
Abstract
Moving research evidence to practice can take years, if not decades, which denies stroke patients and families from receiving the best care. We present the results of an international consensus process prioritizing what research evidence to implement into stroke rehabilitation practice to have maximal impact. An international 10-member Knowledge Translation Working Group collaborated over a six-month period via videoconferences and a two-day face-to-face meeting. The process was informed from surveys received from 112 consumers/family members and 502 health care providers in over 28 countries, as well as from an international advisory of 20 representatives from 13 countries. From this consensus process, five of the nine identified priorities relate to service delivery (interdisciplinary care, screening and assessment, clinical practice guidelines, intensity, family support) and are generally feasible to implement or improve upon today. Readily available website resources are identified to help health care providers harness the necessary means to implement existing knowledge and solutions to improve service delivery. The remaining four priorities relate to system issues (access to services, transitions in care) and resources (equipment/technology, staffing) and are acknowledged to be more difficult to implement. We recommend that health care providers, managers, and organizations determine whether the priorities we identified are gaps in their local practice, and if so, consider implementation solutions to address them to improve the quality of lives of people living with stroke.
Introduction
In recent years, there has been an exponential rise in the publication of randomized controlled trials in stroke rehabilitation; more than 2000 trials inform our practice. 1 Given the significant resources invested in this production and the importance of the knowledge generated, concerted efforts should be taken to move relevant research evidence into practice.
The process of moving research into practice falls under the broader umbrella of knowledge translation (KT). 2 Historically, there has been a large time gap, if not decades between the generation of evidence and its implementation in practice.3,4 While drug development can have a particularly long time lag, even new psychosocial and health service delivery interventions have typically taken over 10 years from the start of phase 3 trials to implementation. 3 This evidence-to-practice gap denies patients the opportunity to benefit from more effective treatments and is a waste of the finite resources in today’s healthcare system. However, one should avoid the “KT imperative” which is a perceived notion to implement all research at all cost. 5 Clearly a process for determining the most impactful research to be implemented is needed.
The overall objective of this project was to identify what stroke rehabilitation research or knowledge to move to practice to have the maximum impact for people after stroke. Relevant stakeholder involvement is essential for prioritizing what research evidence to implement, including the end users; those delivering and those receiving the treatment. 6 Health care providers are most aware of what is currently delivered in practice and where gaps may lie. Patient involvement can change the priorities for healthcare improvement 7 thereby improving their quality and relevance. 8
Prioritizing what should be translated into stroke rehabilitation practice can assist health care providers, managers, and health care organizations in their decision-making and has the potential to have an immediate impact on the quality of lives of people living with stroke. It can also provide guidance for KT researchers and funders as to where to direct their efforts for maximum effect. Lastly, prioritizing KT initiatives can lead to resource development that informs us how to implement specific activities, as well as lead to national and international collaborations to address these practice gaps.
Methods
KT Working Group
The Stroke Recovery and Rehabilitation Roundtable (SRRR) is an international collaboration to accelerate stroke treatments and effective care in rehabilitation practice and this paper represents activities from the second Roundtable. 9 From this network, a KT Working Group was assembled with the aim of ensuring an international perspective, including representation from low- and middle-income countries (LMICs). The 10-member group was geographically spread over North America, Europe, Asia, Africa, and Australia, and had representation from a consumer living with stroke, as well as experts with stroke rehabilitation backgrounds in KT, medicine, physical therapy (PT), occupational therapy (OT), nursing, speech and language pathology (SLP), and management. The Working Group interacted over videoconference and email discussions for six months leading to the face-to-face meeting and undertook the following five steps.
Step 1. Assemble an International Advisory to Achieve Global Perspectives
Recognizing the limits of our small working group, we assembled a larger international advisory group with a mandate to provide additional feedback on our processes, and to assist in seeking input from their local health providers and consumers with stroke. The advisory was solicited from contacts of the wider SRRR Executive and KT Working Group. The international advisory group consisted of 20 representatives from 13 countries (Australia, Brazil, Canada, China, India, Kyrgyzstan, Malaysia, New Zealand, Nigeria, Pakistan, Philippines, Singapore, and the UK) and represented eight professions (neurology, rehabilitation medicine, psychology, OT, PT, SLP, dentistry, nursing).
Step 2: Identify Factors to Consider When Prioritizing Treatments to Move to Practice
The Working Group identified factors to consider when prioritizing treatments or processes to move to practice based on a literature review.10,11 Working Group members individually ranked the factors in order of importance and this data was aggregate rank-ordered 12 with the result that the most important factor was (1) level of evidence (i.e. included consideration of the research design, the size of effect, confidence intervals, sample sizes and relevance of the evidence); (2) personal impact (i.e., Impact on the patient’s quality of life); (3) feasibility (including consideration of local context); and lastly (4) system impact (i.e. impact on the health care system). Treatments were subsequently viewed through the lens of all these factors.
Step 3: Gather Input From Health Care Providers
The Working Group developed a survey with input from the International Advisory to gather perspectives from health care providers on KT priorities for stroke rehabilitation and distributed through the SRRR Executive, the KT Working Group and International Advisory. The survey was translated into Chinese and Portuguese. The survey informed the respondent that not all effective treatments are currently delivered or implemented in every region and asked the respondent to provide up to three examples of treatments or services they thought, based on their knowledge and experience, would have the largest impact on the problems that people have during stroke recovery and rehabilitation. The core survey questions are documented in online Appendix 1.
Step 4: Gather Input From Consumers
The Working Group developed a similar survey (online Appendix 1) to gather wide input from consumers and caregivers, and this was distributed to the same networks as previously mentioned. Approval for the health provider and consumer surveys were obtained from the university’s research ethics board and the local health authority and participants provided informed consent.
Step 5: Prioritize Treatments and Processes to Move to Practice Through a Face-to-Face Consensus Meeting
Two members of the Working Group consolidated the data, independently reducing redundancies and identifying topics, and then comparing for consensus. Recurring topics were identified and background information on the four factors (level of evidence, personal impact, feasibility, system impact) were collated for each topic from existing clinical practice guidelines, Cochrane Reviews, meta-analyses, the Evidence-based Reviews in Stroke Rehabilitation, 1 and studies on patient preferences. 13 At a two-day face-to-face meeting, the Working Group reviewed the survey data and background information and were asked to keep in mind the four factors and their order previously established. The Working Group further consolidated the list of topics and each remaining topic was voted on anonymously (yes/no) to produce a core set of priorities. These priorities were reported back to the entire SRRR collaboration (n = 41) for additional roundtable discussion.
Results
Consumer Survey
A total of 112 people responded to the survey and provided a total of 312 examples or topics. The respondents were primarily consumers living with stroke (97) and the rest were family or caregivers.
The largest response was from Canadian participants (72%) with smaller representation from Australia, Germany, India, UK, and USA. A total of 11 consolidated topics were identified.
Health Care Provider Survey
A total of 502 people responded to the survey and provided a total of 1452 topics. The respondents had the following backgrounds: PT (39%); physician (17%); SLP (14%), OT (14%), nursing (8%), psychology, (2%), and other (5%). Respondents were from 28 countries with 31% responses from LMICs and 69% from high-income countries (HICs). The largest response from HICs was from Australia (20%), the UK (16%), Canada (13%) and the USA (7%). The largest response from LMICs was from China (13%), Brazil (8%), and India (7%). A total of 14 consolidated topics were identified.
Consensus on Priorities
The 14 health provider topics spanned the 11 consumer topics, although not in the same groupings or with the same frequency. For example, interdisciplinary care was cited frequently by the health care providers, while social isolation and family support was frequent with consumers. Access to care was cited frequently by both groups. The largest discrepancy between the health care provider and consumer responses was the topic of fatigue which was highlighted by approximately 10% of consumers, but by less than 1% of the healthcare providers.
After discussion, two of the 14 topics were combined and members then voted whether to retain each of the 13 topics. Nine topics had at least 90% of the members agreeing that it should remain a priority, and the rest had less than 50% consensus. The group decided not to rank-order the topics as the subset was small and differences unlikely to be meaningful. These nine topics were grouped into three domains using an inductive approach. Service Delivery (intervention at the practice level) System (interventions at the system level) Resource (staffing/equipment)
Table 1 provides a short description of the topics included in each domain with supporting quotes from the data. While the labels were meant to represent topics highlighted by health care providers and consumers, they are not independent; for example, more access to services was categorized in the System Domain and could potentially facilitate more intensity of rehabilitation in the Service Delivery Domain. Staffing of clinicians was categorized as both a Resource Domain (with respect to the number of clinicians) and Delivery Domain (with respect to the expertise of clinicians).
Description of identified implementation priorities and evidence.
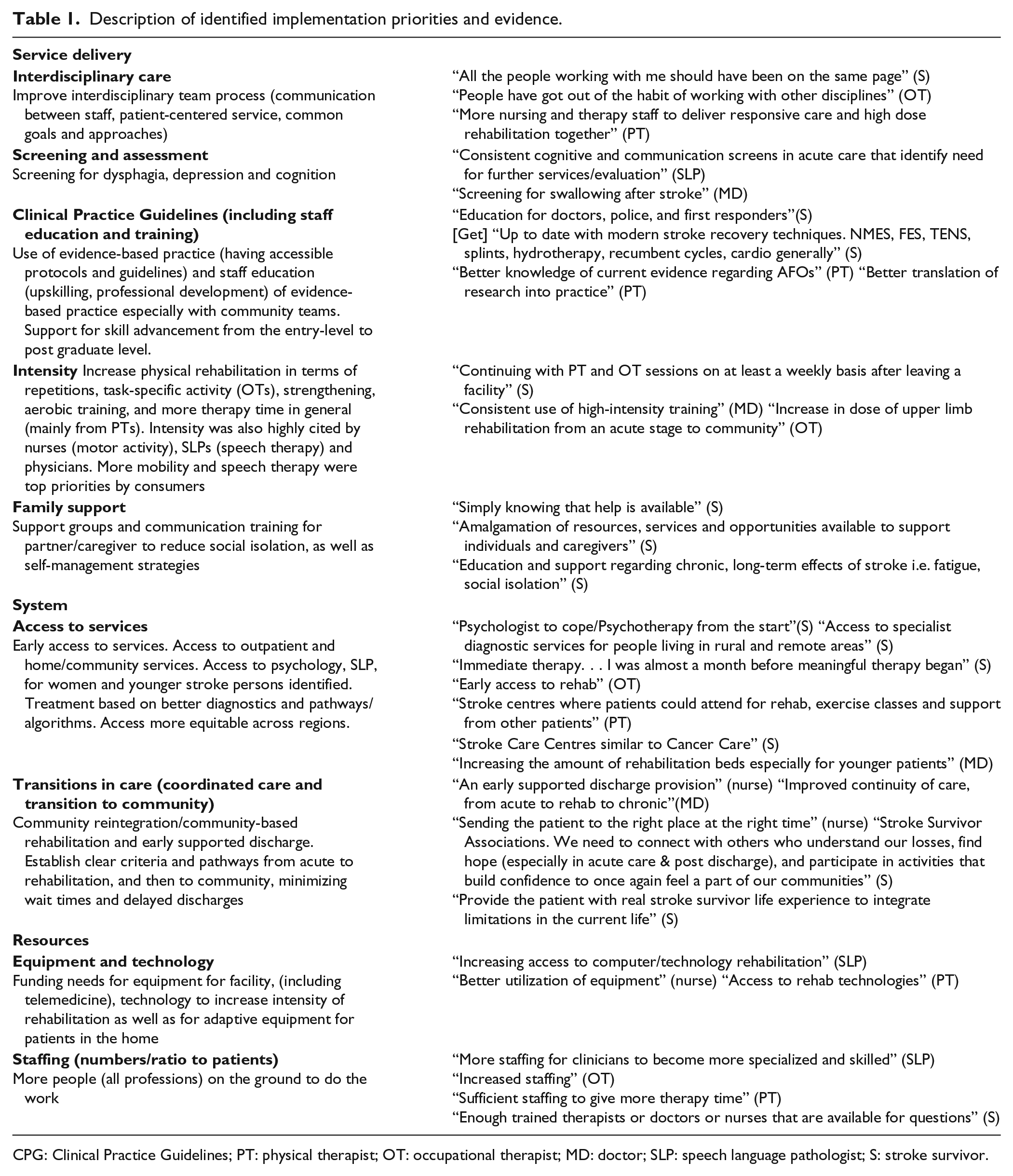
CPG: Clinical Practice Guidelines; PT: physical therapist; OT: occupational therapist; MD: doctor; SLP: speech language pathologist; S: stroke survivor.
LMIC Versus HICs
Most topics spanned across LMICs and HICs. There were some differences with intensity being a topic primarily from HICs (34% vs. 8%). Intensity related to more patient therapy time or activity (e.g. nursing, physical or occupational therapy, speech therapy) or higher levels of physical activity (greater repetitions, strengthening, aerobic training). Very few LMICs (2%) prioritized transitions to care while 14% of HICs did.
Health Care Provider Priorities
Topics of interdisciplinary care, access to services, intensity, staffing and transitions in care spanned across health care providers. Screening and assessment were most frequently identified by physicians.
A small number of discipline-specific topics were identified and included functional electrical stimulation (physical therapy), aphasia/communication training (speech therapy), and continence (nursing), but were not frequent enough to warrant a separate topic.
Discussion
This project utilized input from a range of stakeholders across the world from LMICs and HICs to achieve consensus on priorities for implementing research evidence into stroke rehabilitation practice. We recommend that health care providers, stroke rehabilitation teams and their managers use these recommendations to inform efforts to improve their services and practice. We provide an infographic (Figure 1) which summarizes our findings for front-line clinicians. We recommend that the identified priorities can be used by funding agencies to target implementation activities. We also recommend that researchers develop methods to facilitate implementation of these activities into practice, e.g. toolkit to audit and facilitate interdisciplinary care. This is particularly relevant as a recent systematic review found only 16 RCTs which evaluated the effectiveness of KT interventions for changing clinician behaviour or patient outcomes in stroke rehabilitation. 14
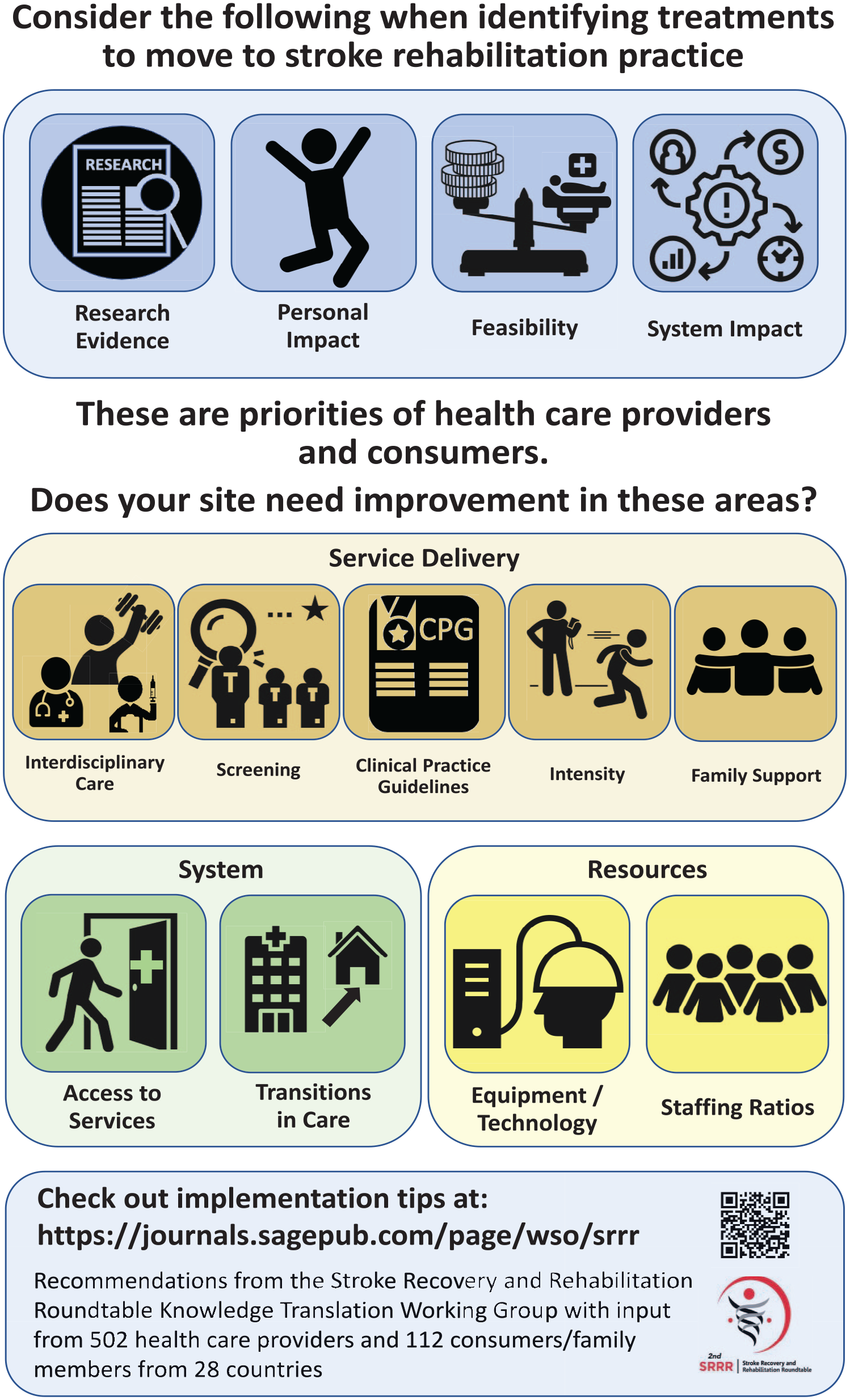
Infographics on implementation priorities from the consensus-based core recommendations of the Stroke Recovery and Rehabilitation Roundtable.
There was general overlap between the consumer and health care provider priorities except for the topic of fatigue. While the Working Group acknowledged the high prevalence and considerable impact of fatigue, they felt that fatigue was not adequately treated in part due to the lack of effective treatments at this time,15,16 and hence a need for further primary research rather than implementation activities. The topic of social isolation was also frequently raised by consumers, and to a lesser extent by healthcare providers and may reflect a lack of knowledge on how to assess or treat social isolation, or implement available treatments. Social isolation is amenable to change and a meta-analysis found that activities that encouraged individuals to leave the house and interact with others, as well as exercise activities could improve social participation. 17 Addressing social isolation in the future with implementation research meets this consumer identified need.
Five of the priorities related to service delivery are generally feasible to implement or improve upon. Suggestions for validated protocols and implementation toolkits relating to the priorities are available at https://journals.sagepub.com/page/wso/srrr and listed in online Appendix 2. For example, screening for dysphagia, cognition and depression has validated screening assessments in multiple languages, straight-forward performance metrics (e.g. proportion of patients screened with documentation), well-defined implementation protocols and do not require advanced technology or highly skilled staff. Their implementation can translate into cost savings by reducing secondary complications and length of stay.18,19 Detailed evidence-based protocols exist to increase the intensity of rehabilitation (online Appendix 2, Intensity) and include group programs, aerobic protocols as well as the use of rehabilitation assistants and caregivers. While a Cochrane Review suggested some benefits of caregivers in assisting with stroke patient exercises, 20 some caution should be exerted in light of the lack of effects from the recent ATTEND trial 21 (n = 1250) and the RECOVER trial 22 (n = 246) which used family caregivers in India and China, respectively, to augment the delivery of stroke rehabilitation (e.g. mobility, self-care).
It is recognized that system and resource issues are more difficult to change. For example, transitions in care require coordination from multiple centres or units. However, a first step could document the critical performance metrics (see online Appendix 2, Transitions in Care) to demonstrate whether care is satisfactory or not.
Rehabilitation interventions are frequently complex, multi-component activities which typically require tailoring to the individual, as well to the local setting. Currently the research community does not sufficiently define their intervention protocols nor identify the active ingredients. 23 From the first SRRR Roundtable, 15 consensus-based recommendations were established related to intervention development, monitoring and reporting to address this gap 23 (e.g. provide a clear description of core intervention components that must be delivered; build an assessment of fidelity into the trial protocol). Journals should endorse reporting guidelines such as these that enable complete and transparent reporting to facilitate translation of the protocol to the real-world setting.
Adherence to evidence-based guidelines is challenging especially as assembling an evidence-based protocol can be difficult for front-line clinicians. The availability of free implementation toolkits (online Appendix 2) overcomes some of the barriers for moving research to practice but are scarce to find. We recommend that future practice guidelines be developed with specific performance metrics that stroke programs can use to measure their adherence and include samples of evidence-based protocols to achieve these milestones. These protocols would benefit from stakeholder input (e.g. front-line health care providers, rehabilitation managers, patients) to ensure that they are feasible and acceptable.
Furthermore, rehabilitation settings need to ensure that staff time, education and resources are sufficient when trying to change clinician behaviour to better adhere to evidence-based guidelines 24 ; support from management is critical for overcoming these barriers and for successful implementation.
Stroke disproportionately impacts LMICs, where individuals have more severe stroke and greater disability and are more likely to have inadequate access to quality care in the acute and rehabilitation phases than those with higher socioeconomic status. 25 Transitions in care was not identified as a priority by LMICs, possibly reflecting the fact that many LMICs have some rehabilitation care primarily in the acute setting with little follow-up into the community. Screening for dysphagia, depression, and cognition was frequently cited by LMICs and is highly relevant in the earlier phase of stroke recovery and could make a substantial impact on patient outcomes.
There are limitations in this dataset. Some professions (e.g. PTs, physicians) had greater representation in the health provider survey than others (e.g. psychologists), although we did analyze across, as well as within professions to identify the most common topics to reduce these biases. While the health care providers represented a variety of countries, the consumers were predominantly from one country (Canada) which may have biased the results.
Conclusions
This study identified priorities and made specific recommendations for implementation in stroke rehabilitation from a wide range of stakeholders, providing useful information to drive decision-making in health care (Figure 1). Of note, the topic of fatigue was frequently raised by consumers but was not included as an implementation priority, but rather a topic requiring more primary research. Social isolation was a common concern from consumers, and healthcare providers should be aware of how to assess social isolation and implement available treatments. The criteria and processes described in the methodology are transferable and may be used by other researchers looking to prioritize implementation of research in their clinical areas. We also challenge researchers to develop effective resources to facilitate implementation of these activities into practice, e.g. toolkit to audit and facilitate interdisciplinary care.
Footnotes
Acknowledgements
We would like to acknowledge our International Advisory—Drs Myzoon Ali, Karen Borschmann, Lilian Braighi Carvalho, Louise Connell, Rebecca Fisher, Lay Fong, Nalia Gurgel-Juarez, Nicola Hayes, Victor Iki, Ayeesha Kamal, Sandra Lever, Elizabeth Lynch, Sandy Middleton, Jacqui Morris, Jeyaraj Pandian, Yue Wang, Shaoshi Wang and Mr Gerado Dimaglia. We would like to acknowledge Julie Bernhardt for convening the second Stroke Rehabilitation and Recovery Roundtable (SRRR II), Dale Corbett and Karen Borschmann for organizing the meeting, and Farrell Leibovitch for moderating discussions.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclose receipt of the following financial support to conduct this meeting: Canadian Institutes of Health Research (CIHR) CaSTOR (Canadian Stroke Trials for Optimized Results) Group (note that CasTOR is a joint initiative of the Canadian Stroke Consortium and the Canadian Partnership for Stroke Recovery), Heart and Stroke Canadian Partnership for Stroke Recovery, and NHMRC Centre of Research Excellence in Stroke Rehabilitation and Brain Recovery. An unrestricted educational grant was provided by Ipsen Pharma.