialisation in a specific family or culture, although it can be a concern as stereotypism and stigmatisation may set in.
Strengths and limitations
The strengths of this study include the large sample size, as Singapore General Hospital and Sengkang Hospital are staffed by the same pool of anaesthetists, which forms the overall largest anaesthetic department in Singapore. The high response rate of the study participants could be attributed to the overall convenience of the online survey, whereby participants could complete it in their own time and at a pace they chose. This also reduced the possibility of non-response bias in our study. The design of the online survey incorporated the use of mandatory questions such that missed questions are highlighted and a response is required before respondents could proceed to the next page, which helped to eliminate incomplete entries.
However, there are slight differences in training programmes across the three main health clusters in Singapore and a cross-cluster study would provide more information on the significance of these variations. In addition, the survey was not designed to evaluate providers’ actual competence in opioid prescription for the chronic pain patient in the postoperative setting. It is unclear from this study whether respondents’ confidence or lack thereof was consistent with their knowledge and practices. Future studies can address the correlations between providers’ confidence and outcomes as well as addressing education needs and training.
Conclusion
The management of chronic pain is usually challenging, and sometimes beyond the scope of what is taught during anaesthesia residency training. We found that a large proportion of respondents maintained joy in managing these patients, although some feel uncomfortable in the management of opioid dosages in these patients. While most prefer the guidance from a pain specialist, many cited the need for improved education or revised training curriculum for pain management in opioid patients. This survey demonstrated a need to improve training in the management of chronic pain and opioid use. Our inter-professional team encompassing physicians, nurses and pharmacists also identified the gaps in opioid management knowledge, skills and attitudes among our junior doctors who are first-line responders to patients in pain. Pharmacists have reported inappropriate opioid prescription by doctors as the main problem requiring their interventions among opioid-related issues.
The results of this survey thus provide the foundation and recommendations for a review of the current curriculum for pain education in anaesthetists. We believe knowledge alone, while crucial, is inadequate to equip a physician to prescribe opioids appropriately and confidently. Addressing opioid management attitudes and skills is important to translate the knowledge into clinical practice. Taking the lead in proactive education of novice doctors in opioid prescribing is important for improving patient outcomes and ensuring safety for patients and the community.
A pilot blended learning programme had been initiated at the time of writing, focusing on comprehensive opioid management in pain, using an interactive online module-based blended learning approach inclusive of participative learning, self-assessments and case-based discussions.
Supplemental Material
sj-docx-1-psh-10.1177_20101058211008197 – Supplemental material for Survey of physician comfort and attitudes on perioperative opioid prescription in patients with chronic pain
Supplemental material, sj-docx-1-psh-10.1177_20101058211008197 for Survey of physician comfort and attitudes on perioperative opioid prescription in patients with chronic pain by Pei Yu Tan, Denise Desiree Bi Si Quah and Diana Xin Hui Chan in Proceedings of Singapore Healthcare
Footnotes
Acknowledgements
None.
Authors’ contributions
PYT and DXHC researched the literature and conceived the study. PYT obtained exemption from ethical review as the principal investigator. All authors were involved in protocol development, patient recruitment and data analysis. PYT wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Availability of data and materials
The datasets generated and/or analysed during the current study are available from the corresponding author.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was waived by the Singhealth Centralised Institutional Review Board D because the research involves a survey without identifiers (CIRB ref 2020/2708).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not explicitly sought for the present study because consent was implied if volunteers proceeded to complete the anonymous survey and there was no cost or risk of harm to participants.
Trial registration
Not applicable as this was a survey and no trial was conducted.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.