
Abstract
Objective
To assess articular cartilage degeneration in anterior cruciate ligament (ACL) reconstructed knees as detected by MR T1rho and T2 mapping relative to controls and longitudinally at 3 months and 1 year after ACL reconstruction (ACLR).
Design
Twenty-five patients with acute ACL injury were enrolled (13 women and 12 men; mean age 30.8), and 14 healthy controls were selected by sex and age matching. The affected knees of the ACLR participants were imaged using a 3.0T magnetic resonance (MR) scanner 3 months and 1 year after ACLR. Cartilage T1rho and T2 values were quantified for subcompartments in the full-thickness, superficial, and deep layers and were compared with the matched subcompartments of control knees. The influence of concomitant meniscal tears identified using proton density-weighted imaging (PDWI) was also investigated.
Results
In the posterior lateral tibia, T1rho and T2 values were significantly higher in ACLR participants at 3 months and slightly decreased at 1-year compared to the control group. T1rho values in the medial compartment exhibited a significant increase at 1-year compared with those of control knees, while T2 showed no significance. In cartilage with medial meniscal tears, the T1rho values in multiple medial subcompartments were significantly higher than those in cartilage without medial meniscal tears, and this alteration was relatively detectable by T1rho.
Conclusions
T1rho and T2 mapping is effective in evaluating cartilage degeneration following ACLR. T1rho may exhibit greater sensitivity for assessing the progression of early degeneration in the medial compartment after ACLR.
Introduction
Anterior cruciate ligament (ACL) tears are among the most common knee injuries and are often treated with arthroscopic ACL reconstruction (ACLR). Although good postoperative results are generally reported, ACL-reconstructed knees remain at a high risk of developing osteoarthritic changes.1-6 The association between bone bruising 7 and cartilage damage at the time of injury, 8 concomitant meniscectomy, 9 and residual abnormal kinematics, such as anterior tibial translation and internal tibial rotation,10-12 contributes to the progression of posttraumatic osteoarthritis (PTOA).
In diagnosing knee osteoarthritis (OA), several imaging methods are available. Conventional magnetic resonance imaging (MRI) is used to detect morphological changes in the cartilage, such as surface fraying, fissuring, and cartilage thinning;13-17 however, it does not show structural changes in the cartilage that occur before morphological changes due to degeneration, as does the quantitative MRI (qMRI).
Advancements in MRI sequences and high-field MRI have enabled the quantitative evaluation of cartilage, which has provided information on cartilage matrix changes, including the primary constituents of collagen, proteoglycans, and water.18-22
T1rho (longitudinal relaxation in the rotating frame) and T2 (transverse relaxation time) mapping are both compositional MRI techniques that are used in clinical practice. T2 relaxation time correlates with the collagen fibril orientation and organization and water concentration in articular cartilage. 23 T1rho values correlate with decrease in proteoglycan content in cartilage. 24 Previous studies25,26 have demonstrated the utility of T1rho and T2 mapping in assessing cartilage, with an initial emphasis on comparing patients with OA to healthy individuals. Several studies show that T1rho is more sensitive for cartilage degeneration and has a higher dynamic range than T2 mapping,27-29 implying that T1rho can detect subtle changes in the extracellular matrix of the cartilage.
Although numerous studies have reported elevated T1rho and T2 values in the articular cartilage of ACL-injured knees,30-40 owing to limited imaging facilities, particularly for T1rho, reports on the longitudinal analysis using simultaneous T1rho and T2 acquisition are still required to compare the efficacy of the two imaging methods.
As articular cartilage has a limited capacity to heal, therapeutic interventions to avoid the progression of cartilage degeneration are essential. To achieve this objective, the characteristics of PTOA after ACLR must be precisely investigated.
Although single-bundle reconstruction is the most commonly performed ACLR technique, double-bundle reconstruction offers greater anatomical and biomechanical resemblance to a normal ACL41,42 and is expected to lower the incidence of PTOA. Previous studies on ACL reconstructed knees with simultaneous T1rho and T2 mapping have exclusively assessed single-bundle reconstruction. This study, to the best of our knowledge, is the first to report the utilization of T1rho and T2 mapping in double-bundle reconstructed knees. We compare this approach to those of previous studies involving single-bundle reconstructed knees to investigate the potential inhibition of postoperative cartilage degeneration.
We hypothesized that both T1rho and T2 would significantly increase in the lateral compartment at the time of injury, which is often damaged by a large force when the knee subluxates, and only T1rho elevation would be observed in the medial compartment, where degeneration appears gradually over time after operative intervention.43,44
Methods
Study Design and Participants
This study was designed as a retrospective, longitudinal cohort study using MRI data obtained in a previous prospective study which had already been conducted between 2012 and 2014. Data collection was approved by the Chiba University Graduate School of Medicine (M10562) and Teikyo University Chiba Medical Center (11-35) institutional ethics review board for Human Research.
Enrollment began in April 2012 and ended in April 2014. Informed consent was obtained from all participants, and parental consent was obtained from individuals under the age of 20.
Individuals with acute ACL injury were enrolled, and MR T1rho and T2 mapping was performed 3 months and 1 year after ACLR. Participants between 16 and 45 years of age were included. The exclusion criteria included concomitant ligament injury or fracture, cases of re-injury or chronic course, history of lower extremity trauma, and full thickness of the chondral defect (unable to draw region-of-interest [ROI] curves).
All surgeries were performed using standardized procedures for double-bundle anatomical ACLR using the transportal technique by 3 surgeons all with more than 15 years of experience. The hamstring tendon autografts were harvested, split, and folded to reconstruct anteromedial (AM) and posterolateral (PL) bundles. Two bone tunnels were created for AM and PL bundles in the femur and tibia, respectively. Each bundle was fixed with buttons on the femur and staples on the tibia. All patients underwent a standardized rehabilitation program which consisted of range of motion, mobility training, and muscle strengthening.
Control participants between 16 and 45 years of age with no complaints or past knee injuries were enrolled.
Imaging Protocols
All MRI examinations were performed using a 3.0-T Signa HDxt MRI scanner (GE Healthcare, Waukesha, WI, USA) with an 8ch transmit-receive knee coil. Three-dimensional (3D) sagittal fat-suppressed spoiled gradient-recalled (SPGR) sequences were used for T2 and T1rho relaxation time quantification. 45 The T2 mapping sequence parameters were as follows: repetition time/echo time (TR/TE), 5.6/0, 10. 30, 60 ms; field of view (FOV) = 140 mm; matrix = 288 × 288; slice thickness = 3.0 mm; number of slices = 32; bandwidth (BW) = 244 kHz; flip angle = 15°; acquisition time for 4 TEs = 7 min 52 s. The T1rho mapping sequence parameters were: TR/TE = 5.6/8 ms; FOV= 140 mm; matrix = 288 × 288; slice thickness = 3.0 mm; number of slices = 32; BW = 244 kHz, time of spin-lock (TSL) = 0/10/30/60 ms; spin lock freq (FSL) = 500 Hz; and acquisition time for 4 TSLs= 7 min 23 s. 46
Meniscus injuries and cartilage defects were identified by using 2-dimensional sagittal and coronal fast spin-echo proton density-weighted images (PDWI). The PDWI sequence parameters were as follows: TR/TE = 2000/32 ms; FOV = 140 mm; matrix = 416 × 416; slice thickness = 3 mm; number of slices = 26; BW = 244 kHz; acquisition time = 4 min 2 s.
In the case of a possible motion artifact in the original images used for T1rho or T2 mapping, images were reacquired.
MR Assessment, Segmentation, and Processing
All MR images were reviewed, and the segmentation of T1rho and T2 mapping was performed by a single investigator with ten years of experience. Meniscal injuries and cartilage defects were identified using sagittal and coronal PDWI performed preoperatively.
Based on previous reports,
47
the cartilage was manually segmented on sagittal T1rho and T2 mapping images. Three slices each were selected from the central, medial, and lateral compartments. After defining the medial femoral condyle (MFC), medial tibial plateau (MTP), lateral femoral condyle (LFC), and lateral tibial plateau (LTP), they were further divided into subcompartments with regard to meniscus which creates 3 subcompartments for MTP and LTP, 4 for MFC, and 5 for LFC (
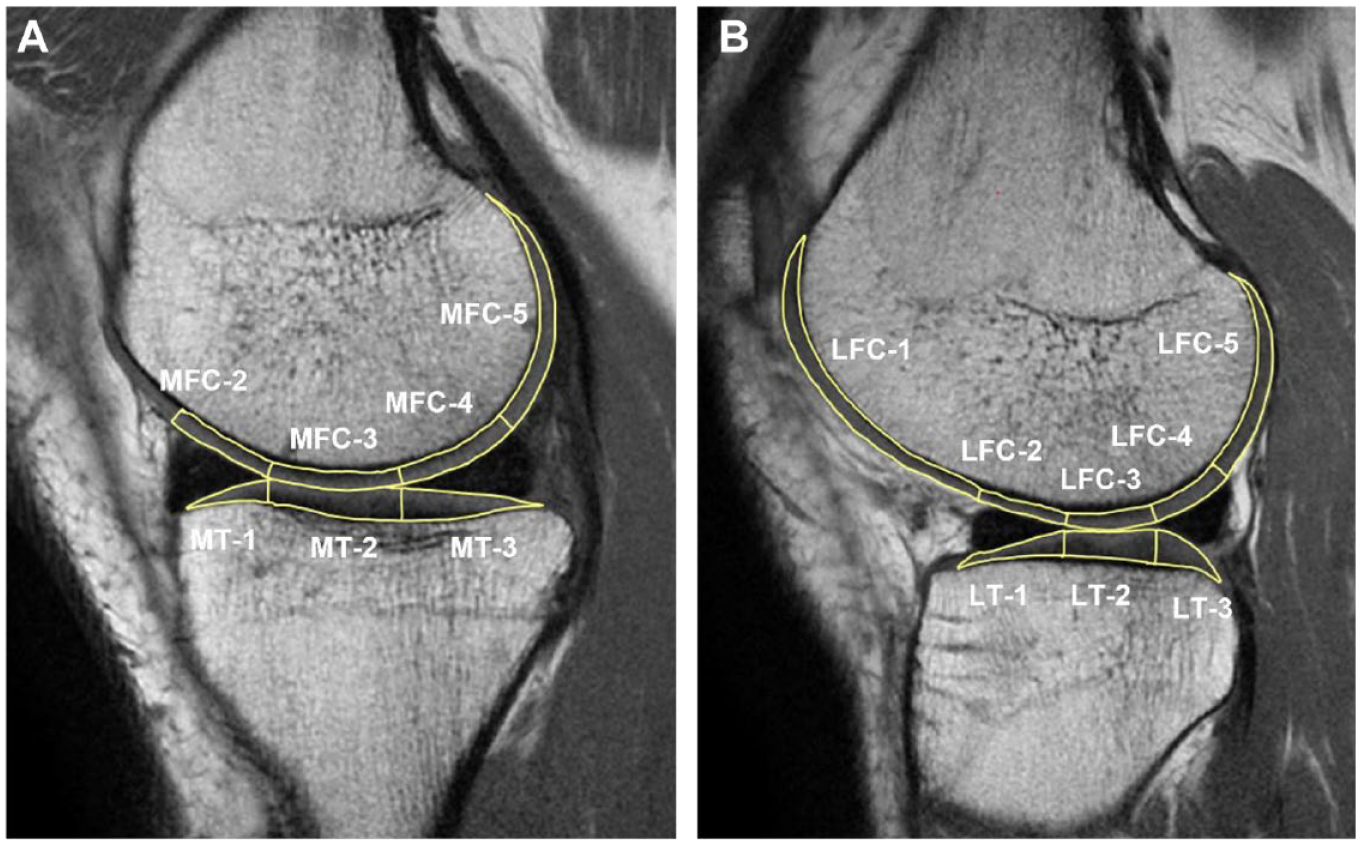
Segmentation of the sagittal MRI image of the (A) medial and (B) lateral compartments of the knee joint. The MFC, MTP, LFC, and LTP are divided into subcompartments with respect to the meniscus. MFC 2-4, MT1-3, LFC2-4, and LT1-3 are weight-bearing regions facing the anterior horn, cartilage, and posterior horn, respectively.
T1rho and T2 calculated maps were generated using the commercially available image processing software AZE Virtual Place (Canon, Tokyo, Japan). A Levenberg–Marquardt monoexponential fitting algorithm was used for T1rho and T2 calculation. 45 T1rho- and T2-weighted image intensities obtained for different TSLs and TEs were fitted pixel-by-pixel to the following equations, respectively:


Statistical Analyses
The T1rho and T2 values of the control participants and patients at 3 months and 1 year of follow-up were compared using analysis of variance and multiple comparison tests. Data are presented as means ± standard deviation. Differences among groups were compared using one-way analysis of variance (ANOVA) with Tukey’s post-hoc tests. The values were compared in matched subcompartments for the full, superficial, and deep layers. Value comparison between subcompartments with and without meniscal tears was performed using Welch’s t-test. T-test was used to generate comparisons of demographics for study participants. The level of significance was set at P < 0.05. All statistical analyses were performed using EZR 48 version 4.2.0.
Results
Table 1 summarizes the demographic information of the ACLR patients and controls analyzed in the current study. Twenty-five patients with acute ACL injuries were enrolled (13 women and 12 men), with a mean age of 30.8 years at the time of injury (range, 15–49 years). Fourteen healthy participants for the control group without any knee injuries or clinical symptoms of OA were selected by matching for sex and age. The mean body mass index (BMI) was 24.28 kg/㎡ and 25.6 kg/㎡ for each ACLR group and control group, and there was no significance between the patient group. Among the patient group, 11 had medial meniscal (MM) injuries, 10 had lateral meniscal (LM) injuries and 6 patients had both MM and LM injuries.
Characteristics of the Study Participants.
Full-Layer Analysis
In the medial compartment, T1rho relaxation times in MFC2 at 3 months exhibited a significant increase compared with those in healthy control participants, and these elevations were stable at the 1-year follow-up (
Table 2
;
Mean T1rho and T2 Values in Full Layers.
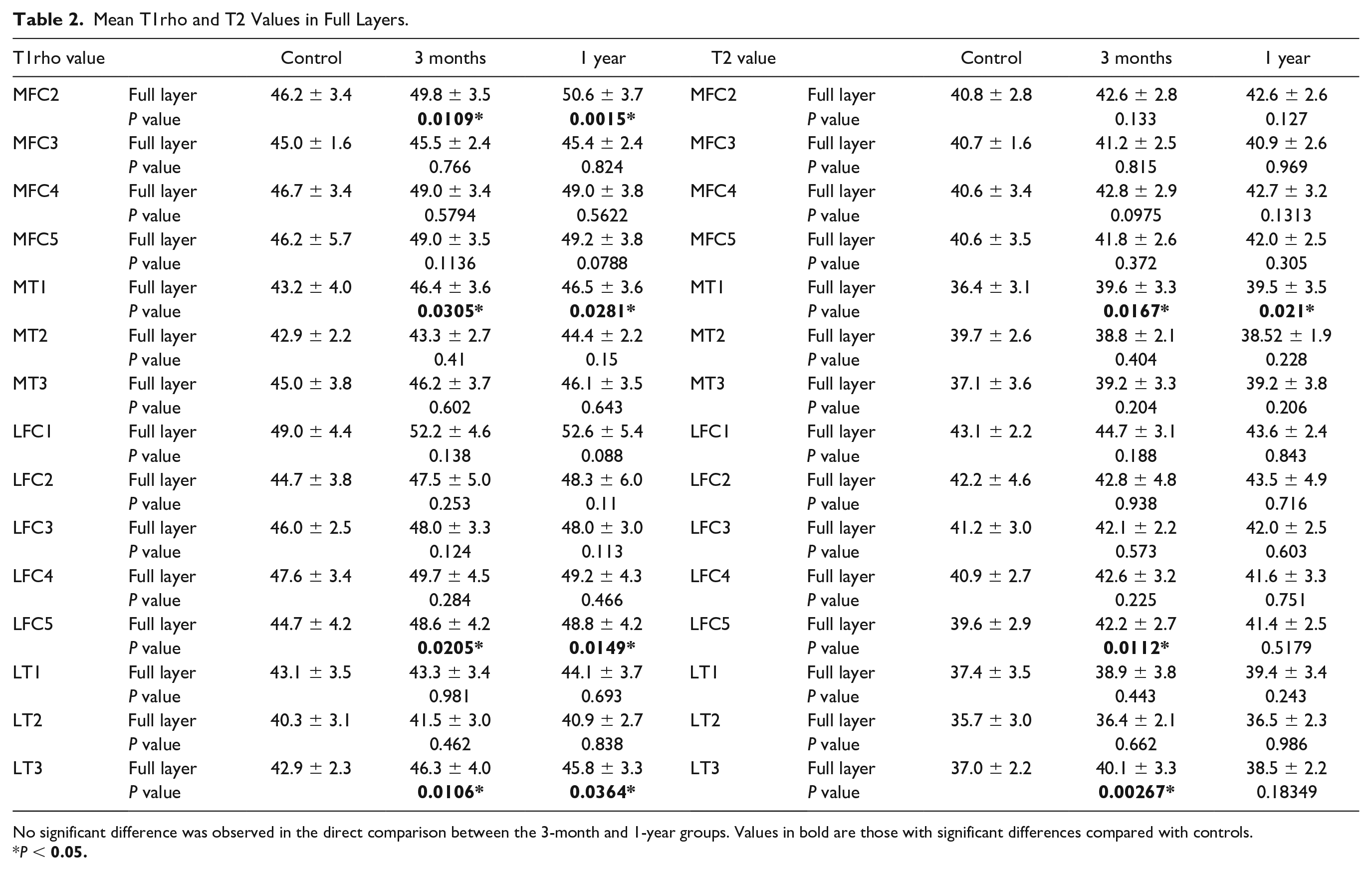
No significant difference was observed in the direct comparison between the 3-month and 1-year groups. Values in bold are those with significant differences compared with controls.
P <
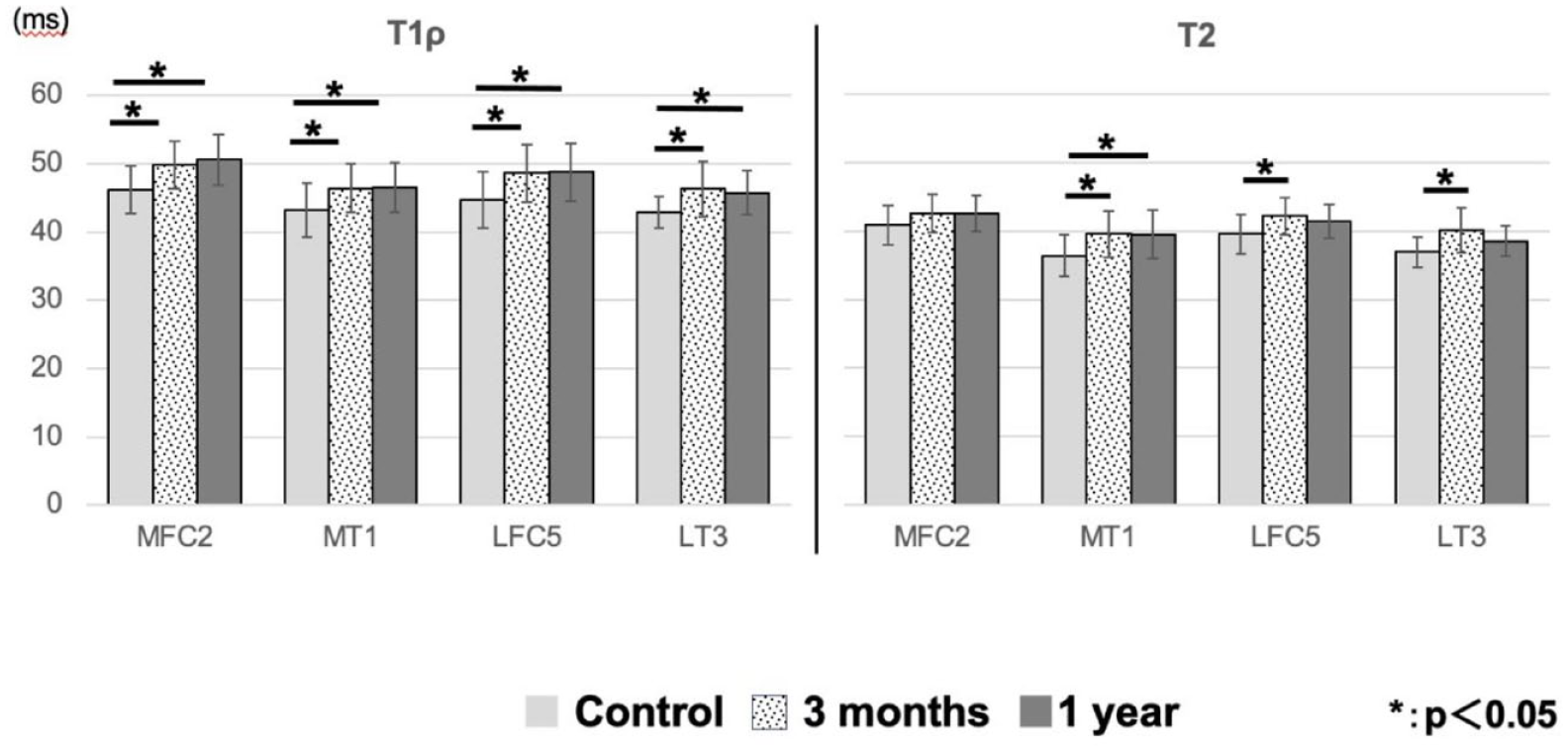
Comparison of T1rho and T2 values in the full-layer cartilage. The T1rho values in MFC2, MT1, LFC5, and LT3 showed significant differences between the control and ACL-reconstructed knees at each time point.
Laminar Analysis
Values revealed differences to the controls in several medial subcompartments and LT3 (
Table 3
;
Mean T1rho and T2 Values in Superficial and Deep Layers.
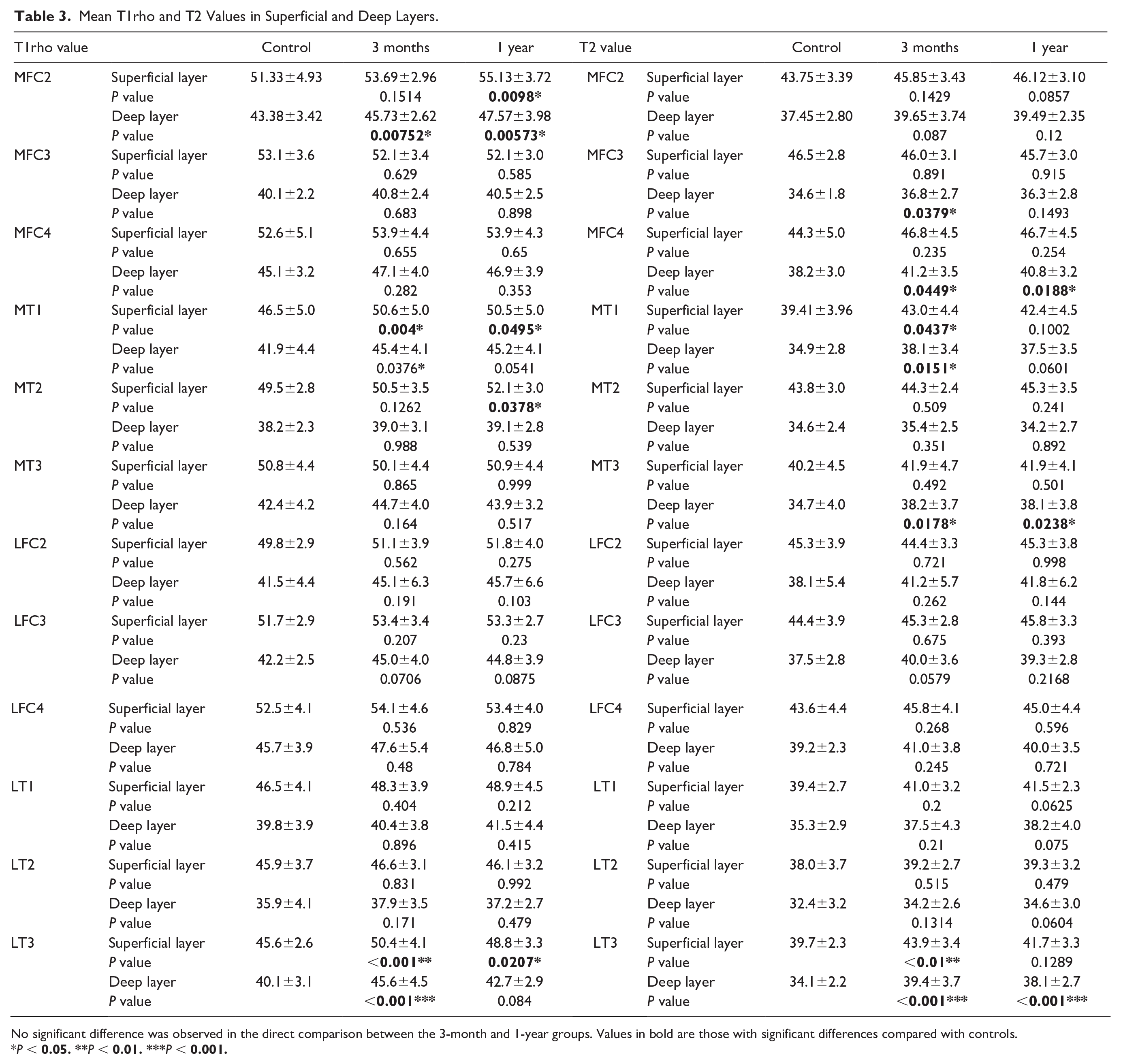
No significant difference was observed in the direct comparison between the 3-month and 1-year groups. Values in bold are those with significant differences compared with controls.
P <
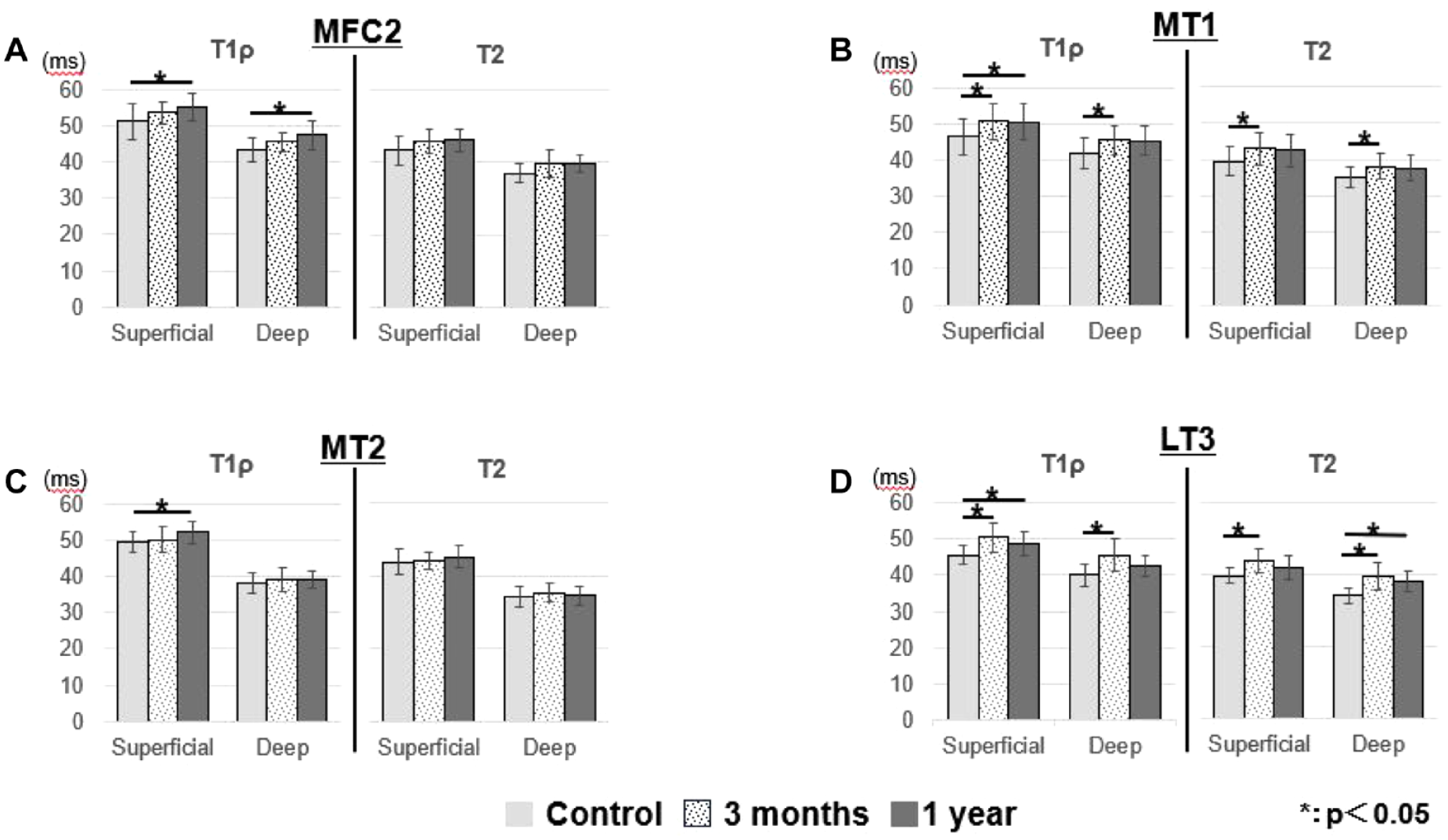
T1rho and T2 value comparisons in the superficial and deep layers of cartilage in (A) MFC2, (B) MT1, (C) MT2, and (D) LT3.
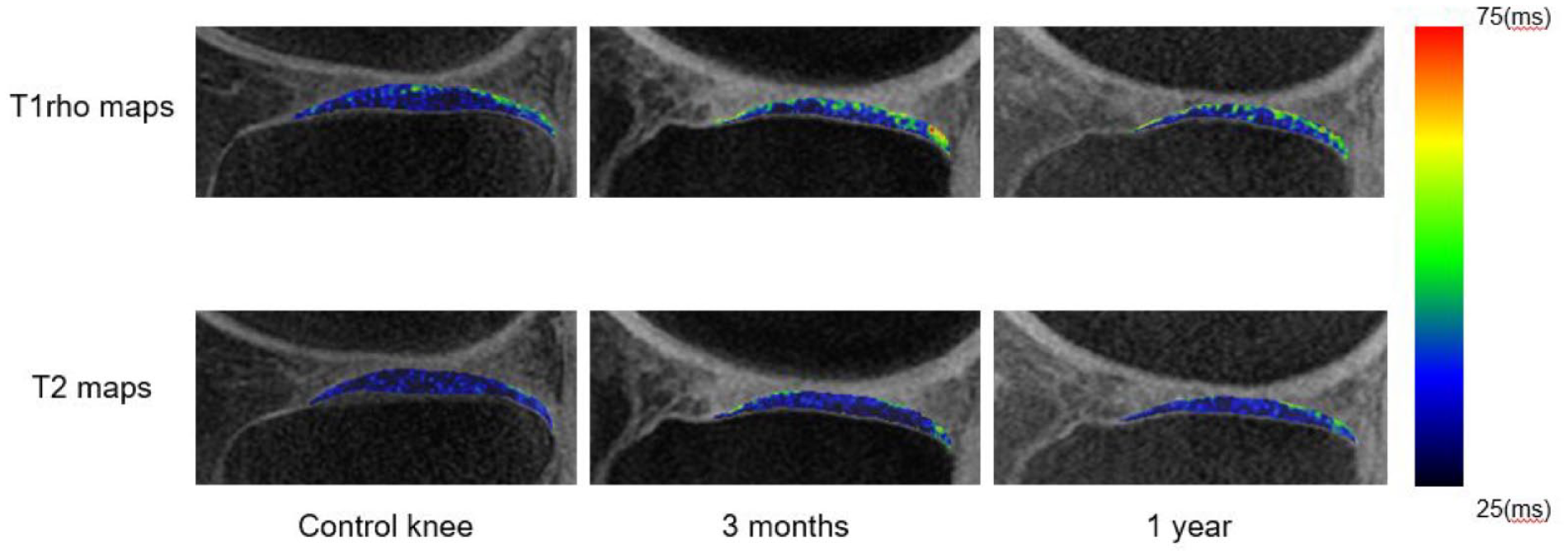
T1rho and T2 mapping of LTP in a control knee (17-year-old, female) and an ACLR knee (21-year-old, male) at 3-month and 1-year follow-ups. LT3 values at the 3-month follow-up showed significant elevation in T1rho and T2 for both layers, however, at the 1-year follow-up, the values decreased to show no significance in the superficial layer in T2 but remained in T1rho.
In MT1, for both layers, T1rho and T2 values were significantly higher than those in the control participants at 3 months and T1rho remained high at 1 year.
LT3 values at the 3-month follow-up showed significant elevation in T1rho and T2 for both layers, but at the 1-year follow-up, the values decreased to show no significance in the superficial layer in T2 but remained elevated in T1rho.
T2 elevation in MFC3, MFC4, and MT3 was observed only in the deep layers compared with the control group. None of the compartments in either analysis indicated significant differences between the 3-month group and the 1-year group.
Comparison by Meniscus Injury
Between the 2 groups with and without MM injuries, there were no differences in T1rho and T2 values in the superficial layer of MFC2, MFC3, and MT3 at 3 months (
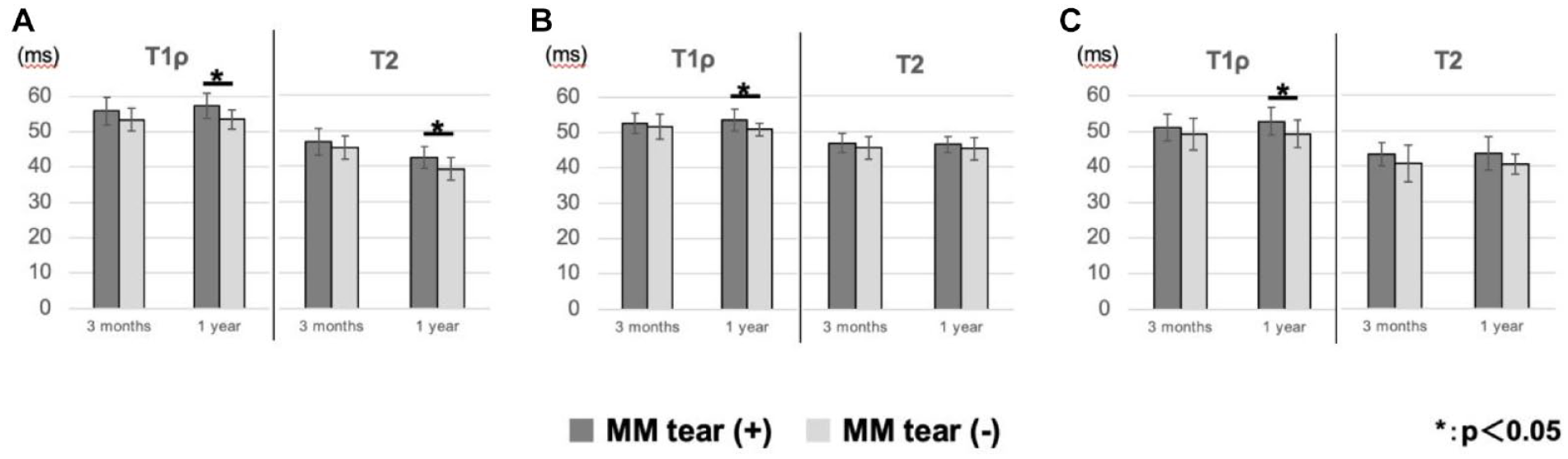
Comparison of T1rho and T2 values of MM tears. The superficial layers of (A) MFC2, (B) MFC3, and (C) MT3 revealed significant differences between values with and without MM tears.
Discussion
In this study, T1rho and T2 mapping was used to assess the state of both the superficial and deep layers of cartilage in various regions of the femur and tibia following double-bundle anatomical ACLR, resulting in 27 distinct subcompartments for the ROIs. Elevations were observed in both the medial and lateral compartments postoperatively. In the lateral compartment, cartilage damage in the posterior tibia generated at the time of injury was captured by both T1rho and T2, and these values decreased over time. In the medial compartment, degenerative changes that progressively advanced postoperatively were only detectable using T1rho, and MM injury further promoted medial cartilage degeneration.
Several studies have advocated a higher sensitivity of T1rho mapping than T2 mapping when assessing the proteoglycan composition in cartilage,27-29,49 which correlates with the early onset of OA. The need for an MR scanner equipped with specialized pulse sequences and the fact that a T1rho sequence is not yet FDA-approved limit the number of institutions capable of conducting T1rho mapping. As a result, the simultaneous utilization of both T1rho and T2 mapping has been infrequent in previous studies, particularly in longitudinal investigations, where it has become even scarcer.
When an ACL injury occurs, the posterior part of the lateral tibia (LT3 in this study) is damaged by traumatic subluxation of the knee. 50 Our study revealed that 3 months after surgery, there were significant elevations in both T1rho and T2 values for the superficial and deep layers in the LT3. However, at 1-year follow-up, the values decreased in the superficial layer in T2 but no differences were detected in T1rho. This result is in accordance with reports by Li et al., 47 indicating that the values at this site increase immediately after injury because of anterior dislocation of the tibia and at the initial giving way. Furthermore, they reported that T1rho elevation persisted in both the superficial and deep layers 1 year after surgery. According to Amano et al., 10 damage to the posterior tibial cartilage continues if postoperative tibial anterior translation and tibial internal rotation persist after ACLR, as evidenced by T1rho and T2 mapping. Similarly, Chen et al. 51 reported that when the femorotibial contact area shifted posteriorly after ACLR, the load remained at the posterior tibia and the relaxation time increased as early as 3 months postoperatively.
Data from our small cohort indicated a significant elevation of T1rho in the superficial layer of MFC2 and MT2 at 1-year follow-up. Previous reports using T1rho and T2 mapping techniques have shown that abnormal knee kinematics exist even after ACLR and that cartilage damage occurs mainly in the medial compartment.11,12 Pietrosimone et al. 52 reported that T1rho elevation appeared in the MFC loading area after ACLR when there was weakness in the quadriceps muscle, particularly in the anterior portion. Although the statistical power was not sufficient for the small sample size, our results partly proved that T1rho is more sensitive in detecting damage caused by abnormal kinematics in the medial compartment than T2.
Multiple reports have described the timing of medial cartilage degeneration after surgical intervention, ranging from 6 months to 2 years.11,12,44,53,54 In this study, no significant differences were observed in any subcompartment when comparing the 3-month and 1-year values. Su et al. 44 reported that a temporary improvement in T1rho was observed 1 year after ACLR, however, it worsened again at the 2-year follow-up. Ushio et al. 53 reported an increase in the T1rho value at the 2-year follow-up in the medial compartment after ACLR. It is possible that OA changes did not occur significantly during this short follow-up period after ACLR, and damage at the time of injury may still be predominant. Therefore, an increase in relaxation times, which could be the start of PTOA, may appear markedly in longer follow-up studies.
While the value comparison comprising individuals with and without meniscal injury did not exhibit any longitudinal variance, when comparing these two groups, it was revealed that those with meniscal injury displayed a significant increase from 3 months to 1 year in the superficial layers of MFC2, MFC3, and MT3. Furthermore, this outcome was only discernible in MFC3 and MT3 with T1rho, indicating the superiority of T1rho in detecting initial cartilage degeneration in the medial compartment.
Our study discovered that LFC5 was the only non-loading area with a significant difference compared with the control group. This non-loading area known as the “far posterior cartilage,” was previously evaluated using conventional MRI and is frequently associated with LM injury when cartilage damage coexists with ACL injury. 55 In our study, the relaxation time of LFC5 was significantly longer than that of the control group; however, there was no significant difference between the groups with and without LM injury.
Studies have reported a 32%–72% rate of LM tears in knees with ACL injuries.56-58 As the menisci function as secondary knee stabilizers, LM tears contribute to increased tibial rotational and anterior instability during knee flexion. 59 Reports indicate that residual tibial internal rotation affects the cartilage in the posterior LFC and that T1rho and T2 values increase. 10 Therefore, the presence of such an LM injury and residual abnormal tibial position may have influenced the cartilage damage in the LFC5.
MT1 relaxation times for both T1rho and T2 were significantly elevated compared with those of the controls at 3 months and although the value decreased, the significance stayed at 1 year follow-up. As the trans-portal technique was used in our ACLRs, the effect of manipulation may be present via the far anteromedial portal (FAM portal; made just above the superior border between the anterior portion of MM and capsule and is adjacent to anterior cartilage of medial tibia) on MT1 cartilages. No previous studies on value elevation in this area have been reported.
Regarding the hypothesis of this study, it was demonstrated that both T1rho and T2 could effectively capture damage in the lateral compartment resulting from the initial injury, as evidenced by the significant difference between the 3-month and control groups. About damage in the medial compartment postsurgery, which is believed to be primarily caused by abnormal kinematics, the T1rho values in the superficial layer of MFC2 and MT2 longitudinally increased from 3 months to 1 year and showed a significant difference from those in the control groups. This result suggests that the T1rho value is an effective indicator of medial cartilage degeneration. However, as no significant difference was observed in the direct comparison between the 3-month and 1-year groups, a longitudinal study is essential to demonstrate the superiority of T1rho over T2 in capturing postoperative cartilage degeneration in the medial compartment.
To the best of our knowledge, this is the first study to investigate the knee articular cartilage after double-bundle anatomical ACLR using T1rho and T2 mapping. Several studies, such as Pedoia et al., 60 have assessed the post-ACLR knee using T1rho and T2 mapping. However, these studies have utilized the single-bundle technique. The findings of their studies and those of this study exhibit similarities: both show improvement in observed damage in the posterior part of the lateral tibia over time postoperatively, while cartilage degeneration progresses over time in the medial compartment. A distinctive finding of the double-bundle ACLR in our investigation was the observed degeneration of cartilage in the anterior region of the medial tibia, which was not reported by previous studies. This finding was possibly attributable to the surgical methodology through the FAM portal; however, this assertion necessitates validation through subsequent research. As reported by Zhou et al. 61 in their meta-analysis, the double bundle technique exhibits no superiority over the single-bundle technique in preventing the progression of radiographic OA. The results of our study partially support this observation. Contrary to our expectations, the cartilage findings on MRI did not suggest that double-bundle ACLR was superior to the single-bundle technique.
This study has some limitations. First, this was a retrospective study, with a potential selection bias. A prospective, large-scale study with sufficient statistical power is needed to confirm the findings of this study. Second, the sample size was small and the follow-up period was short. As no significant difference was observed in the direct comparison between the 3-month and 1-year groups, changes in the extracellular matrix generated in such a short period may have been difficult to detect. Third, data from the contralateral uninjured knee in the ACLR patient group were not available. Physiologic variations in healthy volunteers as a control group may have influenced the range of values in relaxation times 62 . Fourth, the patient group only included those who underwent surgery. It would have been more beneficial to investigate a group of patients with ACL injuries who did not undergo surgery as a second control. Accumulating more data for future comparisons with the conservative treatment group would be ideal. Last, the evaluation of cartilage was solely conducted using MRI images. Although minimal morphological changes in cartilage were observed during the early postoperative period on MRI, arthroscopic examination could have revealed surface damage or softening of the cartilage. Correlating arthroscopic findings with qMRI values could provide greater insight into comparing the sensitivity of T1rho and T2 and elucidating longitudinal value changes.
Conclusion
In this study, cartilage degeneration has been documented to persist after ACLR. Double-bundle ACLR typically exhibits characteristics of cartilage degeneration similar to those observed with single-bundle ACLR. However, the degeneration observed in the anterior region of the medial tibia may be specific to the double-bundle technique, necessitating additional investigation. Both T1rho and T2 mapping has demonstrated efficacy in evaluating cartilage degeneration in ACL-reconstructed knees. Although evidence suggests that T1rho mapping may possess greater sensitivity in detecting cartilage degeneration, specifically within the medial compartment, following ACLR, we were unable to establish the superiority of T1rho over T2 mapping in this longitudinal study. Therefore, subsequent investigations involving extensive longitudinal data from multiple centers are necessary to further evaluate the characteristics of PTOA and to scrutinize the reliability, sensitivity, and specificity of qMRI. In addition, comparing the characteristics of cartilage degeneration between different surgical techniques using qMRI will contribute to the improvement of surgical procedures and postoperative outcomes.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The research protocol for this study was approved by the Chiba University Graduate School of Medicine (M10562) and Teikyo University Chiba Medical Center (11-35) institutional ethics review board for Human Research.