
Abstract
Objective
The use of synthetic bone substitute material (BSM) as osteotomy gap fillers have been reported to improve outcomes in medial opening wedge high tibial osteotomy (MOWHTO). This study aims to evaluate the early radiological outcomes (bone union) and complication rates of the novel patient-specific 3D-printed honeycomb-structured polycaprolactone and tricalcium phosphate (PCL-TCP) synthetic graft compared to allogeneic bone grafts as an osteotomy gap filler in MOWHTO.
Methods
A retrospective matched-pair analysis of patients who underwent MOWHTO with either PCL-TCP synthetic graft or allogenic femoral head allograft as osteotomy gap filler was performed. The osteotomy gap was split into equal zones (Zone 1-5), and bone union was evaluated on anteroposterior radiographs based on the van Hemert classification at 1, 3, 6, and 12 months postoperatively. Postoperative complications including infection, lateral hinge fractures, and persistent pain was measured. The study and control group were matched for age, smoking status, diabetes mellitus, and osteotomy gap size.
Results
Significantly greater bone union progression was observed in the PCL-TCP group than in the allograft group at 1 month (Zones 1-3), 3 months (Zones 1-4), 6 months (Zones 1-2, 4), and 12 months (Zones 2-3, 5) postoperatively (P < 0.05). No significant difference in complications rates was noted between the two groups at 1 year.
Conclusions
Bone union rates observed in patients who underwent MOWHTO with the PCL-TCP synthetic graft osteotomy gap filler were superior to those in the allograft group at 1 year postoperatively, with no significant difference in complication rates (postoperative infection, lateral hinge fractures, and persistent pain).
Keywords
Introduction
Knee osteoarthritis is the most common joint degenerative disease affecting about 10% of men and 13% of women above the age of 60.1,2 Knee osteoarthritis is the top cause of chronic disability among the elderly, commonly associated with varus knee malalignment.3,4 Varus deformity of the knee causes increased loads to be transmitted through the knee medial compartment resulting in cartilage degeneration. 3 High tibial osteotomy (HTO) is a well-established surgical treatment option for medial compartment knee osteoarthritis especially among younger, more active patients with tibial vara deformity. 5 The medial opening wedge HTO (MOWHTO) procedure performed in the treatment of these patients involves the creation of a wedge-shaped defect during the opening of the osteotomy space, which could be filled with either a bone graft or bone substitute material (BSM) or left to heal on its own. 6 Common complications of MOWHTO involves non-union and delayed bone healing of the osteotomy site, along with the loss of correction and lateral hinge fractures. 7
The use of an osteotomy gap filler has been reported in recent literature to improve stability, postoperative pain, and rehabilitation outcomes after MOWHTO.8,9 Furthermore, osteotomy gap fillers have been proposed to reduce blood loss by acting as a tamponade within osteotomy gaps and serving as a vessel for potential therapeutics such as antibiotics to improve patient outcomes.10,11 However, to date, there is still no consensus on the necessity and type of osteotomy gap filler which produces the best outcomes for patients.12,13 Historically, the autograft osteotomy gap filler has been used to achieve bone union at the osteotomy gap site for its osteogenic, osteoinductive, and osteoconductive properties. 14 However, donor-site morbidity and increased operative time, pain, and blood loss have been cited as significant drawbacks associated with the autologous bone graft.15,16 On the other hand, while the use of allogenic bone grafts has reported good short-term outcomes with a reduction of complications associated with autograft bone grafts, its associated high storage costs and increased risk of disease transmission, delayed union, and immune reactions have been cited as reasons against their use.8,13,17 To overcome the mentioned drawbacks of an autologous and allogeneic bone graft such as its associated donor site morbidity, high costs, and risk of adverse immune reaction or infection rates, recent literature has also explored the use of BSM involving synthetic materials such as β-tricalcium phosphate (TCP), hydroxyapatite, and calcium sulfate as osteotomy gap fillers with equivocal outcomes in terms of its complication rates. 10
The rapidly growing field of additive manufacturing (3D-printing) have led to the development of scaffold-based engineered tissue as an alternative method of filling bone defects. 18 Specifically, the use of 3D-printed bioresorbable honeycomb-structured synthetic grafts made of polycaprolactone and tricalcium phosphate (PCL-TCP) to guide bone regeneration in bone defects has demonstrated promising results in both large-scale pre-clinical studies and clinical outcomes studies, showing good biomechanical strength, osteoconduction, biocompatibility, and clinical evidence of bone regeneration with minimal reported complications.19,20 More recently, Henkel et al. 21 and Laubach et al. 22 reported promising cases of successful PCL-TCP scaffold guided bone regeneration in patients with large-volume long bone defects. Nonetheless, the clinical outcomes and complications of using a 3D-printed bioresorbable PCL-TCP synthetic graft as an osteotomy gap filler in MOWHTO have yet to be reported. The aim of this study was to evaluate the early radiological outcomes (bone union) and complication rates of 3D-printed bioresorbable PCL-TCP synthetic graft compared to allogeneic bone grafts as an osteotomy gap filler in MOWHTO at 1, 3, 6, and 12 months. The authors hypothesize that bone union and complication rates following the use of a 3D-printed PCL-TCP synthetic graft osteotomy gap filler are comparable to those of allogenic bone grafts.
Methods
A retrospective matched-pair analysis of patients who underwent MOWHTO with either 3D-printed PCL-TCP synthetic graft or allogenic femoral head allograft as an osteotomy gap filler was conducted. All patients had symptomatic medial compartment knee osteoarthritis with varus deformity and have failed a course of conservative treatment. All patients underwent MOWHTO performed by senior fellowship-trained surgeons (H.R.B.A.R and K.H.L). All patients who underwent MOWHTO with either 3D-printed bioresorbable PCL-TCP synthetic grafts or allogenic bone graft as the osteotomy bone gap filler were included. Patients who had inflammatory arthritis, lateral knee osteoarthritis, concurrent bilateral MOWHTO performed, or MOWHTO necessitating simultaneous ligament reconstruction or meniscal repair were excluded.
The study population comprised two groups of patients divided based on the type of osteotomy bone gap filler used. The study group consisted of 28 patients with the PCL-TCP synthetic graft (Osteopore, Singapore), and the control group had 28 patients with a femoral head allograft as the osteotomy gap filler. The study and control groups were matched for the following factors that affect bone healing, namely age, smoking status, presence of diabetes mellitus (DM), and the osteotomy gap size.
The 3D-printed PCL-TCP synthetic graft is made of a composite scaffold made of PCL-TCP (80:20%) with an interconnected honeycomb structure with a pore size of 350-500 um, 70% porosity, and 100% pore interconnectivity. The synthetic graft as well as the femoral head allograft were fashioned based on preoperative measurements (posterior wedge height, anterior wedge height, wedge angle, wedge width, and wedge length) obtained from an orthopedic templating software (TraumaCad; Brainlab, Munich, Germany) (
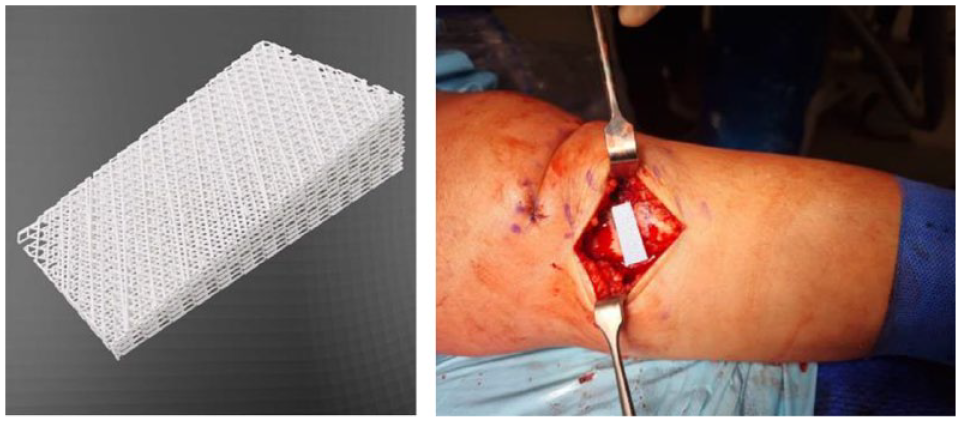
Three-dimensional reconstructions of the PCL-TCP scaffold (Osteopore International, Singapore) and intraoperative image of the PCL-TCP osteotomy gap filler.
Radiographic Assessment and Outcomes
Weight-bearing knee and long lower-limb radiographs for both the anteroposterior and lateral views were obtained preoperatively and postoperatively at 1, 3, 6, and 12 months.
Bone union was evaluated on anteroposterior and lateral radiographs at 1, 3, 6, and 12 months after MOWHTO. For the anteroposterior radiographs, the area of osteotomy gap was divided into five zones in line with the radiographical osteotomy filling index described by Brosset et al. for assessment of bone union. The five zones were numbered from Zone 1 to Zone 5, with Zone 1 beginning from the lateral tibial cortex (
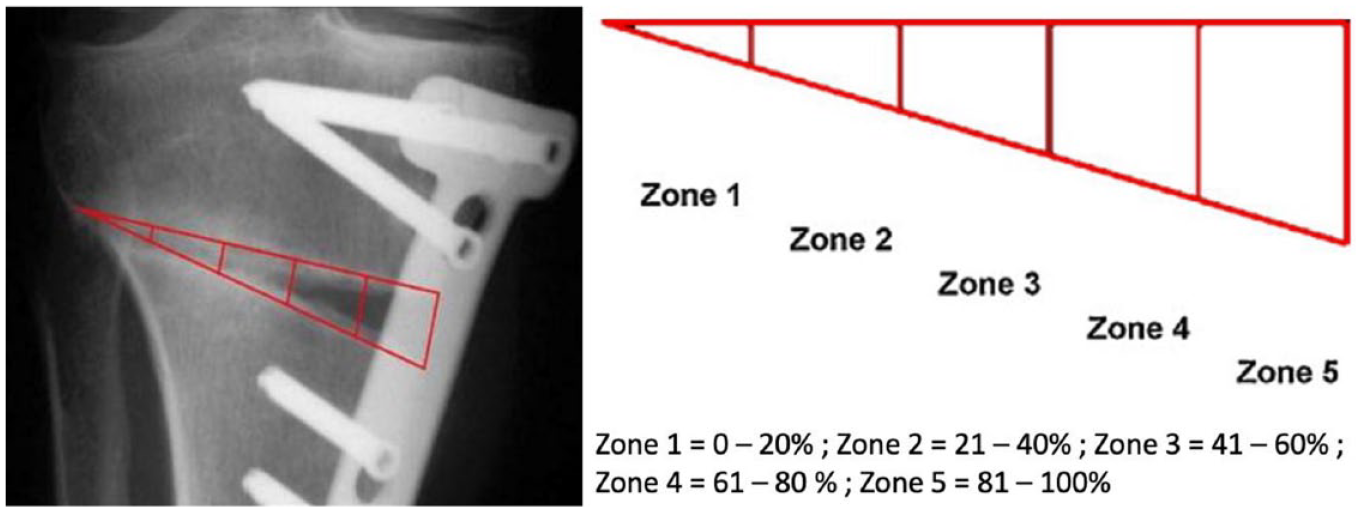
Zone distribution of osteotomy gap as described by Brosset et al. 23
Progress of bone union or phase of bone remodeling was assessed using the radiographic classification system for osteotomy gap fillers proposed by van Hemert et al. 24 which comprises of six phases: phase 0 = direct postoperative; phase 1 = vascular phase; phase 2 = calcification phase; phase 3 = osteoblastic phase; phase 4 = consolidation phase; phase 5 = full reformation ( Table 1 ). The five zones on anteroposterior radiographs were assigned a phase of bone remodeling based on van Hemert et al. 24 at each time point to assess bone union.
Bone Union Criteria by van Hemert et al. 24
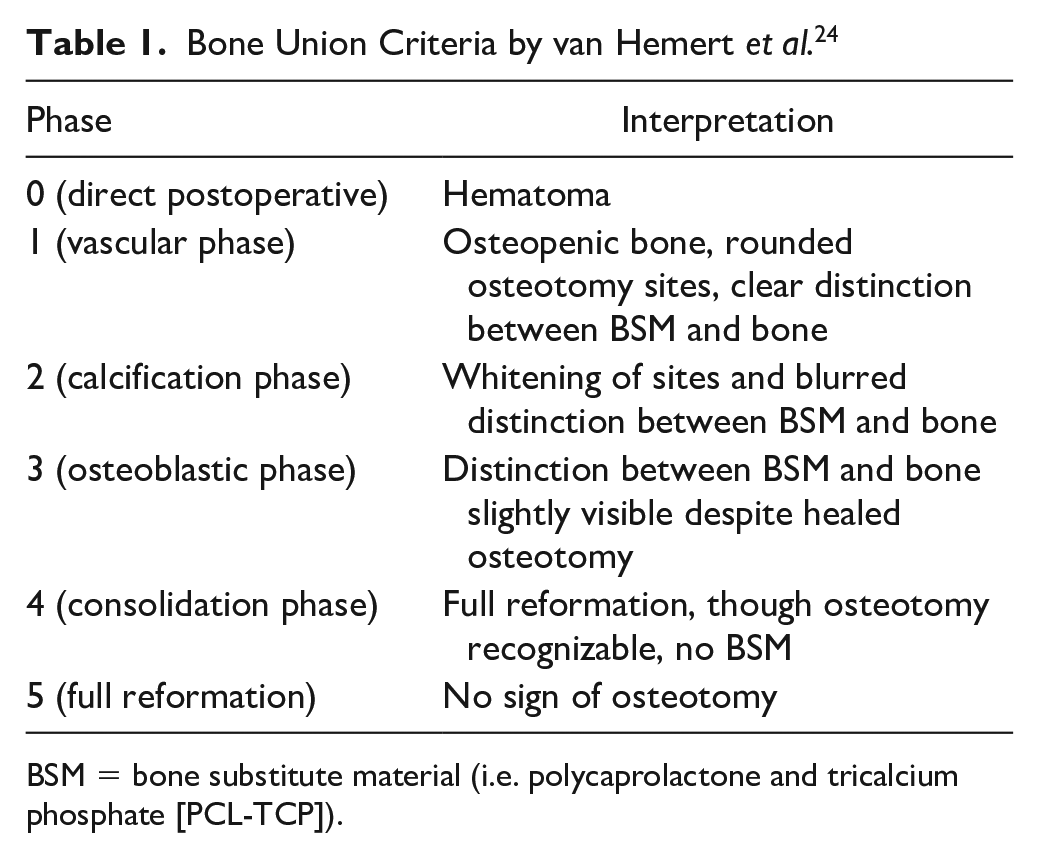
BSM = bone substitute material (i.e. polycaprolactone and tricalcium phosphate [PCL-TCP]).
In addition, patients were also monitored for other non-radiographic postoperative complications including superficial or deep wound infection, lateral hinge fractures, and persistent postoperative pain postoperatively.
Surgical Technique and Postoperative Rehabilitation
The surgical technique for MOWHTO was performed using the technique described by Khakha et al. 25
The operation begins at the medial proximal tibia with a longitudinal incision performed over the pes anserinus. The distal attachment of the anterior superficial medical collateral ligament and pes anserinus released subsequently. Two breakable wires (Arthrex, Naples, FL) were introduced under fluoroscopy guidance to define the osteotomy plane. The lateral hinge was next reinforced with a temporary 1.7-mm K wire drilled from the lateral tibial plateau edge into the intramedullary canal. A biplane osteotomy cut using a precision saw (System 8 Precision; Stryker, Kalamazoo, MI) was performed and with the breakable wires subsequently removed. Sequential distraction of the osteotomy gap using osteotomes was performed to a desired opening size. A metal wedge spacer corresponding to the desired opening size was used to achieve the preplanned correction, with the mechanical axis checked under fluoroscopy to ensure satisfactory alignment. The prefabricated PCL-TCP synthetic graft wedge was press-fitted into the created osteotomy gap, followed by a repeat assessment of the mechanical axis under fluoroscopy for satisfactory alignment. The final construct was secured using HTO locking screws and plate followed up soft-tissue closure.
For the allograft group, a similar surgical technique was performed to plan and create the osteotomy gap. Preoperative planning was done to determine the dimensions of the trapezoidal shaped allograft bone grafts based on principles described by Ruzbasky et al. 26 and Noyes et al. 27 The femoral head allograft was then cut and shaped to the predetermined osteotomy wedge with the aid of a clamp and oscillating saw. The prepared allograft wedge was then press fitted into the osteotomy gap and similarly secured with HTO locking screws and plate with tissue closure subsequently.
Postoperatively, patients were allowed to partially weight bear as tolerated for 4 weeks postoperatively and full weight bearing subsequently. The patients underwent a standardized rehabilitation program with physiotherapists, consisting of graduated exercises from passive and active range-of-motion exercises to full ambulation.
Statistical Analysis
All data analyses were performed using Statistical Analysis System (SAS) (SAS Institute, Cary, NC). Matched-pair analysis was performed to compare the PCL-TCP and allograft groups using the Student’s independent t-test for continuous variables (e.g. age, body mass index [BMI], and clinical outcomes) and Pearson’s chi-square test for categorical variables (e.g. bony union, wound infection, hinge fractures). Linear-by-linear association test was used to evaluate and compare bone union between both groups. Statistical significance was denoted as P < 0.05.
Results
Patient Demographics
There were no significant differences in the preoperative baseline demographics between the PCL-TCP and allograft groups. Patient from the PCL-TCP and allograft groups were matched for age, smoking status, presence of DM, and the osteotomy gap size. The mean age for the PCL-TCP and allograft group were 52.4 ± 9.3 and 53.5 ± 7.2 years, respectively, with a mean opening gap size of 9.1 mm for both the PCL-TCP and allograft groups ( Table 2 ).
Patient Preoperative and Postoperative Baseline Demographic Data.
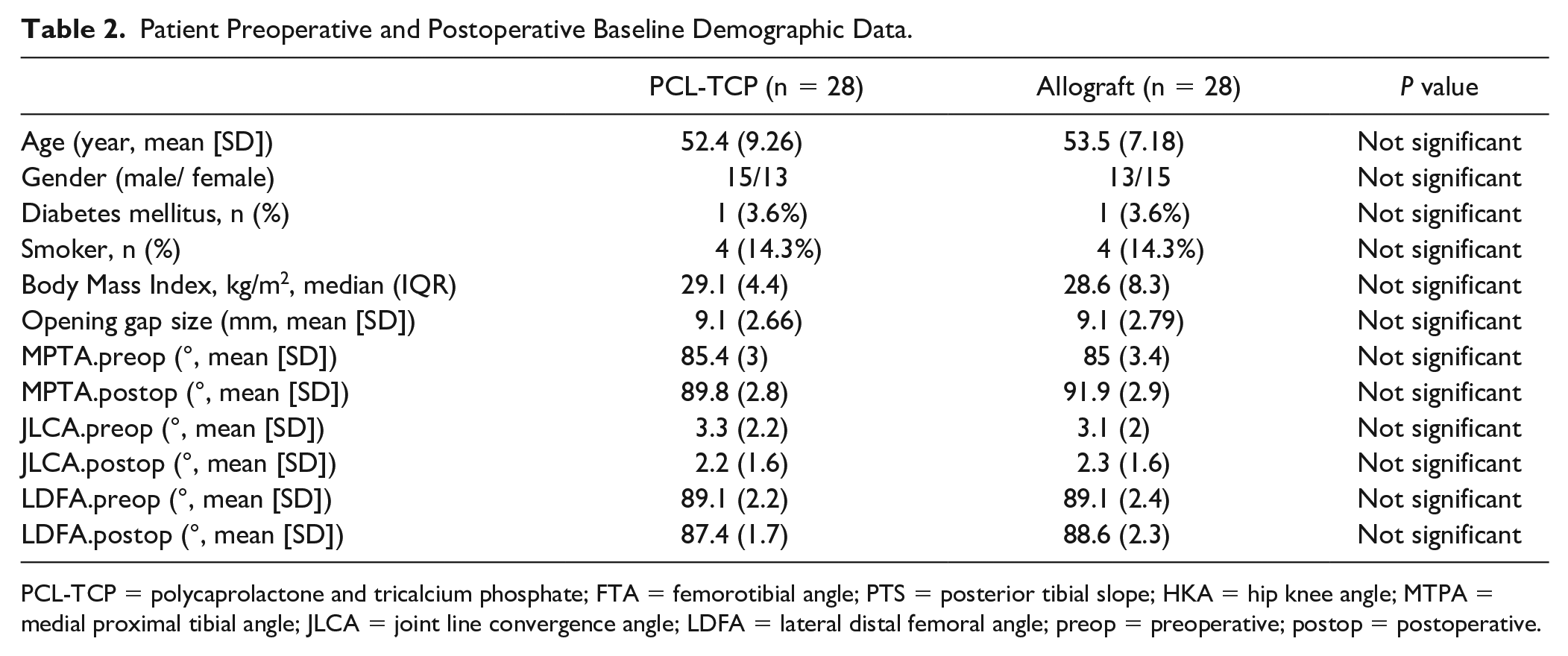
PCL-TCP = polycaprolactone and tricalcium phosphate; FTA = femorotibial angle; PTS = posterior tibial slope; HKA = hip knee angle; MTPA = medial proximal tibial angle; JLCA = joint line convergence angle; LDFA = lateral distal femoral angle; preop = preoperative; postop = postoperative.
Bone Union
Significantly greater bone union progression was observed in the PCL-TCP group than in the allograft group at 1 month (for Zones 1-3), 3 months (for Zones 1-4), 6 months (for Zones 1-2, 4), and 12 months (for Zones 2-3, 5) postoperatively (P < 0.005), as detailed in
Bone Union at 1 Month for PCL-TCP and Allograft Osteotomy Gap Fillers Using the van Hemert et al. 24 Scale.
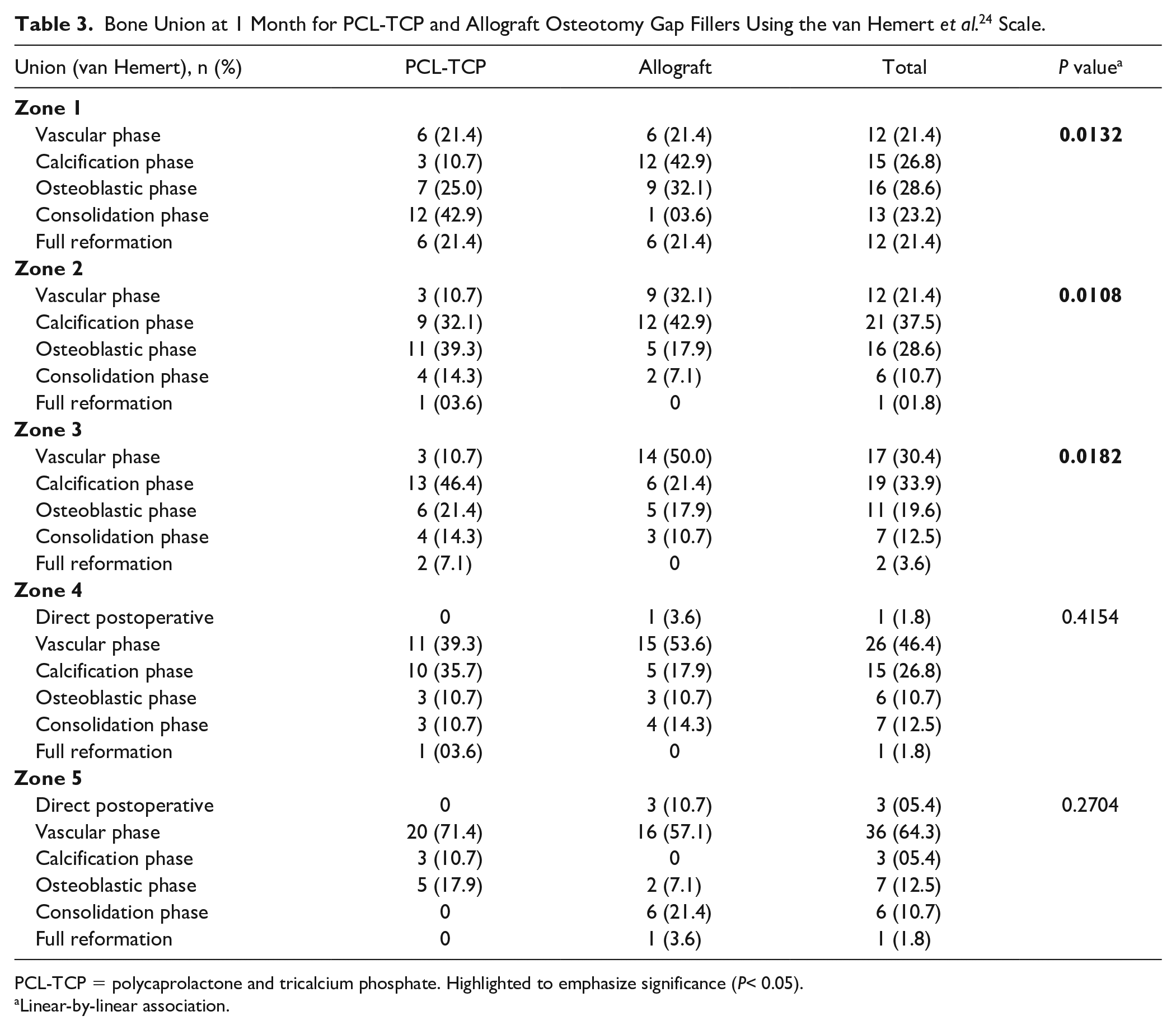
PCL-TCP = polycaprolactone and tricalcium phosphate. Highlighted to emphasize significance (P< 0.05).
Linear-by-linear association.
Bone Union at 3 Months for PCL-TCP and Allograft Osteotomy Gap Fillers Using the van Hemert et al. 24 Scale.
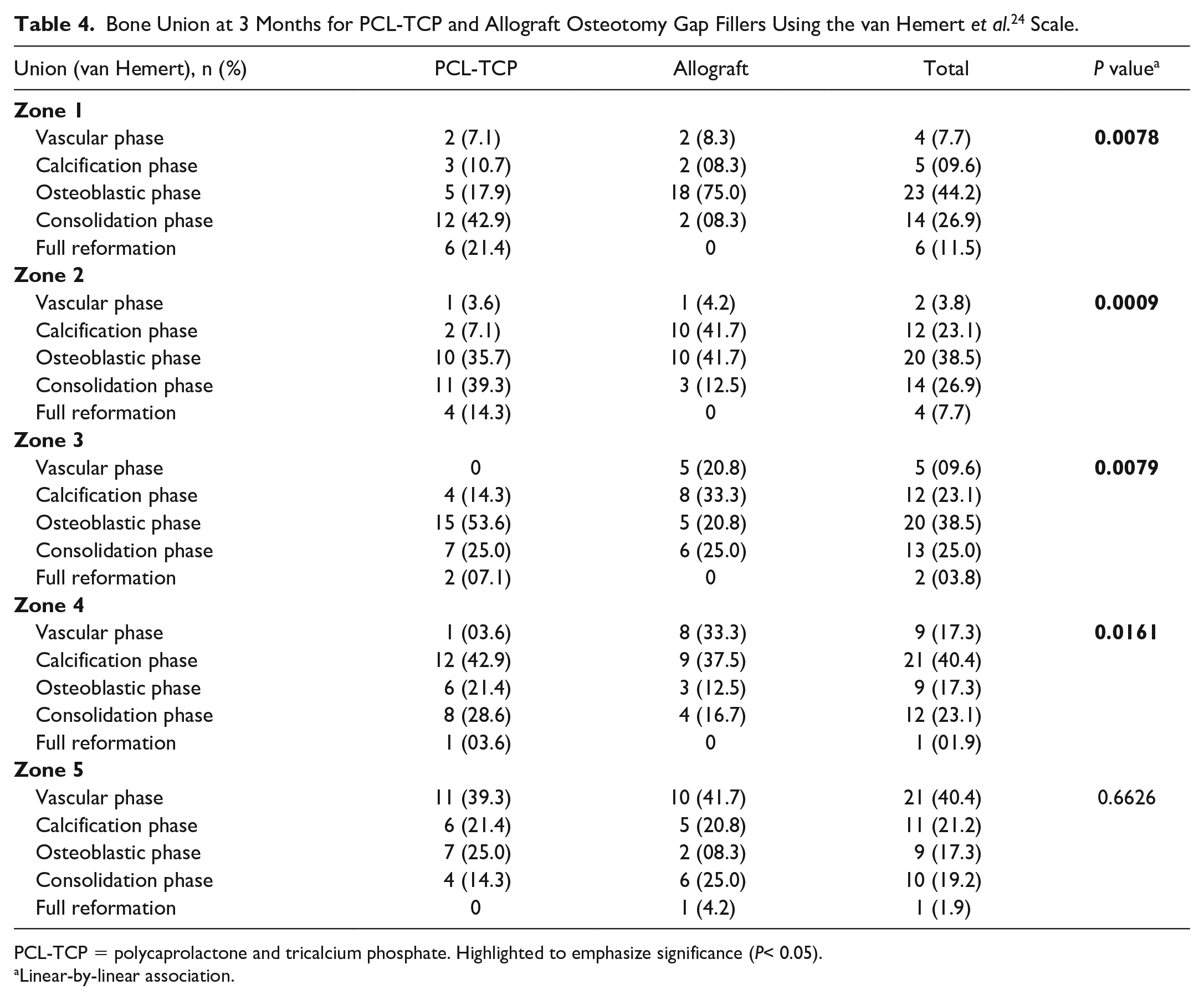
PCL-TCP = polycaprolactone and tricalcium phosphate. Highlighted to emphasize significance (P< 0.05).
Linear-by-linear association.
Bone Union at 6 Months for PCL-TCP and Allograft Osteotomy Gap Fillers Using the van Hemert et al. 24 Scale.
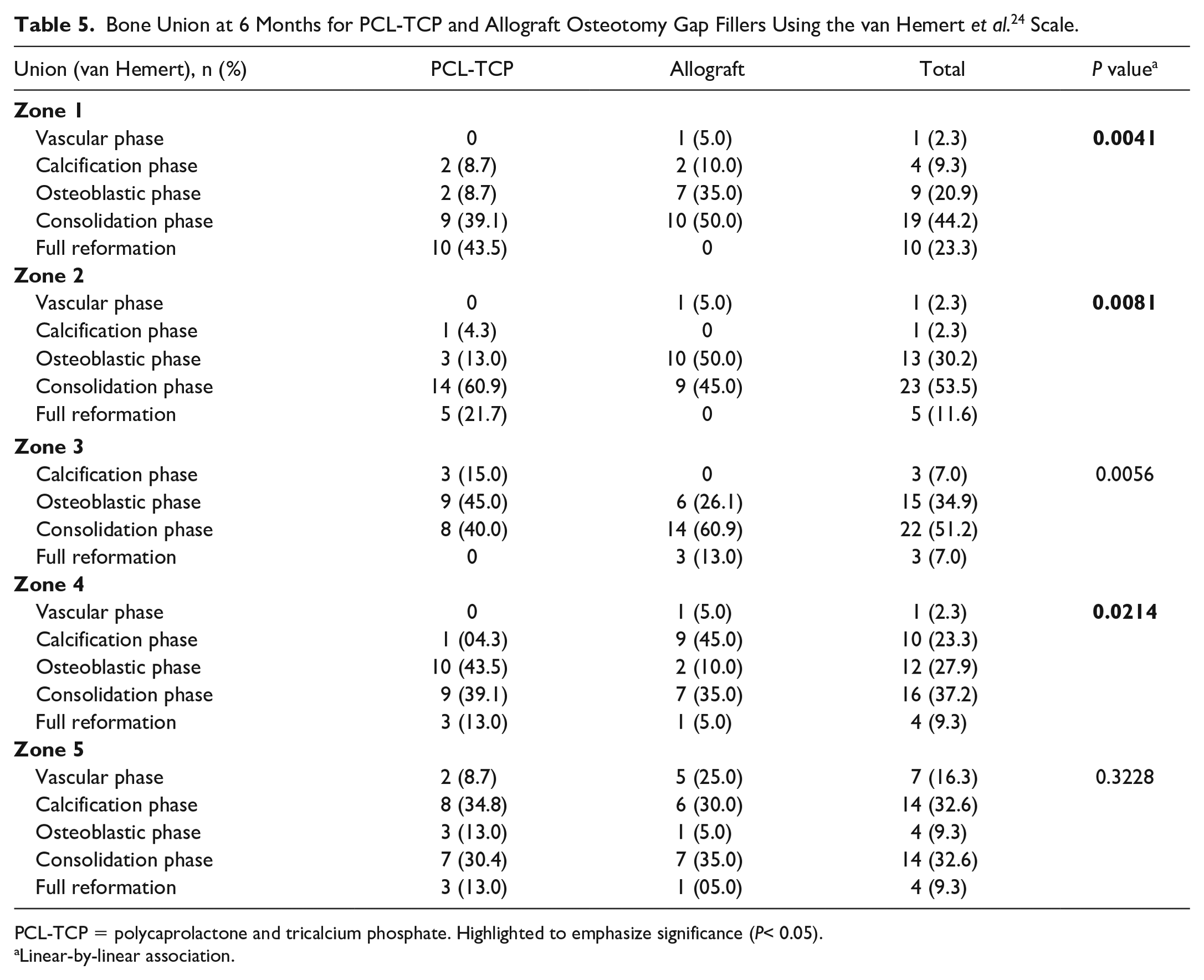
PCL-TCP = polycaprolactone and tricalcium phosphate. Highlighted to emphasize significance (P< 0.05).
Linear-by-linear association.
Bone Union at 12 Months for PCL-TCP and Allograft Osteotomy Gap Fillers Using the van Hemert et al. 24 Scale.
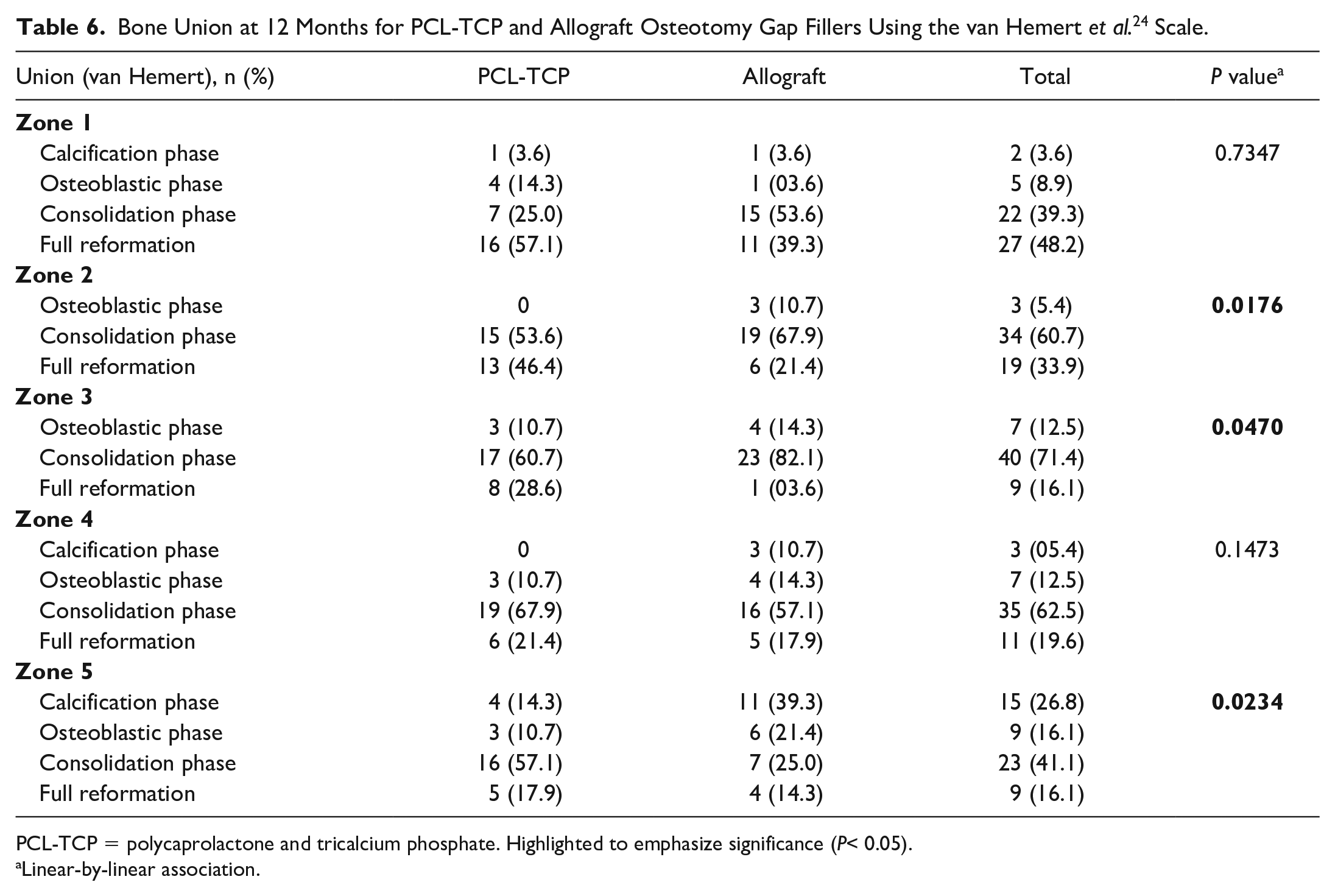
PCL-TCP = polycaprolactone and tricalcium phosphate. Highlighted to emphasize significance (P< 0.05).
Linear-by-linear association.
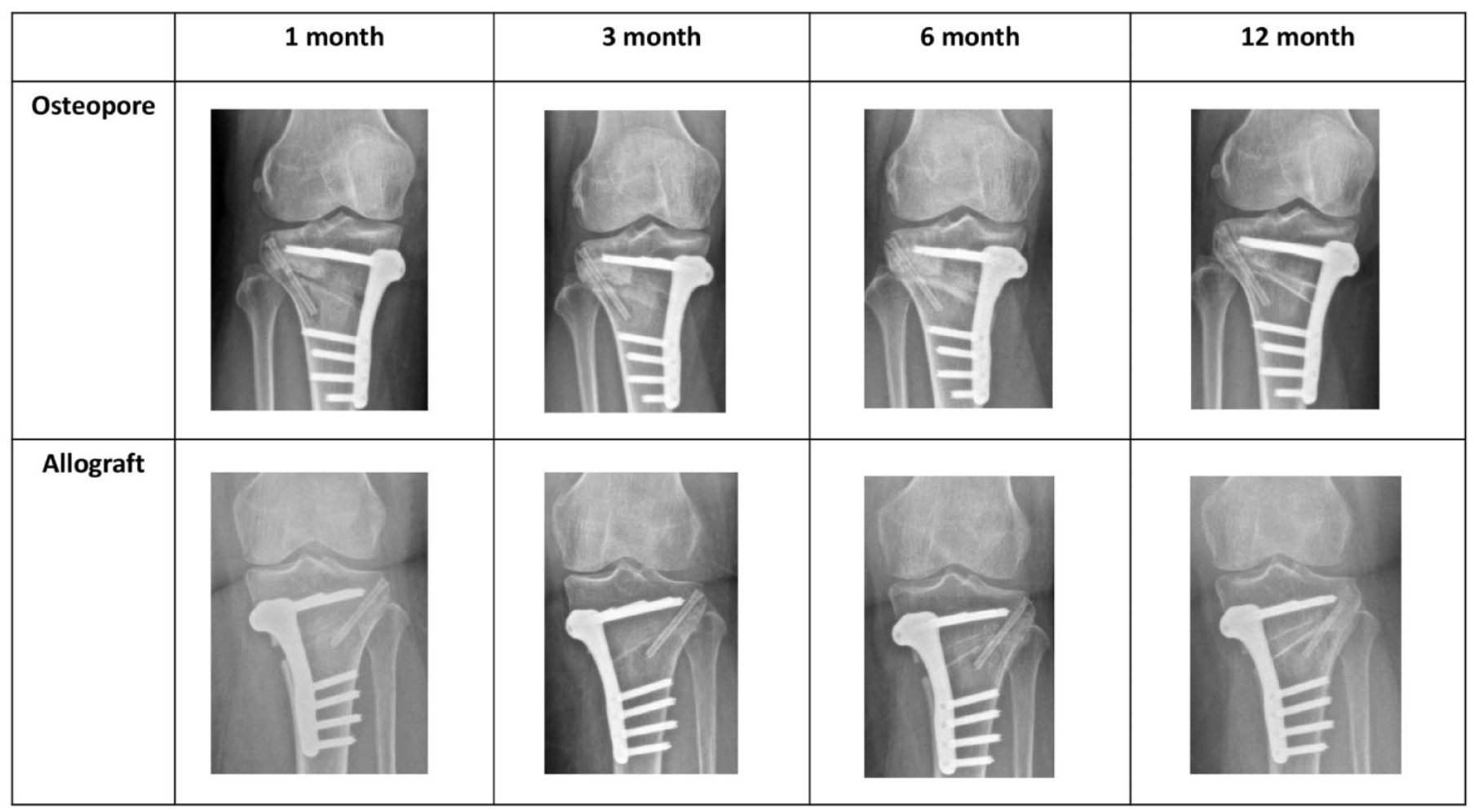
Comparison of radiographs of osteopore and allograft groups at 1, 3, 6, and 12 months postoperatively.
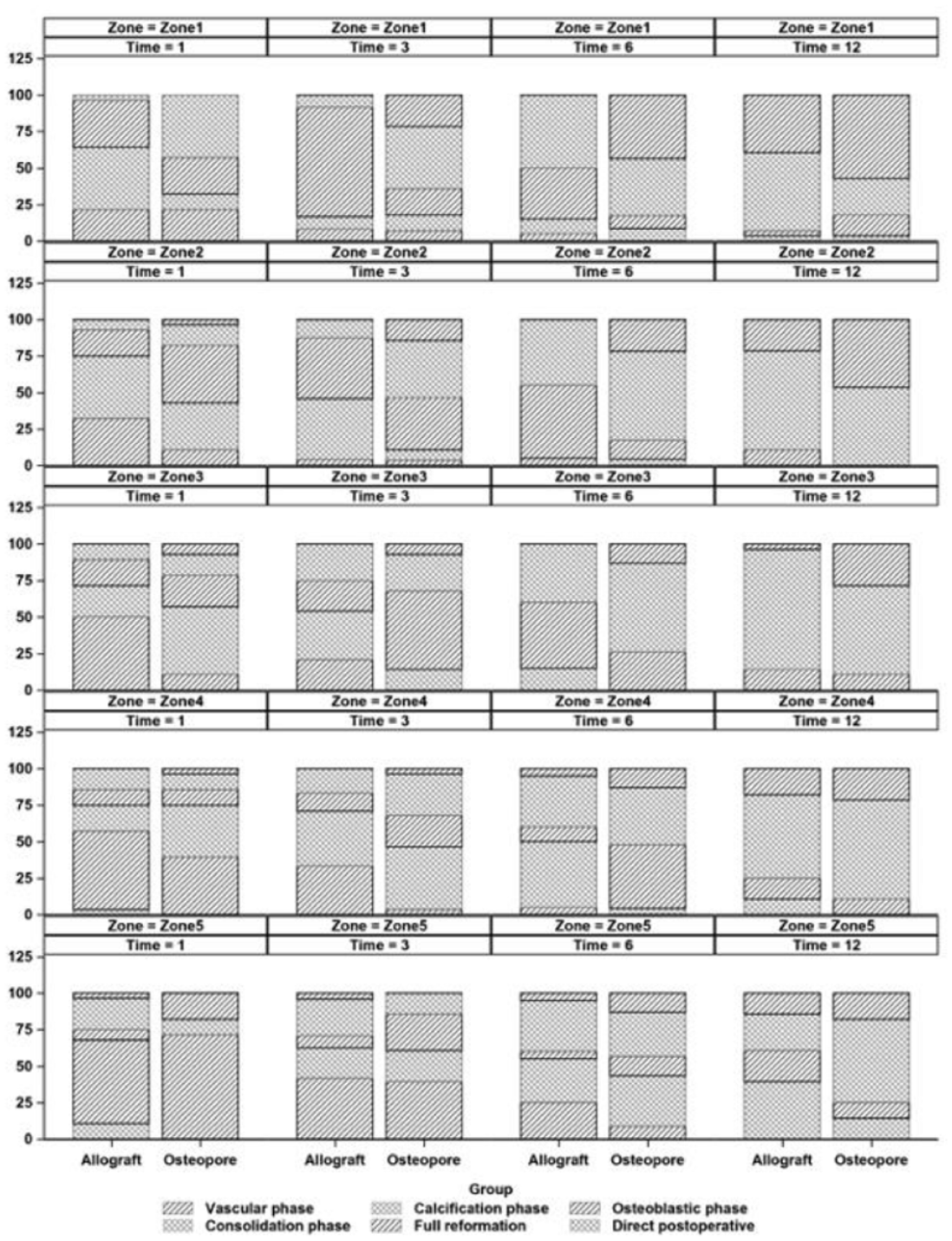
Bone union progression evaluated based on bone union criteria by van Hemert et al. 24
Bone Union of Posterior Tibial Cortex at 1, 3, 6, and 12 Months for PCL-TCP and Allograft Osteotomy Gap Fillers.
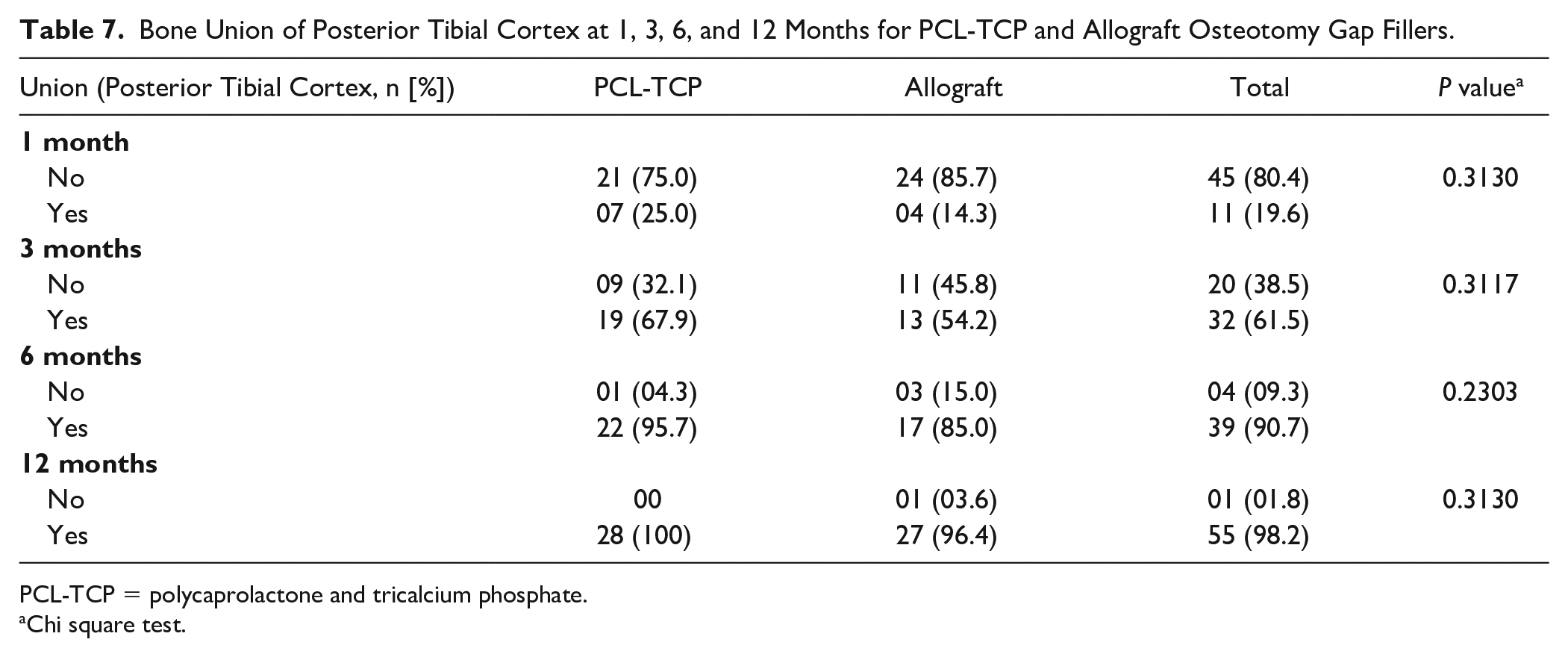
PCL-TCP = polycaprolactone and tricalcium phosphate.
Chi square test.
Complications
The PCL-TCP group reported a case of lateral hinge fracture while the allograft group reported 2 cases of lateral hinge fractures. The PCL-TCP and allograft groups both reported a case each of infection postoperatively (P > 0.05). The allograft group reported 6 cases of persistent pain postoperatively compared to the PCL-TCP group with only 3 cases (P > 0.05) ( Table 8 ).
Complications (Infection, Lateral Hinge Fracture, Persistent Pain) of PCL-TCP and Allograft Osteotomy Gap Fillers Over 12 Months.
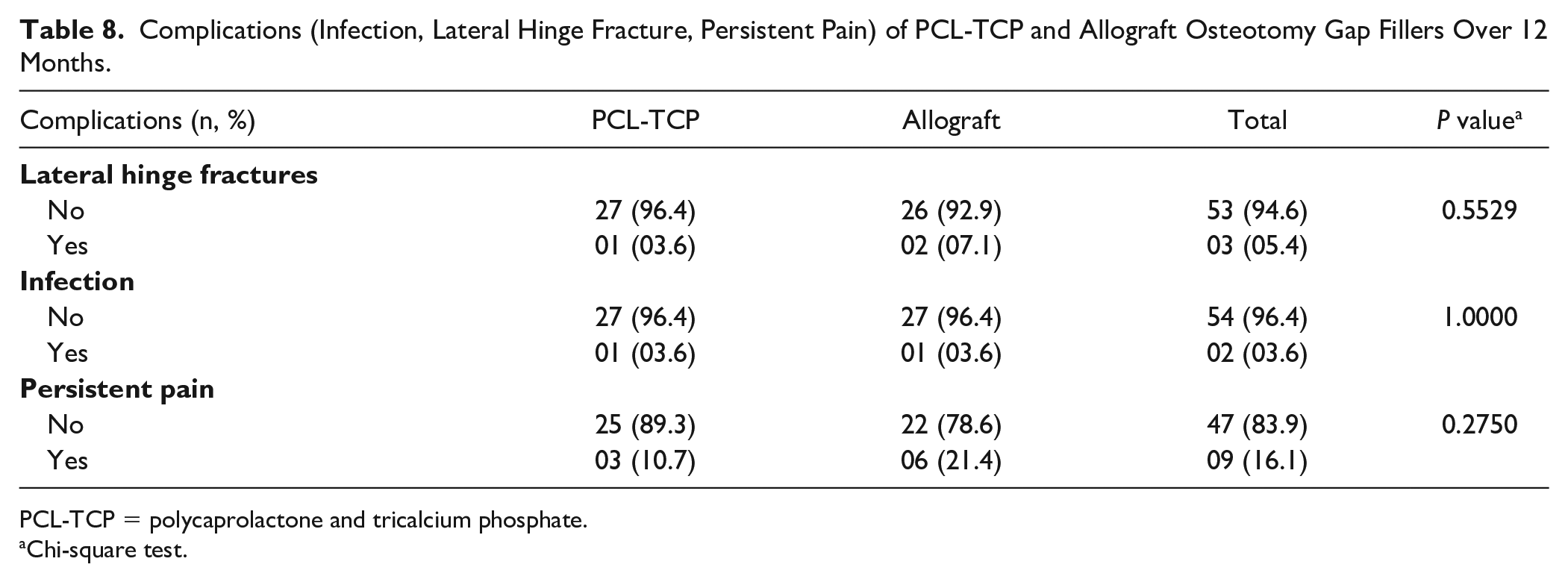
PCL-TCP = polycaprolactone and tricalcium phosphate.
Chi-square test.
Discussion
This was the first study reporting the use of a patient-specific 3D-printed PCL-TCP synthetic graft as an osteotomy gap filler in MOWHTO. Our study aimed to evaluate the early radiological outcomes in terms of bone union and complication rates of patient-specific 3D-printed PCL-TCP scaffold implants compared to allogeneic bone grafts as an osteotomy gap filler in MOWHTO. Our key findings show that greater rate of bone union was achieved for the PCL-TCP group compared to the allograft group during the 1-year follow-up period, with a more advanced phase of bone union noted on plain radiographs at the 1-month, 3-month, 6-month and 12-month follow-ups postoperatively for the PCL-TCP group. Furthermore, it was noted that while the allograft group reported a greater number of cases with lateral hinge fractures and persistent pain, complication rates between both groups were comparable.
A meta-analysis by Han et al.
13
done in 2015 found no significant difference in radiological outcomes of MOWHTO with or without osteotomy gap fillers. However, more recent literature has reported greater construct stability in MOWHTO with osteotomy gap fillers, with low postoperative pain allowing for earlier rehabilitation in MOWHTO.8,9 Furthermore, osteotomy gap fillers have the added benefit of serving as vessels for potential therapeutics such as antibiotics and reducing blood loss by acting as a tamponade within osteotomy gaps in improving postoperative outcomes.10,11 Within the realm of osteotomy gap fillers, autografts have been traditionally identified as the gold standard for its osteogenic, osteoinductive, and osteoconductive properties, but not commonly used due to its associated significant donor-site morbidity and postoperative pain and blood loss.14-16 On the other hand, allografts are associated with problems such as limited supplies, storage cost, risk of disease transamination from donor to hosts, and immune reactions that could result in delayed union.8,13,17 Synthetics or BSMs such as TCP, hydroxyapatite, and calcium sulfate have come into the picture in recent years to fill the “gap” of osteotomy fillers.
10
More recently, PCL has been tested as another alternative BSM with good biocompatibility and reduced rate of degradation.
28
However, to complement for its lack of osteogenic potential for bone regeneration and significant prolonged degradation time of as long as 3 years for complete degradation, TCP was integrated with PCL to create the PCL-TCP material as used in our study.
29
Since its induction, the 3D-printed PCL-TCP scaffold implants have been used as an adjunct to guide bone regeneration in bone defects for which it has demonstrated promising results in both large-scale preclinical studies and clinical outcomes studies, showing good biomechanical strength, osteoconduction, biocompatibility, and clinical evidence of bone regeneration with minimal reported complications.19,20 Our study results serve as a testament to the potential application of PCL-TCP as a viable osteotomy gap filler in achieving superior rate of bone union of osteotomy gaps. Computed tomography (CT) imaging done for 2 patients at 6 and 12 months postoperatively further displays cancellous bone restoration with neo-cortex formation and full integration at 300 Houndsfield units (HU), similar to that of native cancellous bone (
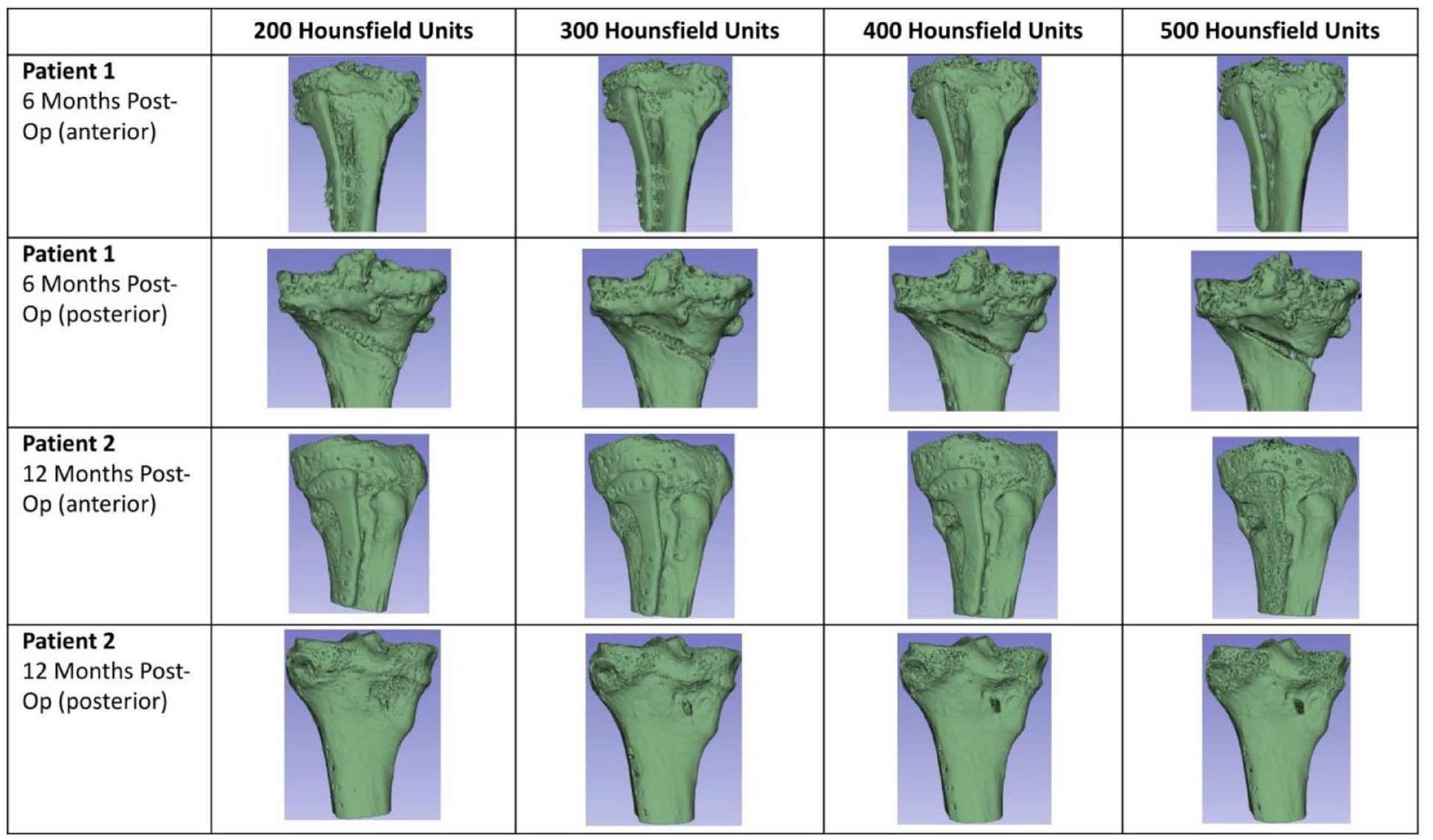
Postoperative computed tomography (CT) images of 2 patients at 6 and 12 months demonstrating cancellous bone restoration with neo-cortex formation and full integration at 300 Houndsfield units (HU), similar to that of native cancellous bone.
A few factors may be involved in promoting bone union with the PCL-TCP implant in osteotomy gaps. First, as mentioned earlier, the biocompatibility and osteoconductive properties of PCL-TCP serve as a good medium for bone regeneration to occur in osteotomy gaps.19,20 Second, the honeycomb structure used in the design of the PCL-TCP scaffold implants has been shown to be an effective geometric structure that mimics the natural construct of bone in terms of porosity and equilateral equidistant triangles.30-35 The honeycomb microstructure hence serves as a potential conduit for favorable bone tissue regeneration and healing to occur, as also described by Henkel et al. 21 and Laubach et al. 22 with promising cases of successful PCL-TCP scaffold-guided bone regeneration in patients with large-volume long bone defects. On the other hand, allografts may have a stronger allogeneic response that could delay bone union especially at the early stages postoperatively. 36
Alongside early available evidence, our study has demonstrated promising results of the 3D-printed honeycomb-structured PCL-TCP scaffold implant as an osteotomy gap filler in promoting osteotomy gap bone union with minimal reported complications. Furthermore, the honeycomb-structured PCL-TCP implant serves as a viable medium for various additives such as mesenchymal stem cells and bone marrow aspirates which have been shown to further aid bony regeneration and improve postoperative outcomes in HTOs.37,38
Limitations and Future Directions
This study had several limitations. First, this was a retrospective cohort study which had inherent risk of selection bias. Nonetheless, patients from case and control groups were matched for confounding factors of bone healing (age, smoking, DM, opening gap size) and underwent the operation under the same surgical technique with standardized postoperative care to improve the strength of analysis. Second, this study focused purely on radiographical outcomes of MOWHTO with the PCL-TCP implant as an osteotomy gap filler but did not describe the clinical outcomes of these patients. Lastly, this was the first study of radiological outcomes of MOWHTO with the PCL-TCP implant as an osteotomy gap filler over a period of 1 year. Clinical outcomes of these patients have not been described, and future studies can aim to report the clinical outcomes of patients who have undergone MOWHTO with the PCL-TCP implant as an osteotomy gap filler.
Conclusion
Bone union rates observed in patients who underwent MOWHTO with the patient-specific 3D-printed honeycomb-structured PCL-TCP synthetic graft osteotomy gap filler were superior to those in the group with allogeneic osteotomy gap fillers at 1 year postoperatively, with no significant difference in complication rates (postoperative infection, lateral hinge fractures, and persistent pain). The patient-specific 3D-printed honeycomb structured PCL-TCP synthetic graft serves as a new and viable option as an osteotomy gap filler for MOWHTO to facilitate bone union without the drawbacks of the traditional autograft or allograft options.
Footnotes
Authors’ Note
This work was performed at the Department of Orthopedics, Singapore General Hospital, Singapore, and the Department of Orthopedics, Sengkang General Hospital, Singapore.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our Institutional Review Board (IRB), SingHealth Centralized Institutional Review Board (CIRB: 2022/2045) with consent for participation obtained for all patients in the study.