
Abstract
Purpose
To evaluate the clinical characteristics and global trends in the surgical treatment of articular cartilage defects.
Methods
Studies in English published between January 1, 2001 and December 31, 2020 were retrieved from MEDLINE, WOS, INSPEC, SCIELO, KJD, and RSCI on the “Web of Science.” Patient data were extracted, including age, sex, defect location and laterality, duration of follow-up and symptoms, and body mass index (BMI). Data were further stratified according to the surgical method, lesion location, procedural type and geographical area, and time period. A comparative analysis was performed.
Results
Overall, 443 studies involving 26,854 patients (mean age, 35.25 years; men, 60.5%) were included. The mean lesion size and patient BMI were 3.51 cm2 and 25.61 kg/m2, respectively. Cartilage defects at the knees, talus, and hips affected 20,850 (77.64%), 3,983 (14.83%), and 1,425 (5.31%) patients, respectively. The numbers of patients who underwent autologous chondrocyte implantation, arthroscopic debridement/chondroplasty, osteochondral allograft (OCA), osteochondral autologous transplantation, and microfracture were 7,114 (26.49%), 5,056 (18.83%), 3,942 (14.68%), 3,766 (14.02%), and 2,835 (10.56%), respectively. European patients were the most numerous and youngest. North American patients had the largest defects. The number of patients increased from 305 in 2001 to 3,017 in 2020. In the last 5 years, the frequency of OCAs showed a greatly increasing trend.
Conclusion
Clinical characteristics and global trends in the surgical treatment of articular cartilage defects were revealed. The choice of operation should be based on the patient characteristics and defect location, size, and shape, as well as the patient’s preference.
Keywords
Introduction
The articular cartilage, an avascular tissue, functions to relieve interarticular pressure and provide a smooth lubricated surface between bones.1,2 Although movement of the articular cartilage does not cause pain under physiological conditions, repairing it is difficult, as its healing is limited. 3 Cartilage repair techniques are evolving, with established and emerging technologies being further developed.
Cartilage restoration has seen several innovations leading to the development of novel surgical techniques and modifications, including microfracture (MF) surgery, 4 osteochondral autologous transplantation (OAT),5,6 osteochondral allograft (OCA),7,8 autologous chondrocyte implantation (ACI),9,10 arthroscopic debridement/arthroscopic chondroplasty (AD/AC),11,12 stem cell transplantation (SCT),13,14 and materials transplantation (MT).15,16 However, these techniques have not been widely applied in clinical practice.
This study aimed to analyze the clinical characteristics of articular defects and cartilage repair in articles published over the past 20 years (2001-2020). By studying the different injury sites and sizes and various surgical methods, we aimed to provide clarification with sufficient data and a guide for choosing the appropriate surgical treatment for cartilage injuries.
Methods
Article Search Process
A literature search was performed on the Web of Science (WOS) databases—MEDLINE, WOS, INSPEC, SCIELO, KJD, and RSCI. The following search terms were used: (“cartilage” or “cartilages”) and (“injuries and wounds” or “wounds and injury” or “injury and wounds” or “wounds, injury” or “trauma” or “traumas” or “injuries, wounds” or “research-related injuries” or “injuries, research-related” or “injury, research-related” or “research related injuries” or “research-related injury” or “injuries” or “injury” or “wounds” or “wound”). We started the search in April 2021, but the WOS database did not show all data from 2021. Therefore, the publication date range was set from January 1, 2001 to December 31, 2020.
Exclusion and Inclusion Criteria
The inclusion criteria were as follows: (1) studies of patients with cartilage injuries; (2) studies of patients who underwent cartilage repair surgery; and (3) articles providing part of the relevant data. The exclusion criteria were as follows: (1) studies with less than 10 patients; (2) pilot studies, patents, review articles, meetings, case reports, abstracts, editorial materials, letters, books, retracted publications, reference materials, corrections, biographies, news reports, publications with expression of concern, data papers, data sets, and early access studies; (3) articles not discussing clinical surgery; and (4) studies where the mean and variance were not provided or could not be estimated.
Data extraction
Total Data
The demographic data of patients, including age; sex; defect area, location, and laterality; follow-up time; duration of symptoms; and body mass index (BMI), were extracted. The sample size, average value, and variance were computed for all data. All data were compiled in an Excel spreadsheet. Some articles did not provide the variance; hence, we referred to the literature to estimate the variance. We also calculated the mean and 95% confidence intervals (CIs).
Location of Lesions
The data were filtered according to the location of lesions (knees, talus, hips, shoulders, and elbows). For knee lesions, the proportion of lesions in the femoral, lateral, patellar, trochlear, and tibial regions was also calculated.
Methods of Surgical Repair
The data were divided according to the surgical method used in each study (MF, ACI, OCA, OAT, AD/AC, MT, and SCT), and the proportion of surgeries using each method was calculated.
Classification of Data According to Continents
We labeled the data according to the continent where the study was conducted (Asia, Europe, North America, South America, and Oceania).
Classification of Data According to Time Period
Excel was used to extract the publication date of each study. We determined the number of patients in the last 20 years and calculated the mean and 95% CIs in each year using StataSE software (StataCorp LP, College Station, TX). Line charts were then created to show the trends.
Statistical Analysis
StataSE software was used to calculate the mean and 95% CIs. Continuous variables are presented as mean ± standard deviation; categorical variables are presented as frequencies with percentages. When partial continuous variables were raw data, the calculation was transformed into means and standard deviations to show the results in a consistent format. When the mean or standard deviation was absent, it was estimated from the median, minimum, and maximum values. 17 Continuous variables were pooled by calculating the mean and 95% CIs, and dichotomous variables were pooled by calculating the proportion and 95% CIs.
Results
Search Results
A total of 23,056 articles were searched; 9,804 of them were excluded for not meeting the study type criterion, while 4,075 were excluded because they did not discuss the surgical treatment of cartilage injuries. After screening 5,729 full-text articles and 443 clinical articles were selected based on their titles and abstracts (
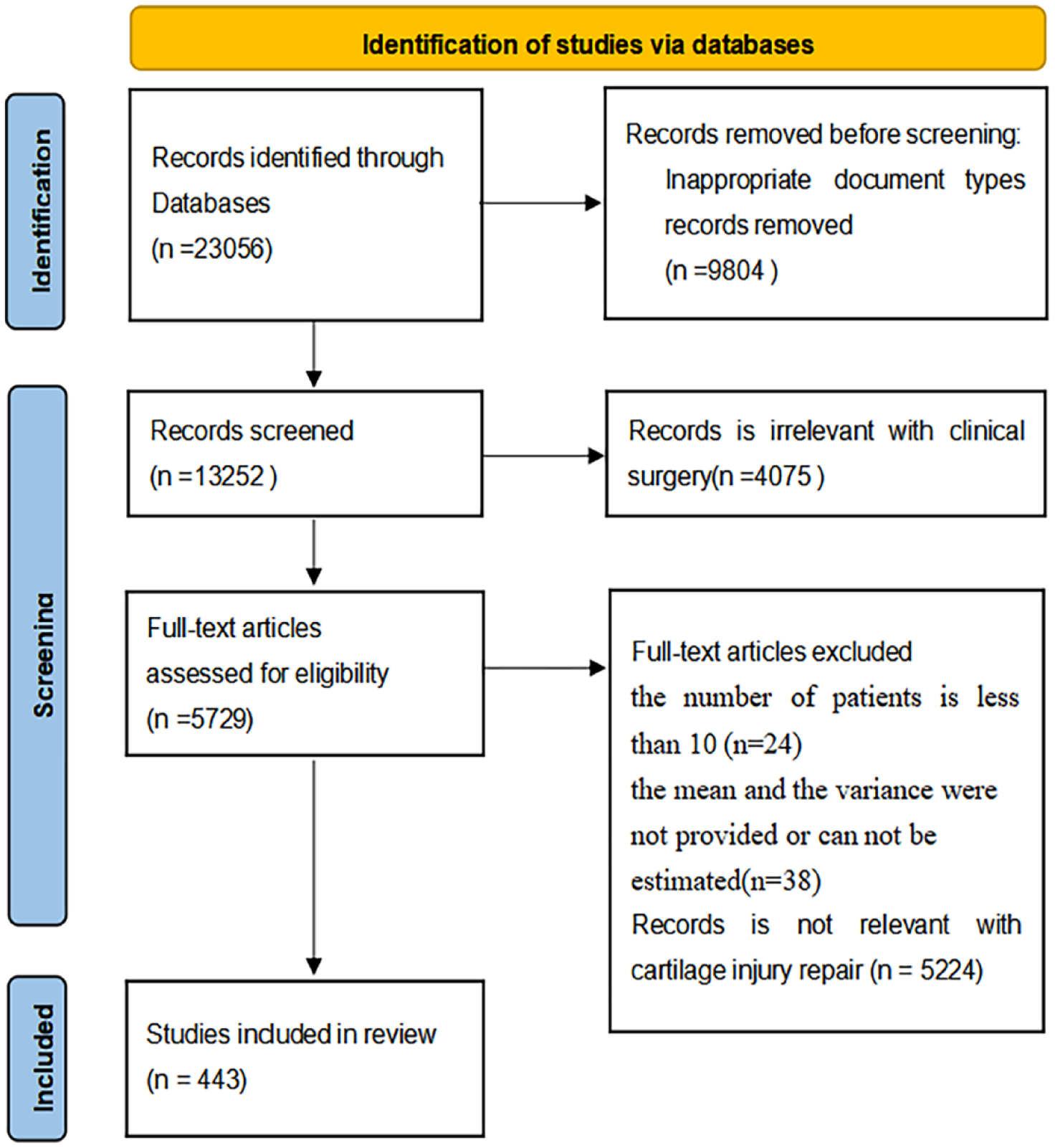
Search results according to the exclusion and inclusion criteria.
Total Data
The 443 articles involved 26,854 patients (mean age, 35.25 years; men, 60.5%) and had a mean follow-up duration of 58.51 months. The mean lesion size, BMI, and duration of symptoms were 3.51 cm2, 25.61 kg/m2, and 38.07 months, respectively. Left- and right-sided lesions comprised 45.1% and 54.9%, respectively.
The numbers of patients with lesions of the knees, talus, hips, elbows, and shoulders were 20,850 (77.64%), 3,983 (14.83%), 1,425 (5.31%), 426 (1.59%), and 107 (0.40%), respectively; 63 (0.23%) lesions were located at other sites.
The numbers of patients who underwent ACI, AD/AC, OCA, OAT, MF, MT, and SCT were 7,114 (26.49%), 5,056 (18.83%), 3,942 (14.68%), 3,766 (14.02%), 2,835 (10.56%), 1,819 (6.77%), and 1,260 (4.69%), respectively; 1,062 (3.95%) patients underwent other types of surgeries.
Data According to the Location of Lesions
Knee
Overall, 318 articles including 20,850 patients (mean age, 35.84 years; men, 60.5%) with a mean follow-up duration of 69.04 months were selected (
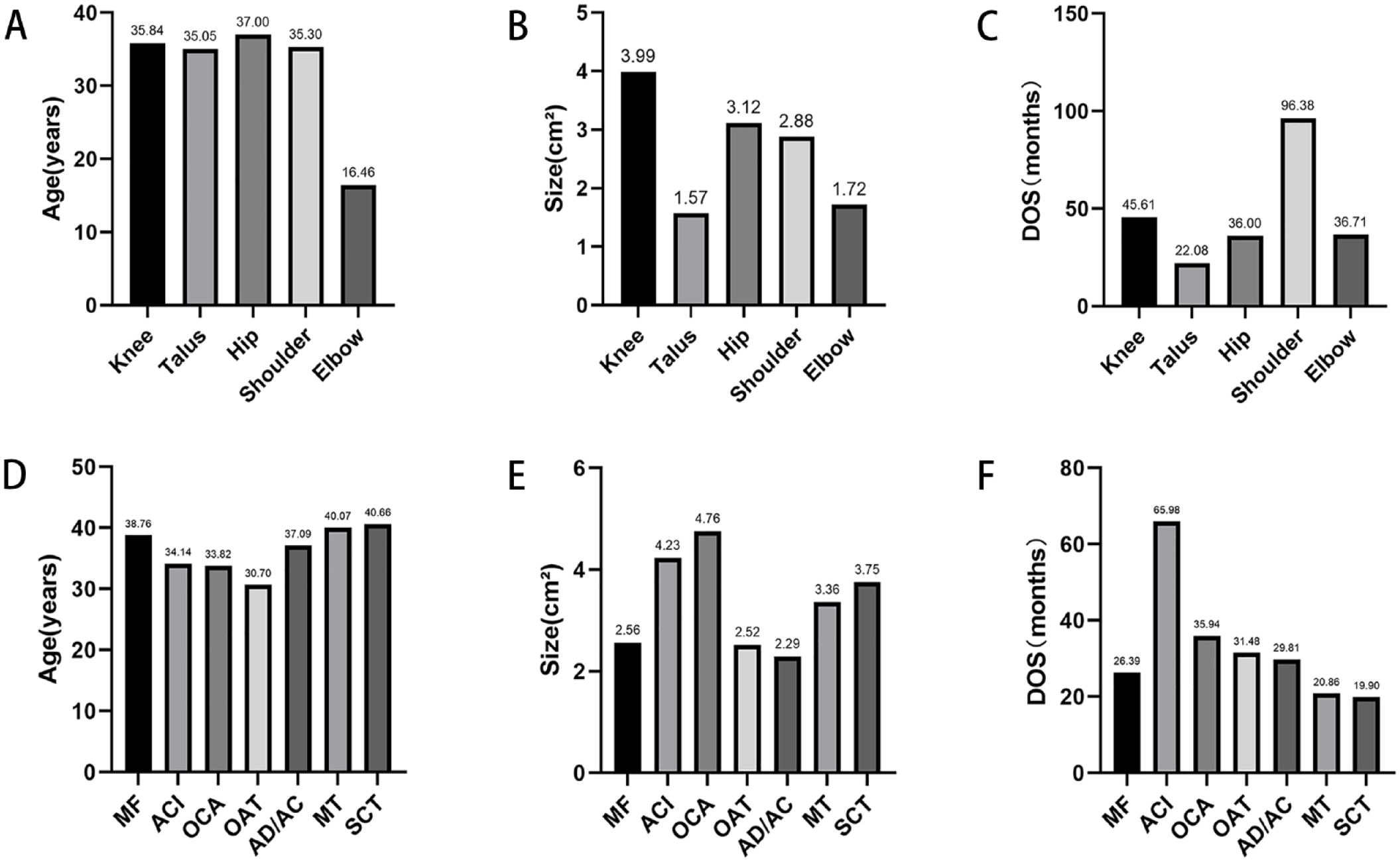
Clinical characteristics by the lesion site and surgical method. (
The numbers of patients with lesions in the femoral, lateral, patellar, trochlear, and tibial areas were 6,591 (60.79%), 2,431 (22.42%), 918 (8.47%), 704 (6.49%), and 198 (1.83%), respectively.
The numbers of patients who underwent ACI, AD/AC, OCA, OAT, MF, MT, and SCT were 6,725 (32.25%), 3,046 (14.61%), 3,485 (16.71%), 2,725 (13.07%), 1,795 (8.61%), 1,676 (8.04%), and 812 (3.89%), respectively.
Talus
Overall, 85 articles including 3,983 patients (mean age, 35.05 years; men, 61.2%) with a mean follow-up duration of 46.00 months were selected (
The numbers of patients who underwent ACI, AD/AC, OCA, OAT, MF, MT, and SCT were 250 (6.28%), 1,064 (26.71%), 295 (7.41%), 644 (16.17%), 817 (20.51%), 89 (2.23%), and 448 (11.25%), respectively.
Hips
Overall, 15 articles including 1,425 patients (mean age, 37.00 years; men, 56.3%) with a mean follow-up duration of 36.99 months were selected (
The numbers of patients who underwent ACI, AD/AC, OCA, OAT, MF, and MT were 139 (9.75%), 893 (62.67%), 123 (8.63%), 57 (4%), 159 (11.16%), and 54 (3.79%), respectively.
Shoulders
Overall, 7 articles including 107 patients (mean age, 35.30 years; men, 76%) with a mean follow-up duration of 44.17 months were selected (
Elbows
Overall, 15 articles including 426 patients (mean age, 16.46 years; men, 65%) with a mean follow-up duration of 46.17 months were selected (
Data According to the Method of Surgery
Microfracture
Overall, 69 articles including 2,835 patients (mean age, 38.76 years; men, 58.4%) with a mean follow-up duration of 61.78 months were selected (
The numbers of patients with lesions at the knees, talus, hips, shoulders, and metatarsus were 1,795 (63.32%), 817 (28.82%), 159 (5.61%), 51 (1.80%), and 13 (0.46%), respectively.
Autologous Chondrocyte Implantation
Overall, 143 articles including 7,114 patients (mean age, 34.14 years; men, 61.9%) with a mean follow-up duration of 68.66 months were selected (
The numbers of patients with lesions at the knees, talus, and hips were 6,725 (94.53%), 250 (3.51%), and 139 (1.95%), respectively.
Osteochondral Allograft
Overall, 68 articles including 3,942 patients (mean age, 33.82 years; men, 60.5%) with a mean follow-up duration of 59.31 months were selected (
The numbers of patients with lesions at the knees, talus, hips, shoulders, and elbows were 3,485 (88.41%), 295 (7.48%), 123 (3.12%), 19 (0.48%), and 20 (0.51%), respectively.
Osteochondral Autologous Transplantation
Overall, 92 articles including 3,766 patients (mean age, 30.70 years; men, 65.7%) with a mean follow-up duration of 50.19 months were selected (
The numbers of patients with lesions at the knees, talus, hips, shoulders, elbows, navicular bone, metatarsus, and wrist were 2,725 (72.36%), 644 (17.10%), 57 (1.51%), 15 (0.40%), 275 (7.30%), 37 (0.98%), 9 (0.24%), and 4 (0.11%), respectively.
Arthroscopic Debridement/Arthroscopic Chondroplasty
Overall, 40 articles including 5,056 patients (mean age, 37.09 years; men, 54.6%) with a mean follow-up duration of 47.30 months were selected (
The numbers of patients with lesions at the knees, talus, hips, shoulders, and elbows were 3,046 (60.25%), 1,064 (21.04%), 893 (17.66%), 22 (0.44%), and 31 (0.61%), respectively.
Materials Transplantation
Overall, 49 articles including 1,819 patients (mean age, 40.07 years; men, 59%) with a mean follow-up duration of 60.11 months were selected (
Stem Cell Transplantation
Overall, 22 articles including 1,260 patients (mean age, 40.66 years; men, 59.6%) with a mean follow-up duration of 51.96 months were selected (
Data According to Different Continents
Asia
Overall, 78 articles including 4,677 patients (mean age, 38.65 years; men, 54.6%) with a mean follow-up duration of 41.61 months were selected (
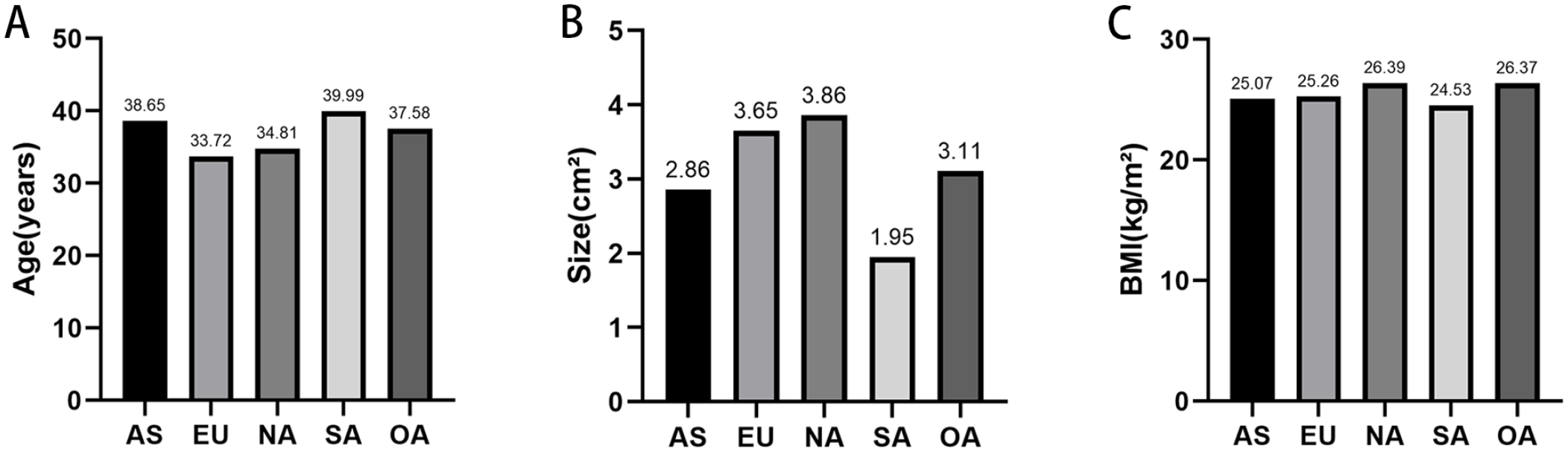
Clinical characteristics by continent. (
The numbers of patients who underwent MF, AD/AC, OAT, SCT, MT, ACI, OCA, and other techniques were 1,186 (25.36%), 1,170 (25.02%), 625 (13.36%), 560 (11.97%), 413 (8.83%), 363 (7.76%), 80 (1.71%), and 280 (5.99%), respectively.
Europe
Overall, 215 articles including 11,955 patients (mean age, 33.72 years; men, 63%) with a mean follow-up duration of 68.46 months were selected (
The numbers of patients who underwent MF, AD/AC, OAT, SCT, MT, ACI, OCA, and other techniques were 1,128 (9.44%), 2,526 (21.13%), 2,289 (19.15%), 330 (2.76%), 1,051 (8.79%), 4,232 (35.40%), 150 (1.25%), and 249 (2.08%), respectively.
North America
Overall, 128 articles including 8,775 patients (mean age, 34.81 years; men, 60.3%) with a mean follow-up duration of 57.82 months were selected (
The numbers of patients who underwent MF, AD/AC, OAT, SCT, MT, ACI, OCA, and other techniques were 521 (5.94%), 1,219 (13.89%), 800 (9.12%), 362 (4.13%), 336 (3.83%), 1,403 (15.99%), 3,638 (41.46%), and 496 (5.65%), respectively.
South America
Overall, 5 articles including 187 patients (mean age, 39.99 years; men, 61.6%) with a mean follow-up duration of 33.45 months were selected (
The numbers of patients who underwent AD/AC, OAT, MT, and OCA were 100 (53.48%), 52 (27.81%), 19 (10.16%), and 16 (8.56%), respectively.
Oceania
Overall, 18 articles including 1,260 patients (mean age, 37.58 years; men, 62.7%) with a mean follow-up duration of 261.60 months were selected (
The numbers of patients who underwent AD/AC, SCT, ACI, OCA, and open surgery were 41 (3.25%), 8 (0.63%), 1,116 (88.57%), 58 (4.60%), and 37 (2.94%), respectively.
Data According to Different Time Periods
In the last 20 years, the peak age of patients was 39.45 years in 2020, and the mean patient age increased from 28.76 years in 2006 to 39.45 years in 2020.
The peak number of patients was 3,230 in 2019, and the number of patients increased from 305 in 2001 to 3,017 in 2020 (
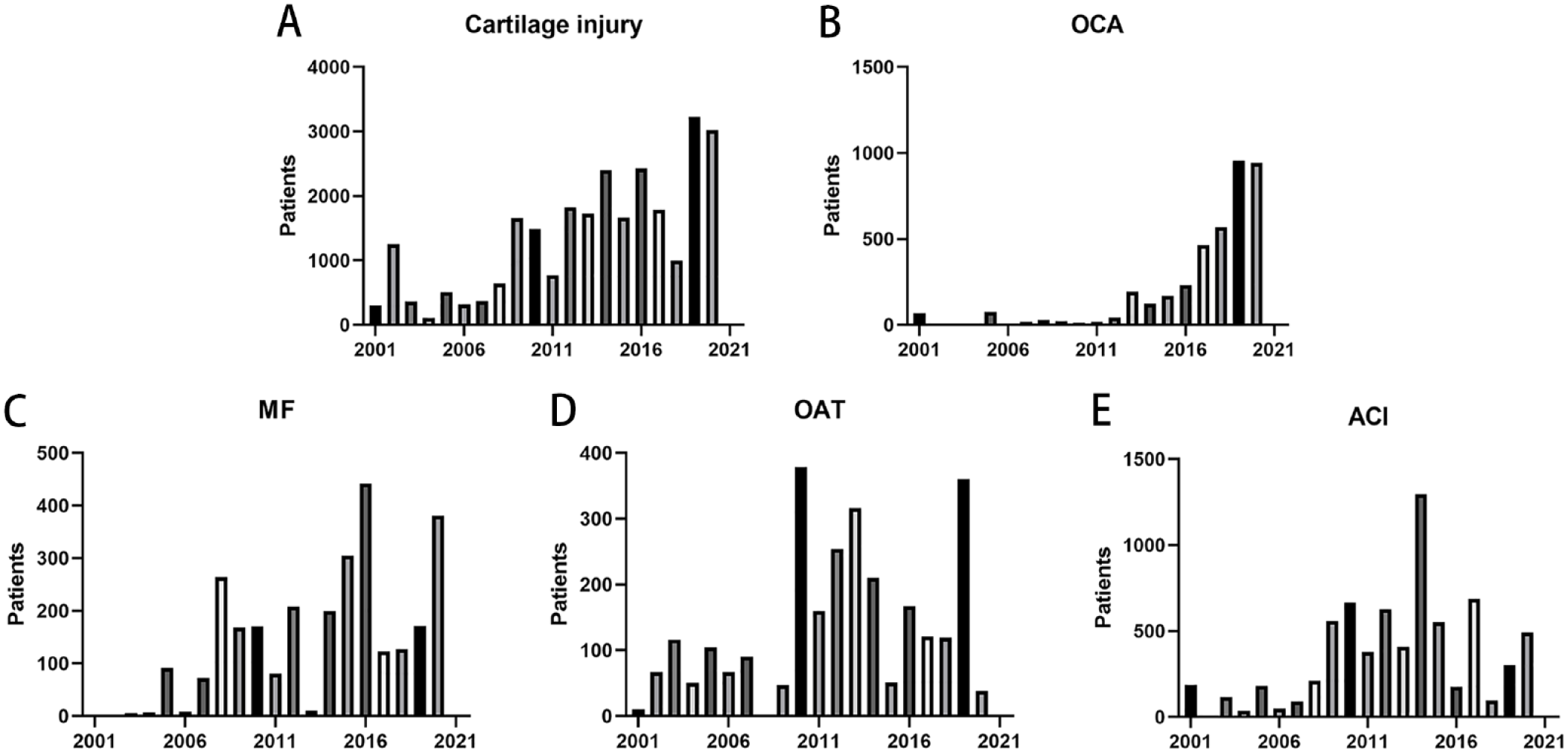
Annual numbers of patients with (
The peak number of patients who underwent knee surgery was 2,201 in 2020, up from 249 in 2001. The total number of patients who underwent talar surgery increased from 56 in 2001 to 515 in 2020. The number of Asian patients increased from 15 in 2002 to 1,006 in 2020. The total number of European patients increased from 47 in 2001 to 621 in 2020. The peak number of North American patients was 2,370 in 2019, and the number of patients increased from 258 in 2001 to 1,382 in 2020.
Discussion
Cartilage injuries are a challenge for both patients and clinicians. Patient characteristics; defect location, size, and shape; and patient preference cause different treatment selections. At present, each procedure for cartilage injury repair is superior in only a few clinical studies.18,19 ACI and OCA are widely used to repair cartilages in the knees, but they are rarely used in the talus and hips. Relatively speaking, AD/AC, MF, and OAT are still partially used in the talus and hips. Gobbi et al.20 reported that debridement or MF is often a first-line treatment for small chondral lesions, whereas chondroplasty achieves favorable outcomes when repairing chondral defects in the knees.20,21 Abolghasemian et al. recommended that OCA is an appropriate treatment for large lesions in young patients who need a higher quality of life postoperatively. 22
Patients in North America had the largest lesions. After stratification, patients who underwent OCA had the largest lesions, followed by those who underwent ACI. Meanwhile, OAT and MF were commonly performed for smaller lesions. The effect of the lesion size on the outcomes of cartilage repair has been well established in the existing literature; thus, treatment decisions should strongly consider the lesion size. Krych et al. reported that chondroplasty and OAT were appropriate for small (
The mean age of patients was 35.25 years; this increased from 34.32 years to 39.45 years in the last 5 years. Age plays a crucial but controversial role in cartilage repair, as it influences the degree of postoperative success. 25 The outcomes following cartilage repair in young people are better than in old people. Weber et al. also suggested that an older age was negatively correlated with postoperative patient-reported outcomes. 26 Middle-aged patients also reportedly have inferior clinical outcomes compared with younger patients. 27 Therefore, patients with cartilage injuries should be treated early to achieve better outcomes.
In our study, the BMI at the time of surgery was 25.61 kg/m2, suggesting that almost all patients with cartilage injury are overweight. Hence, we speculated that excess weight may increase the risk of cartilage degeneration or damage. Jaiswal et al. observed that patients with a standard BMI exhibited a continued improvement in the modified Cincinnati scores during the 2-year study period, whereas patients with obesity (BMI >30 kg/m2) demonstrated no improvement. 28 Losing weight can reduce medial cartilage volume loss and improve knee symptoms, whereas excess body weight has the opposite effect.29,30
Overall, our study observed a decline in ACI and an increase in OCA. However, the two surgical procedures that were often used to treat large cartilage defects were the ACI and OCA, and the mean lesion size of patients was 4.23 and 4.76 cm2, respectively. Sochacki et al. 31 reported that the reoperation rate was significantly higher after index ACI compared with OCA (67.6% vs. 40.4%, P < 0.0001). In addition, the total 2-year cost was significantly higher in the ACI group compared with the OCA group ($56,578 vs. $33,426, P < 0.0001). This increased cost is likely due to the increased reoperation rate following ACI compared with OCA. This appears to affect the decision regarding surgical methods for patients and surgeons alike. Moreover, in the study of Minas et al., 32 ACI in patients with a history of previous marrow stimulation techniques (MSTs) demonstrated a higher failure rate. Defects that had been pretreated with MST showed a failure rate of 26%, compared with a failure rate of 8% in nontreated defects. 33 Based on these studies, OCA seems to be the most reliable treatment for a failed MST. 34 Furthermore, one obvious limitation to ACI is that it involves two surgeries, while OCA is a single-stage procedure and can achieve precise articular surface congruity. In addition, with OCA, patients exhibit rapid subchondral bone healing with restoration of a hyaline or hyaline-like cartilage matrix. 35
Limitations
There were several limitations to our study. The study analyzed articles published over the past 20 years (2001-2020), but the article was finished in 2022. The retrospective design may cause some patients and information to be missed during data collection. Some articles did not provide variances, and we referred to the literature to estimate the variance; this may affect the validity of the results. In addition, we only searched for articles in WOS databases, and this might affect results.
Conclusion
The choice of operation should be based on patient characteristics and the defect location, size, and shape, as well as the patient’s preference. OCA and ACI are typically used for larger cartilage defects, whereas OAT, AD/AC, and MF are used to treat small lesions. Small lesions are not strictly limited to less than 2 cm2, according to the results of our study. ACI is the most commonly performed surgery, and the application of the OCA procedure has increased significantly in the last 5 years. The most common site of cartilage injury is the knee. The United States and European countries perform most cartilage repair procedures.
Supplemental Material
sj-docx-1-car-10.1177_19476035231205695 – Supplemental material for Treatment of Articular Cartilage Defects: A Descriptive Analysis of Clinical Characteristics and Global Trends Reported from 2001 to 2020
Supplemental material, sj-docx-1-car-10.1177_19476035231205695 for Treatment of Articular Cartilage Defects: A Descriptive Analysis of Clinical Characteristics and Global Trends Reported from 2001 to 2020 by Zhiyuan Ren, Yang Liu, Yongsheng Ma, Lingan Huang, Xueding Wang, Qitai Lin, Yugang Xing, Wenming Yang, Wangping Duan and Xiaochun Wei in CARTILAGE
Footnotes
Acknowledgments and Funding
The authors would like to thank Editage (![]() ) for English language editing. One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the National Natural Science Foundation of China (grants U21A20353 and 82172503), the Central Government Guides Local Science and Technology Development Funds (grant YDZJSX2022B011), and the Key Research and Development Program of Shanxi Province (grant 201903D421019).
) for English language editing. One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the National Natural Science Foundation of China (grants U21A20353 and 82172503), the Central Government Guides Local Science and Technology Development Funds (grant YDZJSX2022B011), and the Key Research and Development Program of Shanxi Province (grant 201903D421019).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.