
Abstract
Background
Single photon emission computed tomography (SPECT/CT) is a diagnostic option for knee osteoarthritis patients without osteoarthritic features on X-ray; however, the added value of SPECT/CT remains debatable in the diagnostic algorithm.
Objective
To review the added value of SPECT/CT in the diagnostic algorithm of knee osteoarthritis.
Study Design
Systematic review
Methods
A systematic search was carried out in the databases EMBASE, MEDLINE, and the Cochrane collaboration. The retrieved articles were screened for relevance on title and abstract. This was followed by a full-text study quality appraisal of the remaining articles. Finally, a total of 9 trials were included.
Results
The use of SPECT/CT might objectify some clinical knee osteoarthritis symptoms. It could correlate with findings on plain radiography and magnetic resonance imaging. Furthermore, there is some evidence SPECT/CT gives additional information compared with these imaging modalities; however, superiority is not proven. The uptake on SPECT could predict the intraoperative macroscopic findings. Yet the clinical relevance remains unclear.
Conclusion
There is no strong evidence SPECT/CT should play a role in the diagnosing and decision-making processes of knee osteoarthritis. Yet there is evidence suggesting SPECT/CT might give additional information in the diagnosing process. More research would be of added value to answer this research question.
Introduction
Patients experiencing pain of the knee suggestive of osteoarthritis without the radiologic features present a dilemma for orthopedic surgeons. This discrepancy between clinical and X-ray assessment raises the question whether the treatment should be based on the clinical symptoms and patient’s complaints or if there is an imaging based solution to help drive the decision process. 1 Clear diagnostic criteria for osteoarthritis remain unknown. 2 The National Institute for Health and Care Excellence’s (NICE) recommendations for Osteoarthritis Care and Management in adults do not require imaging diagnostics in some clinical cases. 3 However, the use of imaging is extensive in the clinical practice. Addition of sensitive imaging modalities may increase the recognition of osteoarthritic pathology and may even lead to increased treatment indications.
Changes due to early osteoarthritis remain often unseen in plain radiography. 4 Magnetic resonance imaging (MRI) has some role in the diagnosis and follow up of osteoarthritis, as well as in some research settings. It can visualize structural pathology not seen by radiography. However, due to the lack of correlation with clinical need, as well as high cost and time consumption, it is not routinely used in the clinic.5,6 After an inconclusive X-ray in symptomatic patients, some physicians select nuclear imaging such as single photon emission computed tomography (SPECT/CT) as an additional diagnostic test.
In degenerative lesions, bone scintigraphy with modern SPECT/CT assesses the location and metabolic activity by means of radioisotope accumulation. 5 It is an option if plain radiography is not decisive or when MRI is not possible. SPECT/CT is in general widely available in most large nuclear medicine departments. The CT component helps specify the lesion showing uptake, while the SPECT component makes it possible to grade the activity associated with structural changes of the bone. Thus, in SPECT/CT, SPECT increases the sensitivity, while CT increases the specificity. 7 Compared with SPECT alone, the use of modern SPECT/CT increases the diagnostic accuracy for orthopedic disorders of the extremities. Besides, it reduces the time to the working diagnosis. 8 SPECT/CT would be promising in the diagnosing process and management of orthopedic disorders. 9
Yet, to our knowledge, no systematic review has been done on the overall role of SPECT/CT for knee osteoarthritis. Regardless of the accuracy of the SPECT/CT, the question remains whether decision making should be based on this imaging modality. This systematic review examines and reports the literature to address the role of SPECT/CT in the diagnostic algorithm for knee osteoarthritis.
Methods
A systematic literature search has been conducted on June 9, 2018, in the electronic databases of MEDLINE (http://www.pubmed.com), EMBASE (http://www.embase.com), and the Cochrane collaboration (http://www.cochrane.org). The search included the search terms “(SPECT OR nuclear imaging OR FDG PET OR PET) AND (osteoarthritis OR knee)” and was limited by title and abstract.
All articles were initially screened by the title and abstract for relevance. Any trial potentially focusing on the diagnostic value of SPECT/CT for knee osteoarthritis was identified as relevant. Exclusion criteria were case reports, animal studies, and cadaver studies. Furthermore, only studies with a patient population with knee osteoarthritis or possible knee osteoarthritis were included. Other pathology such as meniscal tears, chondral lesions, and anterior cruciate ligament lesions were excluded unless they were found in an osteoarthritis population.
Full texts of the relevant articles were obtained, and the authors of missing articles were approached by email for the request of the full text. After a full text screening, relevant articles were assessed on risk of bias and applicability based on the QUADAS-2 (Quality Assessment of Diagnostic Accuracy Studies–2). 10 First, the research question was evaluated in general. Second, a flow diagram of the study was drawn. Third, 3 domains were assessed on bias and applicability according to the QUADAS-2, including patient selection, index test, and reference standard. The fourth domain, concerning patients flow and timing of the diagnostic tests, was only assessed on risk of bias. To answer our research question, articles were included based on the risk of bias and applicability. The QUADAS-2 signaling questions assisted in these judgments. The patient selection domain covered selection bias. The index test and reference test sections concerned information bias and detection bias. Confounding was assessed using the flow and timing domain. Articles were excluded if the risk of bias was high once or unclear in more than 2 domains. A high concern on any domain for applicability meant exclusion of that article. These restrictions were made specifically for this review only. The purpose of the QUADAS-2 is not to be a quality score and there are no thresholds for including articles. 10 The threshold in this literature study was found appropriate based on similar criteria after reviewing all relevant evidence, as is recommended. 11 If possible, homogenous outcome parameters of the included studies will be used in a meta-analysis.
Results
The electronic database search resulted in 1760 articles, as Figure 1 illustrates. In the title and abstract screening, 161 articles were selected for full text screening. Among them, 94 articles were marked as irrelevant due to: no involvement of SPECT(/CT) or an unrepresentative patient population for our research question. Often, these studies focused only on positron emission tomography (PET) or had a population with inflammatory arthritis in other joints than the knee. Also, reviews and in vitro studies were among them. In addition, 24 studies were excluded since no full text appeared to be available after contacting the authors. The remaining 43 articles were assessed with the QUADAS-2. Finally, a total of 9 articles were included.12-17,20-22 Table 1 presents the results of the QUADAS-2 assessments of these articles. A meta-analysis was not possible due to the heterogeneity of outcome parameters, as Table 2 presents. The data of the 9 included studies is expressed in this systematic review and will be further explained per diagnostic entity.
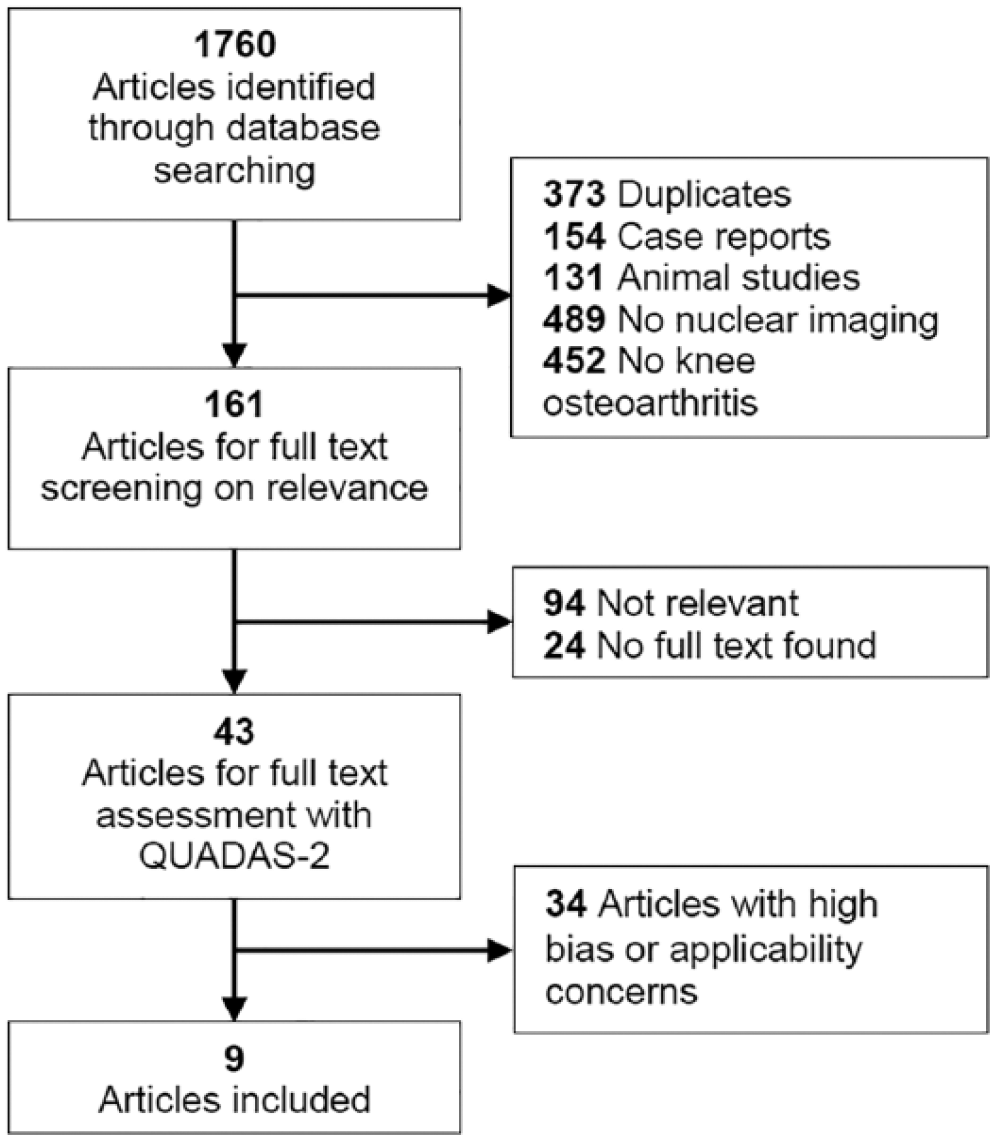
Flowchart of articles.
Quality and Applicability Assessment. a
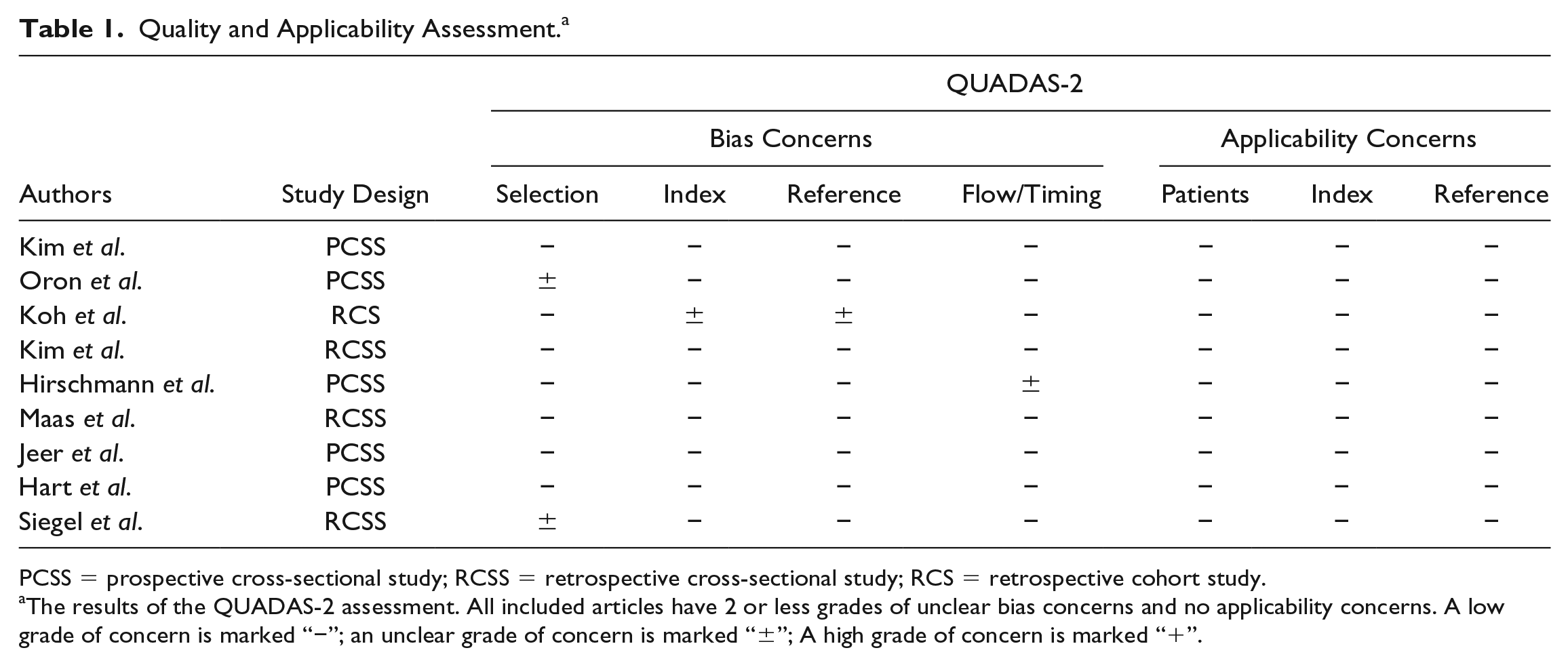
PCSS = prospective cross-sectional study; RCSS = retrospective cross-sectional study; RCS = retrospective cohort study.
The results of the QUADAS-2 assessment. All included articles have 2 or less grades of unclear bias concerns and no applicability concerns. A low grade of concern is marked “−”; an unclear grade of concern is marked “±”; A high grade of concern is marked “+”.
Study and Patient Characteristics. a
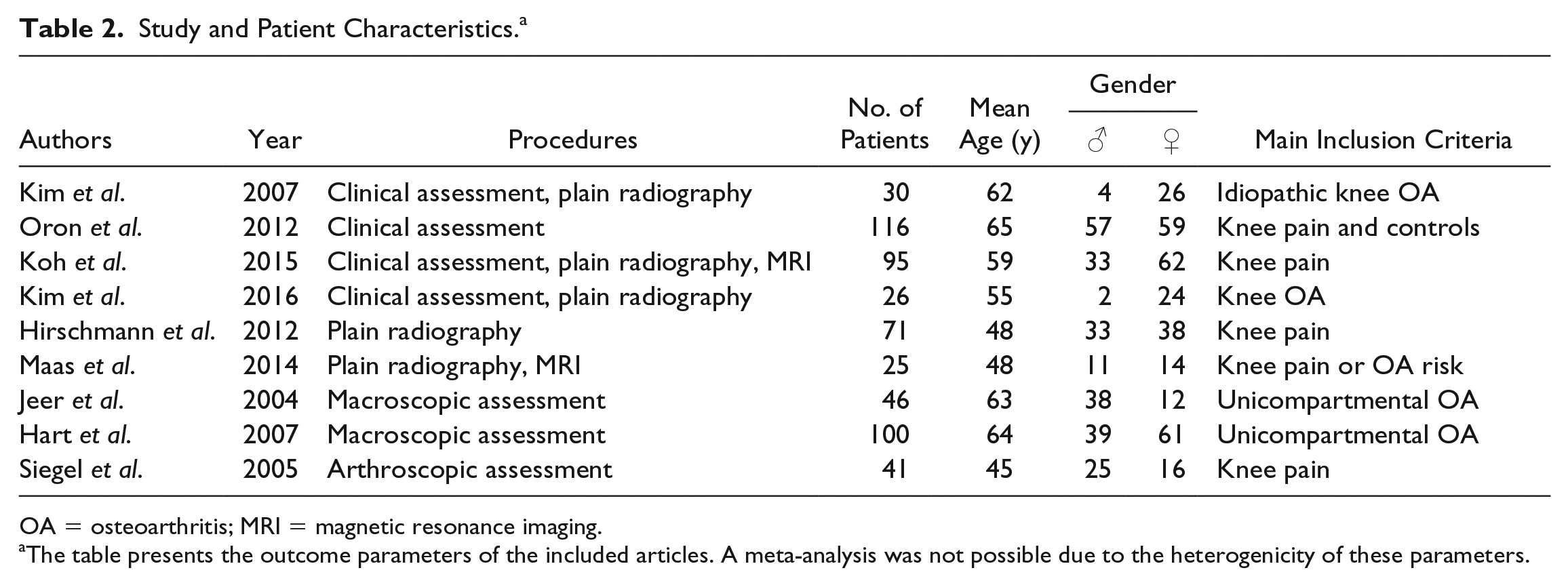
OA = osteoarthritis; MRI = magnetic resonance imaging.
The table presents the outcome parameters of the included articles. A meta-analysis was not possible due to the heterogenicity of these parameters.
Clinical Evaluation
Four articles have covered the comparison with the clinical presentation.12-15 Two prospective studies investigated the correlation of SPECT and the clinical assessment.12,13 In both studies, higher uptakes in symptomatic patients were significantly associated with more knee symptoms such as pain scores and physical examination (joint tenderness and excessive joint fluid). However, this did not count for all compartments and all aspects of a physical examination. Furthermore, Kim et al. 12 found no link between SPECT findings and age, sex, body mass index, and blood variables (C-reactive protein and erythrocye sedimentation rate). However, the uptake in SPECT was correlated with ultrasound abnormalities in especially the medial compartment. 12 Two retrospective studies also compared the clinical evaluation with SPECT/CT.14,15 Koh et al . 14 determined whether uptake on SPECT/CT could predict the treatment response. 14 A group of patients was treated conservatively (medication, physical therapy, lifestyle modification, and exercise) and another group both conservatively and surgically. Type of surgery was unclear and not described. The patients were followed up to determine the decrease in knee pain. Consequently, there was no correlation between treatment method and response (P = 0.8). However, age (P = 0.001) and initial pain (P = 0.02) did correspond with higher uptake in SPECT/CT. The conservative treatment response of patients with an increased uptake was better than patients with no tracer uptake (P = 0.04). Nevertheless, patients with a surgical treatment and increased SPECT/CT uptake showed no better treatment response. 14 Kim et al. 15 examined the correlation of SPECT/CT and clinical assessment only for patients scheduled for surgical treatment of the medial compartment. The overall uptake on SPECT/CT was higher in the knees selected for operation compared with the contralateral knees (P < 0.0001). Yet, no SPECT/CT imaging parameter was related to patient symptom scores. 15 In short, the uptake on SPECT correlates with some clinical aspects; however, discrepancies between clinical symptoms and SPECT are common.
Plain Radiography
Most orthopedic surgeons use X-ray imaging to visualize the extent of knee osteoarthritis. When the X-ray is not clear or decisive, the question arises whether SPECT/CT has an additional value. Kim et al. also compared the diagnostic values of SPECT and plain radiography. 12 Overall, the Kellgren and Lawrence grading correlated with the SPECT uptake. Furthermore, some symptomatic patients lacking osteoarthritis features on plain radiography, still had an increased uptake on SPECT. In addition to this, the Kellgren and Lawrence grading did not correlate with the clinical symptoms, while SPECT did. 12 Three studies investigated the correlation with SPECT/CT.15-17 These studies underline that, in general, Kellgren and Lawrence scores correlate with uptake on SPECT/CT. This was the case in the more severe medial compartment osteoarthritis and in the more moderate cases of multicompartment knee osteoarthritis.15-17 Hirschmann et al. 16 found that higher uptakes on SPECT/CT for the medial compartment correlated with a varus alignment and a higher uptake on the lateral compartment correlated with a valgus alignment. This would be due to a higher stress as a result of varus or valgus alignments. 16 In summary, these studies show correlations between SPECT uptake and plain radiography. However, no study focused on the role of SPECT in symptomatic patients lacking osteoarthritic features on plain radiography.
Magnetic Resonance Imaging
Even if SPECT/CT would have an additional diagnostic value over conventional radiography, the question is whether it is preferred over MRI. Two studies made the comparison of SPECT/CT and MRI. Maas et al. 17 investigated the link between cartilage morphology found on 3T-MRI and remodeling of the subchondral bone on SPECT/CT. 17 Despite having a population with low Kellgren and Lawrence grades (mean 1.6), there was a high prevalence of MRI-detected cartilage lesions (53% of Kellgren-Lawrence grade 1). 17 The authors refer to an epidemiological study with subjects without evident knee osteoarthritis on plain radiography. 18 They suggest that since these patients still had a substantial prevalence of focal cartilage lesions, these lesions might be the cause of some elevations in SPECT/CT uptake. An elevated subchondral uptake on SPECT/CT did correlate with the grade of cartilage lesions found on MRI (P < 0.0001). The thicker and more severe the lesions on MRI, the higher the uptake on SPECT/CT. However, there were cases in which normal cartilage grading on MRI still had an elevated uptake on SPECT/CT. It remains unclear if these precede the onset of cartilage damage. 17 Kim et al. 15 also drew the line between the uptake on SPECT/CT and findings on MRI for medial compartment osteoarthritis. The uptake correlated significantly with the MRI cartilage scores.
Intraoperative Assessment
Arthroscopy and intraoperative findings are not used for diagnosing knee osteoarthritis because that remains a clinical diagnosis. Surgery is however the moment we can properly examine the whole joint internally, including palpation, tracking, and tissue interplay. Diagnostic arthroscopy is considered more obsolete in (inter)national treatment guidelines. 19 Three studies compared the findings on SPECT with an intraoperative assessment. Two studies examined the correlation between preoperative SPECT findings and the intraoperative assessment for the indication unicompartmental knee osteoarthritis.20,21 A significant association was found between the SPECT findings and the macroscopic assessments of knee osteoarthritis.20,21 Normal SPECT uptake predicted minimal macroscopic chondral lesions on the less affected compartment (P < 0.05). 21 Siegel et al. 22 investigated if SPECT can predict the severity of knee pathology in patients undergoing knee arthroscopy. The uptake on SPECT correlated with the arthroscopic findings of articular cartilage pathology in the menisci and the medial femoral condyle (P < 0.001). More uptake at these locations would mean more severe damage at arthroscopy, and less uptake meant less damage. 22
Discussion
This review shows that there is some evidence SPECT/CT has benefits in the diagnosis and decision-making process of knee osteoarthritis. SPECT/CT might help in showing structural and biological signal change related to clinical symptoms, yet there is no study directly designed to illustrate that SPECT/CT gives definitive information that alters the clinical process relevantly. However, it gave, in some studies, similar outcomes compared with plain radiography and MRI in detecting knee osteoarthritis. Furthermore, there are indications that it brings different additional information compared to these imaging modalities. The findings on SPECT predict macroscopic assessment, while the clinical relevance of this remains unknown.
Kim et al. 12 and Oron et al. 13 found some objectification of clinical symptoms by SPECT, especially in the medial compartment. The study of Koh et al. 14 underlined this, while failing to show better post-operative outcomes in patients with high uptakes. Pain would predict uptake on SPECT/CT and patients with higher uptakes showed a better response to conservative treatment. In other words, this seems like patients with more pain showed more relief from treatment. In addition to the fact that hot focal uptakes on SPECT/CT did not predict the location or the severity of initial pain, these results are doubtable. Kim et al. 15 found even no correlation between symptom scores and SPECT/CT uptakes. Regarding the comparison with plain radiography, Kim et al. 12 suggested that SPECT can detect clinical osteoarthritis before its features appear on the plain radiography. This was as symptomatic patients without features on the plain radiography, still had high SPECT uptakes. The identification of abnormal uptake in symptomatic patients without radiographic abnormalities is definitely valuable, as it may objectify the onset of osteoarthritis. Kim et al., 15 Hirschman et al., 16 and Maas et al. 17 found correlations with plain radiography. But, in essence it tells the physician what he already knew from the plain radiography. The study of Maas et al. 17 showed a correlation between SPECT/CT and MRI in the detection of chondral lesions. Kim et al. 15 found this while examining only the medial compartment. 15 Maas et al. 17 illustrated that SPECT/CT did show some alteration, where MRI missed them. This might indicate the additional role of SPECT/CT. The question about which modality is better, remains unclear as real controls and a golden standard lacked in both studies. Jeer et al. 20 did show that preoperative SPECT can predict the macroscopic cartilage damage, especially in the medial compartment. Hart et al. 21 and Siegel et al. 22 found the same correlation for only the medial compartment. Yet these studies do not identify any decisive role for SPECT in whether to proceed to a surgical treatment. These intraoperative studies have done no other examination than a macroscopic assessment. As Saal et al. 23 concluded, even the gold standard might be mildly inaccurate.
The findings of this systematic review are partially in line with the review of Hirschmann et al. 24 They recommended the use of SPECT/CT in discrepant cases, if plain radiography and MRI do not correlate with clinical findings. Based on the evidence, SPECT/CT might detect changes of early osteoarthritis before detection on radiographs or MRI. This gives opportunities for preventive or disease modifying interventions and patient education. However, with the current literature a strong recommendation cannot be made since no evidence is available showing better outcomes of therapy in them. 24 The review of Huellner et al. 7 is in line with Hirschmann et al. 24 while emphasizing the lack of literature on this subject.
We feel this partial discrepancy may be explained because of different methodology used in those studies. We applied the rules and methodology of systematic review when conducting and discussing a heterogeneity of articles. This systematic review included only studies with SPECT(/CT) for the preoperative diagnosis of knee osteoarthritis. A limitation of this systematic review is that all studies with SPECT, without the CT component, were also analyzed due to the lack of literature. All these studies found correlations in the use of SPECT in some way. Since SPECT/CT is a more accurate diagnostic tool than SPECT, these correlations should be taken into account in favor of SPECT/CT.8,24 Nevertheless, none of these significant correlations prove the role of SPECT/CT in the decision-making process. As a result of this review, a study is recommended that actually covers the discrepant cases lacking osteoarthritis features on plain radiography. It should become clear that more SPECT uptake predicts better treatment responses, for example, after total knee replacement. Up until that point, the use of SPECT/CT is not justified from the perspective of evidence-based medicine. Furthermore, given the fact that SPECT/CT is an invasive method, and the cost might not be lower, it should not be considered as a routine method rather than MRI.25-27
The use of SPECT/CT might give potentials for new approaches of diagnosing knee osteoarthritis. Kraus et al. 28 used SPECT/CT and etarfolatide as a tracer for localizing macrophage activation in patients with knee osteoarthritis. Macrophage activation correlated with radiographic knee osteoarthritis and patient symptoms. This was the first in vivo indication for activated macrophage involvement in osteoarthritis. The use of SPECT/CT with etarfolatide as tracer might be of value for selecting patients who are likely to benefit from macrophage-targeted therapies. 28 Furthermore, Cachin et al. 29 found promising results in an ex vivo study investigating the use of 99mTc-NTP 15-5 as a SPECT/CT tracer. This would indicate a functional direct imaging of osteoarthritis at the proteoglycan level, unlike indirect tracers previously used. 29 Additionally in the field of nuclear imaging, the use of PET has been promising in the early detection of metabolic joint alterations linked to osteoarthritis. 18 F-NaF PET/CT imaging might be useful in the objectification of the degree of cartilage and bone interactions in osteoarthritis.30,31 Besides, the joint inflammation, ageing, radiographic severity and clinical symptoms have been quantified using this imaging modality.32,33
Despite new experimental approaches and significant correlations, the role of SPECT/CT in the decision-making process of knee osteoarthritis is not fully clear. There is some evidence that it gives additional information. For example, SPECT has identified abnormal uptake in symptomatic patients without radiographic and MRI abnormalities. Yet, there is no strong evidence for using SPECT/CT in discrepant cases with osteoarthritic knee symptoms and absent radiographic features. More clinical studies are needed to better define the role of SPECT CT in the diagnostic algorithm of knee osteoarthritis.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.