
Abstract
Objective
To evaluate the outcome of patients who have undergone simultaneous osteotomy and osteochondral allograft (OCA) transplantation. Our hypothesis is that use of high tibial osteotomy and fresh OCA in a combined procedure is safe and effective without increasing morbidity in comparison to OCA alone.
Design
A case series of 17 patients underwent tibial osteotomy and simultaneous OCA during a single surgery. Osteotomy was indicated when axial alignment was within the affected compartment. Patients had a minimum of 2 years of follow-up after surgery. The mean graft size was 8.7 cm2, with 82% located on the medial femoral condyle alone and 18% involving the medial femoral condyle and one or more other sites. Data collection included demographics, osteotomy correction, graft site(s) and area, and clinical evaluation. Failure was defined as conversion to arthroplasty.
Results
Two of 17 patients (12%) failed at a mean of 9.3 years. The remaining 15 patients (88%) had intact allografts with mean survival of 8.1 years (SD 3.3). Five patients (29%) had an additional procedure, all undergoing osteotomy hardware removal. Of those with surviving allografts, mean pain and function scores improved significantly from the preoperative to postoperative assessment and International Knee Documentation Committee total scores improved significantly from 40.9 ± 15.4 preoperative to 75.5 ± 24.0 at latest follow-up (P = 0.003); 92% of patients were satisfied with the results of the surgery. No postoperative complications occurred.
Conclusion
Combining high tibial osteotomy and OCA in properly selected patients is safe and effective.
Introduction
The treatment of symptomatic articular cartilage injuries in the young, active patient remains a challenging problem with an adverse natural history if left untreated.1-3 Joint sacrificing options such as arthroplasty have yielded reliable results, but are not ideal in this patient population because of associated activity restrictions and arthroplasty survival due to the greater demands placed on their knees. 4
High tibial osteotomy (HTO) has been shown to be an effective joint preserving option in these patients and does not preclude them from arthroplasty at a later date.5-8 The biomechanical purpose of HTO is to redistribute the weight-bearing forces away from the diseased compartment, while slowing the progression of the degenerative disease and relieving pain.9,10 The overall survival rate of HTO has been estimated to be between 85% and 95% at 5 years and between 75% and 80% at 10 years.8,11 Another joint preserving option is osteochondral allograft (OCA) transplantation. 12 The osteochondral allografting technique has been utilized for a variety of clinical problems including osteochondral lesions, osteochondritis dissecans, and osteoarthritis.13,14 Long-term survival studies have shown OCA survival rates up to 85% at 10 years, 75% at 15 years, and 69% at 20 years.15,16
More recently, the use of osteotomy has gained popularity as an adjunct to cartilage repair procedures in an effort to optimize the biomechanical environment of the joint.17,18 The realignment theoretically protects the graft by preventing overload of the affected compartment and may slow the progression of degenerative changes. Previous studies have reported the successful use of osteotomy in conjunction with various joint preserving procedures.19,20 However, no studies are available looking specifically at the association of OCA and HTO in cases of large osteochondral defects and varus malalignment. The purpose of the present study was to evaluate the long-term outcomes in a group of patients who have undergone HTO and OCA simultaneously. Our hypothesis is that use of HTO and OCA in a combined procedure is safe and effective for patients with varus malalignment and focal osteochondral lesion of the knee.
Materials and Methods
A retrospective review of our institutional review board–approved outcomes database was conducted to identify all consented patients who had undergone corrective opening wedge tibial osteotomy and OCA transplantation during the same surgery. Indications for the procedure were (1) patients with medial femoral condyle lesions with International Cartilage Repair Society grades 3 and 4 associated with 3° or more of varus malalignment and pain on the medial side of the joint, (2) patients who had failed previous surgical and nonsurgical interventions, and (3) patients who wished to avoid prosthetic arthroplasty. Patients with tricompartmental osteoarthritis and with less than 2 years of follow-up were excluded. Between 1998 and 2011, 18 patients were identified who met the criteria. One patient underwent tibial closing wedge osteotomy and was excluded from this case series. The remaining 17 patients underwent tibial opening wedge osteotomy and comprised the current study population. Patients were at least 2 years from surgery and had a minimum 2 years of follow-up.
Surgical procedures were performed through an extended anteromedial parapatellar approach including an opening medial tibial wedge osteotomy and fresh OCA performed simultaneously. The allograft procedure was executed prior to the osteotomy, according to the surgeons’ preference. Osteotomy was indicated when axial alignment was overloading the affected compartment. The aim of the correction with the osteotomy was individualized based on patient parameters such as age, extent of cartilage disease, and deformity. For smaller cartilage lesions, neutral alignment of the limb was planned. If degenerative disease existed in the medial compartment, the mechanical axis was corrected to beyond neutral alignment to the lateral tibial eminence. Fixation was achieved using a medial tibial wedged plate and 4 screws (DynaFix® VS, Biomet or Puddu Plate, Arthrex) ( Fig. 1 ). All osteotomy defects were filled with osseous autograft and/or allograft.

Anteroposterior radiographic view of an opening-wedge proximal tibial osteotomy and fixation using a medial tibial wedged plate and 4 screws.
Allograft donors and recipients were matched preoperatively according to the anteroposterior radiographic measurement of the tibial width, correcting for magnification. Allograft surgical procedure was performed using the dowel technique utilizing 15 mm to 30 mm plugs. Cartilage lesions were identified on the recipient and were debrided with a cylindrical reamer until bleeding of the subchondral bone was found. The depth of the lesion was kept to a minimum in order to transplant the least possible amount of bone from the donor. Osteochondral grafts were harvested from the donor at the same anatomical location of the lesion on the recipient and with the same depth. Fixation was achieved by a press-fit technique and supplemental fixation using compression screws and/or absorbable internal fixation devices when indicated (Chondral Dart; Arthrex) ( Fig. 2 ). Postoperatively, patients were allowed 25% weight-bearing for 6 weeks and a protective rigid brace was used. Full range of motion was implemented as tolerated immediately after surgery. After 6 weeks braces were discontinued and progressive weight-bearing was begun. Patients were allowed to return to recreational and sports activities by 6 months. Clinical evaluation was performed using the International Knee Documentation Committee (IKDC) pain, function, and total scores; the modified Merle d’Aubigné and Postel (18-point) scale; and patient satisfaction scores on a 5-point scale. The modified Merle d’Aubigné and Postel is a nonvalidated outcome scale that has been previously reported in outcome studies involving allograft transplantation, being a simple and effective tool to measure pain, function, and range of motion. 21 Clinical evaluations were collected pre- and postoperatively. Patients that returned for follow-up visits were examined in the clinic. The one patient unable to return for a recent follow-up was contacted via telephone. The most recent available postoperative scores were analyzed for the study. Failure of the combined procedure was defined as conversion to partial or total knee arthroplasty.
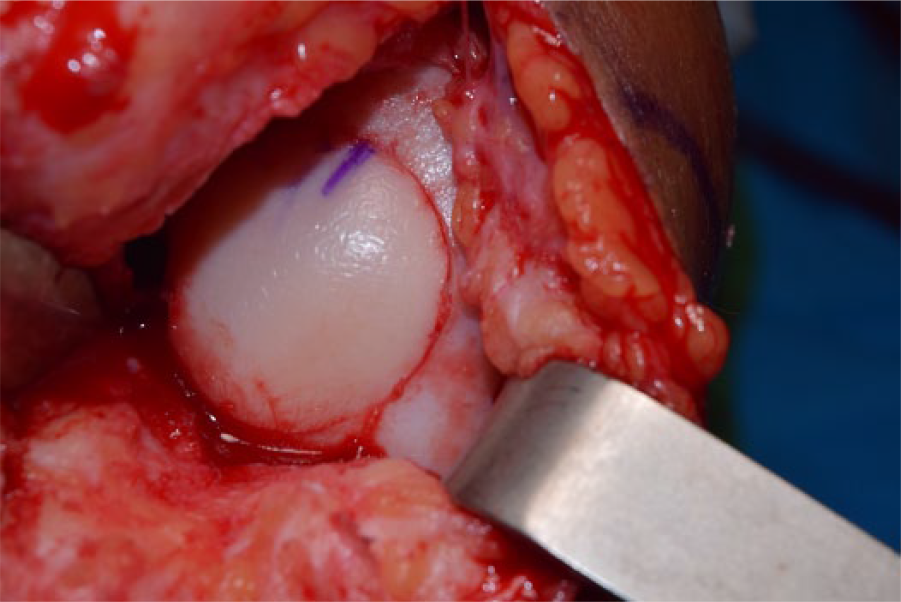
Intraoperative photograph of osteochondral allograft transplantation dowel technique in the medial femoral condyle. Press-fit technique was used for fixation.
Statistics
Means, ranges, standard deviations, and frequencies were calculated to describe study population characteristics, details regarding the allograft (total size, number of graft sites), osteotomy (mm of correction), and postoperative data regarding further procedures. Wilcoxon signed rank tests were used to compare preoperative to postoperative scores on the IKDC and the modified Merle d’Aubigné scores. All statistics were performed using SPSS version 13.0.
Results
Patient demographics are summarized in Table 1 . The mean age of the patients at the time of surgery was 36.5 years (range = 16.9-50.2 years), and mean body mass index was 26.1 ± 3.0. Fifteen patients (88.2%) were male. The OCA was placed in the medial femoral condyle alone in 14 patients (82%). The total graft area averaged 8.7 cm2 (range = 3.2-24.7 cm2). All osteochondral lesions were treated at the time of the surgical procedure. Average number of graft sites was 1.9 (range = 1-4). Twelve of 17 knees (71%) had fixation with bioabsorbable pins; the remaining 5 knees (29%) had press-fit fixation. All knees had varus malalignment with mean coronal correction of 8.7 mm (range = 6.25-12.5 mm). All osteotomies and allografts demonstrated radiographic healing within 6 months.
Patient Demographics and Allograft Details.
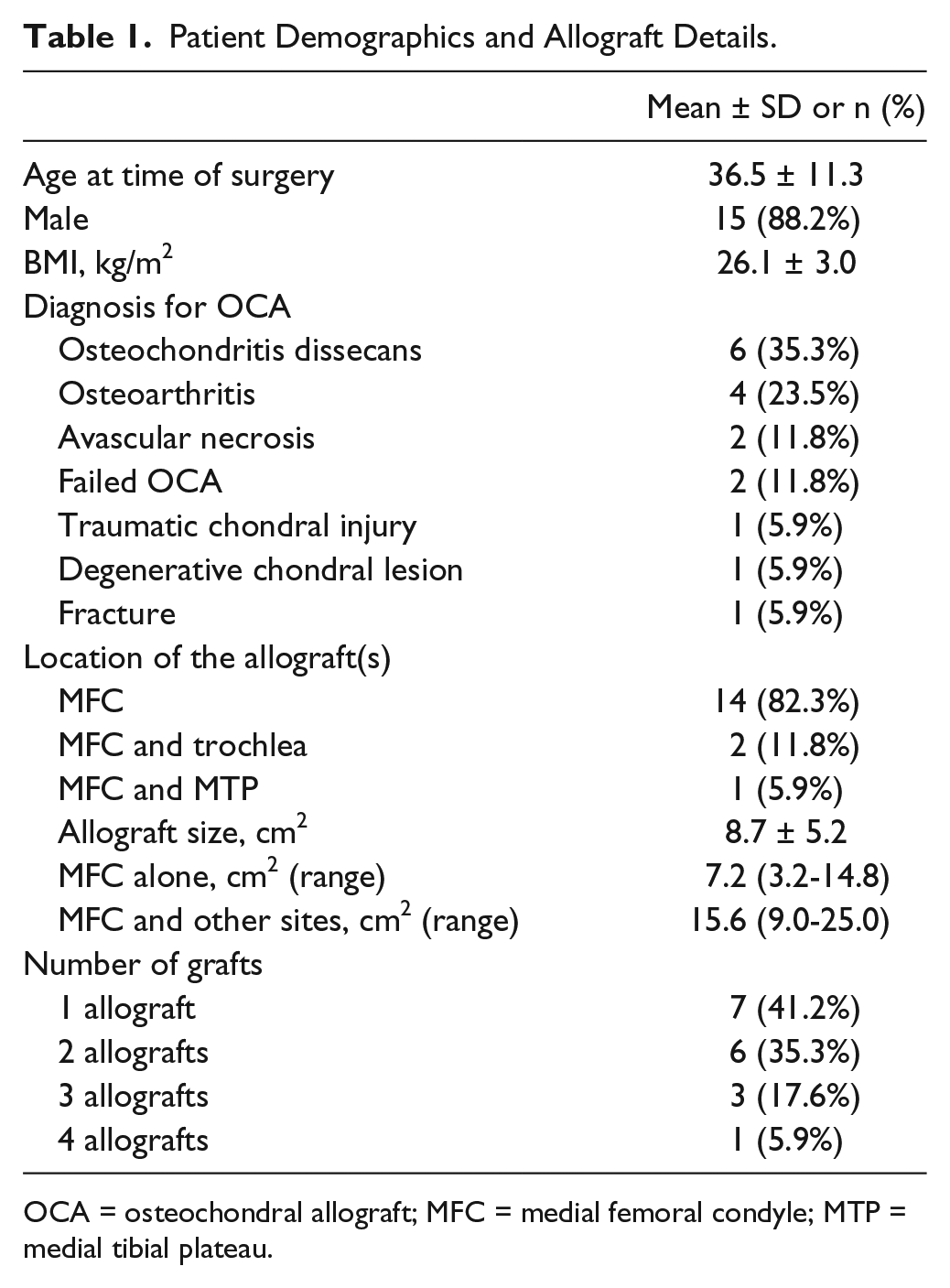
OCA = osteochondral allograft; MFC = medial femoral condyle; MTP = medial tibial plateau.
Overall, 15 patients (88%) had surviving allografts with a mean survival of 8.1 years (SD 3.3). Seven patients required an additional procedure subsequent to the osteotomy and OCA transplantation comprising 5 hardware removals and 2 patients (12%) that failed the allograft procedure with one patient requiring conversion to total knee arthroplasty and one to unicompartmental arthroplasty. The mean time to failure was 9.3 years (range = 7.4-11.2 years). The remaining 5 patients (29%) who required an additional procedure underwent osteotomy hardware removal.
Clinical evaluations were completed for 14 of the 15 patients whose allograft remained in situ at latest follow-up. Scores on the IKDC and modified Merle d’Aubigné-Postel improved significantly from the preoperative visit to latest follow-up ( Table 2 ). Ninety-two percent of the patients expressed satisfaction with the results from their surgery; 57% were extremely satisfied.
Results of Outcome Measures among Patients Who Had OCA and Osteotomy with the OCA In Situ at Follow-up (N = 14).
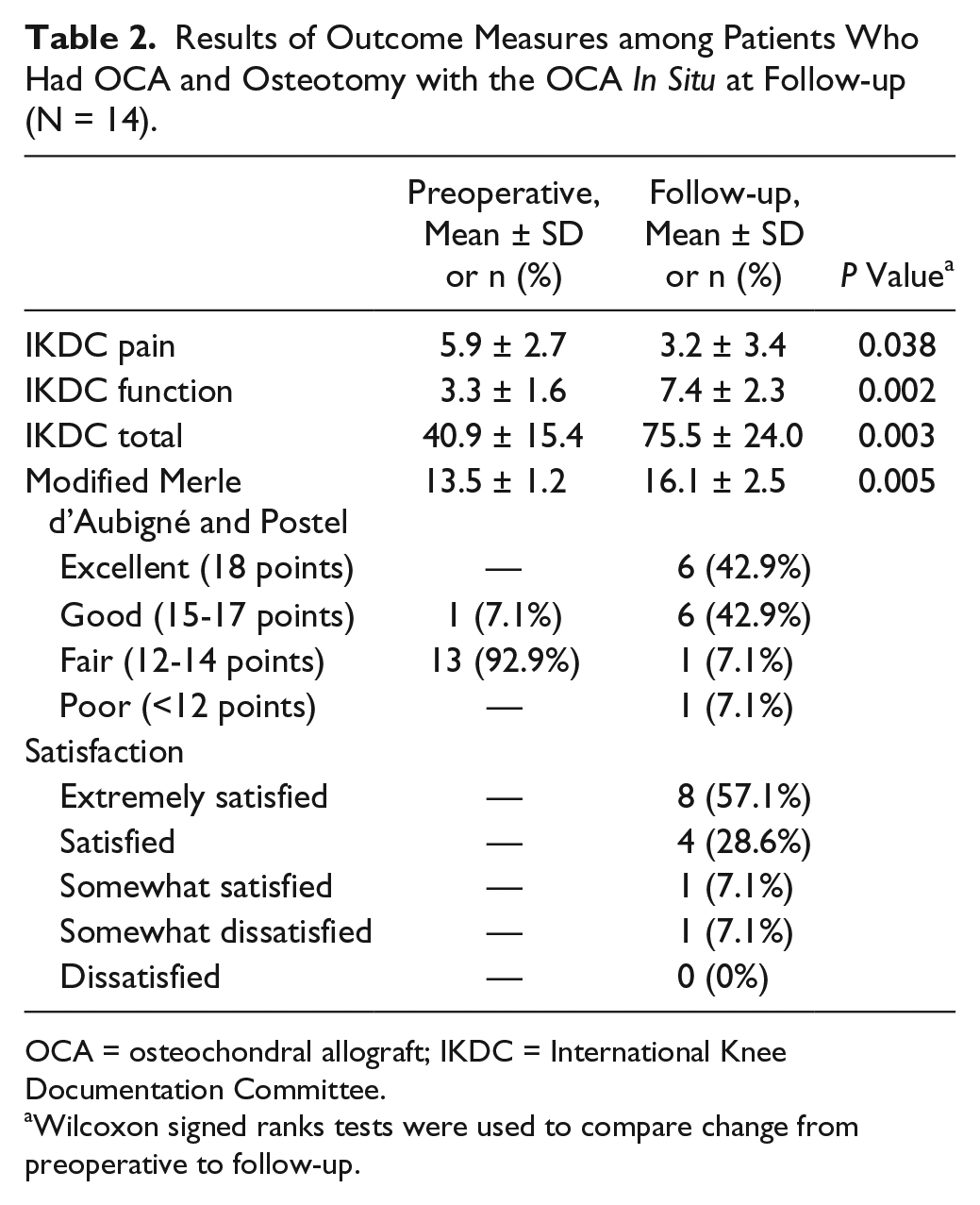
OCA = osteochondral allograft; IKDC = International Knee Documentation Committee.
Wilcoxon signed ranks tests were used to compare change from preoperative to follow-up.
Discussion
In this study, we have reported a case series of HTO and OCA in a combined procedure for patients with varus malalignment and focal osteochondral lesion of the knee. Overall survival and patient satisfaction of the combined procedure was high at midterm follow-up. Two patients were considered failures at mean follow-up of 9.3 years. Hardware removal was performed in 5 other patients in surgery unrelated to the allograft. Patients with grafts in situ at most recent follow-up had significant improvement in pain and function postoperatively, with an average 33 point improvement on IKDC score (P < 0.01).
Fresh OCA transplantation in particular has established itself as a versatile and reliable technique for the treatment of chondral and osteochondral lesions.6,9,14,22-24 In a systematic review of clinical outcomes, Chahal et al. 25 reviewed 19 studies, including 644 knees with a mean follow-up of 58 months. They reported patients had an overall satisfaction of 86% and an 18% failure rate of the OCA. 12
The use of osteotomy alone has been a successful procedure in the treatment of osteoarthritis. Survivorship has been shown to be as high as 98% at 10-year follow-up and 70% at 20-year follow-up. 26 Utilization of high tibial valgus osteotomy alone does not address large osteochondral lesions, and in some patients adjunctive cartilage repair may be desirable in association with an osteotomy.
In a clinical and histologic study of failed fresh OCA, Oakeshott et al. 27 observed a greater number of failures in grafts that were placed in compartments that had increased stress concentrations due to mechanical malalignment. Their histologic study showed that grafts subjected to higher forces led to a delay in revascularization, creeping substitution, and additional loss of articular cartilage. In our study, we individualized the indication for osteotomy with cartilage procedures with no need to use quantified measures as a criteria to indicate the HTO in association with OCA. Osteotomy was performed when axial alignment was overloading the affected compartment, in order to decrease stress concentrations due to mechanical malalignment. The aim of the correction with the osteotomy was individualized based on patient parameters such as age, extent of cartilage disease, and deformity. Patients with small cartilage lesions had their alignment corrected to neutral. In a situation where medial compartment degenerative disease existed, the mechanical axis was corrected a few degrees beyond neutral alignment, overcorrecting it to the lateral tibial eminence in order to slightly shift the axial alignment to the lateral compartment of the knee.
Numerous cartilage repair procedures have been reported with high tibial valgus osteotomies for the treatment of chondral and osteochondral lesions of the knee, including microfracture, autologous osteochondral transplantation, autologous chondrocyte transplantation, and stem-cell therapy.28-35 These cartilage repair procedures may not be optimal for large cartilage lesions and some are not available to surgeons worldwide.29,31,34,36 The treatment of small and medium-size chondral lesions was reported by Minzlaff et al. 32 on a group of 86 patients who underwent osteochondral autologous transfer combined with valgus HTO. Mean defect size measured intraoperatively 21.5 ± 9.3 mm in diameter. The mean follow-up was 7.5 years with mean survival rates of 95.2 ± 2.7% at 5 years, 93.2 ± 3.3% at 7 years, and 90.1 ± 4.4% at 8.5 years after surgery. Using the Lysholm score for knee function they also observed a significant increase (from 40 to 73) following surgery and improvements in pain intensity. A systematic review performed by Harris et al. 37 compared survival and clinical outcome of isolated HTO and combined biological knee reconstruction showing that HTO combined with articular cartilage surgery had significantly greater survival than isolated HTO. This systemic review confirmed that adding a cartilage repair procedure to the osteotomy improves the outcome in selected patients.
Few studies have reported the outcome of OCA associated with HTO for large lesions in a long-term follow-up. Raz et al., 15 evaluating distal femoral fresh OCAs outcomes in a long-term follow-up, reported 62% of associated osteotomies in their patients. In 64% of these cases a high tibial closing-wedge osteotomy was performed and graft survival rate of 91% at 10 years, 84% at 15 years, and 69% at 20 years. In this series we obtained a significant improvement in outcome scores at follow-up, with an average 33-point improvement on IKDC score (P < 0.01). The overall survival of the combined allograft and HTO procedure was 88% at 8.1 years. We followed our patients with clinical evaluations and plain radiographs of the knee to assess healing of the allograft and osteotomy. We did not performed magnetic resonance imaging (MRI) studies at follow-up in our patients because some studies showed a lack of correlation between MRI imaging and clinical results in allografts.38,39 The presence of the osteotomy plate generates metal-induced artifacts on MRI, decreasing the reliability of results with this exam. 40
Whether or not a concomitant osteotomy surgery with allograft transplantation leads to a significantly increased risk of complications is unclear. Inherent risks and complications are associated with each procedure individually. The complications of osteotomy surgery alone are well documented.7,41,42 Most studies report a low complication rate including broken hardware, wound complications, nonunion, infections, fractures, and hardware irritation. In our study, 5 patients (29%) required an additional procedure involving hardware removal. Hardware removal is commonly performed after osteotomy surgery with one study reporting the rate of hardware removal as high as 60%. 43
A theoretical risk of a simultaneous osteotomy and OCA transplantation is compromise to the endosteal and periosteal vascular supply to the bone surrounding the graft, which could potentially compromise graft healing when juxtaposed to the implanted graft. In this study, only one graft (medial tibial plateau) was on the same bone as the osteotomy. Therefore, whether the combined procedure on the same side of the joint (i.e., femoral osteotomy and femoral allograft) would have the same outcome is unclear. Osteotomy exposure requires additional planning of surgical incisions and can lead to increased soft tissue complications. Concomitant osteotomy and osteochondral grafting may also require longer operating room time and predisposes the patient to increased blood loss; however, previous studies showed the association of osteotomies and additional procedures without an increase in complications rates.18,44 In this study, no complications arose directly from the additional osteotomy surgery. This limited data suggest that a simultaneous surgery is well tolerated with good clinical results and patient satisfaction.
This study had several limitations. First, the difficulty involved in obtaining clinical follow-up as the patients within the study group presented from a wide geographic distribution. Due to this difficulty, we chose end points that were obtainable by telephone, mail, or electronic mail. The modified Merle d’Aubigné-Postel score has been used since the 1980s, when no validated outcome scores were available and has not been validated for use in knee surgery. This scoring system has a simple score for pain and function that allows an intrasample comparison within the cohort. Second, we lacked long-term radiographic follow-up and could make no determinations about progression of disease. We did not attempt to measure postoperative alignment because in cases of cartilage repair and osteotomy the degree of correction is individualized with normalization of alignment often a goal rather than the overcorrection most commonly employed when treating medial compartment arthritis. Nonetheless, radiographic evaluations may have provided an objective evaluation not captured by questionnaires. Third, we did not have a comparison group, which would include an allograft group with malalignment without concomitant osteotomy. A comparison group of this sort would have allowed for a better understanding of the benefits of osteotomy in long-term survival of grafts in allograft patients.
Treatment of young, high-demand patients with mechanical malalignment associated with cartilage injuries remains a challenging problem. This study shows that the use of osteotomy along with fresh OCA leads to predictably good and durable outcomes. The overall survivorship and clinical scores in these patients were as good as or better than those reported in other allograft or osteotomy studies. Use of simultaneous corrective osteotomy and OCA may delay the need for arthroplasty and restrictions associated with arthroplasty in young patients. We also demonstrated that the simultaneous surgery did not lead to additional complications. We conclude that combining opening wedge HTO and OCA for the treatment of large osteochondral lesions of the knee in properly selected patients is safe and effective.
Footnotes
Acknowledgment and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Scripps Office for the Protection of Research Subjects (IRB-13-6297)
Informed Consent
Written informed consent was obtained from all subjects before the study.