
Abstract
Introduction
Knee chondral defects are a common cause of pain and dysfunction. This study assessed the prevalence of spin and methodological quality of systematic reviews and meta-analyses on knee chondral defects in orthopedic literature.
Methods
Following PRISMA guidelines, a systematic review was conducted in May 2025 using PubMed, Web of Science, and Embase. Reviews addressing knee chondral defects in orthopedics were included. Abstracts were evaluated for 15 spin types, and methodological quality was rated using AMSTAR 2. Data on PRISMA adherence, publication year, and Level of Evidence were extracted. Associations between study characteristics and spin were analyzed using t tests, ANOVA, Fisher’s exact tests, and Spearman’s rank correlations.
Results
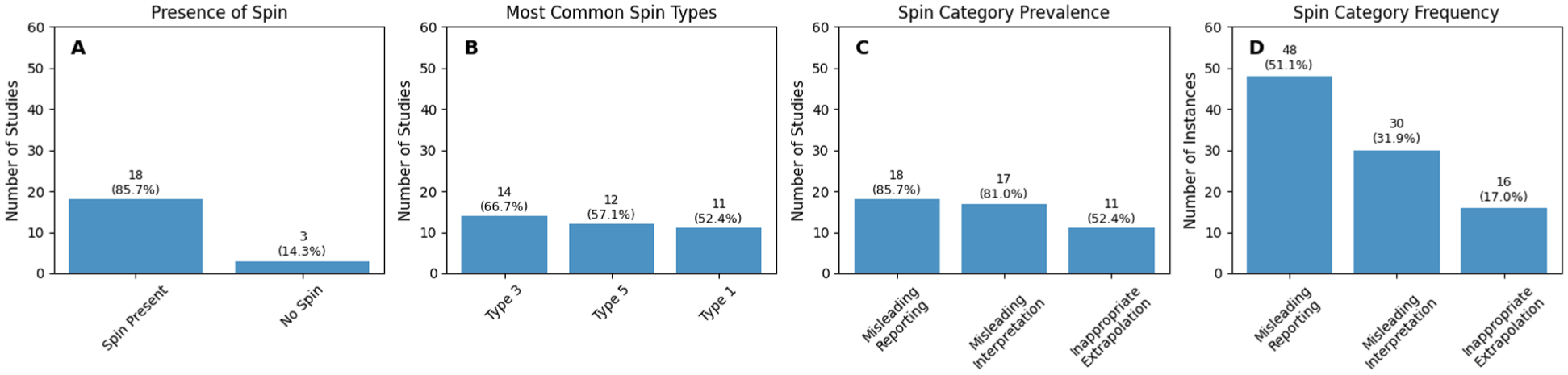
Of 238 studies identified, 21 reviews met criteria. Spin was present in 18 (85.7%). The most common types were type 3 (66.7%), type 5 (57.1%), and type 1 (52.4%). Misleading reporting occurred in 85.7%, misleading interpretation in 81.0%, and extrapolation in 52.4%. AMSTAR 2 rated 95.2% as “critically low” and 4.8% as “moderate.” Journal impact factor correlated with spin presence (P = 0.016) and greater number of spin types (P = 0.012).
Discussion/Conclusion
Most reviews on knee chondral defects contained spin and were of poor quality, underscoring the need for critical appraisal and improved reporting.
Keywords
Introduction
Articular cartilage lesions of the knee are a clinically significant problem. Large registry data suggest that full‑thickness chondral defects are detected in 4.2% to 6.2% of knees undergoing arthroscopy, with focal cartilage lesions reported in up to 36% of athletes. 1 Articular cartilage is avascular with limited regenerative capacity, and untreated lesions often remain symptomatic. 2 Patients with focal cartilage defects frequently report pain, swelling and functional limitations, and the resulting quality‑of‑life impairment is comparable to that of severe knee osteoarthritis.3,4 These lesions are also predictive for total knee arthroplasty (TKA) as their presence is associated with progression to osteoarthritis and a higher likelihood of joint replacement in patients older than 45 years. 3 A wide spectrum of surgical interventions including bone‑marrow stimulation techniques, cell‑based or coral-based repairs and bone‑based resurfacing (osteochondral transplant with either autograft or allograft) have been developed to restore damaged cartilage. 3 Despite these advances, the optimal management strategy, particularly for middle‑aged patients, remains unclear. 3
As the volume of orthopedic research has grown, systematic reviews (SRs) and meta‑analyses (MAs) have become indispensable for synthesizing evidence and informing clinical practice guidelines. Yet the methodological rigor of these reviews varies widely, and numerous process‑related factors contribute to biased or misleading conclusions. Flaws in study selection, data extraction, and statistical synthesis, such as inappropriate pooling despite substantial heterogeneity or incomplete risk‑of‑bias assessments, can distort effect estimates and exaggerate treatment benefits.5,6 These methodological shortcomings often escape detection during peer review due to limited methodological expertise among reviewers, time constraints, and the difficulty of thoroughly evaluating complex statistical analyses and supplementary materials where key details reside. 7
These methodological shortcomings can facilitate “spin,” defined as the use of reporting strategies to emphasize a beneficial effect of an intervention despite statistically non‑significant results. 8 Yavchitz et al. 9 proposed a classification system, including nine types that categorize spin into misleading reporting (e.g., unsupported clinical recommendations, overemphasis of favorable outcomes), misleading interpretation (e.g., claiming benefit despite high risk of bias), and inappropriate extrapolation (e.g., applying results to different interventions). Spin is particularly problematic when it appears in abstracts, as many clinicians read only the abstract and may be swayed by overstated conclusions. 8 Experimental evidence indicates that abstracts containing spin influence physicians’ perceptions of a treatment’s efficacy. 10
Recent meta‑research illustrates the pervasiveness of spin within the field of orthopedics. In systematic reviews on platelet‑rich plasma, 28% of abstracts contained spin, most commonly selective reporting of favorable outcomes and claims of benefit despite high risk of bias. 10 A review study of distal radius fracture SRs/MAs found spin in 46% of abstracts, with unsupported clinical recommendations being the most frequent form. 8 A 2023 assessment of SRs on knee osteoarthritis treatments reported spin in 35% of abstracts. 11 Notably, these studies also highlighted poor methodological quality: over 60% of the included reviews were rated “critically low” on the A Measurement Tool to Assess Systematic Reviews version 2 (AMSTAR 2). 11
AMSTAR 2 is a validated 16‑item instrument for appraising SRs that assigns an overall confidence rating (high, moderate, low or critically low) based on seven critical and nine non‑critical domains.12,13 It emphasizes rigorous literature searches, duplicate study selection and data extraction, and comprehensive risk‑of‑bias assessment. 13 Despite its broad adoption, many orthopedic SRs continue to score poorly, raising concerns that clinical decisions may be influenced by low‑quality evidence containing spin. 11
To date, no study has systematically evaluated spin and methodological quality in SRs/MAs addressing knee chondral defects. Given the high prevalence of these lesions, their impact on patient quality of life, and the multiplicity of available treatments, unbiased and methodologically sound evidence syntheses are essential. This study aims to assess the prevalence of spin and the methodological quality of SRs/MAs on knee chondral defects using the Yavchitz classification and AMSTAR 2. Identifying patterns of reporting bias will inform clinicians and researchers about the reliability of the existing literature and underscore the need for rigorous reporting standards.
Methods
We used the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist when writing our report. 14 The present review was not registered, and no protocol was prepared. Two authors conducted a search of the PubMed, Scopus, and Embase databases using “knee” AND (“chondral defects” OR “knee cartilage” OR “osteochondral defect” OR “focal cartilage defect”) AND (“systematic review” OR “meta-analysis”) in May of 2025. The search strategy was adapted from prior meta-research in orthopedics evaluating spin and methodological quality, using quoted terms to improve specificity for knee chondral defect studies and avoid inclusion of unrelated cartilage or joint conditions.15 -17 Search results were aggregated and deduplicated in Covidence. Two authors independently screened the identified studies for inclusion.
Eligibility
Systematic reviews and meta-analyses related to knee chondral defects published in an English peer-reviewed journal were eligible for inclusion. PubMed, Web of Science, and Embase databases were queried from inception to May 24, 2025 using “knee” AND (“chondral defect” OR “cartilage defect” OR “osteochondral defect” OR “focal cartilage defect” OR “cartilage injury”) AND (“systematic review” OR “meta-analysis”). Studies were excluded if they were not peer-reviewed, not published in English, not systematic reviews and/or meta-analyses, retracted or withdrawn, included nonhuman or cadaver subjects, unrelated to knee chondral defects, published without an abstract, or did not have full text available. The designation “not specific enough” was applied to excluded reviews that discussed general cartilage repair, osteoarthritis, or multi-joint pathology without specifically evaluating knee chondral defects as a distinct focus.
Training
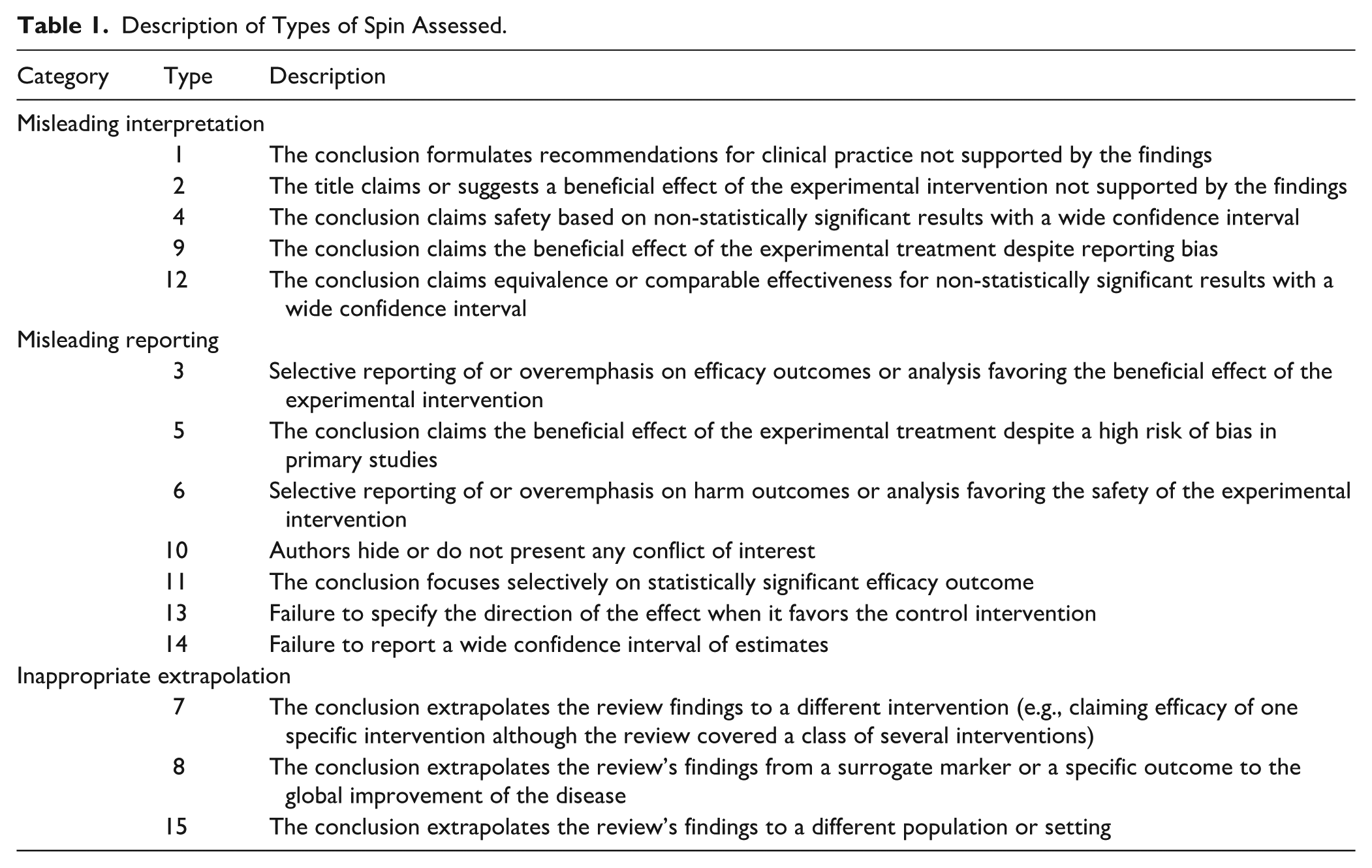
Three authors were trained using previously graded examples to identify study designs and characteristics, and in the definition and classification of the most common types of spin proposed by Yavchitz et al. 9 as summarized in Table 1. The authors also learned to assess study quality using A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2). 13 The adoption of AMSTAR 2 for assessing study quality is supported by its impressive inter-rater reliability and high construct validity. 18
Description of Types of Spin Assessed.
Using AMSTAR 2, a 16-question critical appraisal tool, each study was graded on its methodological quality and assigned an overall confidence rating. This tool evaluates an author’s incorporation of a predetermined study protocol, funding source, conflicts of interest, and an authors’ overall ability to adequately characterize the findings of studies included in the review. The full texts of the included studies were used to assess study quality per the AMSTAR 2 checklist, with particular attention to distinguishing between deficiencies in critical and non-critical domains. In doing so, the AMSTAR 2 assessment identifies critical flaws in systematic reviews and meta-analyses by assigning studies critically low, low, moderate, and high confidence ratings.9,13
Data Extraction
Two authors extracted data independently. In the case of disagreement, resolution was achieved after discussion between the two authors or input from a third author. Study characteristics that were extracted included title, authors, publication year, study design, journal, funding source, level of evidence, reported adherence to PRISMA guidelines, preregistration status, and outcome measures. If not stated within the study, the level of evidence was determined using the American Academy of Orthopaedic Surgeons (AAOS) recommendations. Where study information was missing or unclear, it was recorded as “not reported” and no data was inputted.
Each abstract was assessed for the 15 most common types of spin (Table 1). 9 The full texts of the included systematic reviews were used to assess study quality per the AMSTAR 2 checklist. The AMSTAR 2 confidence ratings were then extracted. In addition, the impact factor was recorded for the journals in which the included systematic reviews and meta-analyses were published. This metric, which gauges the significance of a journal by totaling the number of citations its selected articles receive over a recent period (typically the past few years), serves as a valuable tool for comparing journals within a specific subject category.
Data Analysis
Descriptive statistics were used to characterize the frequency of spin occurring in the included studies. Study characteristics including study type, Level of Evidence, funding source, PRISMA adherence, PROSPERO registration, impact factor, and AMSTAR 2 confidence rating were analyzed. Their association with the presence of spin, as well as the number of spin types present, was determined using t tests, analysis of variance (ANOVA), Fischer Tests, and Spearman’s Rank Coefficients. A P-value < 0.05 was considered statistically significant.
Results
The initial database search identified 395 eligible studies, of which 157 duplicates were removed. An additional 160 studies were removed after the title and abstract screening because they failed to meet the inclusion criteria. The full texts of the remaining 78 articles were assessed for eligibility, of which 57 were excluded based on inclusion criteria. Of the 57 excluded studies, 35 (61.4%) were not specific enough, 5 (8.8%) were focused on other joints other than the knee, 4 (7.0%) were abstracts only, 1 (1.8%) was not in English, 9 (15.8%) were preclinical studies, 2 (3.5%) were the wrong study design, and 1 (1.8%) had an inaccessible manuscript. The 21 remaining systematic reviews, which were published in 13 different journals between 2008 and 2024, were included for analysis (Figure 1).3 -5,19 -36
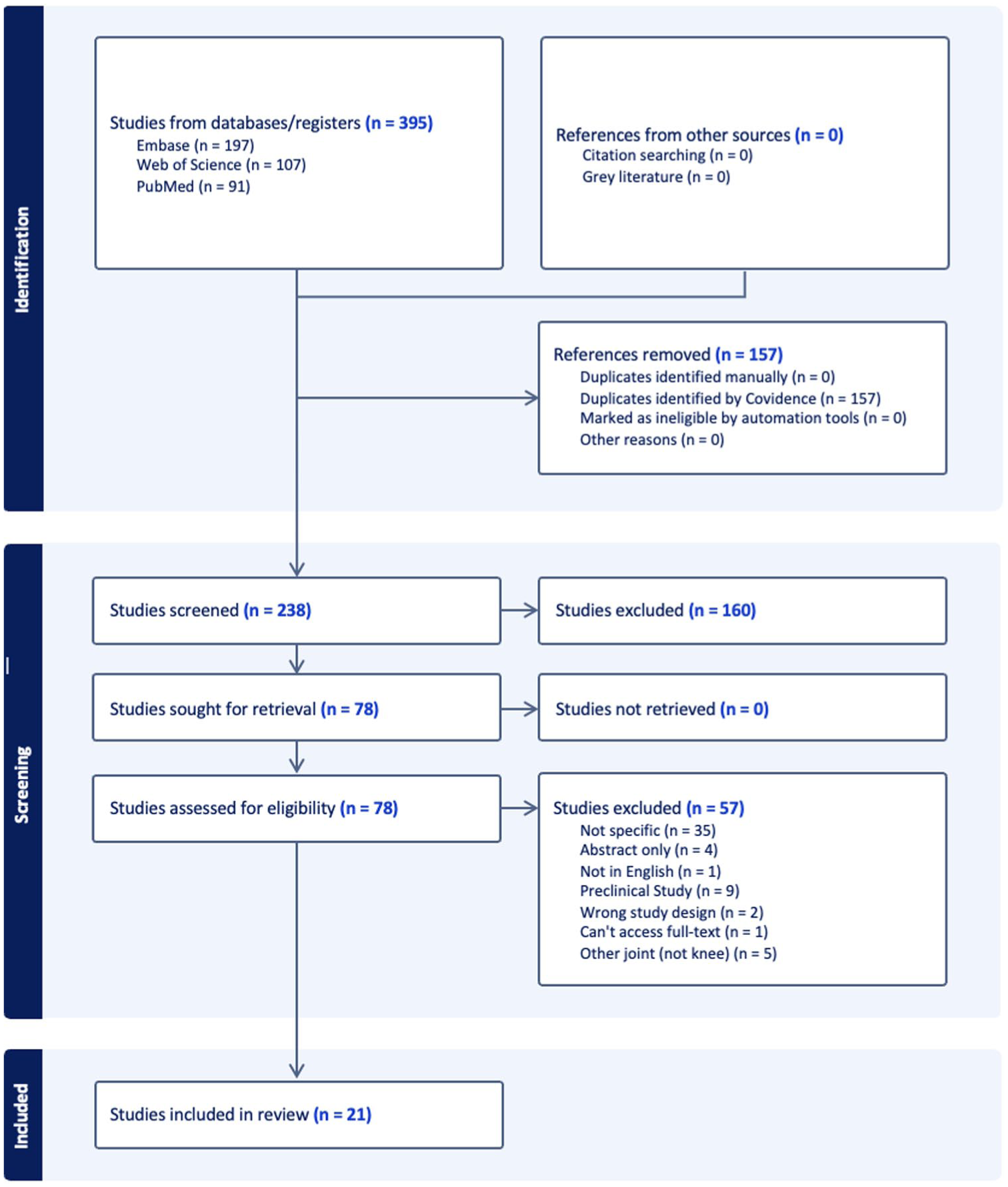
Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram.
Most of the included studies were Level of Evidence IV (13 of 21, 61.9%), 4 (19.0%) were Level of Evidence I, 3 (14.3%) were Level of Evidence II, and 1 (4.8%) were Level of Evidence III (

Distribution of quality indicators among the reviewed studies. (
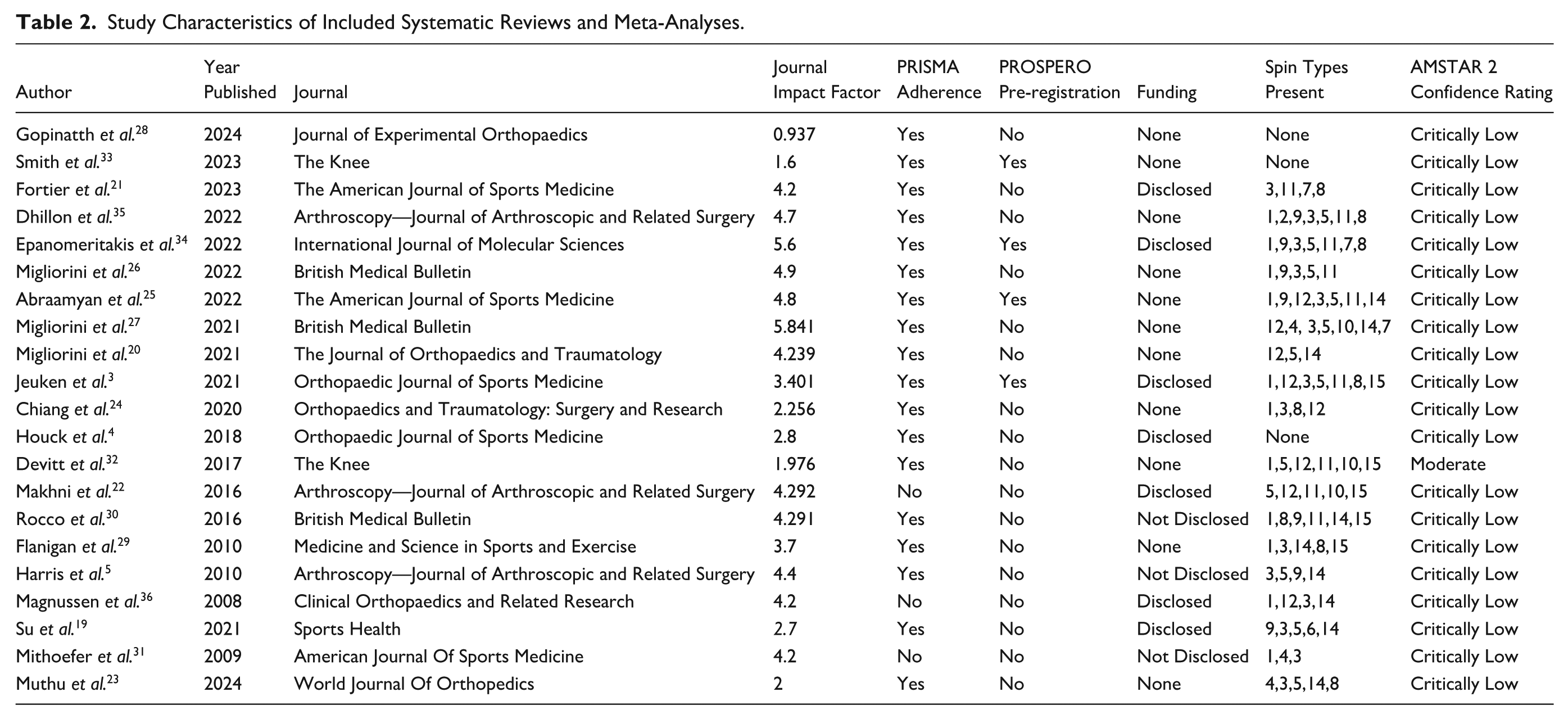
Study Characteristics of Included Systematic Reviews and Meta-Analyses.
Based on their AMSTAR 2 assessments (Table 3), 20 studies (95.2%) received a critically low confidence rating due to the presence of more than one critical flaw. No studies (0.0%) received a low confidence rating, which includes the presence of one critical flaw. One study (4.8%) received a moderate confidence rating, and no studies (0.0%) received a high confidence rating, with both categories requiring the presence of zero critical flaws. Any discrepancy in AMSTAR 2 assessment between the authors was resolved with discussion regarding semantics by multiple reviewers.
AMSTAR 2 Assessment of Reviewed Studies.
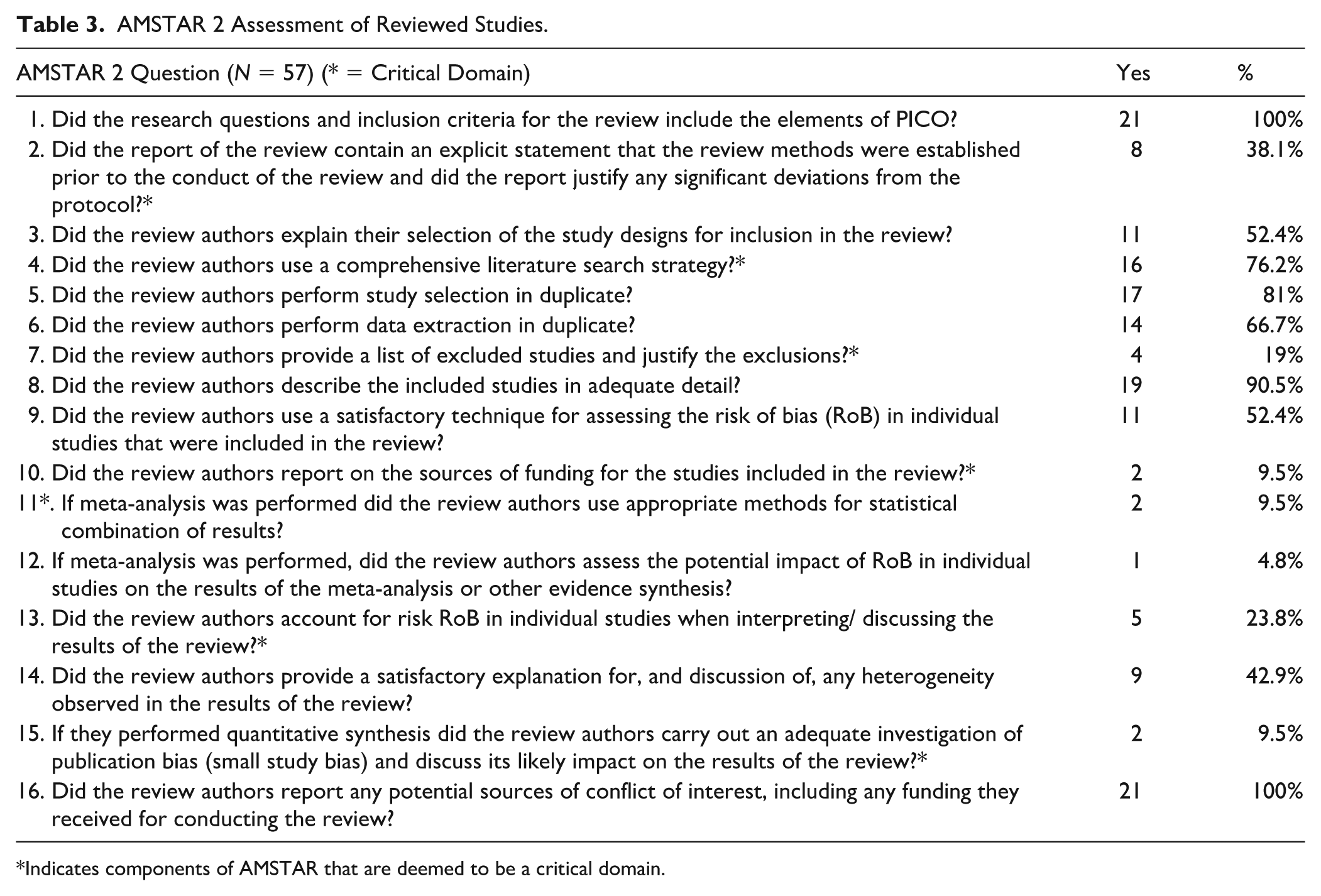
Indicates components of AMSTAR that are deemed to be a critical domain.
Frequency of Spin and Analysis
Spin was present in 18 out of 21 study abstracts (85.7%) and absent in 3 abstracts (14.3%) (
Analysis of spin bias among the reviewed studies. (
Frequency of Spin Type and Category.
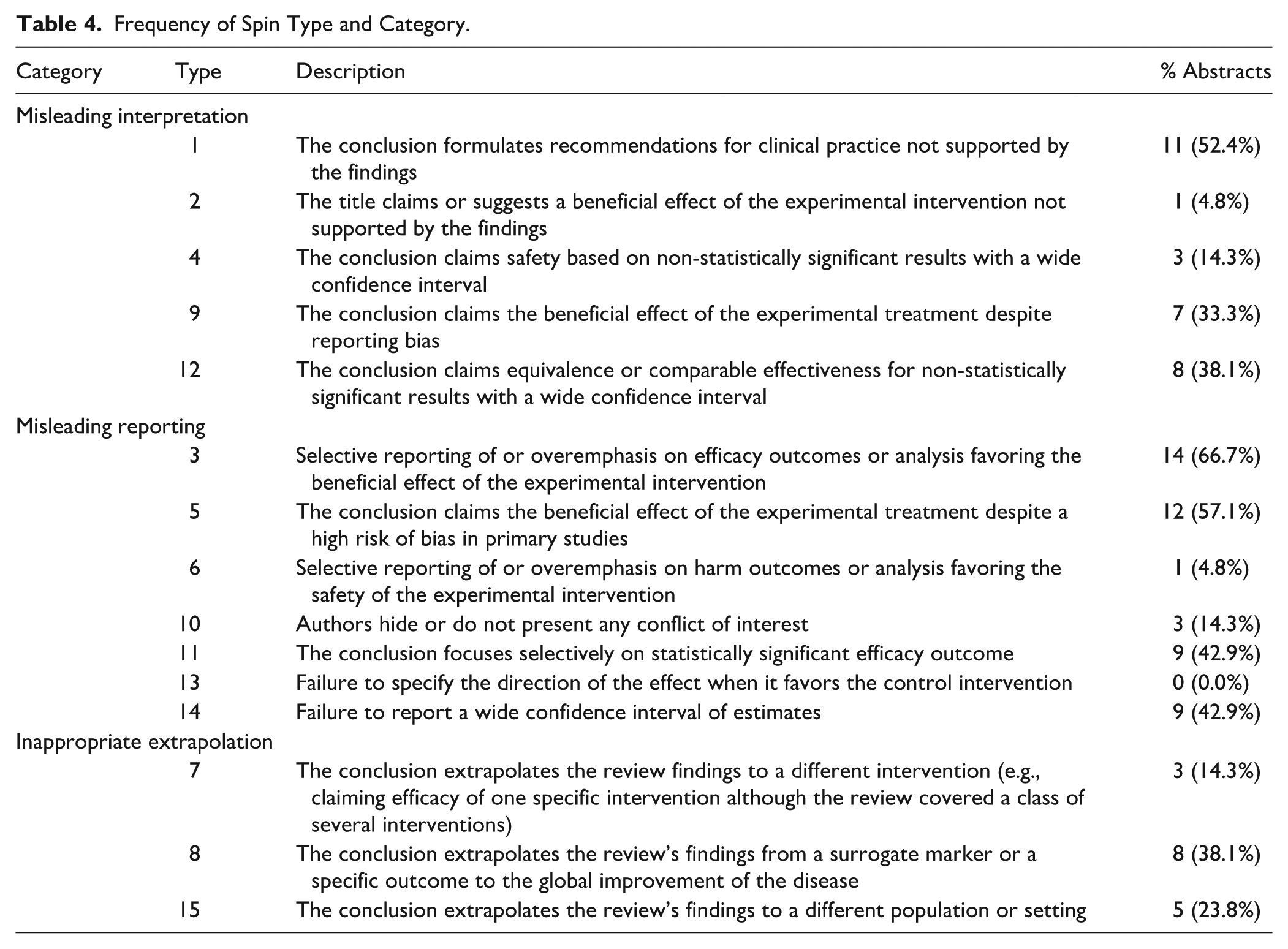
The most prevalent spin category was misleading reporting (types 3, 5, 6, 10, 11, 13, 14), found in 18 of 21 studies (85.7%), with a total of 48 instances
There was a statistically significant association between journal impact factor and the presence of spin in articles, indicating that studies containing spin were statistically more likely to be published in higher-impact journals than those without spin (P = 0.016). The average impact factor for studies with spin was 3.98 ± 1.13, compared to 1.78 ± 0.94 for studies without spin. In addition, the number of distinct spin types was also significantly associated with journal impact factor, suggesting that studies with more types of spin tended to appear in higher-impact journals (P = 0.012).
No statistically significant associations were found between Level of Evidence and the presence of spin or the number of spin types present (P = 0.066 and P = 0.408). Similarly, there was no statistically significant association between year of publication and the presence of spin or the number of spin types present (P = 0.275 and P = 0.792). The AMSTAR 2 tool was used to assess study quality, assigning confidence ratings (critically low, low, moderate, or high) based on the presence of critical methodological flaws. There were no significant associations between AMSTAR 2 confidence ratings and the presence of spin or the number of spin types present (P = 1.000 and P = 0.449).
Discussion
This study demonstrates a high prevalence of spin in the abstracts of systematic reviews and meta-analyses related to knee chondral defects. Of the 21 studies analyzed, 18 (85.7%) contained at least one form of spin. Methodological quality was similarly limited, with 20 studies (95.2%) receiving a critically low confidence rating according to AMSTAR 2 criteria. Only one study (4.8%) was rated as moderate confidence, and none achieved a high confidence rating. These findings underscore significant concerns regarding both reporting practices and methodological rigor in the current literature on knee chondral defect. As clinical decision-making in this area increasingly relies on systematic reviews and meta-analyses, the presence of biased reporting and poor-quality evidence may hinder the development of clear, evidence-based treatment recommendations. These results contribute to growing awareness of the need for greater transparency, consistency, and quality in the reporting of systematic reviews focused on knee preservation and cartilage restoration strategies.
The presence of spin has been well-documented across various areas of orthopedic research, with multiple studies highlighting its frequent occurrence in systematic reviews and meta-analyses. For example, Hwang et al. 37 reported that 86.7% of systematic reviews on primary anterior cruciate ligament (ACL) repair included spin in their abstracts, with spin type 5 being the most commonly identified. Similarly, Carr et al. 38 found spin in 65.1% of systematic reviews evaluating treatments for Achilles tendon ruptures, with type 3 spin occurring most frequently. Foster et al. 8 examined spin in systematic reviews related to distal radius fractures and reported spin in 46% of abstracts, with spin type 1—where conclusions are not supported by the findings—being the most prevalent (19%). Our findings align closely with this broader trend. In the knee chondral defect literature, spin types 1, 3, and 5 were also among the most commonly observed, with type 3 appearing in 64.3% of abstracts. These findings collectively underscore a broader trend in orthopedic research: spin remains a common form of reporting bias across subspecialties. Whether by overstating treatment efficacy or downplaying methodological weaknesses, spin has the potential to distort the perceived strength of evidence. In the context of knee chondral defects—where treatment approaches vary widely and decision-making is often nuanced—the presence of spin further complicates the translation of research into practice. This reinforces the importance of critical appraisal skills among clinicians and greater adherence to reporting standards in future systematic reviews.
However, there remains a scarcity of research specifically examining spin in systematic reviews and meta-analyses related to surgical interventions for knee chondral defects. In an evaluation of spin in systematic reviews and meta-analyses related to surgical management of knee osteoarthritis, Siex et al. 11 discovered at least one type of spin in 35.4% of studies. However, they did not find any significant associations between spin and either AMSTAR-2 rating or extracted study characteristics. In addition, Woolley et al. 39 found that spin was present in 80% of the articles reviewing clinical trials of mesenchymal stromal cells for knee osteoarthritis. They similarly reported no statistically significant associations between spin and journal impact factor. While previous studies—such as those by Siex et al. 11 and Woolley et al. 39 —reported no significant associations between journal impact factor and the prevalence of spin, our analysis not only identifies a statistically significant link but also suggests a potential trend: studies with spin are not only more likely to be accepted by higher-impact journals, but may also present a broader array of spin types. This challenges the commonly held assumption that higher-impact journals are inherently more rigorous in detecting and eliminating biased reporting.
One possible explanation for this pattern is that higher-impact journals may prioritize positive or findings with high clinical impact, creating pressure for authors to frame results favorably. Boutron et al. 40 found that interpretation of findings was frequently inconsistent with the actual results in published randomized clinical trials, often presenting outcomes more optimistically than warranted. Chiu et al. 41 similarly reported that spin distorts the interpretation of results and misleads readers by making findings appear more favorable than they are. These patterns suggest that editorial and peer review processes may not consistently prevent spin, even in high-impact journals. 41
Recognizing spin is crucial for detecting bias in how research outcomes are communicated—particularly in systematic reviews and meta-analyses, which aim to provide clear and accurate summaries of existing evidence. Even when studies follow robust methodologies and employ validated tools like AMSTAR 2 or the Cochrane Risk of Bias tool, spin can still influence the way results are interpreted. Research examining a range of orthopedic procedures—including knee chondral defects, ligament repairs, and fracture management—has shown that abstracts containing spin often exaggerate positive outcomes, downplay limitations, and may lead to misplaced confidence in certain treatments.8,11,37 -41 In the study of knee chondral defects, spin in systematic reviews and meta-analyses is particularly concerning, as these types of studies are designed to provide the most comprehensive and reliable syntheses of available evidence to inform clinical decisions. Although systematic reviews and meta-analyses are generally considered the highest level of evidence, this designation is dependent on methodological quality. Prior meta-research has highlighted that flawed or biased reviews can produce misleading conclusions comparable in reliability to lower-level evidence or even expert opinion.13,42 These findings suggest that evidence hierarchies should account for methodological quality, recognizing that poorly executed reviews may not merit classification as high-level evidence. 43 Greater caution in interpreting such studies and increased emphasis on critical appraisal will help ensure that systematic reviews contribute meaningfully to evidence-based practice. More broadly, the proliferation of systematic reviews across scientific disciplines, sometimes outpacing the production of original studies, raises concerns about the academic and methodological motivations underlying their publication. In some cases, repeated or overlapping reviews may prioritize academic visibility over scientific necessity, thereby diminishing credibility and reproducibility. To preserve their value, systematic reviews should be assessed within a distinct methodological framework that emphasizes preregistration, transparency, and stricter editorial oversight. Therefore, manuscripts with abstracts that may contain biased or exaggerated interpretations must be critically appraised and read in full to ensure the effective and appropriate use of such interventions in clinical practice. A more rigorous approach to ensuring truthful appraisal of results will not only help advance science, but protect patients from interventions with questionable efficacy. Future research on reporting bias in knee chondral defect systematic reviews should also explore article-level bibliometric data, such as the relationship between citation counts of included articles and expected citation counts based on journal impact factors, to determine whether studies exhibiting spin are overperforming or underperforming relative to their expected citation impact. Such analyses could provide valuable insight into how biased reporting influences the visibility, dissemination, and perceived authority of research findings within the orthopedic literature.
Limitations
This study has several important limitations. First, identifying spin is inherently subjective, despite efforts to reduce bias through a consensus approach involving three independent reviewers. Second, the overall quality of included systematic reviews and meta-analyses was generally low, with most studies classified as level IV evidence and only a small proportion at level I, II, or III. In addition, certain limitations stem from study characteristics: many of the included reviews were published prior to the 2020 update of the PRISMA guidelines, which introduced enhanced standards for study selection, appraisal, and synthesis. Finally, the AMSTAR-2 tool used to assess methodological quality was only introduced in 2017, so its application to earlier reviews may have resulted in lower ratings that do not fully reflect study rigor, potentially influencing our quality assessments. Furthermore, although AMSTAR 2 is a validated and widely used appraisal tool, it is subject to inter-rater variability and may not capture all methodological nuances, introducing potential inconsistency in quality assessment. To mitigate this, multiple reviewers independently applied the checklist, and discrepancies were resolved by consensus to enhance reliability.
Conclusion
Most systematic reviews analyzing knee chondral defects were rated critically low in methodological quality according to AMSTAR-2 criteria, indicating generally weak evidence. Importantly, 85.7% of abstracts exhibited at least one type of spin, with the most frequent being spin type 3 (selective emphasis on treatment benefits), type 5 (asserting effectiveness despite high risk of bias), and type 1 (making clinical recommendations not adequately supported by the study results). This pattern reflects a recurring tendency to overstate results related to knee chondral defects. This analysis highlights the widespread presence of spin alongside low-quality evidence in reviews of knee chondral defects, underscoring the need for improved research rigor and critical appraisal to guide clinical decisions.
Footnotes
Ethical Considerations
This study is a systematic review of previously published literature and did not involve the collection of new patient data. As such, institutional review board approval and informed consent were not required.
Informed Consent Statements
This study did not involve human subjects directly and analyzed only previously published data. Therefore, informed consent was not required.
Consent to Participate
Informed consent is not required for this article.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.