
Abstract
Introduction
High tibial osteotomy (HTO) is a surgical procedure aimed at inhibiting the progression of osteoarthritis of the knee joint. The aim of this study was to identify factors influencing the functional outcome after opening wedge valgus HTO.
Methods
A total of 175 cases (155 patients) of varus-correcting high tibial open-wedge osteotomies using the Tomofix plate were reviewed retrospectively. Patients answered the Knee Injury and Osteoarthritis Outcome Score (KOOS) questionnaire and 4 survey follow-up questions.
Results and Discussion
A total of 76 of the 155 patients studied (84 of the 175 knees) completed the KOOS questionnaire, on average 3.1 years (SD 1.8 years) after the surgery. The median scores (with median absolute deviations [MAD]) for the KOOS pain, symptoms, daily activities, sports, and quality of life sections were, respectively, 76.4 (MAD 12.5), 75.0 (MAD 14.3), 85.3 (MAD 11.8), 50.0 (MAD 25.0), and 59.4 (MAD 21.9). No cases of nonunion were observed throughout the length of the study. Identified predictors of worse outcomes were higher weight and body mass index, limited knee flexion, genu varum and tibial varus of small magnitude, active smoking status at the time of surgery, further surgery for plate removal, and some grades of chondropathy in the patellofemoral, medial tibial, and femoral compartments. Patient gender, joint obliquity and over- or undercorrection were not associated with any of the outcomes.
Conclusion
This study shows good results following valgus HTO that are comparable to outcomes following total knee arthroplasty, reinforcing the option of HTO as a valid alternative for total knee arthroplasty.
Keywords
Introduction
For patients with symptoms of early-stage osteoarthritis, surgeons often recommend waiting until the knee’s condition is considerably worse before getting total knee arthroplasty (TKA) surgery. Other than viscosupplement injection, physiotherapy, and weight loss, patients with early-stage osteoarthritis are often asked to “wait things out.” One of the treatment alternatives for medial knee osteoarthritis in active patients with varus knees is valgus high tibial osteotomy (HTO). By shifting weight off the damaged side of the joint to a healthier area, the HTO can correct knee alignment, relieve pain, improve knee function, and slow the progression of osteoarthritis on the affected side. 1 If successful, it may delay the need for TKA and allow the patient to comfortably participate in physical activities. 2
Purpose
Currently reported results within the medical literature are inconsistent, largely in relation to the variability of available HTO implants and techniques, as well as use of bone graft and postoperative weightbearing allowance. The goal of the study was to assess and identify factors influencing functional outcome of medial opening wedge proximal tibial osteotomies in patients with medial knee osteoarthritis.
For this retrospective review, it was hypothesized that medial opening wedge proximal tibial osteotomy is a beneficial procedure for active patients, with best results in selected patients according to different predictive variables such as the weight, knee range of motion, and degree of chondropathy.
Methods
Patient Recruitment
Patients in this retrospective review were included if they presented medial knee osteoarthritis and had a medial open-wedge valgus HTO performed by the senior author (FL) between 2008 and 2016 at our institution using the Tomofix plate (Depuy-Synthes, West Chester, PA, USA). There were no exclusion criteria.
After having obtained every patient’s authorization by phone, questionnaires and consent forms were sent by email. The use of email was deemed a reasonable and inexpensive alternative to paper mail given the age range of the population of interest. Both forms and questionnaires were then sent back by patients via email or fax. Patients who were unable to return the documents via those methods were sent a prestamped envelope that could be used to return the documents by regular mail.
The protocol was reviewed and accepted by the local ethics committee (registration number 16.116).
Surgical Technique
Knee arthroscopies were systematically performed prior to any HTO procedures to address any unstable meniscal tear and assess cartilage damage for the whole knee, using the International Cartilage Regeneration & Joint Preservation Society (ICRS) grading system. 3
HTOs were performed proximal to the tibial tuberosity under fluoroscopic guidance through a longitudinal anteromedial incision. The lateral hinge was made at the level of the proximal tibiofibular joint. Opening of the osteotomy was determined based on preoperative planning using long-leg films. Intraoperatively, a metallic rod was centered on the femoral head using fluoroscopy as well as the centre of the ankle. The osteotomy opening was then increased until the planned opening was obtained. Proper alignment was confirmed with the rod when it was aligned with the lateral aspect of the lateral tibial eminence. The osteotomy was stabilized with a titanium plate and locking screws (Tomofix, DePuy Synthes, West Chester, PA, USA).
Compression of the lateral hinge was routinely performed by first pressing the flat plate against the concave surface of the medial proximal tibia with a temporary nonlocking screw. Locking screws were then inserted in the proximal and distal fragments and the nonlocking screw was finally replaced by a bicortical locking screw. No bone grafts were used as part of the standard aforementioned procedure, with the exception of 4 knees operated early in the series, and for which cancellous bone allograft or bone graft substitute was inserted in the wedge space. The final alignment of the leg was assessed using a metallic rod and fluoroscopic images for each knee were saved for operative patient records.
Postoperatively, physical therapy was initiated within a week. Weightbearing was immediately allowed as tolerated. Thromboprophylaxis was used strictly in instances when patients had previously sustained a thromboembolic event. In these cases, subcutaneous low-molecular-weight heparin was administered twice daily for 2 weeks.
Data Collection
Retrospective Evaluation
A retrospective chart review was performed for all the patients of the cohort. Recorded data included age, gender, body mass index, tobacco use, ICRS chondropathy grading for all knee surfaces, 3 operative date, length of surgery and hospital stay, use of bone graft, presence or absence of complications, and knee range of motion compiled for every clinical visits. The following grading systems were used to assess preoperative and postoperative radiographs: Ahlback osteoarthritis grade for the tibiofemoral compartments 4 and Iwano osteoarthritis grade for the patellofemoral compartment. 5 Radiographs were also used to measure tibial slope, medial opening, 6 limb alignment and patellar height (as measured from the distal edge of the patellar articular surface to the upper limit of the anterior tibia). Additionally, the Caton-Deschamps index 7 and joint line orientation relative to the ground were used.
Provincial data were revised for all patients to identify those who underwent total knee arthroplasty following HTO. For 9 knees (5.1%) only local data from our institution were used, since provincial data were not available.
KOOS Questionnaire and Patient Satisfaction
Functional outcome was assessed using the French version of the Knee Injury and Osteoarthritis Outcome Score (KOOS). 8
Four survey follow-up questions assessing treatment satisfaction were also submitted to the participants, as a way to assess patient satisfaction with the treatment. The questions were: “Are you satisfied with the surgery?”; “Are you able to practice all the physical activities you like?”; “Is the knee pain you used to have prior to surgery still present?”; “If you could go back in time, would you undergo the same surgery again?” Possible answers were based on a visual assessment scale ranging from “Not at all’ to “Totally.” Patients were instructed to mark the scale as precisely as they could. Results were then measured with a ruler and reported as a percentage of the total length of the scale, 0% being at the “Not at all” mark and 100% being at the “Totally” mark.
Data Analysis
Data management and statistical analysis were conducted using SPSS version 25 (IBM Corporation, Armonk, NY, USA). Preoperative baseline variables and KOOS outcome were assessed using standard descriptive statistics. Continuous variables were described using means, standard deviations, and ranges. Categorical variables were described using absolute and relative frequencies.
KOOS and follow-up survey questions were analysed using medians and median absolute deviations (MAD) because of the nonnormal distribution of the results.
Linear regressions were produced for every continuous and categorical variable. All possible associations between variables and outcomes were assessed. In total, 252 statistical tests were completed. Corrections for multiple testing were not performed in this exploratory analysis. Significant findings should be validated in future studies. Additionally, splined regressions were calculated for every continuous variables associations and compared with the standard linear regression using a likelihood ratio test in order to assess if nonlinear models were a better fit for the different variable-outcome relationships.
Survivorship analyses were conducted using the Kaplan-Meier method. 9
Results
Among the 155 patients (175 knees) included in the continuous operative series of this retrospective review ( Table 1 ), 76 participants (84 knees) returned the questionnaire (49% response rate).
Patients Characteristics.

There were no statistically or clinically significant differences at baseline between patients who returned the questionnaire and those who did not. Minor, major, and total complications did not differ statistically between responders and non responders.
Median KOOS scores for pain, symptoms, activities of daily living (ADL), sports, and quality of life sections were respectively of 76.4 (MAD 12.5), 75.0 (MAD 14.3), 85.3 (MAD 11.8), 50.0 (MAD 25.0), and 59.4 (MAD 21.9) ( Fig. 1 ).
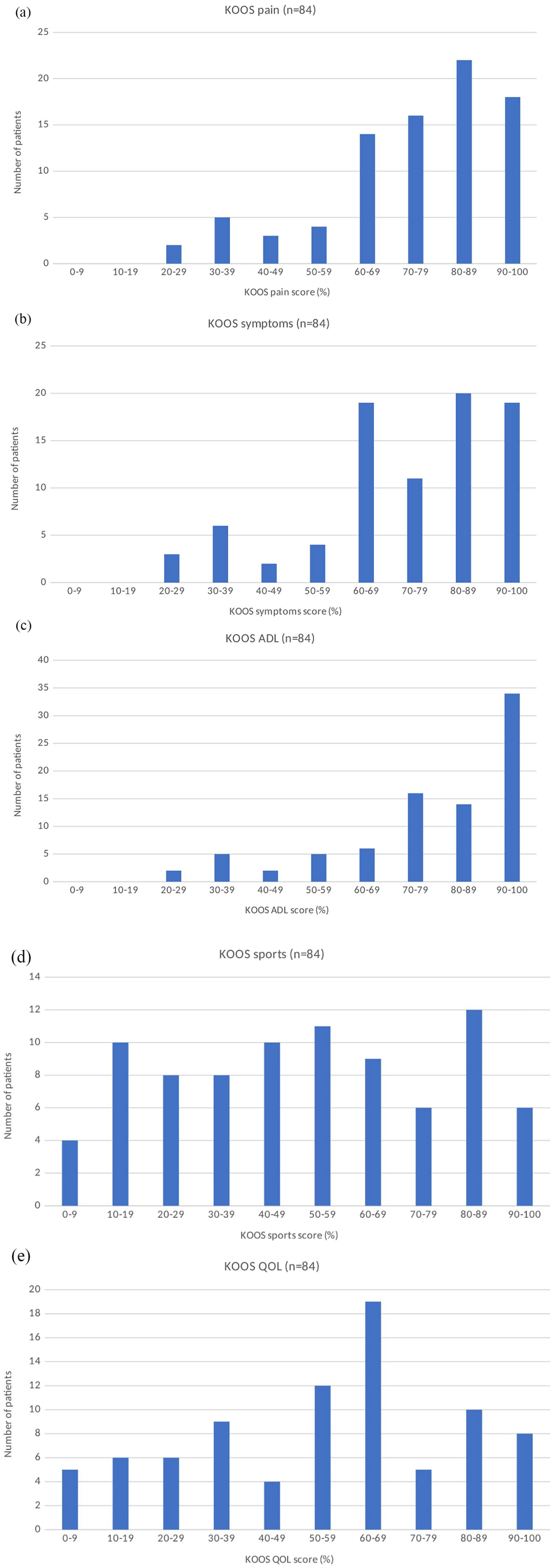
Postoperative scores of the cohort for Knee Injury and Osteoarthritis Outcome Score (KOOS) pain (
Median scores for the investigator-made additional questions pertaining to satisfaction, physical activities, residual pain, and reoperation were, respectively, of 80.0% (MAD 13.0%), 55.0% (MAD 26.0%), 14.0% (MAD 11.0%), and 94.5% (MAD 4.5%) ( Fig. 2 ).
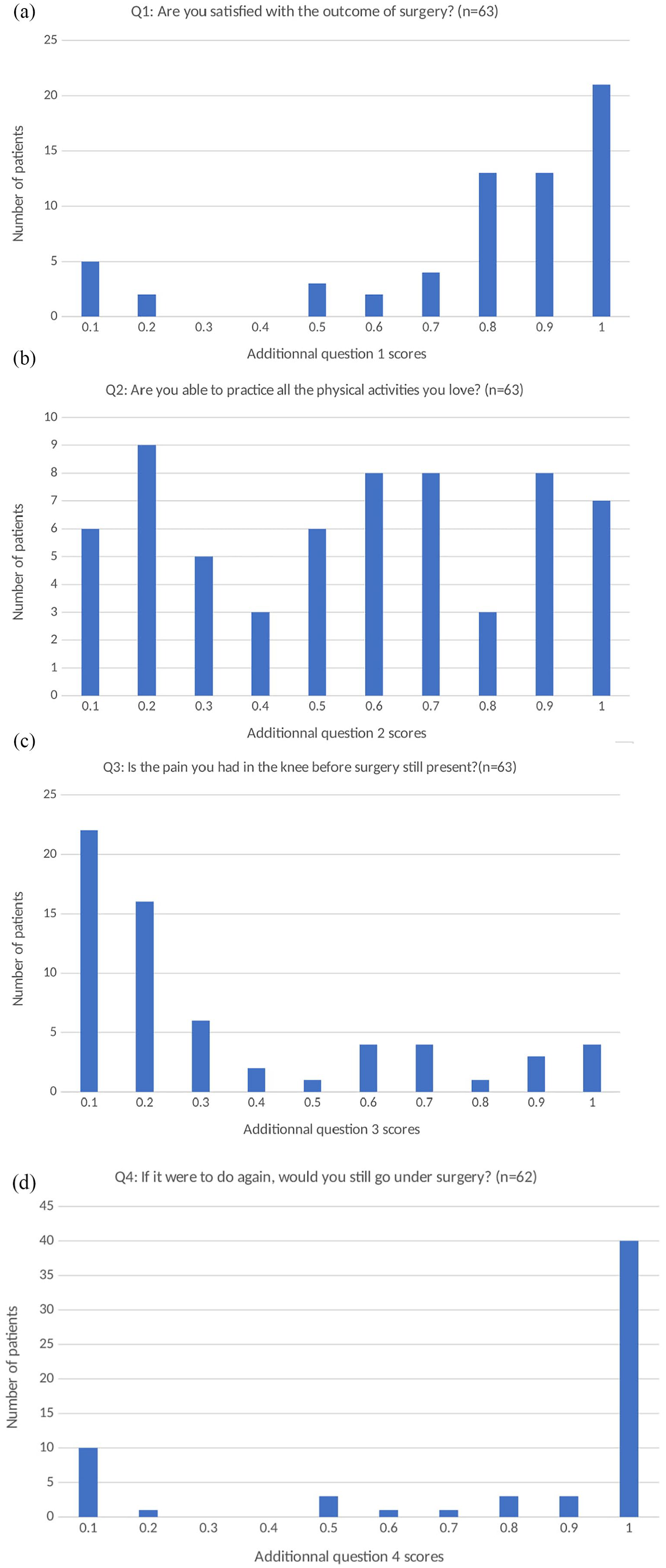
Postoperative scores of the cohort for additional question 1 (
Complications
Minor Complications
Sixty-two patients (35.4%) returned to the hospital prior to their planned follow-up visit; 20 patients (11.4%) for whom a minor complication was diagnosed (cellulitis, n = 17; blisters, n = 1; purpuric rash, n = 1; intense pain, n = 1). Superficial infections (n = 17, 9.7%) were treated for the most part with an initial dose of intravenous antibiotics followed by oral antibiotic treatment. Six of the 17 superficial infections required readmission. Other complications were related to postoperative leg swelling and resolved spontaneously. A total of 13.1% of responders had a minor complication, compared with 9.9% of nonresponders (P = 0.506).
Major Complications
In 1 case, profuse bleeding was noted from the surgical site at the release of the pneumatic tourniquet. Computed tomography angiography revealed an aberrant tibial anterior artery, that is, located anterior to the popliteus muscle and right on the posterior tibial cortex. 10 The artery was iatrogenically lacerated, probably by the sawblade. Following this intraoperative finding, the artery was embolized with vascular coils the same day without further complication.
Deep infections (n = 3, 1.7%)) were treated using intravenous antibiotics and surgical lavage. Eleven patients were treated for a thromboembolic complication (6.3%), 10 infrapopliteal thromboses and 1 case of suprapopliteal thrombosis; every case was treated with oral anticoagulants on an outpatient basis. There were no cases of pulmonary embolism among the patients reported within this continuous operative series. Overall, 9.5% of responders had a major complication, compared with 6.6% of nonresponders (P = 0.475).
Hospital readmission was necessary for 5.1% (n = 9) of all patients. Four of these patients completed the study.
Reoperation
Forty-three patients (24.6%) were eventually reoperated for plate removal because of residual pain. Three patients (1.7%) were revised to TKA after an average of 2.1 years (SD 0.6 years) following HTO due to residual pain and stiffness.
Eleven knees (6.3%) were converted to TKA after an average of 4.4 years (SD 3.2 years). Using Kaplan-Meier survivorship analysis, 96.0% (95% CI: 93.1% to 98.9%) and 91.9% (95% CI: 86.0% to 97.8%) of knees had not required conversion to TKA at 5 and 10 years after HTO, respectively ( Fig. 3 ).
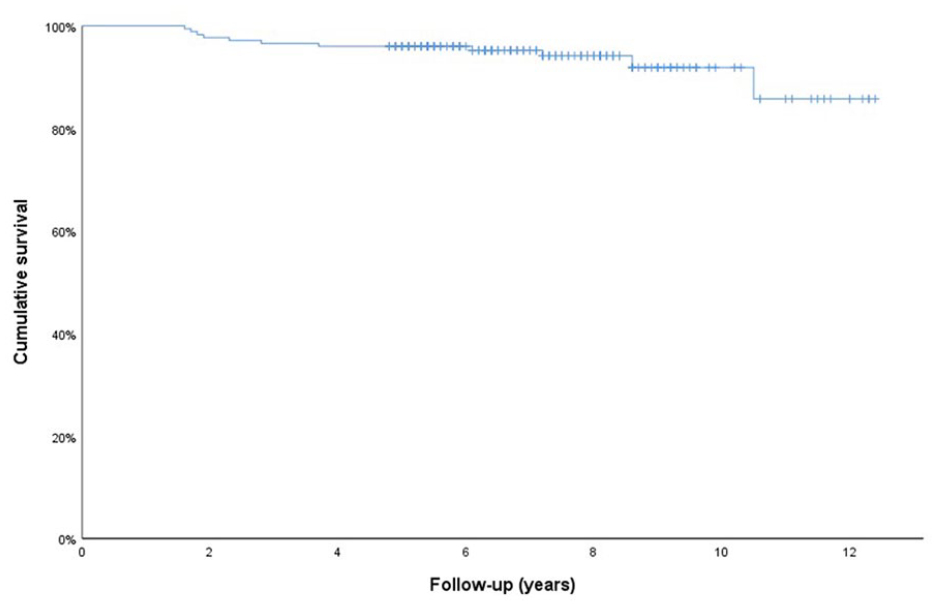
Kaplan-Meier survivorship analysis of high tibial osteotomy (HTO) for conversion to total knee arthroplasty (TKA).
Predictive Factors
Through statistical analysis of the collected data, several continuous and categorical preoperative variables were correlated to HTO outcomes ( Tables 2 and 3 ). Every additional degree in preoperative knee flexion was linked to better outcomes. Higher weight and body mass index (BMI), as well as decreased genu varum (as seen with higher preoperative medial tibial angle, higher preoperative hip knee ankle angle, or more lateral preoperative leg axis intersection) were all associated with worse outcomes.
Significant Linear Regressions between Outcomes and Continuous Variables, with Corresponding Coefficient of Determination (r2) and P Value.

KOOS = Knee Injury and Osteoarthritis Outcome Score; BMI = body mass index; ADL = activities of daily living.
Significant Linear Regressions between Outcomes and Categorical Variables, with Corresponding Coefficient of Determination (r2) and P Value.

Weight and BMI.
In relation to weight, every increase by one kilogram corresponded to a score decrease in KOOS pain, ADL, and symptoms by 0.26, 0.29, and 0.31 points on the KOOS score scale from 1 to 100. Similarly, every BMI increase of 1 kg/m2 was associated with a decrease of 0.99, 1.10, and 1.04 points for the same respective categories as the ones mentioned for weight.
Preoperative Angles
Every additional preoperative medial tibial angle degree was linked to a decrease of 1.69 points of the KOOS pain. Every additional preoperative hip knee ankle angle degree correlated with decreases of 2.12 points for the KOOS pain score, and 1.83 points for the satisfaction question. Similarly, decreased genu varum, as seen by a more lateral preoperative leg axis intersection, was associated with decreases in the same categories (KOOS pain and satisfaction question) with respective regression coefficient values of 0.53 and 0.45 for every 1% increase of the preoperative leg axis intersection.
Plate Removal
Plate removal was statistically correlated with worse outcomes for KOOS pain, ADL, symptoms, and sports subscores. Scores for patients who had a second surgery for plate removal were lower by 14, 16, 13, and 24 points on a scale of 1 to 100, respectively.
Chondropathy
Medial femoral chondropathy, particularly grade 2 and grade 3 chondropathy, was associated with worse outcomes on KOOS pain, ADL, and sports. It was also associated with lesser level of physical activity, as assessed by the additional investigator-implemented follow-up survey questions (question 2 “Are you able to practice all the physical activities you like”) ( Table 3 ). KOOS pain scores were 8 points lower for grade 1 medial femoral chondropathy (nonsignificant [n.s.]), 29 points for grade 2 (P = 0.023), 22 points for grade 3 (P = 0.046), and 12 points for grade 4 (n.s.). Similarly, patellofemoral chondropathy tended to be associated with poorer outcomes, as assessed by the KOOS pain and QOL categories. KOOS pain scores were 6 points lower for grade 1 patellofemoral chondropathy (n.s.), 9 points for grade 2 (n.s.), 7 points for grade 3 (n.s.), 43 points for grade 4 (P = 0.027) ( Table 3 ). Medial tibial chondropathy was correlated with worse KOOS sports subscores, with a decrease of 25 points for grade 1 chondropathy (n.s.), 45 points for grade 2 (0.034), 40 points for grade 3 (n.s.), and 41 points for grade 4 (P = 0.047) ( Table 3 ).
Smoking
Active smoking status at the time of the surgery was associated with a decrease of 21% (P = 0.032) for the satisfaction question (“Are you satisfied with the surgery?”).
All the coefficients of determination (r2) for continuous variables were less than 10%. For categorical variables, one coefficient of determination was calculated for every variable. Some associations involving medial femoral chondropathy and plate removal were correlated with an r2 >10% (medial femoral chondropathy had a r2 of 12.7% with KOOS pain, 11.5% with KOOS ADL, 11.0% with additional question 1, 13.1% with additional question 2, and 12.0% with additional question 4, plate removal had a r2 of 11.6% with KOOS sports), although most significant categorical associations remained with r2 values <10%.
Other Findings
Splined regressions were a better fit for only 2 of the measured variables: preoperative knee flexion on additional question 3 ( Fig. 4 ), and age on some KOOS subscores (pain, ADL, symptoms, and sports) ( Fig. 5 ).
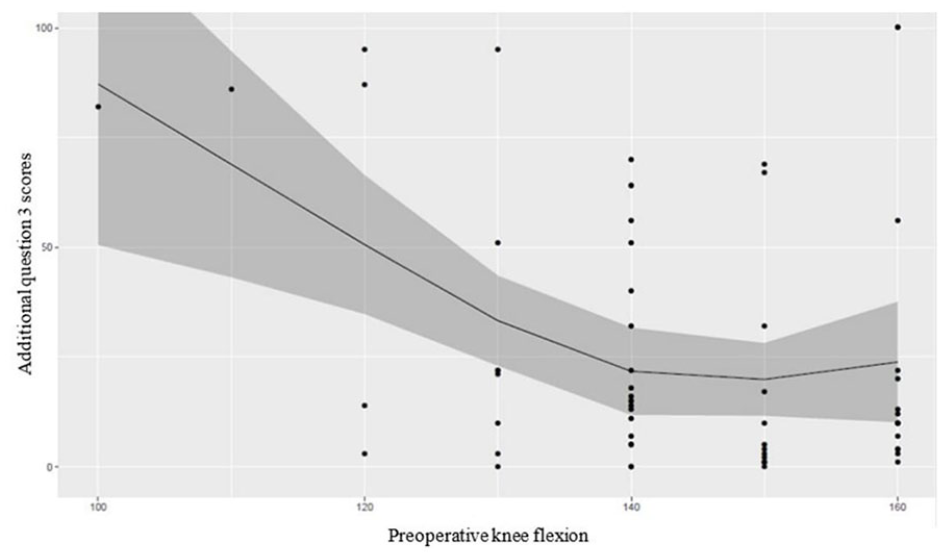
Additional question 3 (residual pain) scores in relation with preoperative knee flexion.
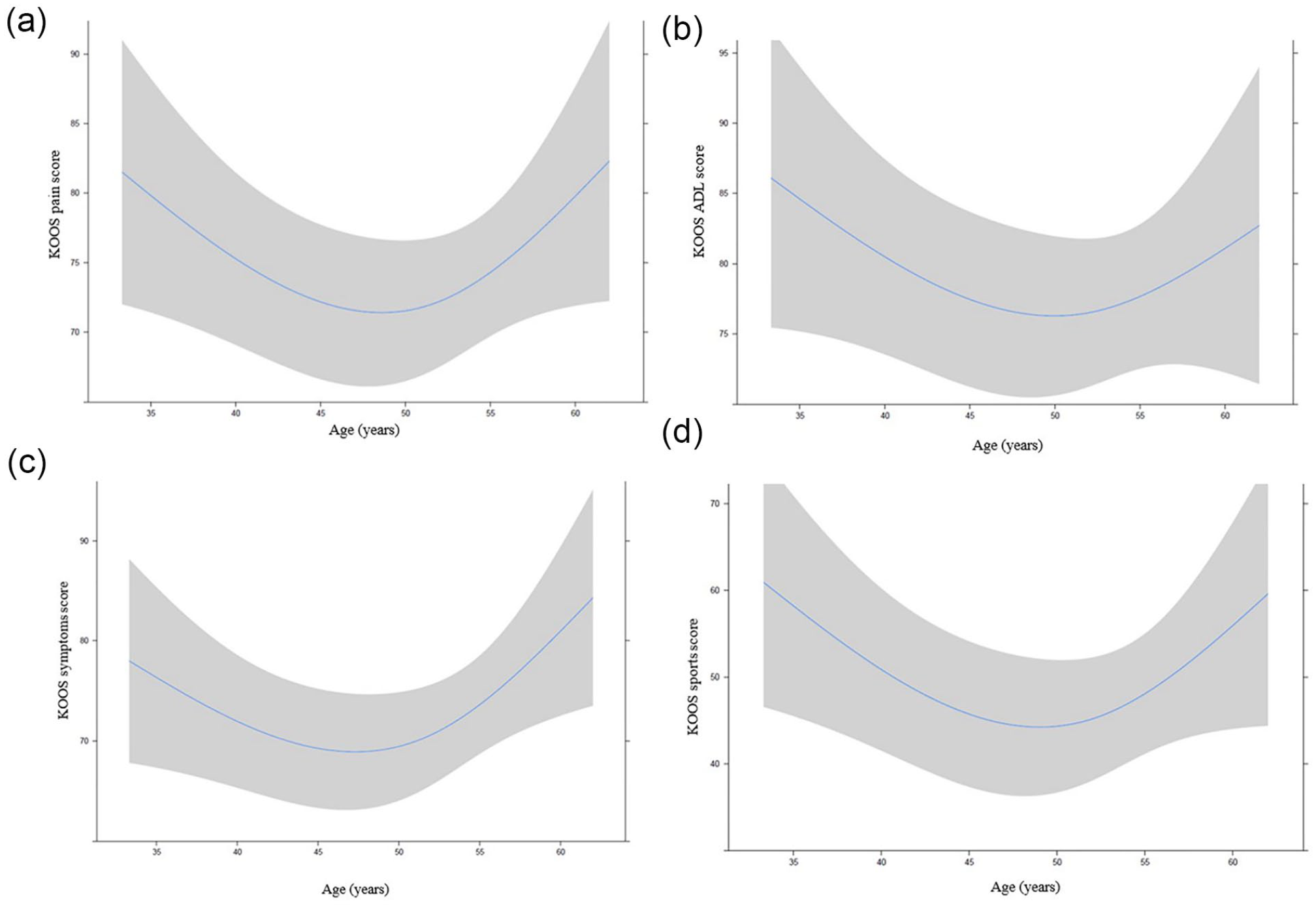
Nonlinear regression between age and Knee Injury and Osteoarthritis Outcome Score (KOOS) pain (
The relation between age and different KOOS outcomes seemed to be quadratic, meaning that better results were seen with younger or older patients, whereas patients around 50 years old had worse scores ( Fig. 5 ).
Leg mechanical axis intersection at the knee being important in surgery planning and procedure, its postoperative value was analyzed to assess any influence on the outcome. No statistical significance was found in relation to various percentages of over- or undercorrection of the intersection axis described in the literature and both the KOOS and additional questions scores among surveyed patients. 11
Similarly, an association was not observed between joint obliquity and KOOS scores or any of the answers to the additional survey questions.
Finally, angular correction of the lower limb, as assessed by the medial cortical opening, had an inverse correlation with postoperative patellar height, according to the postoperative Caton-Deschamps index. The association was statistically significative with a Pearson coefficient of −0.246 (P = 0.025, r2 = 6.0%).
Discussion
Known risk factors for less satisfactory outcome were confirmed, namely high BMI and weight,11 -14 and limited knee flexion.12,14 -16 Some degrees of chondropathy in the patellofemoral, medial femoral and medial tibial compartments were also associated with worse outcomes,14,17,18 as discussed further in the discussion. Gender did not play a significant role in relation to outcomes within this patient cohort. This is in line with the available literature, although some authors found that women have generally poorer postoperative outcomes and/or earlier total knee arthroplasty.13,14,19,20 Knee flexion contracture was also not statistically related to outcome within this cohort, whereas some authors reported an association in the literature.14,16 Comparison with the literature is difficult on account of the vast variety of techniques and implants, but we found no studies clearly stating genu varum of low amplitude as a risk factor for a worse clinical outcome.
Globally, the present study confirmed an overall good clinical outcome after medial opening wedge proximal tibial osteotomy in spite of the studied cohort’s heterogenicity, with median KOOS scores of 76.4 (MAD 12.5), 75.0 (MAD 14.3), 85.3 (MAD 11.8), 50.0 (MAD 25.0), and 59.4 (MAD 21.9) for the pain, symptoms, ADL, sports, and QOL categories, respectively. This is also supported by the additional questions results, as well as by the low rate of severe complications or revision to TKA. The high rate of early return to hospital within the first postoperative week highlights it is difficult for patients on account of swelling and pain. This would warrant better preoperative patient education on better pain and swelling coping strategies for this surgical procedure. It is worth mentioning that despite the arduous initial postoperative recovery, most patients responded they would still undergo the procedure if they were again given to choose (median score of 95% at additional question 4). Complication rates vary in the literature according to definitions and are comparable to the present study with rates ranging between 6% and 55%.11,14,20
Linear regressions performed in this study between age and the different outcomes were not statistically significant. However, splined regressions were found to be a better fit for some of these associations, especially KOOS subscores. Results tend to indicate better outcomes are observed with either younger or older patients, while patients between the ages of 45 and 50 years appeared to have worse KOOS subscores. A post hoc analysis of variance was performed to compare different age subgroups for the distribution of all preoperative variables. Only lateral tibiofemoral arthrosis barely reached statistical significance (P = 0.05) as grade 1 arthrosis was noted in 2 knees in both the 45- to 49-year-old and 50- to 54-year-old subgroups and not in the 2 other age subgroups. Although the numbers are small, this finding is not very surprising for younger patients as they are less likely than older patients to display signs of lateral compartment arthrosis. For older patients, lateral arthrosis is likely to make osteotomy a less attractive option as compared with total knee arthroplasty, therefore it is unsurprising that no patient in the older subgroup showed radiographic signs of lateral compartment arthrosis. Additionally, results within this cohort study seem to indicate that lateral tibiofemoral arthrosis is not significantly correlated with any of the outcomes. This is however most likely due to the small number of patients with lateral compartment arthrosis. HTO is not formally contraindicated solely based on age. Nonetheless, since HTO is less commonly performed for younger or older patients, it seems likely that these 2 subsets of the reported cohort presented other factors making them good candidates for this procedure. Therefore, a selection bias may explain why slightly better results were found for them. We found no study clearly stating that type of association, although some studies found that increasing age is associated with a worse clinical outcome.18,21,22 In addition, Floerkemeier et al. 20 also found that age had no linear effect on postoperative outcome in a study with similar patient demographics and methodology.
Risk factors mentioned above should not be considered as absolute contraindications but rather as guides for surgical decision making, as some of the associations mentioned above are based on a relatively low number of participants. It must be recognized that, although statistically significant, most correlations were weak, with most coefficients of determination being <0.1.
No cases of nonunion were observed, although only 4 out a total of 175 osteotomies within this cohort made use of any kind of graft or bone substitute. This is comparable to observations made by Kolb et al. 23 who only reported 1 case (2%) of nonunion after performing open wedge osteotomies without the use of bone grafts.
Eleven patients were treated for a thromboembolic complication postoperatively, all but one being infrapopliteal thrombophlebitis that were diagnosed by a duplex ultrasonography that was ordered because of leg swelling. This raises 2 questions: Should the phlebitis have been treated and should chemical thromboprophylaxis be used postoperatively for high tibial osteotomy? Indeed, considering that no pulmonary embolism and a single proximal venous thrombosis were diagnosed in the reported cohort, that patients were instructed to mobilize their knee and ankle immediately and bear weight on the operated leg as soon as tolerated, and the 31% false positive rate of duplex ultrasonographies performed after knee surgery, 24 a portion of the reported phlebitis may in fact be cases of overdiagnostic and/or overtreatment. Furthermore, systematic chemical thromboprophylaxis may even exacerbate postoperative leg swelling and related symptoms. We hypothesize that mechanical methods to decrease swelling, like leg elevation and compressive stockings, are a better way to mitigate this problem. A recent study by Erickson et al. 25 following 141 patients who underwent high tibial osteotomy, distal femoral osteotomy or tibial tubercule osteotomy found only 2 cases of deep venous thrombosis, one of which progressed to pulmonary embolism. They claim that thromboprophylaxis after these osteotomies may not be warranted.
Patients with a more lateral preoperative mechanical axis regarding the knee had worse results on the KOOS sports subscore and satisfaction question, meaning that patients with a bigger knee varus deformation ended up with better outcomes. Postoperatively, we found no statistically significant differences for the KOOS or additional questions scores between patients with a correction greater than or less than 62.5% of the mechanical axis. This differs from what can be found in the literature. El-Azab et al. 11 found that open-wedge high tibial osteotomy results in significant improvement of symptoms and function in all patients in the short term, even with under- and overcorrection of the osteotomy. However, they found that undercorrection (defined as a mechanical axis <50%) was associated with a significantly lower clinical outcome in comparison to the accurate correction (between 50% and 70%) and overcorrection (defined as a mechanical axis >70%) 11 ; this association was not observed for this cohort’s results, even when patients were analyzed using the same alignment values. This discrepancy suggests that final limb alignment is one of many factors to consider in the aftermath of an open wedge HTO and could be less important than is currently thought.
Greater corrections, as assessed by the medial cortical opening, were however associated with a lower postoperative patellar height, according to the Caton-Deschamps index. Those results are consistent with the literature, in cases where HTO performed above the tibial tubercle were associated with decreased postoperative patellar height.26,27 No association was found between patellar height, either preoperatively, postoperatively, or its variation, and any of the outcomes assessed in this exploratory study, with all correlations being found to be nonsignificant. In addition, when taken separately from other factors, we were not able to establish any threshold beyond which for this variable from which postoperative patellar height becomes a statistically significant risk of worse outcome. Although patella baja is known to be linked to more challenging total knee arthroplasty procedures if that becomes necessary, 28 it remains to be seen if it actually affects the clinical outcome post high tibial osteotomy. On this question, El Amrani et al. 29 found that patellar height decrease did not affect functional results whether height remained normal or became low. However, in their study, the worst functional results were associated with patella baja. 29
Postoperative joint line obliquity was not associated in any way with the KOOS or the additional questions results. Differences in KOOS or additional questions scores between patients with a lateral joint line slant of 4° or more and those with a lesser obliquity were nonsignificant. The 4° value represents the joint line obliquity value beyond which a double level osteotomy should be performed instead of an isolated tibial osteotomy according to Babis et al. 30 Our results therefore challenge the notion that increased joint line obliquity is not well tolerated.30 -32 It remains to be seen how patients with laterally slanted joint lines fare in the long term and/or if joint replacement has to be performed.
Grade 4 chondropathy in the patellofemoral compartment was associated with worse outcomes seen in the KOOS pain and quality of life categories. This is supported by the literature as most authors report worse outcomes with patellofemoral arthrosis.14,18,33 Even though there was a negative trend with all grades of chondropathy, only patients with grade 4 patellofemoral chondropathy reported statistically significant worse scores on both the KOOS pain and quality of life categories. On the latter, although it was less important, grade 1 chondropathy also had a statistically significant impact. The degree of patellofemoral chondropathy should therefore be taken into consideration when contemplating HTO for a given patient.
Chondropathy in the medial femoral compartment influenced different outcomes as seen with KOOS pain, KOOS ADL, KOOS sports and additional question 2. As more precisely described in the results, grade 2 or grade 3 chondropathy significantly decreased scores for the KOOS subscores previously mentioned. While it is easy to understand that patients with less important chondropathy have better outcomes, it is less easy to explain why patients with grade 4 chondropathy at the medial femur tend to have better outcomes. Although Floerkemeier et al. 20 observed a tendency for lower outcomes with more severe preoperative cartilage lesions, they found that patients with grade 4 lesions still had a good outcome score and the surgery still had a positive effect on the patients’ functional outcome. One hypothesis is that patients with more important articular damage are the ones who, being the more affected by the disease, benefit most from surgery. It is worth noting that grade 4 medial femoral chondropathy was noted in 44% of the knees of our cohort, so lack of power is difficult to evoke to explain our conflicting findings at the femur. On the other hand, chondropathy in the medial tibial compartment was associated with worse outcomes on the KOOS sports subscore. The association was statistically significant for grade 2 and 4 chondropathy, but there was a clear tendency that worse results were seen with chondropathy grades 2, 3, and 4 compared with grades 0 or 1. This once again corresponds to most of what is found in the literature where most authors agree that worse outcomes are seen with severe medial tibiofemoral articular damage.18,20,33
A likelihood ratio test between the splined and standard linear regression revealed a better fit for the nonlinear model for the relationship between preoperative maximum knee flexion and question 3 (Is the pain you had in the knee before surgery still present? Fig. 4 ). While a visual inspection appears to suggest a stabilization in better outcomes regarding residual pain for those with a preoperative knee flexion of 140° and more, the data are highly clustered toward higher flexibilities. This result would need to be validated in a larger sample.
Smoking had no statistically significant effect on any of the KOOS scores. However, it influenced the question 1 score in a way that smokers appeared to be less satisfied with the outcome of the surgery. Indeed, scores among smokers for additional question 1 (Are you satisfied with the outcome of surgery?) was 21 points below that of nonsmokers on a scale of 1 to 100. In the current literature, smoking seems to be associated with a worse outcome overall.14,20 Studies specifically designed to evaluate the impact of smoking cessation are necessary to conclude that changing this single habit could have an impact on the postoperative outcome. However, we think that this result is interesting and could be communicated to patients to encourage smoking cessation.
Plate removal was statistically associated with many of the outcomes. Patients who resorted to postoperative plate removal had worse outcomes on 4 out of the 5 KOOS subscores: pain, ADL, symptoms, and sports. This was somewhat expected as plate removal is often undertaken in patients with residual pain as a way of ruling out that the hardware is causing the symptoms. Since the patients within this study only filled questionnaires once, it is not possible to assess whether plate removal was beneficial and how much it played on the patient’s postoperative satisfaction and overall outcome. However, the significantly lower KOOS scores of the patients who underwent plate removal suggests that symptoms persisted thereafter in a certain proportion of them. It would be useful to predict which patients will tolerate the plate or not. However, in this study, patients who proceeded to have an additional surgery for plate removal were no different statistically, for all measured variables, from patients who kept the hardware.
HTO offered low conversion rates to TKA and an excellent survivorship at 5 and 10 years, which were 96.0% and 91.9%, respectively. A meta-analysis conducted by Kim et al. 34 reported similar results with a pooled 5-year survival rate of 95.1% and a pooled 10-year survival rate of 91.6% for open wedge HTO. These data support that valgus HTO is an effective treatment alternative in active patients with medial knee osteoarthritis to delay TKA.
When compared with outcomes following TKA, our results show similar scores for the ADL, sports, and QOL subsections of the KOOS score. However, pain and symptoms subsections are a little lower in our study, by an average of about 10 points each, than what is found in the literature following TKA.35,36 Matsumoto et al. 35 described the same differences of the KOOS score when comparing HTO and TKA outcomes. However, they also found that pain relief satisfaction was higher in the HTO group compared with the TKA group. 35 Perhaps the difference in pain relief is not that significant between both techniques, reinforcing the option of HTO as a valid alternative for TKA.
Some of the limitations noted within this study are, first, that preoperative KOOS scores were not available for the patients in this cohort. It is as such not possible to quantify the functional impact of surgery. Also, only 49% of participants returned their questionnaire. Although no significant difference with regard to data contained within their individual chart was found between the patients who returned the questionnaire and those who did not, we cannot be sure that conclusions for the KOOS and additional questions are representative of the whole cohort. Second, although the KOOS is a good questionnaire for assessment of knee-related conditions, it does not take into account the potential effect that the surgery performed at the knee may have had on the other joints of the same limb. For instance, some patients of the reported cohort mentioned on the phone interview that their knee was fine, but that their lower limb felt nevertheless uncomfortable at the level of the ankle or the hip since their surgery. A more comprehensive questionnaire that would include questions regarding symptoms affecting the entire lower limbs or even the entire body could provide a better overview and more representative results. Finally, a few preoperative factors were noted to potentially have an impact on postoperative outcomes; however, the size of the cohort in this study and the number of patients with given risk factors was too low to draw any strong conclusion. A larger cohort study might help determine whether some variables such as patellar height (or Caton-Deschamps index), postoperative mechanical axis or joint line obliquity, and knee flexion contracture significantly affect postoperative clinical outcomes and patient satisfaction.
Conclusion
Results confirm the relevance of open-wedge valgus HTO in active patients with medial gonarthrosis and genu varum. However, the benefits of this procedure may be lower for some patients, like those with higher weight and BMI, limited knee flexion, or genu varum of small magnitude. Postoperative pain and swelling of the leg should not be taken lightly and warrant additional measures like leg elevation, patient education, and increased use of compressive stockings.
Footnotes
Author Contributions
VC conceived the study, participated in the design of the study, carried out the data collection, participated in the statistical analysis and drafted the manuscript. PAS contributed to the data collection and statistical analysis and helped draft the manuscript. FAS contributed to the statistical analysis and helped review the manuscript. FL conceived the study, participated in the design of the study, supervised the data collection and statistical analysis, and helped to draft the manuscript. All authors read and approved the final manuscript.
Acknowledgments and Funding
The authors would like to thank Lydia Mychaltchouk for her help with the ethics comity approval and her contribution to the manuscript. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The protocol was reviewed and accepted by the local ethics committee (registration number 16.116).
Informed Consent
After having obtained every patient’s authorization by phone, questionnaires and consent forms were sent by email. Both forms and questionnaires were then sent back by patients via email or fax.
Trial Registration
Not applicable.