
Abstract
Objective. The aim of this study was to assess whether the combination of Adapted Physical Activity (APA) and Therapeutic Patient Education (TPE) improves function and quality of life in survivors of strokes. Methods. This nonrandomized controlled study enrolled patients with mild to moderate hemiparesis referred to 2 physical medicine and rehabilitation units in Emilia-Romagna, Italy, 3 to 18 months after a single unilateral mild to moderate stroke. The experimental group (n = 126) received 16 APA sessions and 3 sessions of TPE, and the control group (n = 103) received usual care; 86.9% completed treatment. The main outcome measure was a 4-month change in gait endurance (that corresponds to 2 months after intervention in the experimental group), and secondary outcomes included the Short Physical Performance Battery, Berg Balance Scale, Barthel Index, Geriatric Depression Scale, 12-item Short-Form Health Survey, and Caregiver Strain Index. Changes in scores at 4 months were compared between groups using analysis of variance and controlling for group imbalance by means of the propensity score. Results. Gait endurance, physical performance, balance, and the physical component of the quality of life score increased significantly at 4 months in the APA group and remained stable in the control group. The propensity-adjusted between-group change was significant for these scores at P < .01. Conclusions. Our results confirm that it is feasible and potentially effective to implement APA programs for elderly patients with complex clinical conditions as early as 3 months after a stroke and suggest that, when combined with TPE, the effects of a postrehabilitation APA program are relatively enduring.
A stroke is one of the main public health concerns because it is a leading cause of death and long-term disability in elderly people. 1 Among countries of the European Union, Italy has the highest percentage of people >65 years of age (19.9%), with an expected number of 195,000 new cases of strokes per year in 2020. 2 Responding to the need for secondary and tertiary prevention strategies to improve function after strokes and prevent or delay subsequent strokes as well as other disabling conditions, Italy has pioneered the development of Adapted Physical Activity (APA). This study is the first to evaluate the safety of APA for survivors of strokes as early as 3 months after a stroke and to combine APA with Therapeutic Patient Education (TPE), providing an intervention specifically designed to transition patients from rehabilitation to community living.
Background
The growing literature in the last decade suggests that the implementation of preventive strategies is important to reduce the burden of chronic disease on health care systems 3 and highlights the positive potential of exercise for survivors of strokes. Increasing evidence links exercise for survivors of strokes to the preventive benefits of improved cardiovascular health, physical fitness, ambulatory function, 4 and bone health. 5 Exercise can lead to significant improvements in balance 6 and a decreased risk of falling, 7 a potentially major risk reduction for patients with chronic strokes who are at a significantly increased risk of fractures. 8 In addition to affecting physical function, strokes influence mood, social participation, and quality of life. Depression after strokes is common, with an estimated prevalence ranging between 33% and 50%, and has been associated with a reduced quality of life and poor social participation.9,10 There is evidence that exercise may improve quality of life 11 and reduce depressive symptoms and social isolation after strokes. 4 Furthermore, converging evidence supports a positive role for exercise in the prevention of a stroke and its sequelae. 12
Since 2004, the American Heart Association guidelines 13 have recommended physical activity for survivors of strokes, but limited evidence exists on outcomes of exercise programs after discharge from hospital rehabilitation. Unfortunately, various behavioral and psychosocial barriers associated with disability and aging and the lack of adequate community gymnasiums influence the adherence to exercise programs, resulting in patients with strokes deconditioning after rehabilitation. 14 Relatively few studies of the effects of community-based exercise programs for strokes have been conducted; however, these have consistently found that community group exercise is associated with improvements in mobility, functioning, and quality of life in patients with chronic strokes.5,15,16 Cramp et al 17 report that participants’ muscle strength and walking speed increased significantly during the training period in a small community-based study. A larger randomized trial (N = 243) found that a community-based program improved physical functioning and psychological well-being. 18
A recent Cochrane review 19 concluded that “cardiorespiratory training reduces disability after stroke and this may be mediated by improved mobility and balance. There is sufficient evidence to incorporate cardiorespiratory and mixed training, involving walking, within post-stroke rehabilitation programs to improve the speed and tolerance of walking; improvement in balance may also occur.”
Services for exercise after strokes are developing in different countries, based on existing evidence about the benefits of exercise after strokes. The Cochrane Collaboration advocated larger clinical trials to assess the effects of physical training after strokes and to determine the optimal regimen for improving fitness. The review suggested a broader population of survivors of strokes (to allow stratification by sex, level of impairment, and functional ability) and long-term follow-up.
Important research questions remain, including the following: What are the best approaches for integrating exercise into a comprehensive risk reduction program for survivors of strokes? Are the health benefits associated with repeated exercise (eg, several short bouts of aerobic training) generalizable to the deconditioned patient with strokes, both within the first 3 to 6 months after the acute event and thereafter? What is the impact of exercise training on quality of life in patients who suffer the consequences of a stroke, including those with residual gait instability?
The Italian APA model, designed to improve health and function of survivors of chronic strokes, started in Azienda Unità Sanitaria Locale( AUSL) 11 Empoli, Tuscany, in December 2003. Two studies carried out by Macko et al 20 and Stuart et al 21 demonstrated the efficacy of APA in improving gait velocity, balance, physical performance, depression, and social participation. The first was a small, uncontrolled pilot feasibility study on 20 participants with chronic hemiparesis who completed a 2-month APA program. The second 21 subsequently confirmed the safety, feasibility, and efficacy of the “Empoli model” of APA group exercise in a larger 6-month community trial using geographic controls in 2009. While APA community classes have demonstrated success in providing social support for survivors of strokes to maintain a regular program of exercise, a gap remains in the transition from rehabilitation to the community. This transitional period is potentially a key time for survivors of strokes in adopting new healthy lifestyle behaviors.
Therefore, we planned a new study in the Emilia-Romagna region to maximize this window of opportunity for an effective transition by starting APA earlier, adding an educational component and engaging caregivers as well as patients. The educational component in the present study, TPE, was aimed primarily at improving patients’ awareness of exercise as an essential component of a healthy lifestyle and at increasing the capacity of self-management of chronic conditions. While effective disease-specific self-management programs exist for diabetes, asthma, and arthritis, there is limited evidence for strokes.22,23 This innovative approach emphasizes the patient’s central role in managing his or her health and highlights the potential for health systems to create a culture, organization, and mechanisms that promote the transition to a healthy community lifestyle and quality of life. We hypothesized that changes in functioning and quality of life would be higher in patients assigned to APA and TPE compared to the control group. We also expected that this intervention would increase the patients’ awareness of exercise as an essential component of a healthy lifestyle, thereby reinforcing the continuation of exercise following conclusion of the group exercise program.
Methods
Study Design
This was a prospective cohort study with nonrandomized concurrent controls. Participants (N = 229) completed rehabilitation at 2 similar hospitals, serving similar populations in Italy. The intervention group (Bologna) received APA, enhanced with TPE (APA-TPE). The control group (Reggio Emilia) received usual care, consisting of a planned follow-up in which patients were only encouraged to practice regular exercise. Both the intervention and control groups were assessed at baseline and 4 months (that corresponds to 2 months after the intervention in the experimental group). A 1-year follow-up study is ongoing.
Participants
The experimental sample included consecutive patients diagnosed with a stroke who were discharged home from the Physical Medicine and Rehabilitation Unit of Sant’Orsola Malpighi Hospital, Bologna, Italy, at the end of the rehabilitation program from November 2009 to May 2012. Patients recruited during the same period from the Physical Medicine and Rehabilitation Unit of IRCCS Santa Maria Nuova, Reggio Emilia, Italy, served as the control group and received usual care. The Reggio Emilia unit has similar characteristics as the Bologna unit in terms of the care pathway (from the acute phase in the stroke unit to the hospital and community rehabilitation) and clinical case mix.
Inclusion criteria were the following:
age >18 years;
a confirmed stroke according to the World Health Organization’s definition in the previous 3 to 18 months, with mild to moderate hemiparesis;
ability to walk 25 m independently (with or without an assistive device such as a cane);
discharged home from a rehabilitation center;
no need to continue physical therapy; and
informed consent to participate in the study.
Exclusion criteria were the following:
severe cognitive impairment (Mini-Mental State Examination [MMSE] <15/30 and/or a score >3 on the Disability Communication Scale),
severe heart failure or other medical conditions preventing participation in low-intensity exercise (Cumulative Illness Rating Scale [CIRS]: index of comorbidity >3), and
severe perceptual disorders (ie, deafness or blindness).
The Ethics Committee of the Hospital Trust Sant’Orsola Malpighi of Bologna and of the Hospital Trust Santa Maria Nuova of Reggio Emilia approved the study. All participants provided written informed consent after eligibility requirements were checked.
Outcome Measures
The primary outcome was the change in gait endurance (distance walked) from baseline to 4 months, measured using the 6-minute walk test (6MWT).24,25 This outcome has proven to be a clinically relevant indicator of function and prognosis after strokes. 26 Participants were evaluated at baseline and 4 months. The 4-month assessment was conducted by independent physical therapists who were not involved in the exercise programs. The MMSE and Disability Communication Scale were used to screen patients for cognitive impairment,27,28 while comorbidity was measured through the CIRS.29,30 The modified Barthel Index was used to assess the ability to perform activities of daily living. 31 Mobility was measured using the 6MWT, Short Physical Performance Battery (SPPB),32,33 Berg Balance Scale (BBS), 34 and Motricity Index. 35 The caregiver’s burden was assessed using the Caregiver Strain Index. 36 The presence and severity of depression were measured using the Geriatric Depression Scale. 37 Scores of 0 to 5 are considered normal, 6 to 8 indicate mild depression, and ≥9 indicate moderate to severe depression. The 12-item Short-Form Health Survey (SF-12) was used to assess health-related quality of life. 38 A self-reported visual analog scale (VAS), with a score from 0 to 100, was used to assess patients’ overall perception of their recovery from acute strokes.
Intervention
The experimental intervention (APA-TPE) included 3 group sessions of interactive TPE involving both patients and families/caregivers and 8 weeks of 1-hour long, twice-weekly APA group exercise sessions. 21 Usual care consisted of recommendations provided in the letter of discharge and 2 follow-up visits in a year (Table 1). The first TPE session was held by a physician and focused on the causes and mechanisms of strokes, the modifiable and nonmodifiable risk factors, the course of illness, and the extent to which recovery is possible. The second TPE session was held by physical therapists and aimed at discussing the consequences of strokes in terms of disability, how to cope with them through the use of aids, and how to adapt the home environment to one’s needs. The third TPE session set out the benefits of physical activity for maintaining a healthy lifestyle. During this session, physical therapists explained the sequences of exercises, and participants could directly experience the APA program to get used to performing the exercises themselves at home. Participants were given a booklet that illustrated the consequences of a sedentary lifestyle and the benefits of physical activity to maintain a healthy lifestyle and prevent complications. In addition, home exercises were described in detail along with a diary in which the patient recorded the physical activity carried out at home. The APA exercises were taken from a protocol specifically designed and standardized for strokes by Stuart et al 21 and include mobility, balance, and stretching. The sessions began with free walking around the gymnasium with a progressive increase in length of walking, from 6 minutes in the first week up to 12 minutes in 6 weeks. Then, the protocol included exercises of weight shifting from leg to leg, half-squats, hip rotational movements, leg-trunk flexions and extensions, and leg lifts. Participants, seated in chairs, completed upper limb stretching exercises including sit-to-stand, arm rolls, shoulder girdle rotations while both seated and standing, trunk twists, and hemi-pelvis lifting. At the end of each session, participants walked around an obstacle course of ropes and hoops placed on the floor. Participants were also encouraged to follow a home exercise program and to record the activities in the structured diary.
Components of the Experimental Group Program and of Usual Care.
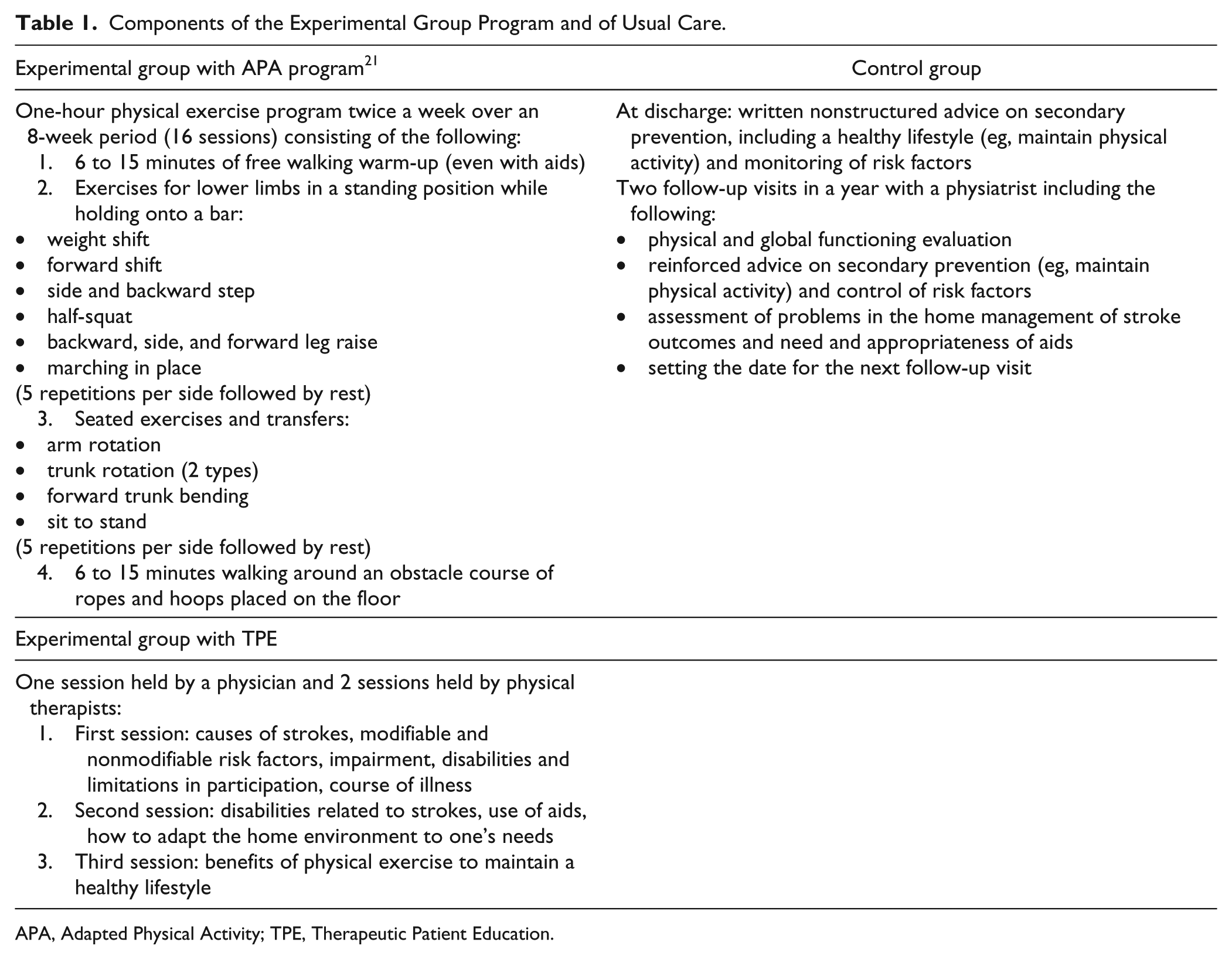
APA, Adapted Physical Activity; TPE, Therapeutic Patient Education.
Statistical Analyses
Patients in the APA groups were compared with those in the control group on demographic and clinical baseline characteristics using the t test, Mann-Whitney test, or χ2 test, as appropriate. Changes in clinical and functional measures were examined separately in each study group using the paired-samples t test or Wilcoxon test. Because the study groups are expected to differ in a nonrandomized study design, we used an analytic approach based on the propensity score 39 to compare changes in scores at 4 months between the APA-TPE group and controls after adjusting for group imbalance. The propensity score for an individual is the probability of being assigned to the experimental group conditional on (or based only on) the individual’s characteristics. Specifically, we estimated for each study participant the probability of being assigned to the experimental group as a function of demographic and clinical characteristics using logistic regression. All baseline variables significantly different between the 2 groups at P < .05 were included in the logistic regression as independent variables. To analyze the effect of the APA-TPE intervention, each outcome was then regressed on treatment status (1 = APA-TPE, 0 = control) and the estimated propensity score. A change in distance walked of 20 m was used as the minimal clinically important difference (MCID), in line with Perera et al. 40 All the analyses were carried out using IBM SPSS Statistics version 20.0 (IBM, Armonk, New York, USA).
Results
A total of 251 patients were assessed for eligibility. Twenty-two were excluded because they did not meet inclusion criteria (n = 12), declined to participate (n = 5), or could not be traced (n = 5) (Figure 1). Overall, 229 patients entered the study. Table 2 shows participants’ demographic and clinical characteristics at baseline. The 2 study groups had a similar mean age and sex distribution but differed in the number of characteristics. Specifically, blood pressure and the balance component of the SPPB were significantly higher in the control group than in the APA group; however, the MMSE score, BBS score, gait, repeated chair stands and the summary performance score of the SPPB, Motricity Index, distance walked of the 6MTW, Caregiver Strain Index, and Barthel Index were significantly higher in the APA group than in the control group. A higher percentage of patients in the APA group had right hemiparesis compared to the control group. Moreover, the time since a stroke was significantly higher in the experimental group in which 20% of patients were recruited 3 to 5 months after a stroke compared with 61% in the control group. Lastly, the Geriatric Depression Scale score was higher in the control group, with 85.7% of patients exceeding the threshold (≥6) for mild to severe depression compared with 67% in the APA group. The propensity score calculated for each study participant included days since a stroke, diastolic and systolic blood pressure, SPPB score, BBS score, Geriatric Depression Scale score, Motricity Index, Barthel Index, and walking endurance at baseline.
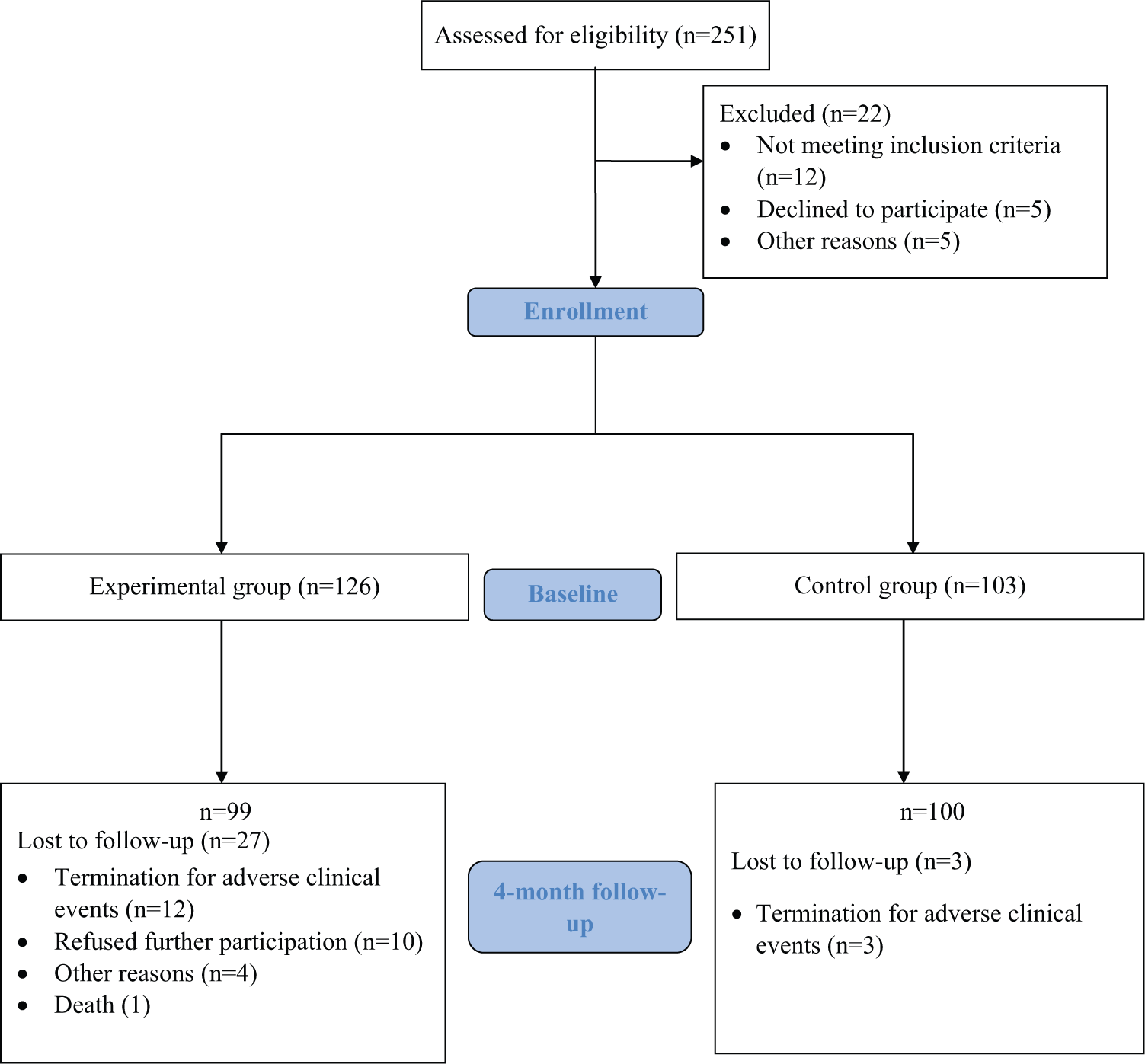
Study population.
Baseline Demographic Characteristics, Vital Parameters, and Psychometric Testing in the 2 Groups.
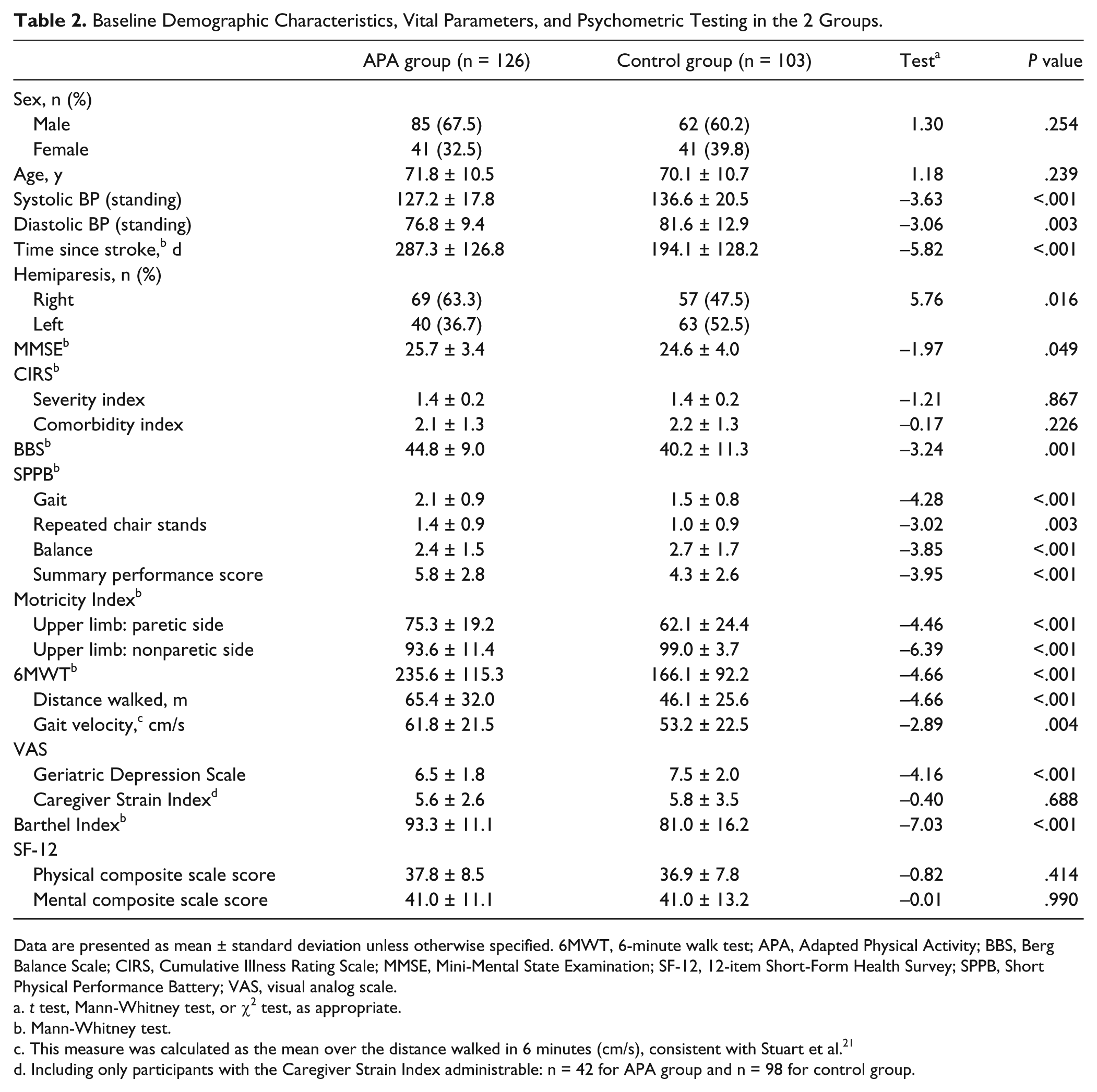
Data are presented as mean ± standard deviation unless otherwise specified. 6MWT, 6-minute walk test; APA, Adapted Physical Activity; BBS, Berg Balance Scale; CIRS, Cumulative Illness Rating Scale; MMSE, Mini-Mental State Examination; SF-12, 12-item Short-Form Health Survey; SPPB, Short Physical Performance Battery; VAS, visual analog scale.
t test, Mann-Whitney test, or χ2 test, as appropriate.
Mann-Whitney test.
This measure was calculated as the mean over the distance walked in 6 minutes (cm/s), consistent with Stuart et al. 21
Including only participants with the Caregiver Strain Index administrable: n = 42 for APA group and n = 98 for control group.
One hundred ninety-nine patients (86.9%) completed treatment, whereas 30 (13.1%) discontinued the program. The attrition rate was higher in the APA group compared with the control group (21.4% vs 2.9%, respectively;χ2 (df = 1) = 17.07, P < .001). Completers did not differ from dropouts on demographic and clinical variables, except for the Motricity Index of the upper limb of the nonparetic side and the SF-12 mental composite scale score that were significantly higher in completers.
Adherence to APA
Of the 99 patients in the APA group who completed the 4-month follow-up, 76 (76.8%) attended all 16 APA sessions, 9 (9.1%) attended 15 sessions, 11 (11.1%) attended 10 to 14 sessions, and only 3 participants (3.0%) attended <10 sessions. Moreover, 62.4% of patients completed the diary of their home exercise sessions.
4-Month Outcomes
Table 3 reports the total scores of clinical variables in the 2 groups at baseline and changes in scores from baseline to 4 months, adjusted for the propensity score. Gait endurance and velocity (6MTW), SPPB summary score, BBS score, and SF-12 physical composite scale score increased significantly at 4 months in the APA group and were unchanged in the control group. The changes from baseline to 4 months on these scores proved to be significantly different between the 2 groups. An MCID of 20 m in gait endurance was achieved by 50% in the experimental group and by 29% in the control group. A significant improvement on the Motricity Index of the paretic side, VAS score, and SF-12 mental composite scale score was found for the APA group and not for the control group, but propensity-adjusted changes in scores did not differ significantly between groups. No significant change from baseline to 4 months was found on the Caregiver Strain Index and Barthel Index. In assessing depression, we excluded those individuals with no depressive symptoms at baseline.
Clinical Measures at Baseline and Change at 4 Months.
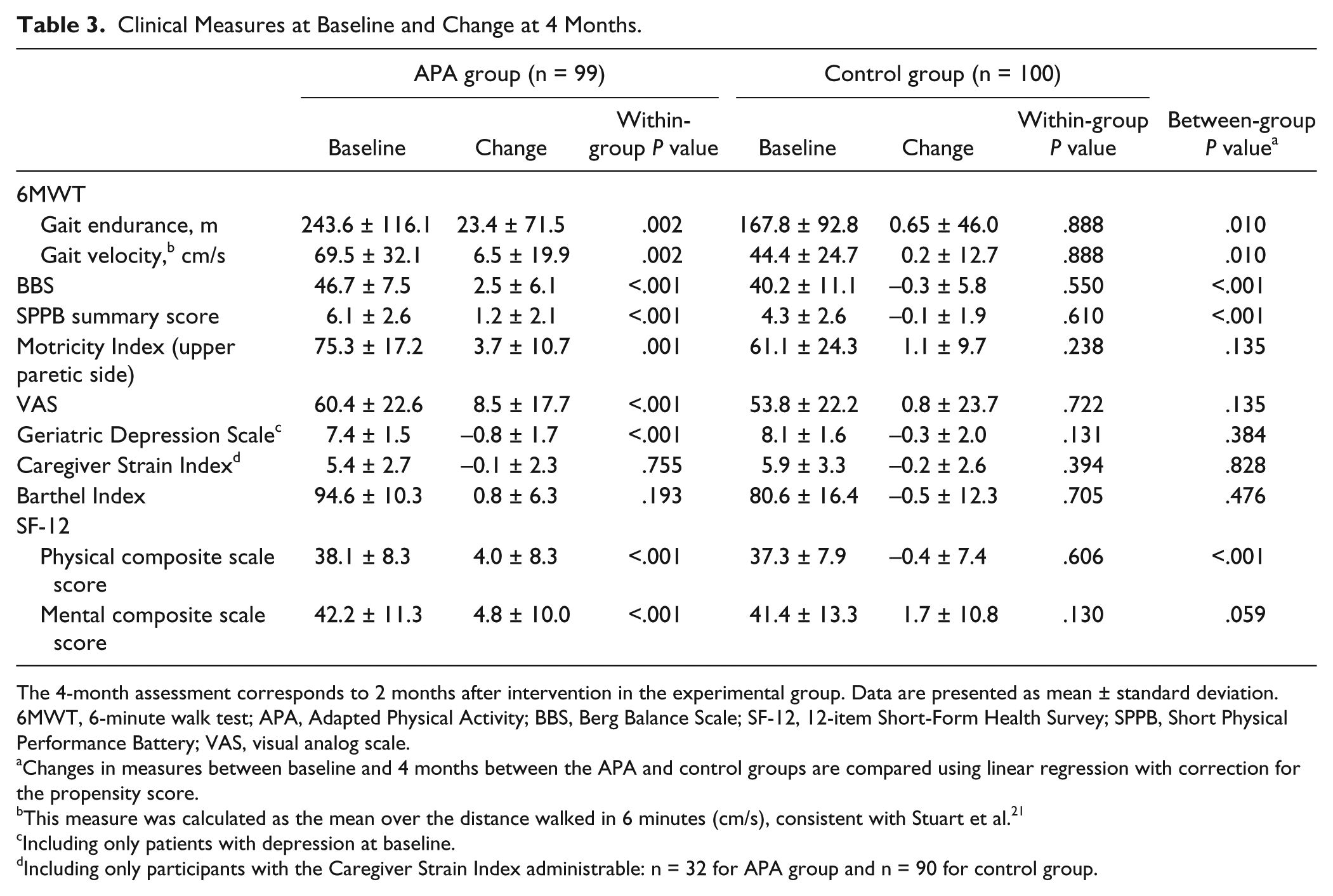
The 4-month assessment corresponds to 2 months after intervention in the experimental group. Data are presented as mean ± standard deviation. 6MWT, 6-minute walk test; APA, Adapted Physical Activity; BBS, Berg Balance Scale; SF-12, 12-item Short-Form Health Survey; SPPB, Short Physical Performance Battery; VAS, visual analog scale.
Changes in measures between baseline and 4 months between the APA and control groups are compared using linear regression with correction for the propensity score.
This measure was calculated as the mean over the distance walked in 6 minutes (cm/s), consistent with Stuart et al. 21
Including only patients with depression at baseline.
Including only participants with the Caregiver Strain Index administrable: n = 32 for APA group and n = 90 for control group.
When we examined patients depressed at baseline, a significantly higher proportion was improved at the 4-month follow-up (27.4% in the APA group had no symptoms compared with 15.9% in the control group; χ2 = 11.4, P = .003). Participants in the APA group improved a mean Geriatric Depression Scale score of 0.8 ± 1.7 points (paired-samples t test = 3.6, P < .001) compared to 0.3 ± 2.0 points (paired-samples t test = 1.5, P = .131) for controls. However, propensity-adjusted changes between groups on the Geriatric Depression Scale were not significantly different (F = 0.76, P = .384).
Moreover, we carried out a secondary analysis to examine in deeper detail the effect of time since a stroke on our primary outcome (change in gait endurance) in each group. This was done to take into account the mean difference of about 3 months in the time since a stroke between the 2 groups at study entry. A linear regression with the change in gait endurance as the dependent variable and time since a stroke as the independent variable showed that these variables were unrelated in each study group (APA-TPE group: b = −1.77, P = .319; control group: b = −0.77, P = .479).
Discussion
Our results indicate a significantly higher improvement in gait endurance among patients attending the APA-TPE program compared with those receiving usual care when assessed 2 months following the conclusion of the APA group exercise program. In particular, 50% of patients receiving the APA-TPE intervention improved their gait endurance over 6 minutes by at least 20 m compared with 29% of controls. A distance walked of 18 to 20 m was determined to be the MCID for fragile, elderly patients undergoing rehabilitation interventions.40,41 Our results add to the existing evidence from a systematic review of trials involving community-dwelling survivors of strokes that circuit class therapy is effective in improving walking ability. 42
The significant changes in mobility and balance found in the APA-TPE group, above and beyond those observed in the control group, confirm the efficacy of the program in terms of physical function. Moreover, both the mental and physical components of quality of life increased on average by 4 to 5 points in the APA-TPE group but remained stable or only modestly improved in the control group. Although quality of life is hard to affect in this population, it is noteworthy that APA-TPE provided some benefit, especially as measured by the SF-12 physical composite scale.
We found that patients with mild to severe depression at baseline benefitted more from APA-TPE than from usual care when we compared the proportion of patients recovered in the 2 groups. This result is consistent with a meta-analysis on rehabilitation and/or care coordination interventions delivered in the community that demonstrated a significant reduction in depression with exercise interventions (n = 137; effect estimate standardised mean difference (SMD) = −2.03; 95% confidence interval, −3.22 to −0.85). 9 Still, propensity-adjusted changes in Geriatric Depression Scale scores did not differ significantly between groups, suggesting that our results should be interpreted with caution because they depend on the use of a categorical or continuous measure of depression and on an adjustment for group imbalance.
As to the other secondary outcomes, we found that the Barthel Index did not change significantly during the follow-up in the 2 study groups. A likely reason for this finding is that patients at baseline had very high scores on this scale, and therefore, there was limited room for improvement during the intervention. Similarly, we did not find a significant change on the Caregiver Strain Index in the study groups. Our interpretation of this finding is that the burden on caregivers was similar before and after the intervention because patients were already able to walk independently for several meters at baseline.
A 1-year follow-up study is ongoing. The 1-year preliminary results indicate a lower number of falls, fractures, and readmissions in the experimental group compared to the control group. Should these preliminary results be confirmed at the end of the follow-up period, we would provide evidence of the long-term effectiveness of exercise and the potential of the APA program to reduce health care costs.
Our results are consistent with those of Stuart et al, 21 despite differences in the timing, amount, and duration of the APA program. We augmented APA with TPE. The current study offered APA classes 2 times a week for just 8 weeks, whereas in the previous study, APA classes were offered 3 times a week for 6 months. The earlier study recruited patients with a mean time from a stroke >3.5 years; we recruited patients 3 to 18 months from the stroke event, following rehabilitation, and also included those with aphasia or moderate cognitive impairment. Thus, we included participants having less “stable” clinical conditions, and the sample is more homogeneous regarding both duration following a stroke (3-18 months) and timing with regard to rehabilitation. Notably, time since stroke onset proved to be unrelated to our primary outcome, suggesting that patients may be safely enrolled in the APA-TPE intervention any time from 3 to 18 months from a stroke and benefit from it because the margin of improvement is not limited to the early period after the event.
The low attrition rate (13.1%) and high compliance with the APA sessions in this study are particularly noteworthy. Only 12 of 101 patients chose to discontinue the APA program, and another 12 were terminated for medical reasons. Of those who completed the program, 86% attended almost every session. This suggests that APA is safe and feasible for about 4 in 5 survivors of strokes with moderate hemiparesis, starting as early as 3 months after a stroke.
Strengths of this study include the large sample size and blinded assessors. While most previous trials on this topic enrolled <100 patients,5,19-21 we recruited >200 participants. Outcomes were measured by raters not involved in therapy or exercise sessions to reduce the possible bias related to therapists’ expectations on improvement.
The present study has a possible selection bias related to the nonrandomized study design. This bias has been partially mitigated by the inclusion of consecutive patients with strokes referred to the physical medicine and rehabilitation units of 2 hospitals in local health authorities of the same Italian region and with a similar care pathway, from stroke unit care to rehabilitation unit and community rehabilitation. In addition, a comparison between completers and dropouts did not show any differences for demographic and clinical variables, except that the Motricity Index of the upper limb of the nonparetic side and SF-12 mental composite scale score were significantly higher in completers than in dropouts. Our analytical strategy based on the propensity score allowed an adjustment of the outcome comparisons for group differences at baseline. The use of this strategy, advocated by Rosenbaum and Rubin 43 in 1984 to reduce bias in observational studies, has found many recent applications in outcome research. Its advantage is the ability to adjust the treatment effect for multiple known confounders, although it cannot control for residual confounding related to unknown variables.
Our results do not allow us to disentangle the specific effect of TPE sessions on outcomes, in particular on quality of life. However, the high compliance rate with the interactive TPE sessions and the completion of the home exercise diary suggest that the TPE intervention increased patients’ involvement and met their needs for information and support after discharge from hospital rehabilitation. Moreover, TPE appears to be a promising component of a comprehensive stroke care program, filling the service gap that arises at the end of rehabilitation, when the patient experiences a sense of abandonment from professionals. It seems likely that the addition of TPE increased the effectiveness of APA interventions because the exercise program lasted only 2 months and the follow-up evaluation was carried out at 4 months. Frequently, people reduce exercise and decondition rapidly at the end of an intervention, but in the present study, the intervention group maintained better performance presumably because of continuing an active lifestyle. Our findings are consistent with those of previous studies that suggest that patient education may influence health beliefs, 44 and the perceived benefit of exercise to reduce risk has been found to be strongly and positively associated with the intention to exercise. 45
Currently, in Italy, the Tuscany region serves as the reference model for the APA intervention, but other Italian regions are following its example. At the community level, the main objective is to develop a network of local gymnasiums that can offer the APA intervention at a low cost. In Emilia-Romagna, for example, APA programs have been included in the regional guidelines, and a gymnasium network for patients with strokes is already functioning in some areas of the region. Also, APA community exercise programs are ongoing in other Italian regions. The results of this study suggest that adding a TPE program during the phase of rehabilitation may strengthen the role of patient self-management and improve the transition from rehabilitation.
Conclusion
This study confirms the effectiveness of APA to improve function and quality of life for survivors of strokes by providing evidence from a large trial conducted in a different region of Italy. Furthermore, it appears to be safe and efficacious to have patients exercise as early as 3 months after a stroke, including those with moderate cognitive impairments and aphasia. Our results suggest that, in routine clinical practice, it is feasible and potentially effective to implement APA programs immediately following rehabilitation for elderly patients with complex clinical conditions with the aim of counteracting the decline of motor function and the worsening of quality of life. This short and early intervention appears to be valuable in filling the service gap once rehabilitation is complete. Findings highlight the potential for TPE, in concert with APA group exercise classes, to provide a foundation for sustained home exercise following rehabilitation and to encourage ongoing participation in community APA classes wherever these are available.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: The research project was funded by the Regional Agency for Health and Social Care, Regione Emilia-Romagna, Grant “Progetto di Modernizzazione MOD-2008-0022”.
Note*
EFG/2009 investigators: Mariangela Taricco, MD, Elena Bassi, PT, Chiara Bernucci, MD, Noemi Gaudenzi, PT, Besa Kopliku, MD, Vincenzo Manigrasso, PT, Matteo Morara, PT (University Hospital Policlinico Sant’Orsola Malpighi, Bologna, Italy); Laura Dallolio, PhD, Simona Calugi, PsyD, Maria Pia Fantini, MD, Paolo Pillastrini, PT, Paola Rucci, PhD (Department of Biomedical and Neuromotor Sciences, Alma Mater Studiorum–University of Bologna, Bologna, Italy); and Stefania Fugazzaro, MD, Mattia Gandini, PT, Barbara Piccinelli, MD, Francesco Sassi Zanichelli, PT, Claudio Tedeschi, MD, Stefania Testoni, MD (IRCCS Arcispedale Santa Maria Nuova, Reggio Emilia, Italy).