
Abstract
Background
Stroke is a major cause of morbidity and mortality worldwide. Despite advances in acute treatments, timely intervention remains crucial. This study assessed stroke knowledge in Malta to identify gaps that could contribute to treatment delays.
Methods
A mixed methods approach was used, starting with qualitative interviews of stroke patients, relatives, and bystanders, followed by a quantitative survey among the general Maltese population and healthcare workers. The online survey included demographics, stroke knowledge, and stroke response questions. Data were analysed using descriptive and inferential statistics to identify knowledge gaps and influencing factors.
Results
The study surveyed 1872 participants, representing the Maltese population. Significant knowledge gaps were found in stroke symptoms, risk factors, and appropriate responses. Younger participants, males, non-Maltese, urban residents, those with higher education, and higher-income individuals showed better stroke knowledge and response. Healthcare workers scored higher than the general public. A strong positive correlation was found between stroke knowledge and appropriate response actions.
Conclusions
The study highlights the need for targeted educational interventions to improve stroke awareness and response, especially among older adults, women, rural residents, and lower-income groups. Recommendations include comprehensive public education campaigns, culturally tailored materials, and ongoing professional development for healthcare workers. Addressing these gaps could enhance stroke prevention and management, reducing stroke-related morbidity and mortality.
Background
Stroke remains one of the leading causes of morbidity and mortality worldwide. 1 Recent advances in acute stroke treatment, specifically the introduction of mechanical thrombectomy, have improved the outcomes of affected patients. Stroke treatment remains time-sensitive, as alluded to in the acronym ‘Time is Brain’. 2 Although the time window for mechanical thrombectomy has now been extended beyond 24 h in certain cases, 3 time to reperfusion remains one of the key factors in functional outcome. Delays to treatment occur both pre-hospital and within the hospital.
In this study, stroke knowledge in Malta was assessed to determine potential lacunae in knowledge, assuming that delays to treatment could be improved if such knowledge gaps are addressed.
Method
The study was based on a sequential exploratory design proposed by Cresswell and Plano Clark 4 and consisted of three different phases. This specific design was chosen to leverage the strengths of both qualitative and quantitative approaches in a structured manner. This design begins with an in-depth exploration of the phenomenon through qualitative data collection, allowing the researcher to gain a deep understanding of participants’ experiences and identify key themes. The subsequent quantitative phase then tests these findings on a larger sample, providing generalizability and statistical validation. This approach is particularly useful when little is known about the research topic, allowing for theory development that can be empirically tested, thereby enhancing both the depth and breadth of the findings.
During phase one, qualitative data collection and analysis were performed by interviewing stroke patients, relatives, and bystanders. Phase two involved the construction of a survey tool which could quantitatively assess stroke knowledge. A matrix was developed to facilitate and standardize the transformation of the quantitative data collected in phase 1 into a survey tool, enabling its deployment across a larger population to enhance generalizability. 5 In phase three, the tool was then deployed in a sample of the Maltese population, as well as to a group of healthcare workers. Prior to its deployment, the tool was subjected to several quality assurance tests using a critical appraisal framework developed by Hou et al. 6 This appraisal framework evaluates the following aspects: (1) conceptual framework, (2) psychometric properties, including validity and reliability, and (3) feasibility.
The questionnaire (Figure 1) has three sections as follows: (i) Demographics (including age, gender, ethnicity, region of Malta, education, income, risk factors, and whether they were employed as healthcare workers); (ii) Stroke knowledge (17 questions); and (iii) Stroke response (17 questions). Responses for the Knowledge and Response sections were collected using a 5-point Likert scale (strongly agree, agree, undecided, disagree, strongly disagree). A 5-point Likert scale was chosen as it strikes a balance between simplicity and depth, making it easy for participants to understand while capturing nuances in attitudes or perceptions. It also helps prevent response fatigue and ensures consistency, making the data more reliable and easier to analyse. Questionnaire.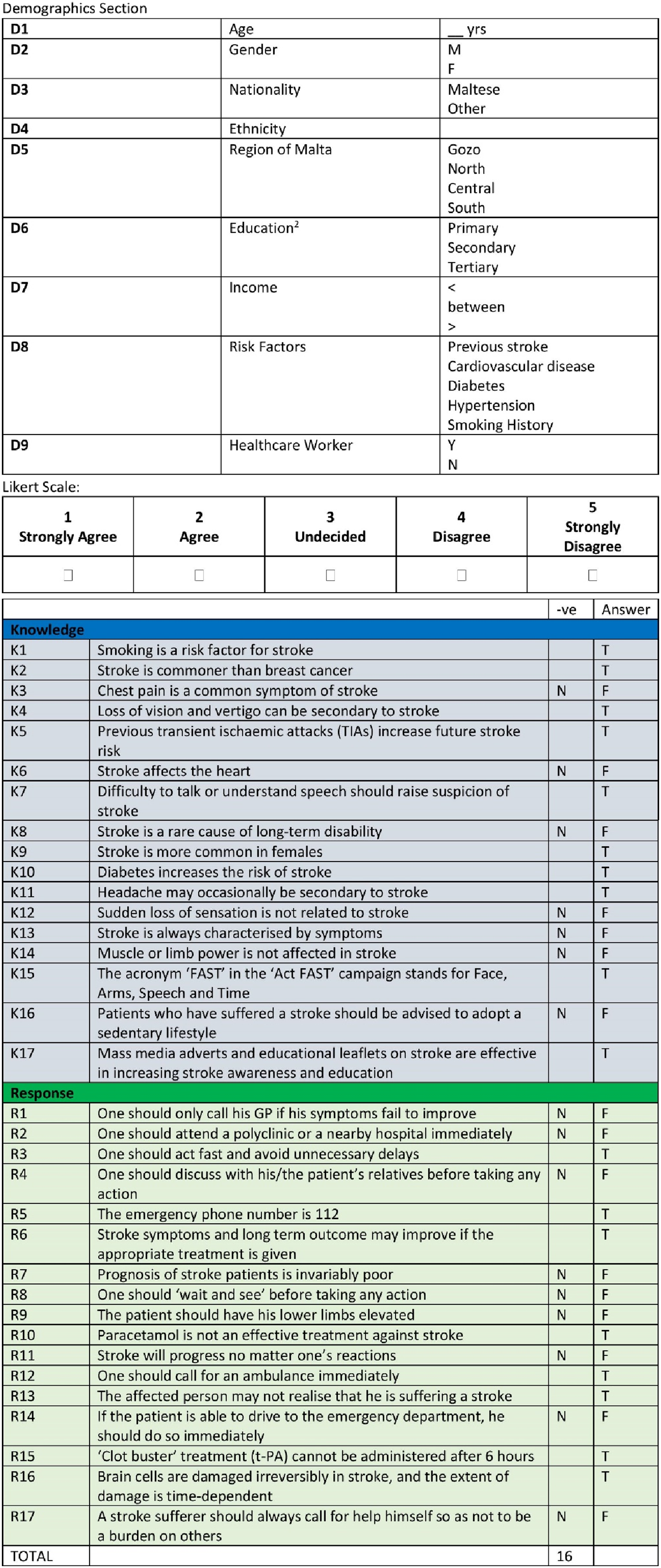
This article will focus on the results of Phase three of the study, that is, Instrument Implementation. The quantitative survey tool was deployed among two distinct sample groups: the public and healthcare professionals. This phase aimed to quantify the level of stroke knowledge and identify educational gaps in the Maltese population.
The survey was conducted online, ensuring accessibility and ease of use. Regular checks were performed to monitor data collection and address any issues promptly. The data collected were analysed using descriptive statistics and correlations to understand the patterns and relationships in stroke knowledge among the participants.
The sample size required for representation of the Maltese population was between 1500 and 2000. 1872 participants answered the questionnaire. Since the Maltese population at the time when the study was performed was 450,000, the sample size guaranteed a maximum margin of error of 2.26%, assuming a 95% degree of confidence. A stratified probability sampling technique was employed to allow for adequate representation of sub-groups (strata) within the whole population (Crossman, 2016), as listed in the general electoral register.
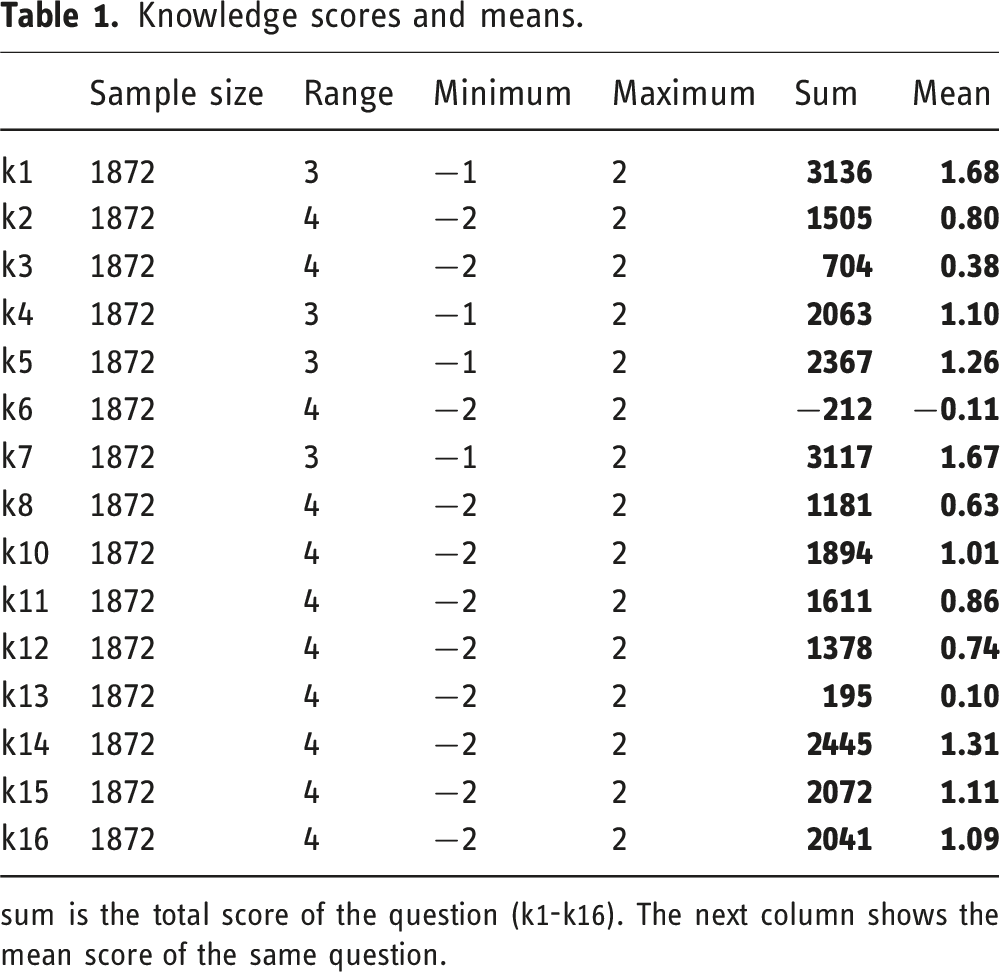
Correct answers were scored +1 or +2 (for strongly agree/disagree), whilst −1 and −2 (for strongly agree/disagree) points were deducted for incorrect answers. This scoring system was employed to include all scores from the 5-point Likert scale used for data collection. Negative values were necessary to indicate incorrect answers, ensuring these scores did not contribute to the overall mark. This generated individual scores for Stroke Knowledge and Stroke Response for each participant, as well as a Total score. Mean values for each of the 34 questions were also generated, and a total score representative of the Maltese population was obtained. Questions that had low mean scores indicate a stroke knowledge gap.
Quality assurance
Throughout all stages, quality assurance was a critical focus. Various strategies were employed to ensure the credibility, transferability, dependability, and confirmability of the research findings guided by the works of Shenton 7 and Yin. 8 These included methodological triangulation, the use of different types of informants, iterative questioning during interviews, and respondent validation of data collected. Furthermore, the data integration process was meticulously planned and executed to ensure that qualitative insights effectively informed the quantitative phase.
Ethical considerations
Ethical approval was obtained for the study, and all participants provided informed consent. Measures were taken to ensure anonymity and confidentiality, and participants were protected from discomfort and harm. Transparency was maintained throughout the research process to uphold the integrity of the study.
Results
Descriptive statistics
Descriptive statistics were utilized to summarize the demographic characteristics and stroke-related knowledge and response of the 1872 respondents from the Maltese population (Figure 2). The demographic data included variables such as age, gender, nationality, ethnicity, geographical region, education level, income, risk factors, and healthcare worker status. Column charts showing mean knowledge, response and total scores segregated by (a) Age, (b) Gender, (c) Education, (d) Income, (e) Risk factors, and (f) Health care worker status.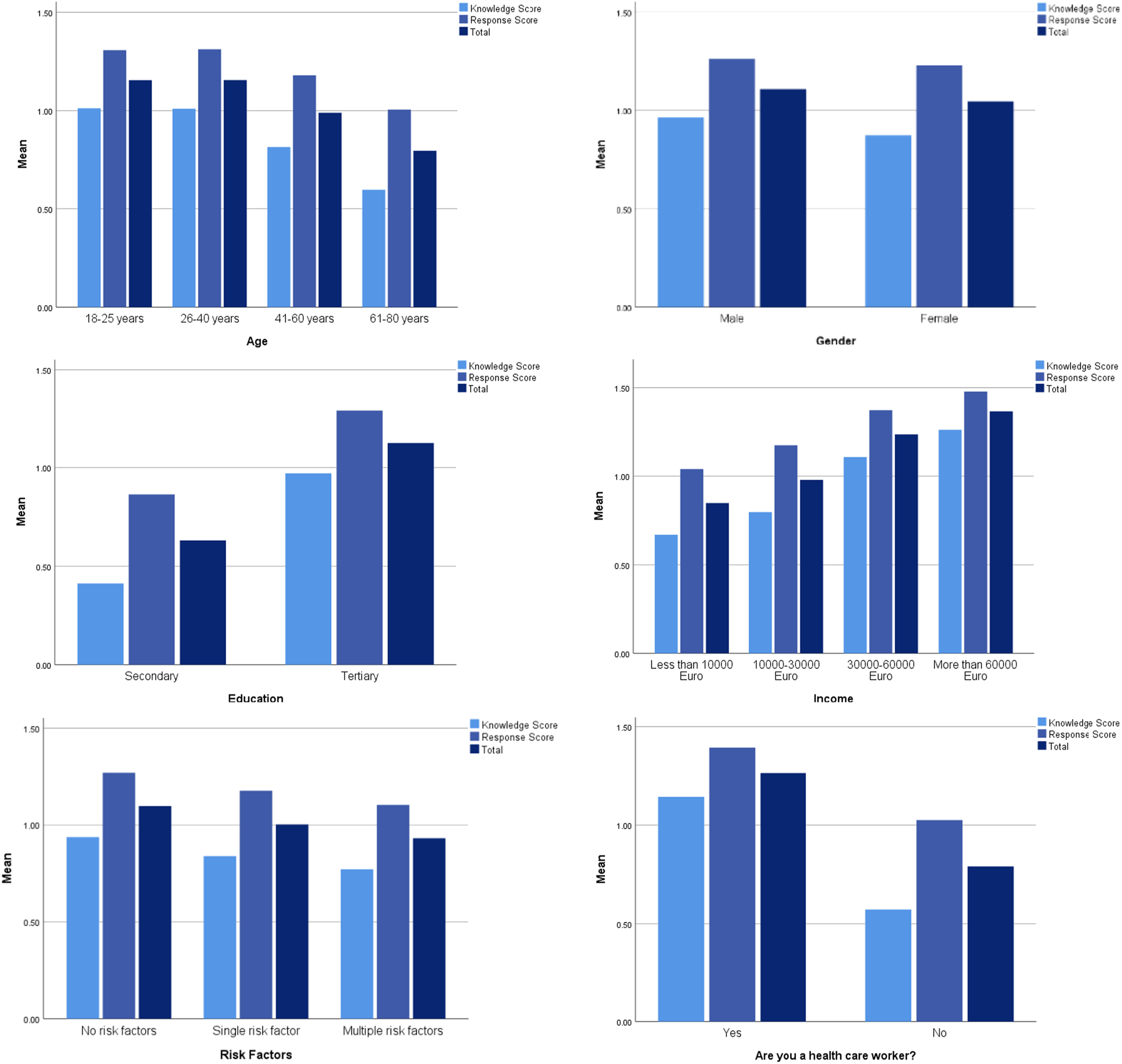
Each of these variables was coded for statistical analysis. Age was categorized into four groups: 18–25, 26–40, 41–60, and 61–80 years. Gender was coded as male, female, and other, while nationality was divided into Maltese and other. Ethnicity included categories such as White, Black, Mixed/Multiple, Asian, and Other. The regions of Malta were categorized into Gozo, North, Central, and South. Education levels were divided into primary, secondary, and tertiary, and income was grouped into four brackets: less than 10,000 euros per annum, 10,000–30,000 euros, 30,000–60,000 euros, and more than 60,000 euros per annum. Risk factors were listed as hypertension, diabetes, smoking, heart disease, previous stroke/TIA, multiple risk factors, and none. Healthcare worker status was coded simply as yes or no.
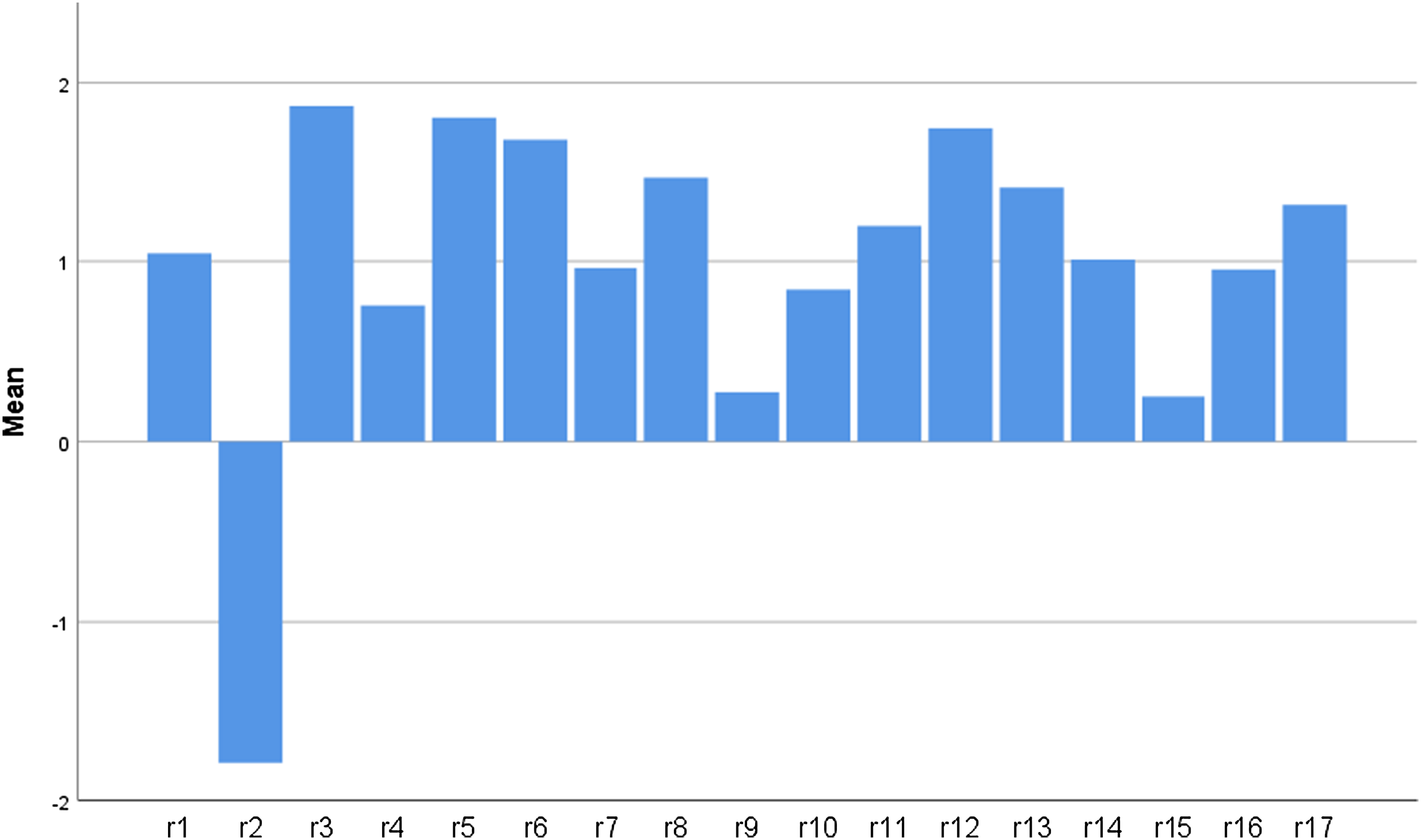
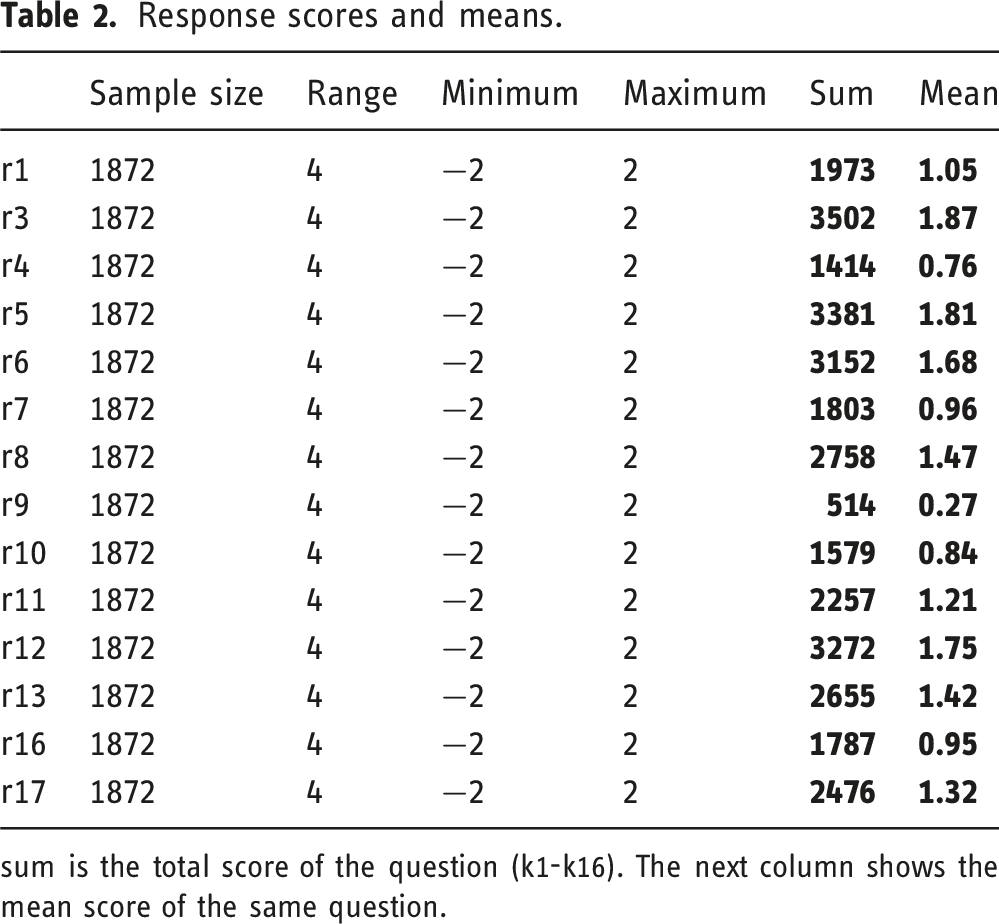
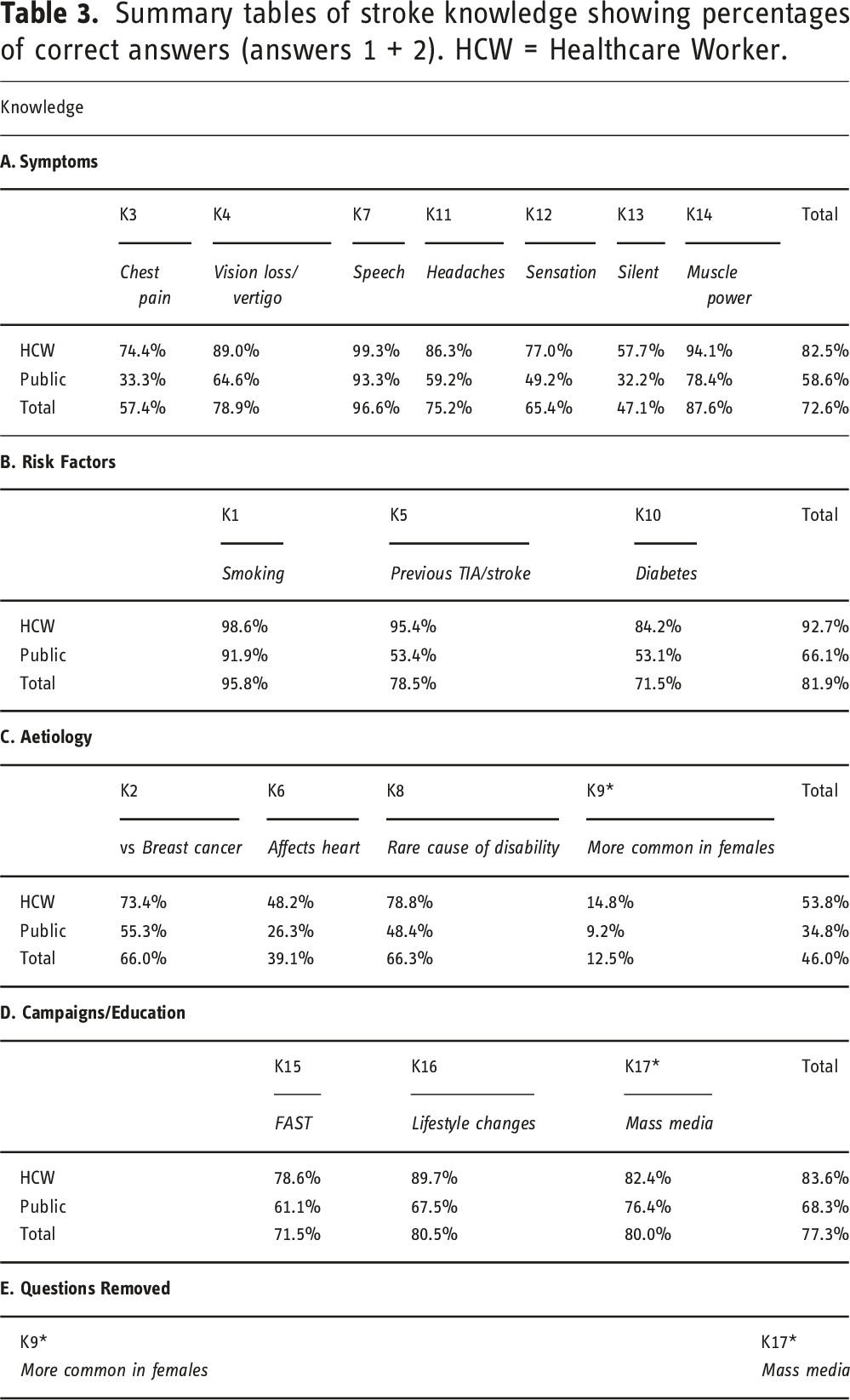
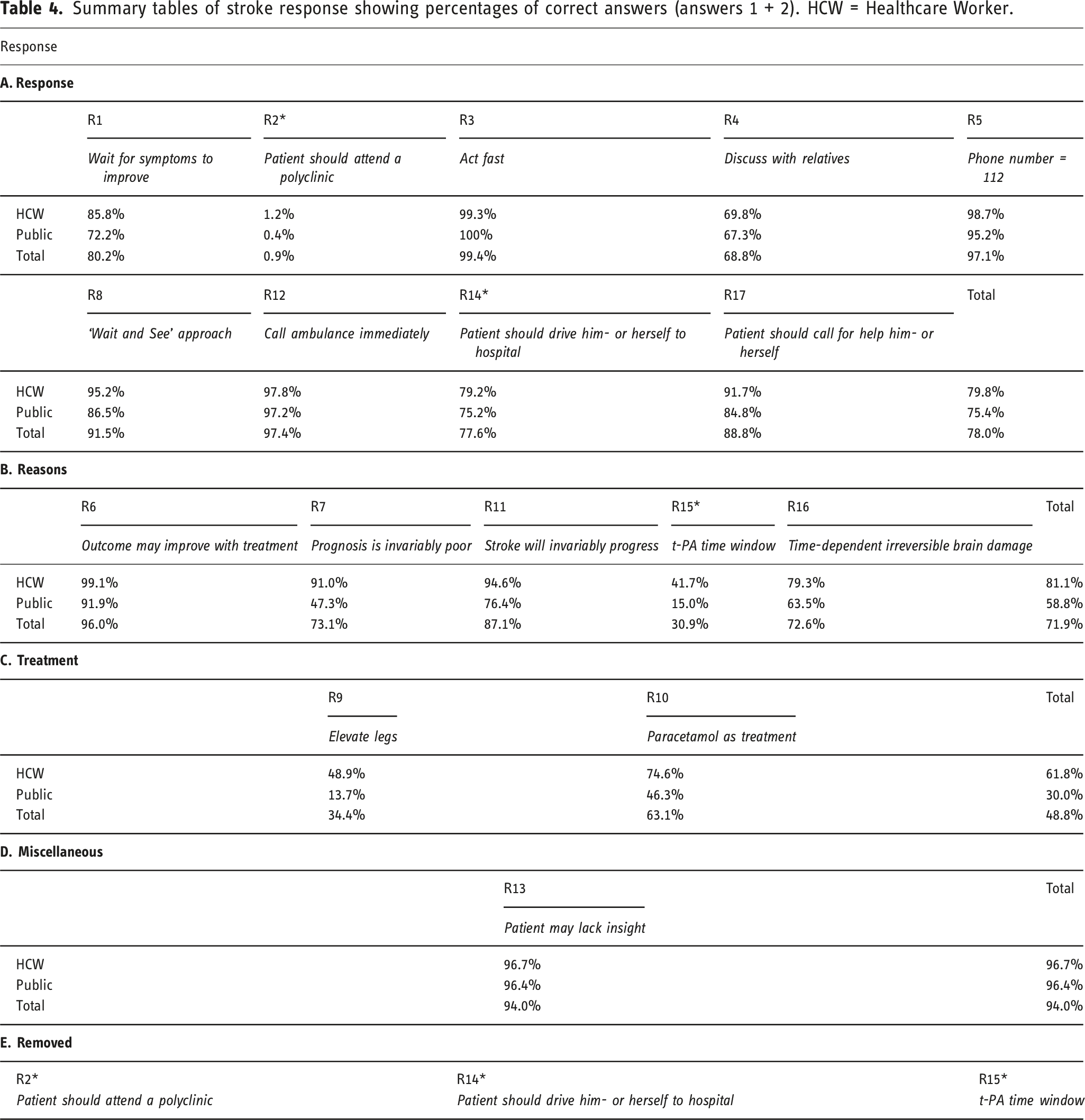
The knowledge and response sections of the questionnaire employed a 5-point Likert scale to measure participants’ responses, which were scored based on correctness: strongly agree, agree, undecided, disagree, and strongly disagree. Each response was coded and mean scores for knowledge (K1-K17) (Figure 3, Table 1) and response (R1-R17) (Figure 4, Table 2) items were calculated. Knowledge scores highlighted key educational gaps, particularly in areas such as stroke symptoms, risk factors, aetiology, and the impact of educational campaigns. Mean scores indicated that participants generally struggled with specific knowledge questions, revealing significant gaps in stroke awareness (Table 3). Similarly, response scores provided insights into the respondents’ ability to correctly identify and act upon stroke symptoms (Table 4). Healthcare workers consistently scored higher than the public, reflecting their professional training. Overall, these descriptive statistics underscored the need for targeted educational interventions to address the identified gaps in stroke knowledge and response among the Maltese population. Mean scores for knowledge questions. Knowledge scores and means. sum is the total score of the question (k1-k16). The next column shows the mean score of the same question. Mean scores for response questions. Response scores and means. sum is the total score of the question (k1-k16). The next column shows the mean score of the same question. Summary tables of stroke knowledge showing percentages of correct answers (answers 1 + 2). HCW = Healthcare Worker. Summary tables of stroke response showing percentages of correct answers (answers 1 + 2). HCW = Healthcare Worker.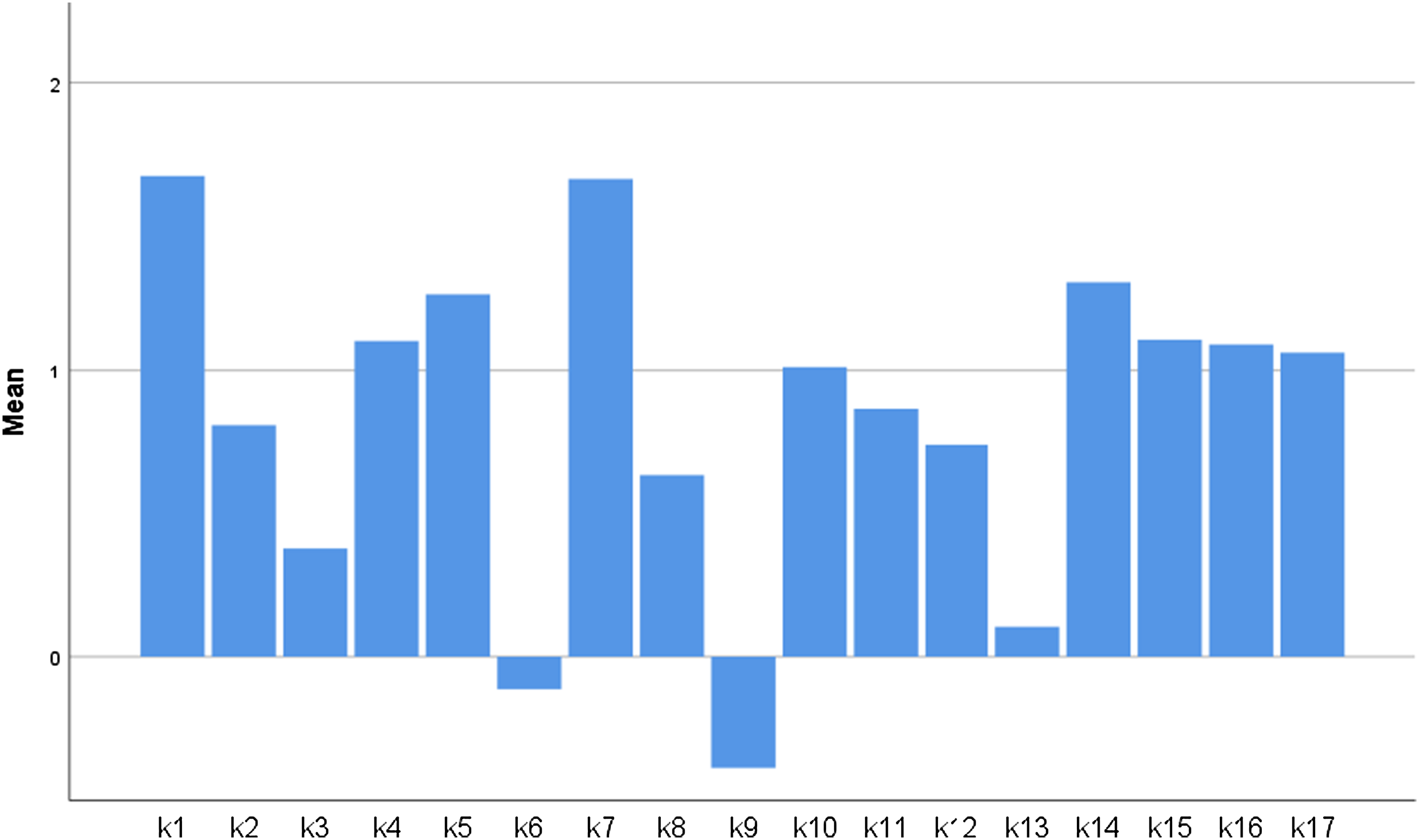
Inferential statistics
Inferential statistics were employed to analyse stroke knowledge and response among 1872 Maltese respondents, focusing on variables such as age, gender, ethnicity, region, education, income, risk factors, and healthcare worker status.
The degree of non-normality in the data was assessed using the Shapiro–Wilk test. For both the pilot study and the total sample of 1872 responses, the p-values for Knowledge Score, Response Score, and Total Score were all below 0.05, indicating that the distributions were significantly skewed and did not meet the normality assumption. Specifically, the p-values for these tests were approximately zero, leading to the rejection of the null hypothesis of normality. Additionally, the distribution curves for Knowledge and Response scores were found to be flatter and left-skewed compared to a normal distribution. This necessitates the use of non-parametric tests. The Kruskal–Wallis test revealed significant differences across demographic groups.
Age emerged as a crucial factor, with younger participants exhibiting higher mean ranks for knowledge, response, and total scores compared to older participants, suggesting that stroke-related knowledge and response efficacy decline with age.
Gender differences were also notable, with males generally scoring higher than females in knowledge and response metrics, although the differences were not always statistically significant.
Ethnic background showed significant variation, with non-Maltese participants scoring higher on average, potentially reflecting diverse cultural influences on health knowledge and behaviours.
Regional analysis indicated that respondents from urban areas had higher mean ranks compared to those from rural regions, underscoring the potential impact of healthcare access and educational outreach.
Educational attainment was positively correlated with stroke knowledge and response scores, affirming that higher levels of formal education contribute to better health literacy.
Income levels similarly influenced scores, with higher-income groups demonstrating superior stroke-related knowledge and response behaviours, likely due to better access to health resources and information.
Among risk factors, a history of cardiovascular conditions was associated with higher knowledge scores, possibly due to increased exposure to medical advice and education. Healthcare workers unsurprisingly scored significantly higher (p < .05) than the public, reflecting their professional training and awareness.
Correlation analysis between knowledge and response scores showed a strong positive relationship (Figure 5), indicating that greater knowledge of stroke symptoms and risk factors is linked to more appropriate and timely responses to stroke events. Scatter plot of response score versus knowledge score.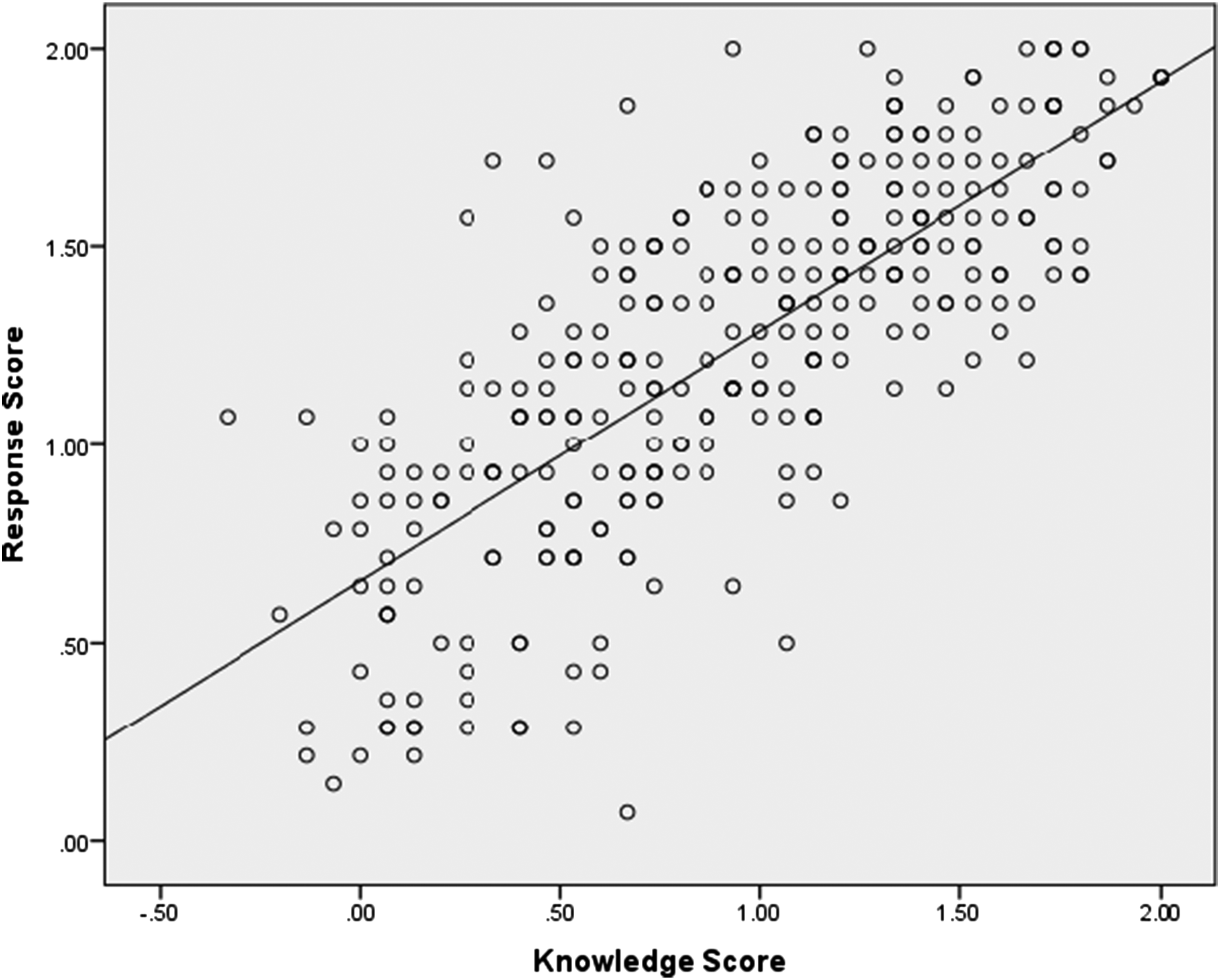
These findings highlight critical areas for targeted educational interventions, particularly for older adults, women, rural residents, and lower-income groups to improve stroke awareness and response. Enhancing public health strategies to address these disparities could lead to more effective stroke prevention and management, ultimately reducing morbidity and mortality associated with stroke.
This comprehensive analysis underscores the importance of demographic factors in shaping health knowledge and behaviours, providing a foundation for future research and policy development aimed at mitigating the impact of stroke through improved education and healthcare access. The study’s robust methodological approach, including the use of non-parametric tests to accommodate non-normal data distributions, enhances the reliability of these findings, offering valuable insights for public health practitioners and policymakers in Malta and similar settings.
Correlation between stroke knowledge and response
The correlation between stroke knowledge and response was analysed using Spearman’s rho, given that both datasets were non-normalized. The study found a Spearman correlation coefficient of 0.753 between knowledge and response scores, with a p-value approximately equal to 0, indicating a strong and statistically significant positive relationship between the two variables. This means that participants with higher stroke knowledge scores also tended to have higher response scores. This suggests that stroke educational campaigns could play a crucial role in enhancing stroke response, potentially reducing pre-hospital delays. Given the time-sensitive nature of stroke treatment, this could lead to increased administration of acute therapies, which are linked to better clinical outcomes. However, the study emphasizes that a high response score does not necessarily translate into appropriate action during a stroke event. Previous research by Fussman et al. 9 and Marx at al. 10 demonstrated that increased knowledge did not always result in the correct actions being taken during a stroke. Several factors might contribute to this dissociation between knowledge and action. Firstly, an affected individual might be physically or mentally unable to act appropriately following a stroke onset. Secondly, perceived barriers 11 might prevent patients from taking the correct actions. Lastly, unless patients believe they will benefit from the necessary actions, they may refrain from activating emergency services. These factors, along with the process of health-seeking behaviour and the perceived seriousness 12 and control of the situation, play critical roles in determining whether individuals will act appropriately during a stroke. Numerous health promotion theories aim to explain behaviour following a stroke and are crucial for understanding how stroke knowledge impacts the responses of patients and bystanders. 13
Discussion
The study reveals a concerning inverse relationship between age and stroke knowledge, with older individuals, despite being at higher risk, demonstrating lower awareness and understanding of stroke symptoms and appropriate responses. This trend also extends to individuals with multiple risk factors for stroke, who paradoxically display lower levels of knowledge compared to those without such risks. These findings suggest that existing educational strategies are not effectively reaching or engaging these vulnerable groups. Furthermore, the study highlights the positive correlation between higher levels of academic education and better stroke knowledge and response, suggesting that educational attainment plays a critical role in enhancing health literacy and prompting timely medical intervention. Similarly, individuals with higher-income levels and those working in healthcare settings show better stroke awareness and are more likely to take appropriate actions during a stroke event.
One cannot emphasize enough the role of psychological barriers, such as feelings of helplessness and fatalistic attitudes, which can impede timely medical intervention. These barriers highlight the need for educational initiatives that not only provide information but also address these psychological factors, encouraging a more proactive approach to stroke symptoms. Inappropriate stroke responses are often attributed to anxiety, lack of insight, failure to recognize symptoms, and the influence of significant others who may also lack adequate knowledge. These findings underscore the necessity for targeted education strategies that focus on both individuals at risk and their immediate social circles to ensure a supportive and informed response network.
To improve stroke education in Malta, a structured framework should be developed, incorporating needs assessment, comprehensive educational strategies, pilot testing, phased implementation, ongoing monitoring, and sustainability measures. First, local community surveys and systematic record-keeping should identify educational gaps and monitor awareness levels, particularly among high-risk groups. Based on these findings, a culturally sensitive educational program can be designed, targeting multiple levels (individual, family, community, and healthcare system) using a combination of mass media and in-person community programs. The program should initially be pilot-tested in selected regions before a national roll-out, allowing for adjustment based on initial feedback. Monitoring and evaluation would involve setting measurable objectives, using pre- and post-campaign surveys, and analysing healthcare data to assess program impact. Finally, sustainability efforts, including the integration of stroke education into routine public health activities and ongoing reinforcement through community-based sessions, would help ensure long-term effectiveness. This framework aims to enhance public stroke knowledge, reduce pre-hospital delays, and improve timely medical interventions across Malta. Post-stroke care recommendations emphasize the importance of lifestyle changes, motivational support, psychological care, and robust community support systems to aid recovery and prevent recurrent strokes. These holistic care approaches are essential for improving long-term outcomes and quality of life for stroke survivors.
Limitations of the study
Potential biases in both qualitative and quantitative data collection, include interviewer bias, recall bias, and selection bias. For instance, while the online survey method ensures accessibility, it may also introduce bias by excluding individuals without internet access or digital literacy. Although participants were given the option to complete the survey via a telephone call, this could still have been a source of bias. To reduce recall bias (in the qualitative phase of the study), bystanders were also interviewed when available, as their recollections were less likely to be influenced by the patient’s outcome. During study design, patients were recruited at an optimal time – neither too soon after the stroke (when emotions could affect recall) nor too late (when key details might be forgotten). This timeframe was defined in the inclusion criteria before recruitment began. It is crucial to recognize and mitigate these biases to ensure the accuracy and reliability of the findings.
Despite these limitations, the study demonstrates the value of a mixed methods approach, combining qualitative and quantitative data to provide a comprehensive understanding of stroke knowledge and response in Malta. This integrated approach informs the development of effective educational interventions and policy decisions, highlighting the need for ongoing research and adaptation of strategies to address the evolving needs of the population. The findings call for a concerted effort from healthcare providers, educators, and policymakers to implement these recommendations, ultimately aiming to reduce stroke incidence and improve outcomes for individuals and communities in Malta.
Conclusion
The study’s findings indicate that stroke knowledge in Malta is generally limited but aligns with existing literature, highlighting significant areas for improvement in public education. The correlation between stroke knowledge and the likelihood of appropriate action in the event of a stroke is significant, even when accounting for social and cultural barriers. To address this, new public education strategies are recommended, which should include culturally tailored descriptions of stroke symptoms, educational campaigns targeting a broader audience beyond high-risk patients, and emphasizing the availability of effective treatments that can improve outcomes. Moreover, the importance of seeking immediate medical attention for any stroke symptoms, however minor, must be stressed.
The study also reveals a concerning gap in stroke knowledge among stroke survivors, some of whom remain unfamiliar with stroke symptoms despite their personal experiences. This gap is attributed to a lack of motivation to make necessary lifestyle changes and an overall disinterest in learning about their condition, even when aware of the increased risk of recurrence. These insights point to the need for sustained support and education for stroke patients to help them manage risk factors effectively.
The findings further demonstrate that educational interventions must consider demographic variables, as stroke knowledge varies significantly with education level, age, and income. For instance, those with higher education and income levels displayed better stroke knowledge and response capabilities. This underscores the necessity for targeted educational efforts to bridge knowledge gaps among lower-income and less-educated populations. Additionally, cultural influences on stroke knowledge and response behaviours were noted, suggesting that educational materials and campaigns should be culturally sensitive and appropriate. Lastly, healthcare professionals must stay updated with evolving stroke treatment and practice guidelines to ensure the best possible care for stroke patients.
These results collectively suggest a multi-faceted approach to improving stroke knowledge and response in Malta, involving public education reforms, targeted interventions for vulnerable demographics, and ongoing professional development for healthcare workers. The scores generated by the Stroke Knowledge Tool allow for temporal comparisons within the same population and facilitate the comparison of stroke knowledge across different populations or countries. Additionally, these scores highlight knowledge disparities based on demographic factors (e.g. age and gender), assisting in the targeted planning of future stroke education campaigns.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.