
Abstract
Background
Matrix-induced autologous chondrocyte implantation (MACI) relies on secure collagen membrane fixation for successful cartilage repair. However, comparative biomechanical data on fixation techniques remain limited.
Objective
To evaluate and compare the fixation strength of various collagen membrane fixation techniques used in autologous chondrocyte implantation (ACI) using an in vitro porcine model.
Design
Fifty porcine knees were used to test 17 different fixation methods for securing collagen membranes (Chondro-Gide®). Fixation techniques included various combinations of absorbable and non-absorbable anchors, different suture materials, knotted and knotless techniques, and absorbable pins. Membrane thickness was measured using digital micrometry. Tensile testing was performed using a digital force gauge until failure. Peak fixation strength and failure modes were recorded. Results. Mean collagen membrane thickness was 0.492 ± 0.151 mm with moderate correlation to tensile strength (r = 0.554, P < 0.001). Among tested methods, the 2.0-mm absorbable pin demonstrated significantly superior fixation strength compared to all other techniques (16.67 ± 4.17 N vs. 5.54-10.01 N, P < 0.01). No significant differences were observed among various anchor-suture combinations. Failure occurred predominantly through membrane tearing at anchor insertion sites (47.1%) and suture fixation points (35.9%), rather than anchor pull-out or suture breakage.
Conclusions
Most conventional fixation methods showed comparable mechanical performance, limited by the inherent properties of the collagen membrane. The 2.0-mm absorbable pin achieved superior fixation through a compression-embedding mechanism rather than simple surface fixation. These findings suggest that fixation strategies incorporating membrane compression into the subchondral bone may provide enhanced mechanical stability for ACI procedures.
Keywords
Introduction
Autologous chondrocyte implantation (ACI) has evolved as an established treatment for focal cartilage defects since its introduction by Brittberg et al. 1 The technique has undergone significant refinements, particularly in the method of securing the cell-seeded construct to the defect site. While first-generation ACI utilized periosteal flaps, the invasiveness of periosteal harvest and associated complications led to the adoption of collagen membranes as the standard coverage material.2,3
Matrix-induced autologous chondrocyte implantation (MACI) represents the current standard, employing type I/III collagen membranes as scaffolds for chondrocyte seeding. 4 The mechanical stability of these constructs during the critical early postoperative period directly influences clinical outcomes, with inadequate fixation potentially leading to graft delamination, cell loss, and treatment failure.5,6
Traditional fixation relies on suturing the membrane directly to surrounding cartilage. However, this approach faces inherent limitations: fixation strength depends on cartilage quality, which may be compromised in degenerative conditions, and suture cutout through damaged cartilage remains a significant concern.7,8 To address these limitations, various anchor systems have been developed to achieve fixation through the subchondral bone, theoretically providing more robust mechanical stability.9,10
Despite widespread clinical use of these various fixation methods, comparative biomechanical data regarding their relative performance remains limited. Previous studies have evaluated individual techniques but have lacked comprehensive comparison under standardized conditions.11 -14 Furthermore, the optimal balance between fixation strength, technical complexity, and biological compatibility remains undefined.15,16
Previous biomechanical studies have successfully utilized porcine models to evaluate cartilage repair techniques, with results showing strong correlation to clinical outcomes. The porcine knee provides a validated platform for comparative biomechanical testing due to its anatomical similarity and commercial availability.
This study aimed to systematically evaluate and compare the mechanical performance of currently available collagen membrane fixation techniques using a standardized in vitro model, with particular focus on identifying factors that influence fixation strength and failure modes.
Materials and Methods
Study Design and Sample Size Determination
This comparative biomechanical study evaluated 17 different collagen membrane fixation techniques using an in vitro porcine model. Based on previous biomechanical studies of collagen membranes and cartilage repair techniques,8,13 we anticipated a coefficient of variation of approximately 30% in fixation strength. To detect a clinically meaningful difference of 40% between fixation methods with 80% power at α = 0.05, we calculated a minimum sample size of n = 9 per group using G*Power 3.1 software. We used n = 10 per group to account for potential technical failures and to ensure robust statistical analysis. To address potential within-knee correlation bias, we implemented a randomized allocation strategy where test sites from the same knee were distributed across different fixation groups rather than clustered within a single group. This approach minimizes the impact of knee-specific factors on group comparisons. However, we acknowledge that this does not fully eliminate the correlation structure, and our reported P-values should be interpreted conservatively.
To minimize potential influence of individual membrane properties on fixation strength results, each of the 10 trials within a specific fixation method utilized a different collagen membrane from our characterized pool of 30 membranes. This randomized assignment prevented any single membrane from disproportionately affecting the results of a particular fixation technique.
Specimen Preparation
The porcine knee was selected as the experimental model based on established anatomical and biomechanical similarities to human joints. Porcine cartilage thickness (2.0-2.5 mm) closely approximates human femoral condyle cartilage (2.2-2.5 mm), and the biomechanical properties including compressive modulus (0.5-0.8 MPa) and tensile strength are comparable to human tissue. Previous validation studies have demonstrated that porcine models provide reliable predictions of fixation behavior in human applications. 17
However, it should be noted that porcine cartilage from young animals (6-8 months) used in this study may differ from typical ACI patient cartilage in several aspects: (1) higher proteoglycan content and water content compared to aged human cartilage, (2) intact tidemark and calcified cartilage layer versus potentially disrupted architecture in degenerative conditions, and (3) absence of inflammatory mediators present in osteoarthritic joints that could affect membrane integration.
Fifty fresh-frozen adult porcine knees were obtained from a commercial supplier and stored at −18 °C until testing. Specimens were thawed at room temperature for 12 hours before experimentation. Both medial and lateral femoral condyles were exposed through a standard medial parapatellar approach, and multiple areas of intact cartilage were identified for testing. Each knee provided 3-4 test sites (medial femoral condyle, lateral femoral condyle, and trochlea), yielding a total of 170 test sites for the study.
Membrane Preparation
Thirty collagen membranes (Chondro-Gide®, Geistlich Pharma AG, Wolhusen, Switzerland) measuring 50 × 40 mm were each divided into 20 × 10 mm test samples. One sample from each membrane was designated for material property evaluation. Membrane thickness was measured at 4 standardized points 5 mm from the edge using a high-precision digital micrometer (Litematic VL-50, Mitutoyo Corporation, Kawasaki, Japan) with 0.001 mm resolution. The average of 4 measurements was calculated for each sample. These 30 samples served as controls for baseline tensile strength assessment.
Fixation Methods
The selection of fixation methods and materials was based on current clinical availability and usage patterns. Statistical analysis and data interpretation were performed independently.
(
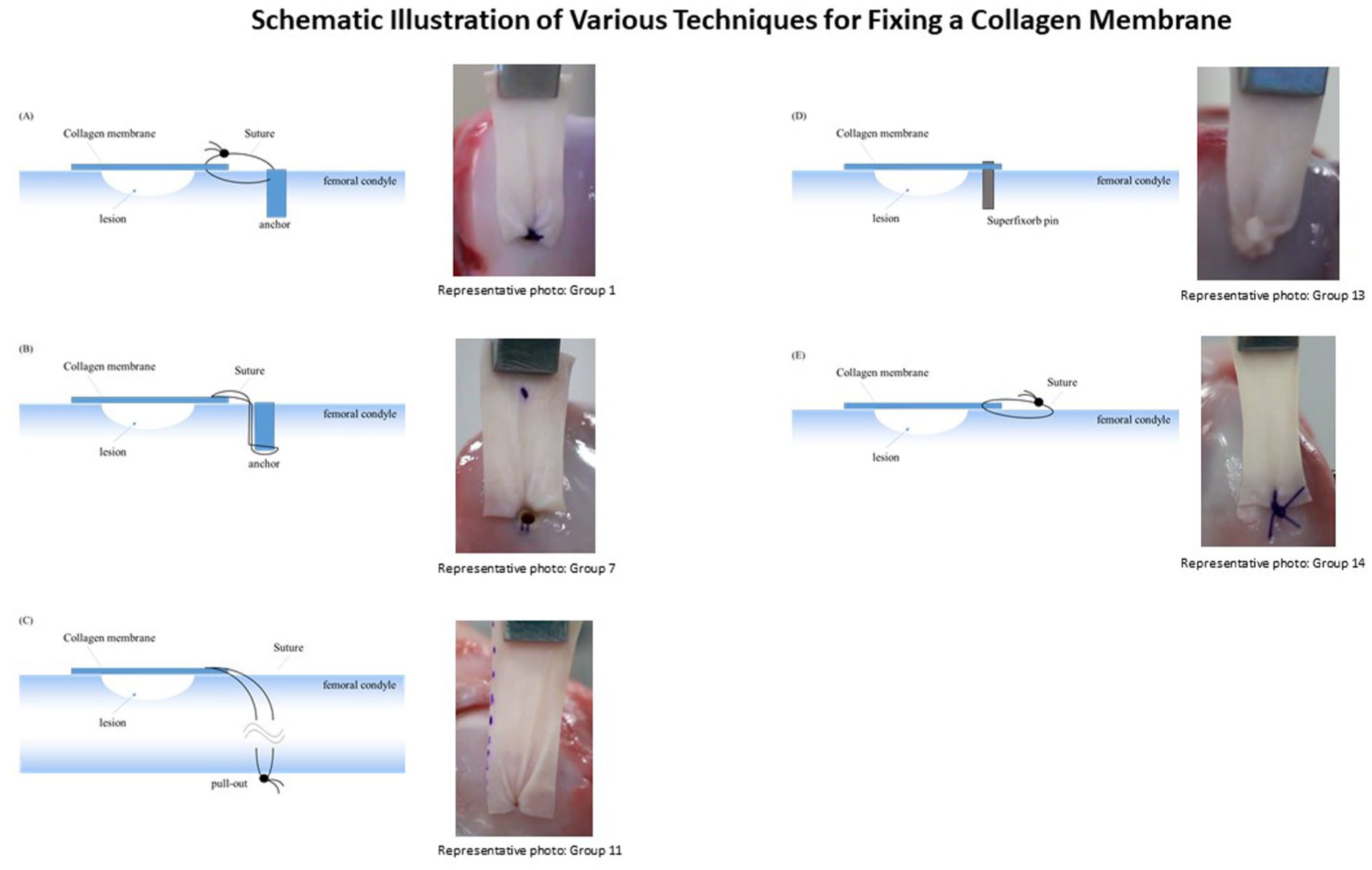
Schematic illustrations of collagen membrane fixation techniques with corresponding group numbers from
Seventeen fixation techniques were evaluated, representing clinically relevant combinations of anchors, sutures, and fixation strategies:
Anchor Systems
GRYPHON BR Anchor (DePuy Synthes, Raynham, MA)—absorbable
JuggerKnot Soft Anchor (Mini 1.0 mm and System 1.4 mm, Zimmer Biomet, Warsaw, IN)—non-absorbable
Suture Materials
Ethibond 4-0 (polyester, non-absorbable; Ethicon, Somerville, NJ)
Nylon 5-0 (non-absorbable; Matsuda Ika Kogyo, Tokyo, Japan)
PDS II (polydioxanone suture) 3-0 and 4-0 (absorbable; Ethicon)
Pin Systems
Super-Fixorb Thread Pins 1.5 mm and 2.0 mm (poly-L-lactic acid; Teijin Medical Technologies, Osaka, Japan)
Fixation Techniques
Conventional knotted suture
Knotless press-fit (GRYPHON anchor only)
Direct cartilage suture (without anchors)
Pin fixation (without sutures)
Biomechanical Testing
All mechanical testing was performed at room temperature (23 ± 1 °C).
Membranes were hydrated in physiological saline at 37 °C for 60 seconds before fixation. This standardized hydration time was selected based on typical intraoperative handling duration and manufacturer’s guidelines for clinical use, ensuring consistent membrane properties across all experimental conditions.
Previous studies have shown that collagen membranes reach equilibrium hydration within 30-90 seconds without significant changes in mechanical properties, 8 supporting our selected duration.
Each membrane was secured to intact cartilage using one of the test methods. The free edge was clamped 5 mm from the margin using an 8-mm jaw-width chuck.
Tensile testing was performed using a digital force gauge (ZTA-50N, IMADA, Toyohashi, Japan) mounted on a motorized test stand (MX2-500N-FA, IMADA). Horizontal tensile force was applied at a constant rate of 10 mm/min until failure, following standard protocols for biomechanical testing of soft-tissue constructs. This quasi-static loading rate was selected based on established methodologies in cartilage repair biomechanics 8 and allows controlled evaluation of maximum fixation strength while minimizing viscoelastic and strain-rate dependent effects that could confound results. Force-displacement data were recorded at 1,000 Hz using Force Recorder Light software (IMADA).
Peak load at failure and failure mode were documented for each specimen. Failure modes were categorized as: (1) membrane tear at anchor insertion site, (2) membrane tear at suture site, (3) membrane tear at pin insertion site, (4) membrane tear in central region, or (5) cartilage failure.
Statistical Analysis
Data normality was assessed using the Shapiro-Wilk test. Correlation between membrane thickness and tensile strength was evaluated using Pearson correlation coefficient.
We assessed homogeneity of variances using Levene’s test. In our data, Levene’s test centered at the mean was not significant (W = 1.01, P = 0.450), and the Brown–Forsythe test centered at the median was also not significant (W = 0.81, P = 0.669). Given possible heteroscedasticity across techniques and unequal standard deviations, we nevertheless used Welch’s one-way ANOVA to compare fixation strength across the 17 methods, F(16, 515.83) = 5.25, P = 2.64e-10, followed by the Games–Howell test for multiple comparisons.
Failure mode distribution was analyzed using chi-square test. Post-hoc power analysis was performed to confirm adequate statistical power for the primary comparisons. Statistical significance was set at P < 0.05. All analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY).
Sensitivity analyses were conducted to assess the impact of within-knee clustering. When analyzing only one randomly selected site per knee (reducing sample size to n = 3-4 per group), the 2.0-mm pin remained significantly superior (P < 0.05), though power was reduced for detecting differences among conventional methods. The intraclass correlation coefficient (ICC) for sites within the same knee was 0.12 (95% CI: 0.05-0.19), indicating modest but non-negligible clustering. Future studies should consider using generalized estimating equations (GEE) or linear mixed models with knee as a random effect to more appropriately account for this correlation structure.
Post-hoc sensitivity analysis was performed to evaluate the potential impact of within-knee clustering. Given that each knee provided 3-4 test sites, we conducted a conservative analysis treating each knee as a cluster. While mixed-effects modeling would be ideal, our randomized assignment of membranes across fixation methods helps mitigate systematic bias from within-knee correlation. Nevertheless, P-values should be interpreted with appropriate caution given this limitation.
Results
Membrane Properties
Mean membrane thickness across all samples was 0.492 ± 0.151 mm (range: 0.281-0.814 mm). Control membrane tensile strength averaged 21.6 ± 10.0 N. Correlation analysis revealed a moderate positive relationship between thickness and tensile strength (r = 0.554, P < 0.001;
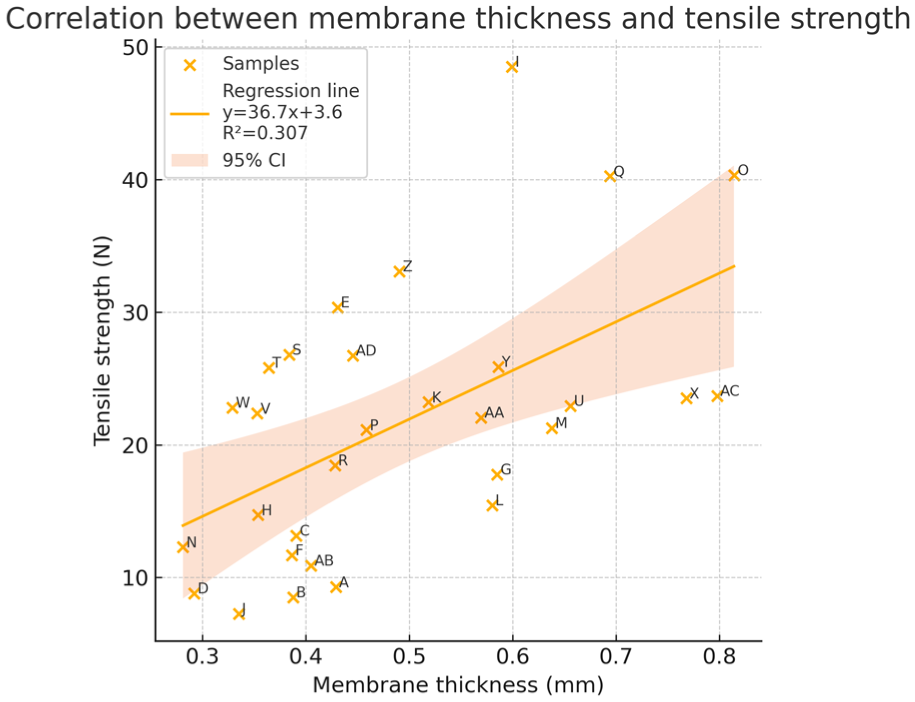
Correlation between collagen membrane thickness and tensile strength. Scatter plot demonstrating a significant positive correlation (Pearson r = 0.554, P < 0.001) between membrane thickness and tensile strength for 30 Chondro-Gide® collagen membrane samples (Geistlich Pharma AG). Each data point represents individual membrane samples with thickness measured as the average of four standardized measurements at points 5 mm from the edge using high-precision digital micrometry. The regression line shows R² = 0.307 (regression equation: y = 36.7x + 3.6), indicating that membrane thickness explains 30.7% of the variance in tensile strength. Despite the moderate correlation, considerable variability exists across all thickness levels, suggesting additional factors such as collagen fiber orientation and cross-linking density contribute to membrane mechanical properties. Data range: thickness 0.281-0.814 mm, tensile strength 7.27-48.51 N.
Individual Collagen Membrane Properties (n = 30).
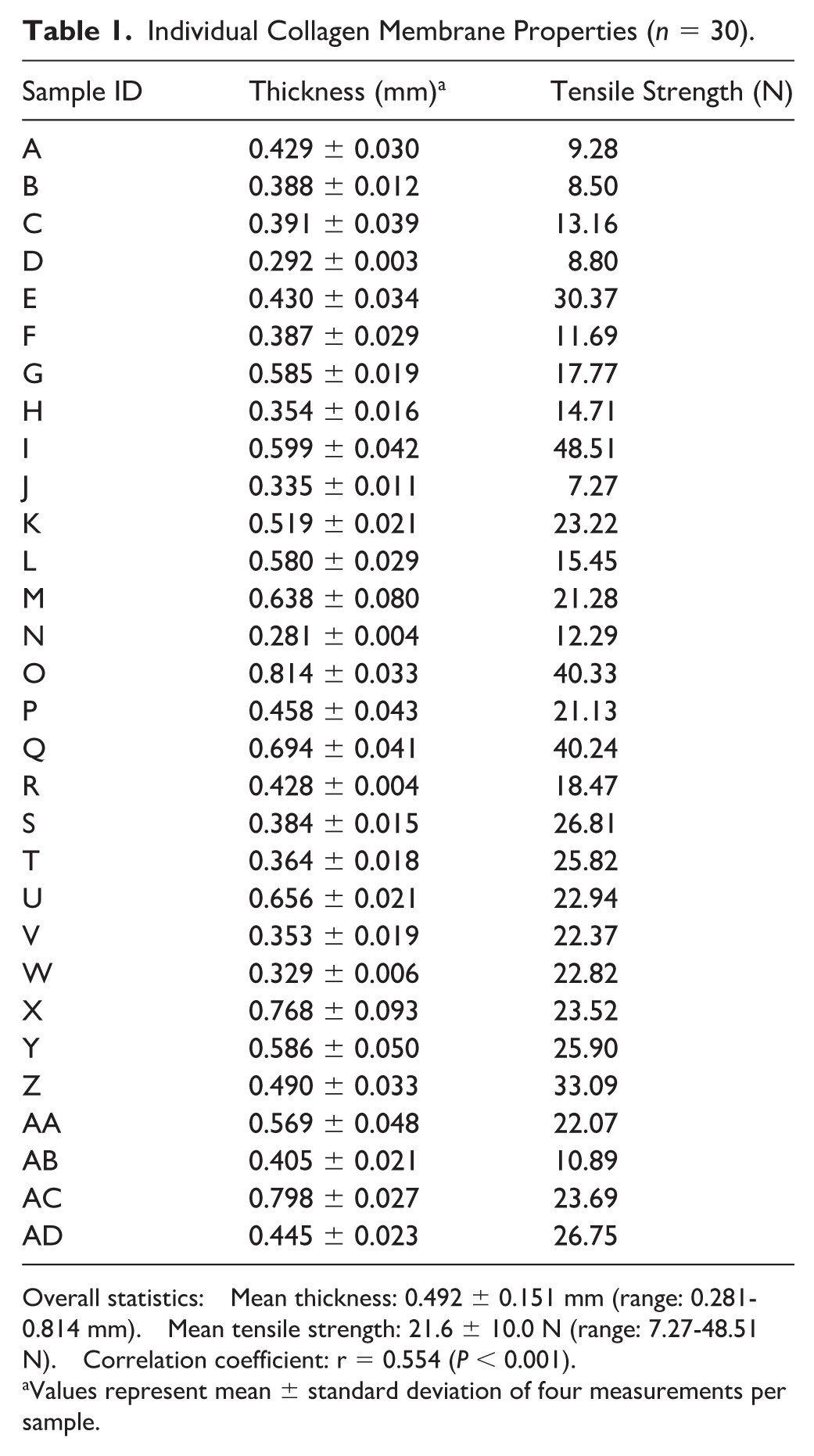
Overall statistics: Mean thickness: 0.492 ± 0.151 mm (range: 0.281-0.814 mm). Mean tensile strength: 21.6 ± 10.0 N (range: 7.27-48.51 N). Correlation coefficient: r = 0.554 (P < 0.001).
Values represent mean ± standard deviation of four measurements per sample.
Fixation Strength by Method
The 2.0-mm absorbable pin demonstrated significantly higher fixation strength (16.67 ± 4.17 N) than all other methods (P < 0.01;
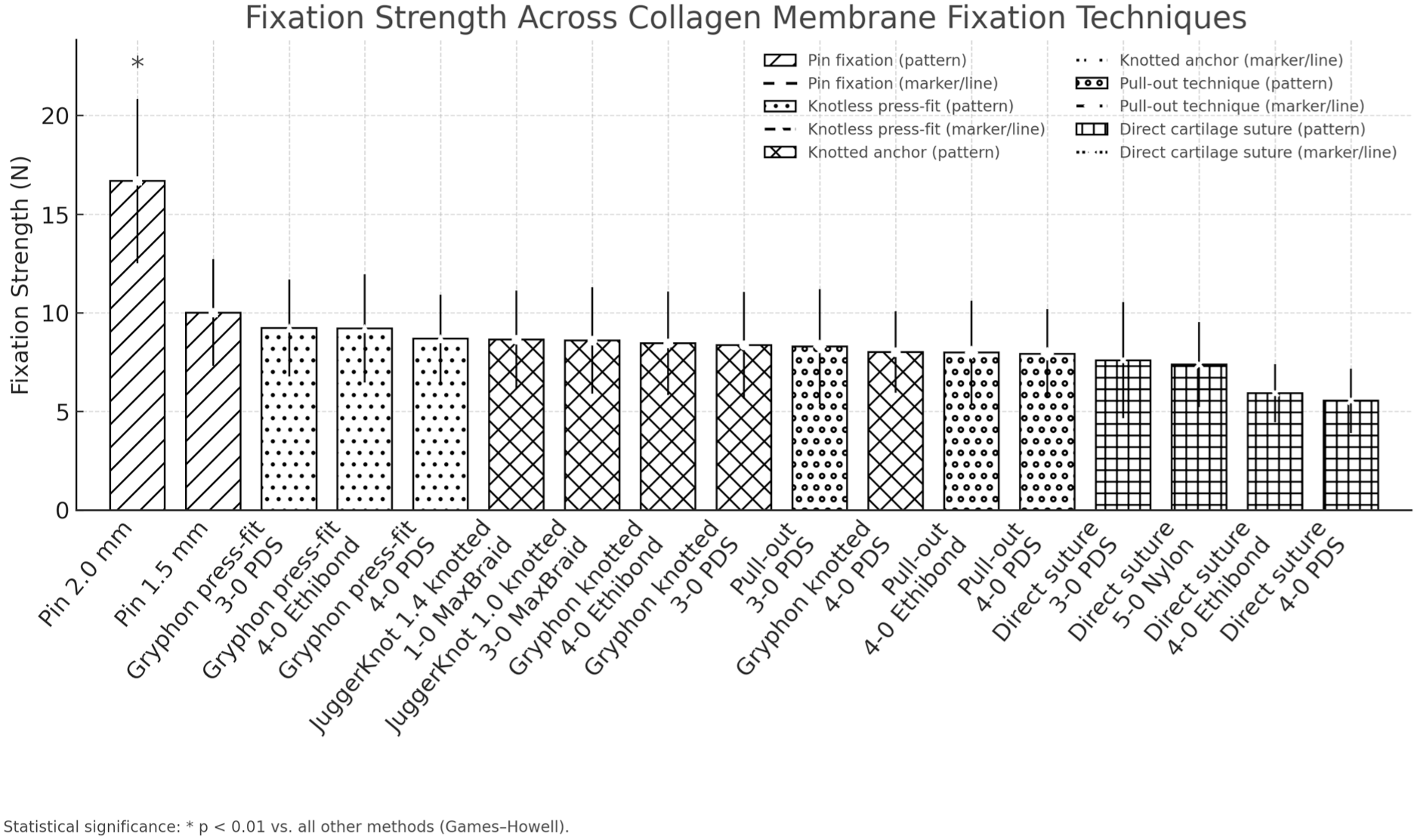
Comparison of fixation strength across different collagen membrane fixation techniques. Bar chart showing mean fixation strength (±SD) for 17 collagen membrane fixation techniques in autologous chondrocyte implantation. The 2.0-mm absorbable pin achieved significantly superior performance (16.67 ± 4.17 N, P < 0.01) compared to all other methods, while conventional fixation methods showed no significant differences (range: 5.54-9.22 N). The 1.5 mm pin demonstrated intermediate strength (10.01 ± 2.70 N). Technique categories (pin fixation, knotless press-fit, anchor-based methods, pull-out techniques, and direct cartilage sutures) are indicated by the x-axis labels. Error bars indicate standard deviation (n = 10 per method). Asterisk (*) indicates P < 0.01 versus all other methods (Games–Howell).
Fixation Strength of Collagen Membrane Using Different Fixation Methods.
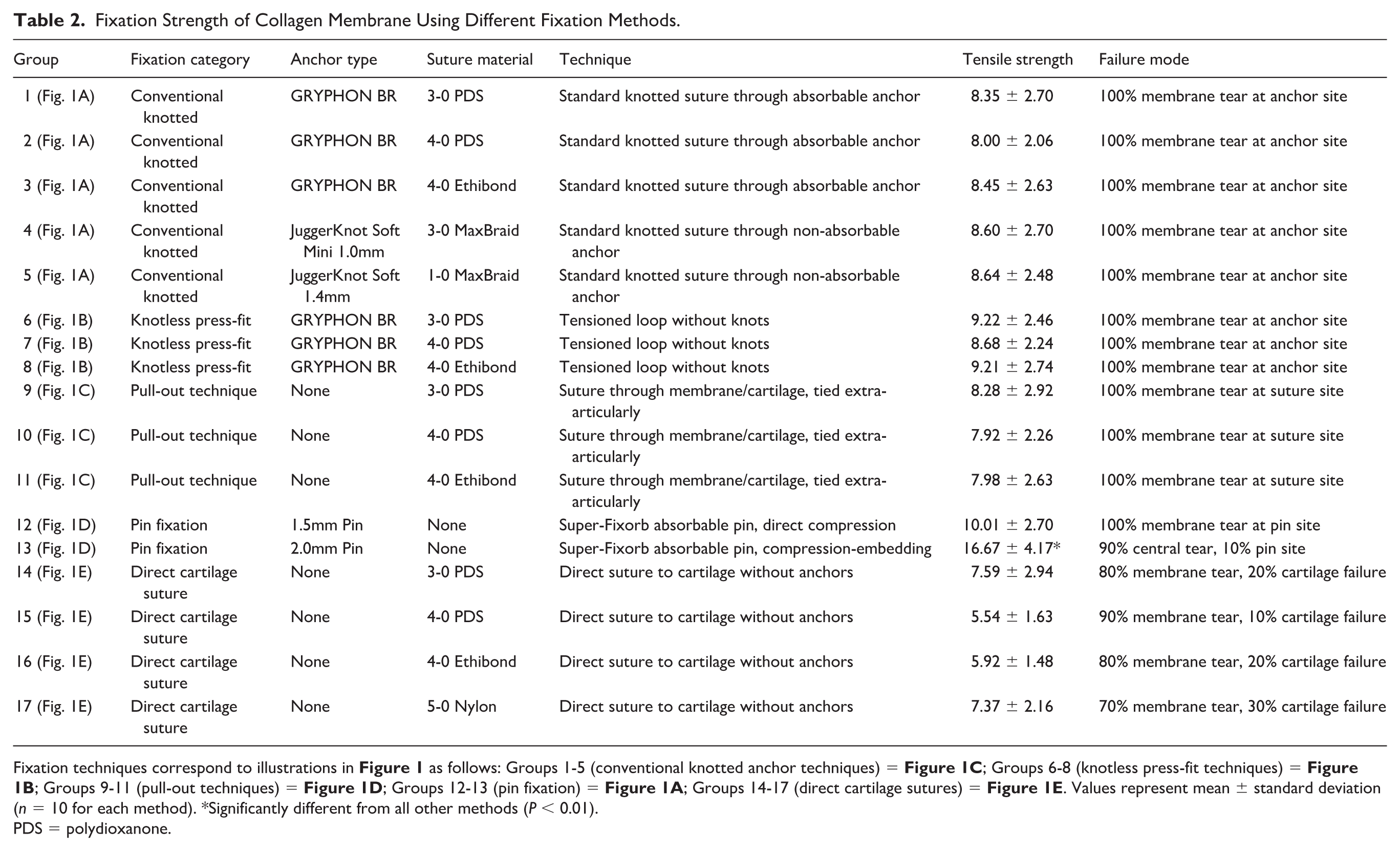
Fixation techniques correspond to illustrations in
PDS = polydioxanone.
The achieved power for detecting the observed difference between the 2.0-mm pin (16.67 ± 4.17 N) and conventional methods (mean 7.5 N) exceeded 95% (effect size Cohen’s d = 2.35), validating our sample size selection.
When comparing the same suture material with and without anchors, minimal differences in strength were found:
PDS 3-0: Direct suture (7.59 ± 2.94 N) vs. with GRYPHON anchor (8.35 ± 2.70 N), P = 0.58
PDS 4-0: Direct suture (5.54 ± 1.63 N) vs. with GRYPHON anchor (8.00 ± 2.06 N), P = 0.09
Ethibond 4-0: Direct suture (5.92 ± 1.48 N) vs. with GRYPHON anchor (8.45 ± 2.63 N), P = 0.11
The GRYPHON anchor system showed no significant difference between knotted and knotless press-fit techniques when using 3-0 PDS suture (8.35 ± 2.70 N vs. 9.22 ± 2.46 N, P = 0.44).
Failure Mode Analysis
Failure mode distribution varied significantly by technique (χ² analysis, P < 0.001):
Technique-Specific Failure Patterns
1.5 mm pin: 100% failure at pin insertion site 2.0 mm pin: 90% failure in membrane central region, 10% at pin insertion site
The 2.0-mm pin system demonstrated a unique failure pattern, with membrane tearing occurring circumferentially around the central embedded portion rather than at discrete fixation points, suggesting a more distributed load transfer mechanism.
Representative examples of these failure patterns are shown in
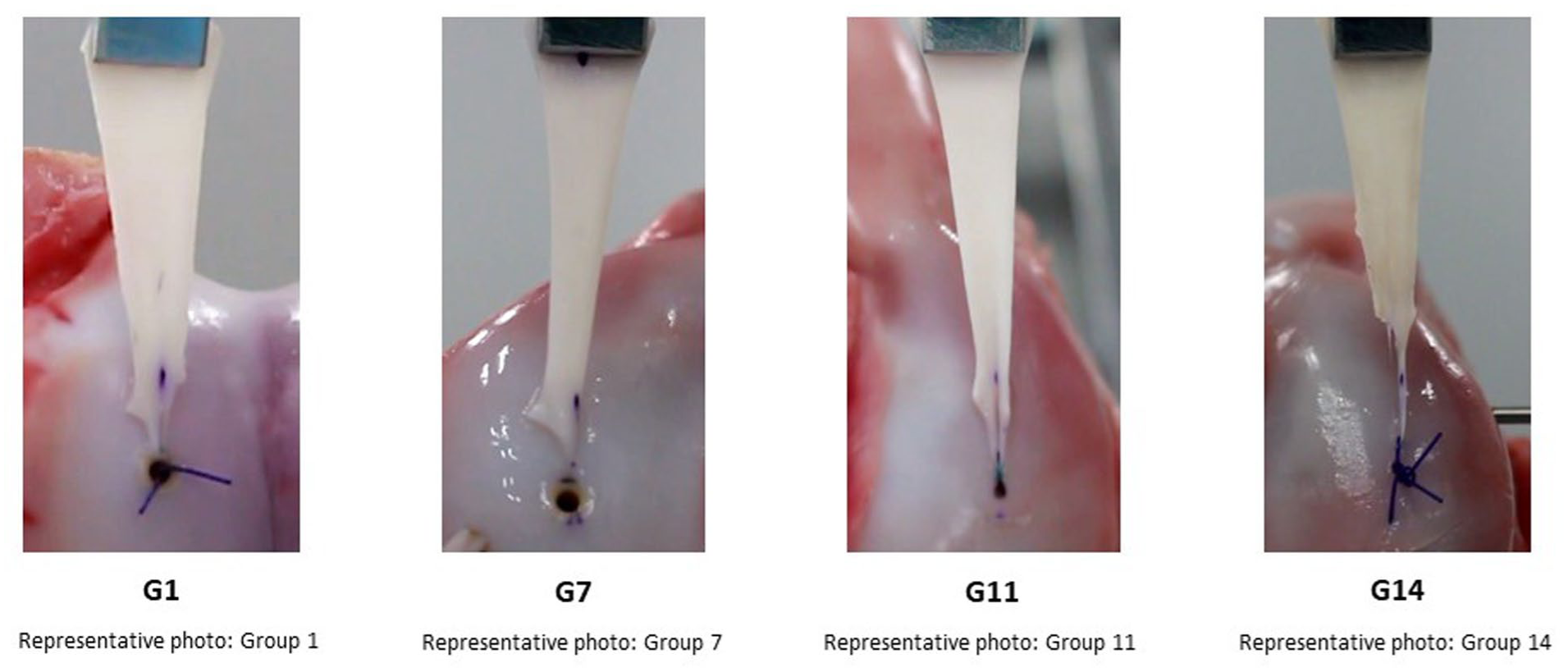
Representative failure patterns of collagen membranes during tensile testing across different fixation techniques.
Discussion
This study provides a systematic biomechanical comparison of currently available collagen membrane fixation techniques for ACI under standardized conditions. Our findings reveal that most conventional fixation methods achieve similar mechanical performance (5.54-9.22 N), with failure predominantly occurring through the membrane rather than the fixation interface. These observations have important implications for optimizing fixation strategies in clinical practice.
The fixation strengths observed in our study (5.54-16.67 N) should be contextualized within expected physiological loads during early rehabilitation. Previous studies have reported that passive range of motion exercises generate shear forces of 2-5 N at the cartilage surface, while partial weight-bearing can produce forces up to 15-20 N depending on defect location and size (Hunziker and Stähli 18 ). Our findings suggest that conventional fixation methods (5.54-9.22 N) may be adequate for initial passive rehabilitation but could be at risk during early weight-bearing phases. The superior strength of the 2.0-mm pin fixation (16.67 N) provides a greater safety margin for accelerated rehabilitation protocols. However, it should be noted that clinical failure often results from repetitive cyclic loading rather than single peak loads, emphasizing the need for fatigue testing in future studies.
The superior performance of the 2.0-mm absorbable pin (16.67 ± 4.17 N) warrants particular attention. Unlike conventional surface fixation methods, this technique achieves stability through a fundamentally different mechanism—compression and embedding of the membrane into a subchondral drill hole. This distributed load transfer appears to overcome the point-loading limitations inherent to suture-based fixation. The larger diameter compared to the 1.5-mm pin (10.01 ± 2.70 N) likely contributes to increased membrane engagement and load distribution, resulting in a 67% increase in fixation strength.
However, the biomechanical superiority of the 2.0-mm pin fixation must be weighed against potential biological considerations. The compression-embedding mechanism that provides enhanced mechanical stability may theoretically compromise chondrocyte viability at the insertion site. Previous studies have demonstrated that excessive mechanical loading can induce chondrocyte apoptosis through mechanotransduction pathways, with compressive strains exceeding 20-30% associated with increased cell death.19,20 The localized compression zone created by the 2.0-mm pin likely exceeds this threshold, potentially creating a zone of cellular compromise. However, given that the pin insertion sites represent a small percentage of the total membrane area (<5%), and that surrounding viable chondrocytes can potentially repopulate these zones through migration and proliferation, the clinical impact may be limited. Future studies incorporating live/dead cell staining and metabolic activity assays following pin insertion would provide valuable insights into this biomechanical-biological trade-off.
Long-term biological integration represents another critical consideration beyond immediate mechanical stability. The embedded portion of the membrane in the 2.0-mm pin technique may experience altered nutrient diffusion dynamics compared to surface-fixed membranes. Synovial fluid, the primary nutrient source for articular cartilage and implanted chondrocytes, reaches the cells through diffusion across the membrane. The compressed and embedded membrane portion may exhibit reduced permeability, potentially limiting nutrient and oxygen supply to chondrocytes in these regions. 18 In addition, waste product removal could be impaired, leading to local accumulation of metabolic byproducts. Conversely, the intimate contact between the membrane and subchondral bone achieved through compression may facilitate earlier vascular invasion and enhanced integration with underlying tissue, as observed in other scaffold-based repair techniques. 21 The balance between these competing factors—reduced synovial nutrition versus enhanced subchondral integration—requires longitudinal in vivo evaluation to determine the net biological effect on tissue regeneration.
Our findings demonstrate that anchor systems provided no mechanical advantage over direct cartilage sutures, challenging the theoretical benefits of subchondral fixation. For example, when using PDS 3-0 suture, the GRYPHON anchor achieved 8.35 ± 2.70 N compared to 7.59 ± 2.94 N for direct suturing—a difference that was not statistically significant.
This unexpected result is explained by our failure mode analysis: in all anchor-based methods (100%), membrane failure occurred at anchor insertion sites rather than at the anchor-bone interface. This indicates that the membrane itself represents the weakest component of the fixation system. Therefore, efforts to increase anchor or suture strength may yield limited benefit without simultaneously addressing membrane integrity at insertion points.
The clinical implications of these findings extend beyond pure mechanical considerations. While the 2.0-mm pin demonstrated superior strength, its use requires membrane oversizing to accommodate the embedded portion—a potential limitation given current single-membrane packaging for ACI procedures. Conversely, while anchor-based methods showed no mechanical advantage, they may offer benefits in challenging anatomic locations where direct cartilage suturing proves technically difficult.
Long-term biological integration represents another critical consideration beyond immediate mechanical stability. The embedded portion of the membrane in the 2.0-mm pin technique may experience altered nutrient diffusion dynamics compared to surface-fixed membranes. Synovial fluid, the primary nutrient source for articular cartilage and implanted chondrocytes, reaches the cells through diffusion across the membrane. The compressed and embedded membrane portion may exhibit reduced permeability, potentially limiting nutrient and oxygen supply to chondrocytes in these regions. 18 In addition, waste product removal could be impaired, leading to local accumulation of metabolic byproducts. Conversely, the intimate contact between the membrane and subchondral bone achieved through compression may facilitate earlier vascular invasion and enhanced integration with underlying tissue, as observed in other scaffold-based repair techniques. 21 The balance between these competing factors—reduced synovial nutrition versus enhanced subchondral integration—requires longitudinal in vivo evaluation to determine the net biological effect on tissue regeneration.
Clinical Translation Considerations
The translation of our findings to clinical practice requires consideration of several factors unique to the human operative environment. First, human cartilage defects often present with sclerotic subchondral bone, which may provide different anchor purchase compared to our healthy porcine model. The increased bone density could theoretically improve anchor stability but may also increase the risk of anchor breakage during insertion. Second, the presence of synovial inflammation in osteoarthritic joints creates a proteolytic environment that could accelerate membrane degradation, potentially altering the relative performance of different fixation methods over time. Third, patient-specific factors such as body mass index, activity level, and rehabilitation compliance introduce variability not captured in our standardized model. Clinical studies have reported early failure rates of 5-15% for MACI procedures,5,6 suggesting that mechanical factors alone do not determine clinical success. Our biomechanical data should therefore be interpreted as providing relative comparisons between techniques rather than absolute predictions of clinical performance.
Comparison With Alternative Fixation Methods
Our study focused on mechanical fixation methods currently available in clinical practice; however, biological adhesives represent an important alternative approach not evaluated in this investigation. Fibrin glue has gained considerable attention as a fixation adjunct or alternative for MACI procedures, offering several theoretical advantages including uniform load distribution, elimination of suture-related trauma, and potential biological benefits through growth factor release.22,23 Recent clinical studies have reported successful outcomes using fibrin glue alone for membrane fixation, with fixation strengths ranging from 2-8 N depending on glue concentration and application technique. 24 While these values appear lower than our measured strengths for mechanical fixation (5.54-16.67 N), the distributed nature of adhesive fixation may provide adequate stability for clinical success.
Furthermore, fibrin glue avoids the point-loading limitations we observed with suture-based methods and the potential compression-related cellular damage associated with pin fixation. However, concerns remain regarding the reliability of fibrin glue in the aqueous intra-articular environment, with some studies reporting early delamination rates of 15-20%. 25 In addition, the cost-effectiveness of fibrin glue compared to mechanical fixation methods requires consideration, as biological adhesives can significantly increase procedure costs. Future studies should directly compare mechanical fixation methods with biological adhesives, as well as combination approaches, under standardized conditions, incorporating both immediate biomechanical testing and long-term biological outcome measures including cell viability, proliferation, matrix production, and clinical integration rates.
Combination of Mechanical and Adhesive Fixation
An emerging approach involves combining mechanical fixation with biological adhesives to leverage the advantages of both methods. The mechanical fixation provides immediate structural stability while the adhesive distributes loads across the membrane-cartilage interface and potentially enhances biological integration. Preliminary clinical reports suggest that using fibrin glue as an adjunct to suture fixation can reduce the number of sutures required while maintaining adequate stability, potentially minimizing suture-related cartilage trauma. 26
Based on our findings, a combination approach using fewer anchor points (reducing point-loading stress concentrations) supplemented with fibrin glue for distributed fixation could theoretically provide optimal mechanical stability while minimizing tissue trauma. For example, using 2-3 anchors at strategic locations combined with fibrin glue application could achieve the target fixation strength of 15-20 N needed for early rehabilitation while reducing the risk of membrane tearing at fixation points. However, this hypothesis requires experimental validation through comparative biomechanical testing of combined versus individual fixation methods.
Study Limitations
Several limitations merit consideration in interpreting our findings:
First, our in vitro model, while standardized, cannot replicate the complex multiaxial loading patterns experienced in vivo.26,27 Our testing utilized a constant displacement rate of 10 mm/min, representing quasi-static loading conditions. This does not capture the full spectrum of loading rates experienced in vivo, which range from slow passive motion during rehabilitation to rapid loading during ambulation. Future studies incorporating cyclic loading at various frequencies (0.5-2 Hz) would better simulate physiological conditions during different phases of rehabilitation.
Second, our testing protocol employed only quasi-static uniaxial tensile loading at 10 mm/min. While this approach provides standardized comparison of maximum fixation strength, it does not replicate the complex multiaxial and cyclic loading patterns experienced during joint motion. In vivo, collagen membranes experience compression during weight-bearing, shear forces during joint rotation, and cyclic loading at frequencies ranging from 0.5 Hz during slow walking to 2 Hz during running. The fatigue behavior under repetitive loading may differ substantially from the single-cycle failure strengths we measured. Future studies should incorporate cyclic loading protocols (e.g., 1,000 cycles at 50% ultimate tensile strength) and multiaxial loading conditions to better predict long-term fixation performance during rehabilitation and normal activities.
Third, while the 60-second hydration protocol was not validated through systematic preliminary testing, this standardized approach ensured consistency across all experimental conditions. The selected duration reflects typical intraoperative handling time and was sufficient to achieve uniform surface hydration without visible membrane degradation. All specimens were treated identically, ensuring valid comparative results between fixation methods.
Fourth, although the porcine model is widely accepted for cartilage repair research, several anatomical and biological differences from human tissue should be acknowledged. Porcine cartilage demonstrates higher cellularity (approximately 1.5-fold) and slightly different collagen fiber orientation compared to human tissue. The subchondral bone density in porcine specimens (younger animals) may be lower than that in typical ACI patients (middle-aged adults with early osteoarthritis). However, these differences primarily affect biological responses rather than immediate mechanical fixation, which depends more on structural properties that are similar between species.
Fifth, the use of normal porcine cartilage may not reflect the compromised tissue quality often encountered clinically. 28 In addition, our testing focused on immediate fixation strength without considering biological integration or degradation over time.29,30
Furthermore, our study did not evaluate biological parameters such as chondrocyte viability, metabolic activity, or membrane permeability following fixation. The mechanical superiority of certain techniques, particularly the 2.0-mm pin fixation, may come at the cost of reduced cell viability in compression zones. Future studies should incorporate cell viability assays (e.g., live/dead staining, MTT assays), assessment of glucose and oxygen diffusion rates through compressed versus uncompressed membrane regions, and evaluation of matrix production (GAG and collagen synthesis) over time to provide a comprehensive understanding of the biological implications of different fixation strategies.
Finally, the sample size of n = 10 per group, while consistent with similar biomechanical studies and adequately powered for our primary comparison, may have limited power to detect smaller differences between conventional fixation methods.
In addition, multiple test sites were obtained from the same knee, which may introduce within-knee correlation and partial violation of the independence assumption; future studies should confirm these findings using mixed-effects models or cluster-robust inference.
Our experimental design incorporated an important methodological consideration: each trial within a fixation method utilized a different collagen membrane from our characterized pool of 30 membranes. This approach effectively distributed the inherent variability in membrane properties across all fixation techniques, preventing any systematic bias that might arise from using the same membrane repeatedly. Given the observed variability in membrane thickness (coefficient of variation: 31%) and the moderate correlation with tensile strength (r = 0.554), this randomization strategy was essential for ensuring that our comparisons reflected true differences in fixation methods rather than membrane-specific characteristics.
The moderate positive correlation between membrane thickness (0.492 ± 0.151 mm) and tensile strength (21.6 ± 10.0 N) observed in our study (r = 0.554) suggests that thicker membranes generally provide greater mechanical resistance. However, this relationship explains only about 31% of the variance in tensile strength, indicating that other factors such as collagen fiber orientation and cross-linking density also contribute to membrane mechanical properties.
Future investigations should address several key areas: (1) development of fixation methods that distribute loads more effectively across the membrane, 31 (2) evaluation of fixation performance under cyclic loading conditions more representative of physiological joint motion, (3) assessment of biological compatibility and integration of various fixation materials, and (4) correlation of biomechanical findings with clinical outcomes. 32
Conclusions
This biomechanical evaluation demonstrates that conventional collagen membrane fixation methods for ACI achieve comparable mechanical performance, limited primarily by the membrane material properties rather than fixation interface strength. The 2.0-mm absorbable pin system achieved superior fixation (16.67 ± 4.17 N) through a compression-embedding mechanism that more effectively distributes mechanical loads. These findings suggest that future optimization of ACI fixation should focus on load-distribution strategies rather than simply increasing interface strength. While immediate mechanical stability represents only one aspect of successful ACI, these data provide an evidence base for surgical technique selection and future implant development.
Supplemental Material
sj-docx-1-car-10.1177_19476035251412115 – Supplemental material for Biomechanical Evaluation of Collagen Membrane Fixation Techniques in Autologous Chondrocyte Implantation: A Comparative In Vitro Study
Supplemental material, sj-docx-1-car-10.1177_19476035251412115 for Biomechanical Evaluation of Collagen Membrane Fixation Techniques in Autologous Chondrocyte Implantation: A Comparative In Vitro Study by Hideto Harada in CARTILAGE
Footnotes
Acknowledgements
The authors thank the laboratory staff for their technical assistance with specimen preparation and biomechanical testing. We gratefully acknowledge Japan Tissue Engineering Co., Ltd. (J-TEC) for their technical support and guidance throughout this study.
Ethical Considerations
This study utilized commercially obtained porcine specimens and did not require institutional review board approval. All experiments were conducted in accordance with institutional guidelines for biomechanical testing.
Author Contributions
HH conceived and designed the study, performed all experiments, analyzed the data, and wrote the manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available in the supplementary materials of this article. Additional data are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.