
Abstract
Objective:
Mechanical alignment of the lower limbs has been suggested to cause abnormal uneven loading across the compartments at the knee, but its contribution to the initiation and progression of arthritis remains controversial. This study aimed to establish whether malalignment of the lower limb after trauma is associated with worsened arthritis scores in the theoretically overloaded compartment, and if arthritis scores continuously correlate with the degree of malalignment and time with deformity.
Design:
After screening 1160 X-rays, 60 patients were identified with long-leg radiographs > 2 years after fracture. Measurement of mechanical axis deviation (MAD) divided into groups of varus malalignment (n = 16, >16 mm), valgus (n = 25, <0 mm), and normal alignment (n = 19). Alignment and bilateral knee compartmental arthritis scores were recorded by three clinicians, compared via analysis of variance and assessed with linear regression against time since injury using MAD as a covariate.
Results:
In varus and valgus malalignment, there was a greater mean arthritis score in the “overloaded” compartment compared to the contralateral side, with varus medial Osteoarthritis Research Society International (OARSI) scores 5.17 ± 2.91 vs 3.50 ± 2.72 (P = 0.006) and Kellegren-Lawrence scores 2.65 ± 1.19 vs 1.79 ± 1.24 (P ≤ 0.001). In a linear regression model, OARSI arthritis score was significantly associated with absolute MAD (0.6/10 mm MAD, P < 0.001) and time (0.7/decade, P ≤ 0.001).
Conclusions:
Malalignment consistently results in more advanced arthritis scores in the overloaded compartment, most likely related to abnormal loading across the knee. Severity of arthritis using OARSI grading continuously correlates with degree of malalignment and time with deformity after post-traumatic malunion.
Introduction
Although perhaps intuitively obvious and widely accepted in principle by clinicians, the contribution of lower limb coronal plane malalignment to degenerative arthritis in the knee remains controversial. It has proven difficult to objectively document this relationship, despite this, in clinical practice it is generally accepted that malalignment may increase the risk of arthritis by altering the distribution of the mechanical load across the knee. 1 In the setting of limited evidence, acceptable limits of lower limb fracture angulation or malalignment in relation to the potential risk of arthritis are not clearly defined.2,3 Nevertheless, use of corrective osteotomies to restore normal alignment has long been considered a routine practice by orthopedic surgeons.4,5
The established standard for clinical assessment of malalignment is long-leg standing radiographs. The mechanical axis of the limb should demonstrate collinearity of the hip, knee, and ankle—with a straight line from the center of the femoral head, to the center of the talus passing just medial to the center of the tibial spines (
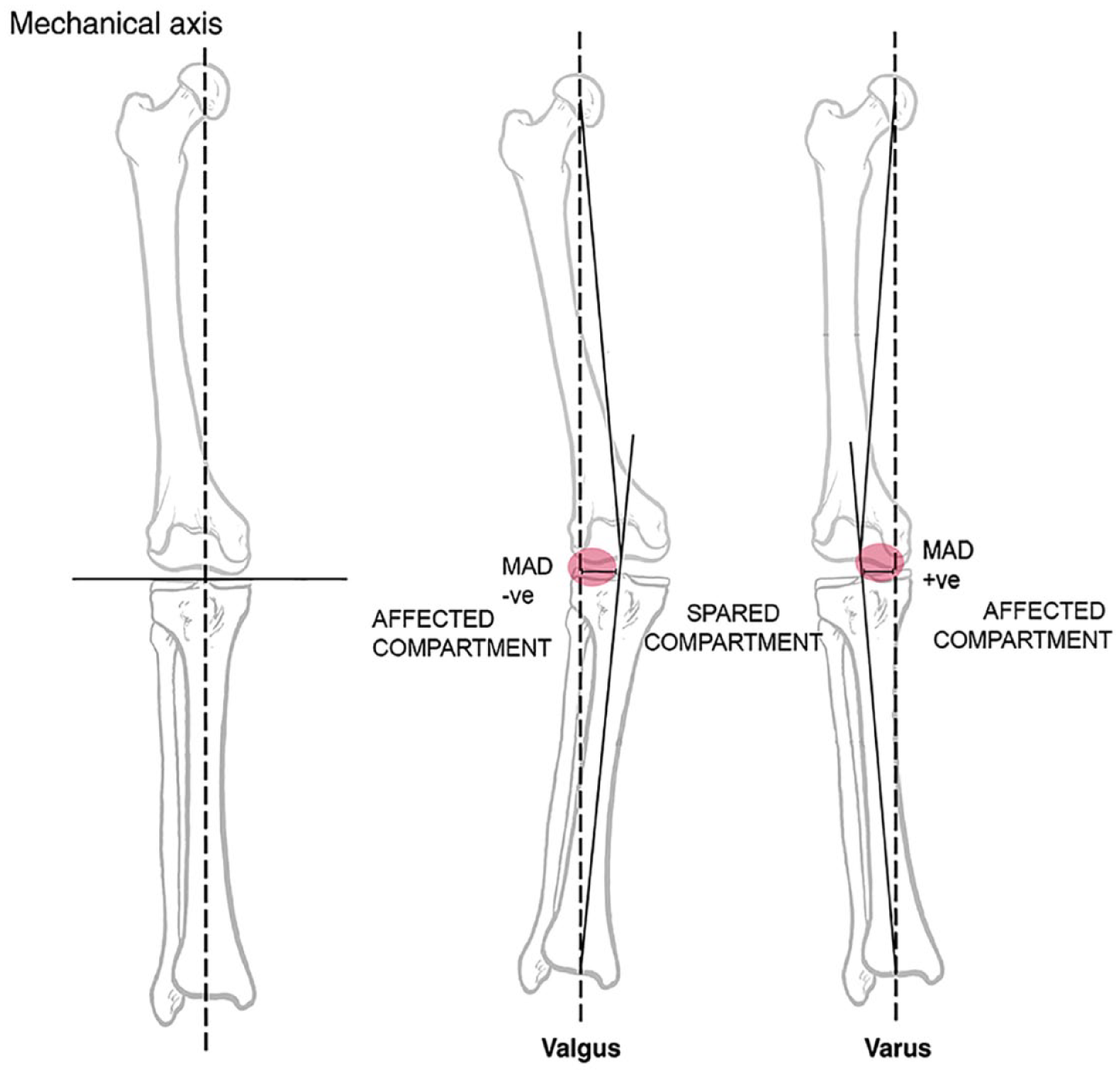
Mechanical axis in normal, valgus, and varus alignment. In valgus, there is negative MAD, and the theoretically affected compartment is lateral. In varus, there is positive MAD, and the theoretically affected compartment is medial. Obtained with permission from Merchant and Dietz (1989). 2 MAD = mechanical axis deviation.
The literature is complicated by varying interpretations of malalignment and its measurement, some of which could be considered flawed. In an influential paper, from a Framingham cohort study of 110 patients with incident osteoarthritis over 9 years compared to matched controls, Hunter et al. 11 suggested that alignment did not predict the onset of arthritis but was rather a marker of severity/progression. This proposition initiated a causation dilemma that has perpetuated in the literature, reinforced in Hunter et al. 12 as well as subsequent reviews.13,14 The alignment was only measured locally on short leg films at the knee, measuring the anatomical tibiofemoral axis and measures of joint orientation. There is ample evidence that even significant fracture malunion and angulation can be well tolerated and may not predictably lead to arthritis, but the key factor of overall limb alignment has consistently been overlooked.2,3,15 It is absolutely critical to recognize the contribution of translation as an additional element of deformity, and that this can be considered either aggravating or compensatory with respect to the alignment of the limb.4-6 The putative relationship between malalignment and osteoarthritis, specifically after malunion, has not yet been fully investigated, acknowledging several of the relevant key studies may be considered fundamentally flawed. The primary aims of this study were therefore to determine: if malalignment of the lower limb (from extra-articular deformity after trauma) is associated with worsened arthritis scores in the theoretically overloaded compartment, and, does the severity of asymmetric unicompartmental knee arthrosis correlate with the degree of malalignment and time from the onset of deformity?
Methods
This was a retrospective cohort study of patients with post-traumatic malunion and resulting malalignment at a major metropolitan tertiary referral medical center. The unaffected contralateral limb acts as a case control for comparison, negating many of the common confounding factors in cohort studies for arthritis. There is another control group of patients with normal alignment after fracture. The study was approved by the institutional ethics committee (Metro North Health HREC/17/QRBW/495), with a waiver for consent to access retrospective data.
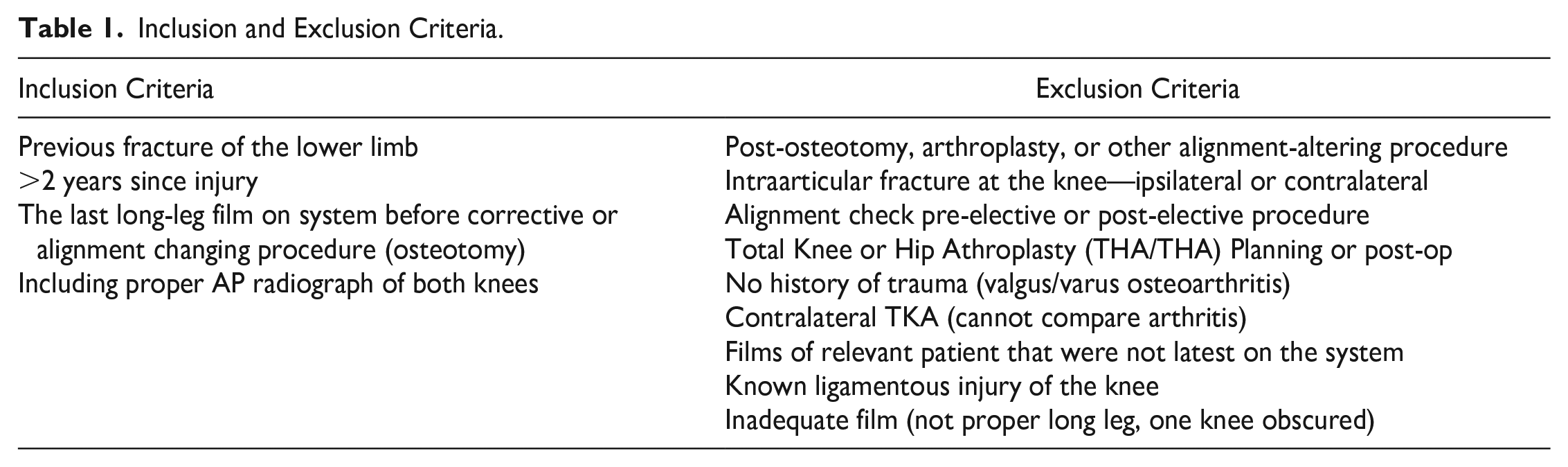
The digital radiograph archives of our institution were searched to identify all long-leg standing films in adults spanning a 10-year period, 1160 long-leg films and reports were identified and assessed. These studies were performed in a standardized anteroposterior fashion from 3 meters, with patients bearing weight equally on both lower extremities. Patients were included only if they were >2 years after lower limb long-bone fracture, with varus malalignment defined as MAD >16 mm, valgus malalignment defined as <0 mm (from neutral) and a normal alignment (0-16). All patients were excluded with confounding ipsilateral or contralateral injuries that might affect alignment or contribute to arthritis; patients with intra-articular fractures, those with ligamentous instability, and evidence of meniscal pathology were excluded. Only 89 patients met inclusion for closer review (
Table 1
); after further detailed review 29 of these were <2 years since injury, and 60 cases were selected for complete analysis (
Inclusion and Exclusion Criteria.
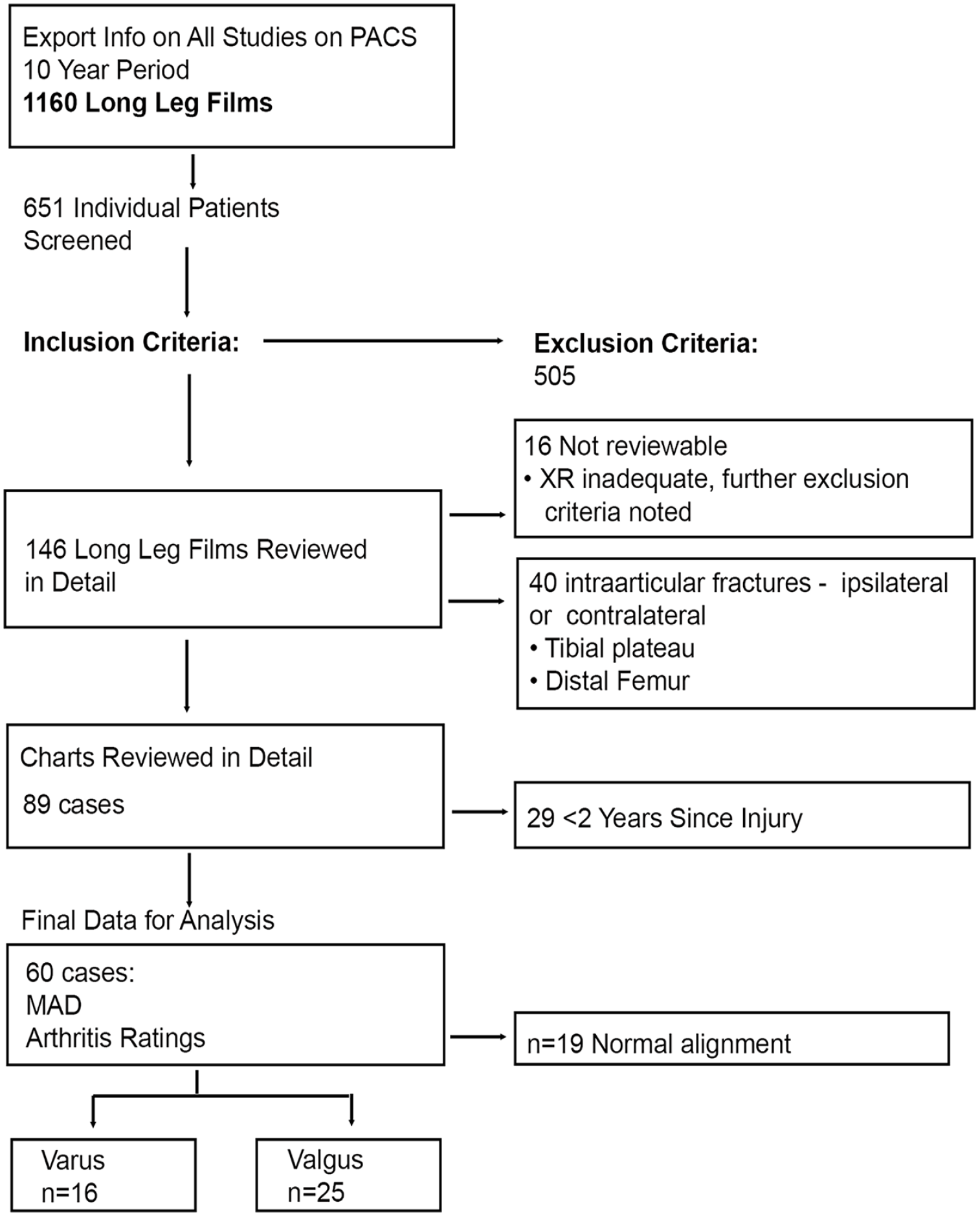
Flow chart of case identification. MAD = mechanical axis deviation.
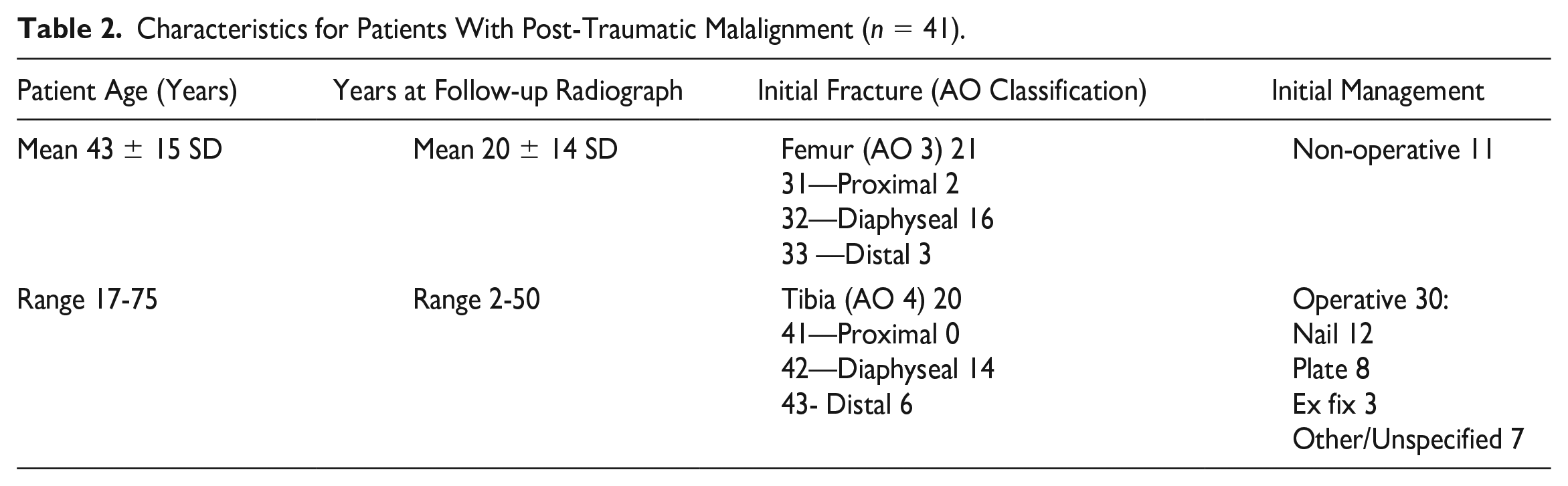
The latest available radiographs for each patient were used, and time since injury recorded. Using the tools native to the Inteleviewer Picture Archiving and Communications System (PACS; Interlad Medical Systems, Montreal, Canada), three independent trained reviewers measured the parameters of limb alignment and joint orientation in each radiograph according to widely accepted methods.4-6 Radiographic arthritis severity in both the medial and lateral tibiofemoral compartments was graded by the same three independent reviewers using the Osteoarthritis Research Society International (OARSI), and Kellegren-Lawrence (KL) scores as primary outcomes; to limit the risk of observer bias, this assessment of the severity of radiographic arthritis was performed absolutely blinded to overall alignment of the limb, using cropped images isolating the views of each knee independently. The Brandt and International Knee Documentation Committee (IKDC) methods were included with slight variations which were considered in secondary sensitivity analyses. The OARSI score is a comprehensive arthritis rating system that may better track arthritis progression (A more detailed description of the specific methods and reference OARSI atlas provided to raters is submitted in the supplemental material). Patient characteristics are provided in Table 2 . The cases were almost all high energy trauma, with motor vehicle accident the most common cause, and other causes including vehicle versus pedestrian or falls from height. The cases were 2:1 male to female. Where available, the detailed AO fracture classification exhibited simple (44%), wedge (15%), and multifragmentary (41%) patterns, of which a quarter were intact segmental and three-quarters comminuted. Other potentially relevant data, body mass index (BMI), smoking status, knee range of motion, and sagittal plane deformity were not reliably documented in the retrospective dataset and could not be included in analysis.
Characteristics for Patients With Post-Traumatic Malalignment (n = 41).
After stringent inclusion and exclusion criteria were applied, the final cohort included 41 patients with post-traumatic malalignment, compared to their matched contralateral side resulting in 82 limbs. This was divided into pairs of varus (n = 16) and valgus knees (n = 25). The cohort with normal MAD (n = 19) was used as another separate control group for comparison.
Statistics
Statistical analysis was performed in R 4.0 (RStudio, Boston, USA). Analysis compared the arthritis grades OARSI and KL, in the theoretically affected (overloaded) or spared (unloaded) compartment to the same compartment in the contralateral limb, as well as comparing the other compartment in the same knee. Analysis was with the one-way analysis of variance (ANOVA) on linear regression results with the Tukey honestly significant difference test as a strategy to address multiplicity. The results were analyzed visually with scatter plots and trend lines. The association between OARSI arthritis grade and malalignment (MAD in mm) and time (years) was investigated with linear regression models, first without interaction of terms and subsequently with interaction of terms. To account for multiple measurements, a random effect was included in the linear models. The regression was done in R studio, formatting the data into long format, using the linear mixed model function for independent variables OARSI ~|MAD| +TIME+ as.factor(rater) +1|StudyID, and for interaction of terms OARSI ~|MAD| *TIME + as.factor(rater) + 1|StudyID. The threshold for statistical significance was P < 0.05 after addressing for multiplicity.
Results
The results of this study consistently demonstrated higher mean arthritis scores in the compartments that would be theoretically affected as a result of malalignment. With varus malalignment (n = 16), there was a greater mean arthritis score in the medial compartment compared to the contralateral medial compartment in the same individual. The OARSI scores were significantly greater 5.17 ± 2.91 SD vs 3.50 ± 2.72 (difference 1.67, 95% confidence interval [CI] = 0.37, 2.96; P = 0.006) and KL scores were 2.65 ± 1.19 SD vs 1.79 ± 1.24 (difference 0.85, 95% CI = 0.29, 1.41; P ≤ 0.001), as well as Brandt and IKDC ( Table 3 ). These results all support the prior proposition. The theoretically “spared” lateral compartment did also have higher arthritis scores compared to the contralateral knee, with significance for the primary measures (OARSI and KL), but not Brandt and IKDC ( Table 3 ). The difference in trends between “affected” and “spared” compartment scores is addressed subsequently.
Compartment Arthritis Score Comparisons in Varus Malaligned Knees (n = 16).
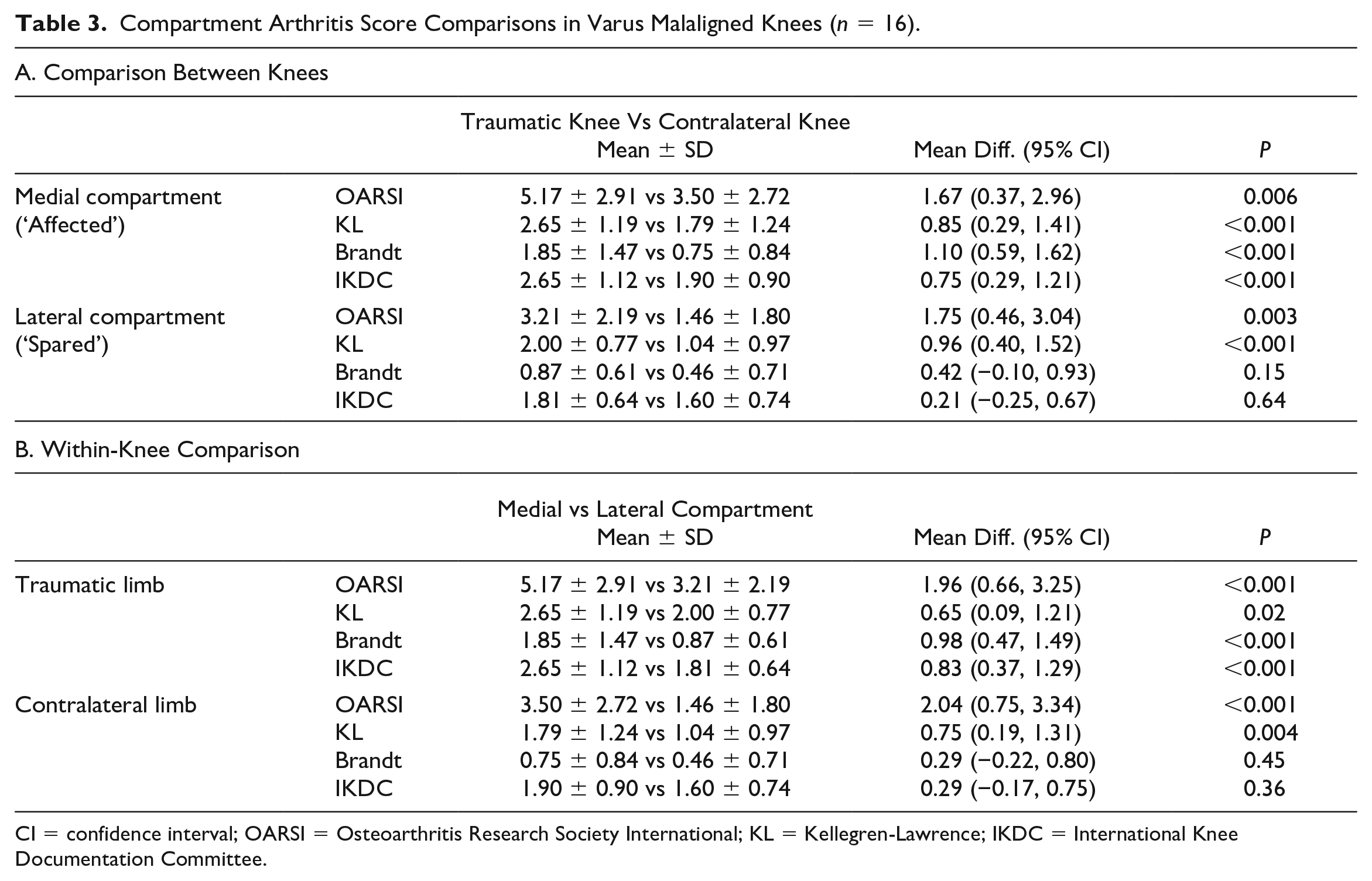
CI = confidence interval; OARSI = Osteoarthritis Research Society International; KL = Kellegren-Lawrence; IKDC = International Knee Documentation Committee.
In valgus malaligned knees (n = 25), a similar pattern was observed ( Table 4 ). The lateral compartment had significantly higher mean arthritis score across all grades OARSI scores were 2.44 ± 2.49 SD vs 1.55 ± 1.56 (difference 0.89, 95% CI = -0.01, 1.80; P = 0.05) and KL 1.51 ± 1.17 SD vs 1.03 ± 0.80 (difference 0.48, 95% CI = 0.05, 0.91; P = 0.02). Within the affected knee the mean lateral compartment arthritis score was higher than medial across all grading scores but confidence intervals included a potential for no discernible difference.
Compartment Arthritis score Comparisons in Valgus Malaligned Knees (n = 25).
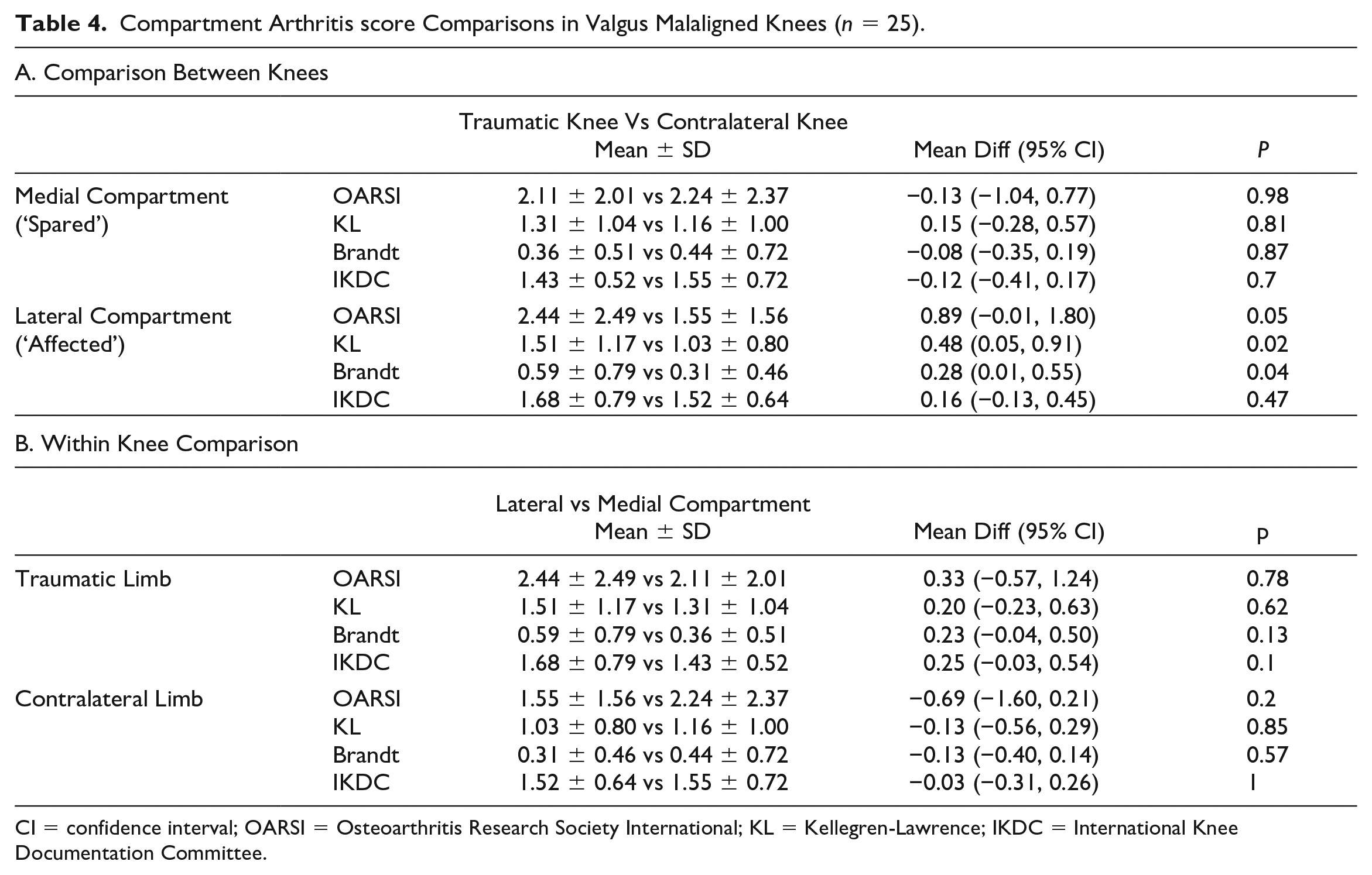
CI = confidence interval; OARSI = Osteoarthritis Research Society International; KL = Kellegren-Lawrence; IKDC = International Knee Documentation Committee.
Comparing the varus group to the group with normal MAD revealed significantly higher medial compartment arthritis in the varus group OARSI 5.17 ± 2.91 SD vs 2.61 ± 1.90 (difference 2.55, 95% CI = 1.31, 3.79; P ≤ 0.001) and KL 2.65 ± 1.19 SD vs 1.61 ± 1.01 (difference 1.03, 95% CI = 0.45, 1.61; P ≤ 0.001). The valgus group exhibited higher lateral compartment OARSI score compared to the normal MAD group that trended toward significance, OARSI 2.44 ± 2.49 SD vs 1.49 ± 1.58 (difference 0.95, 95% CI = -0.16, 2.06; P = 0.14) and higher KL 1.51 ± 1.17 SD vs 1.14 ± 0.93 (difference 0.37, 95% CI = -0.16, 0.89; P = 0.34).
There was statistical evidence for a correlation between severity of knee OARSI arthritis score and degree of deformity (MAD) and time with deformity. The results for all varus and valgus malaligned knees were combined by taking the absolute value of the MAD of the affected side and plotted (

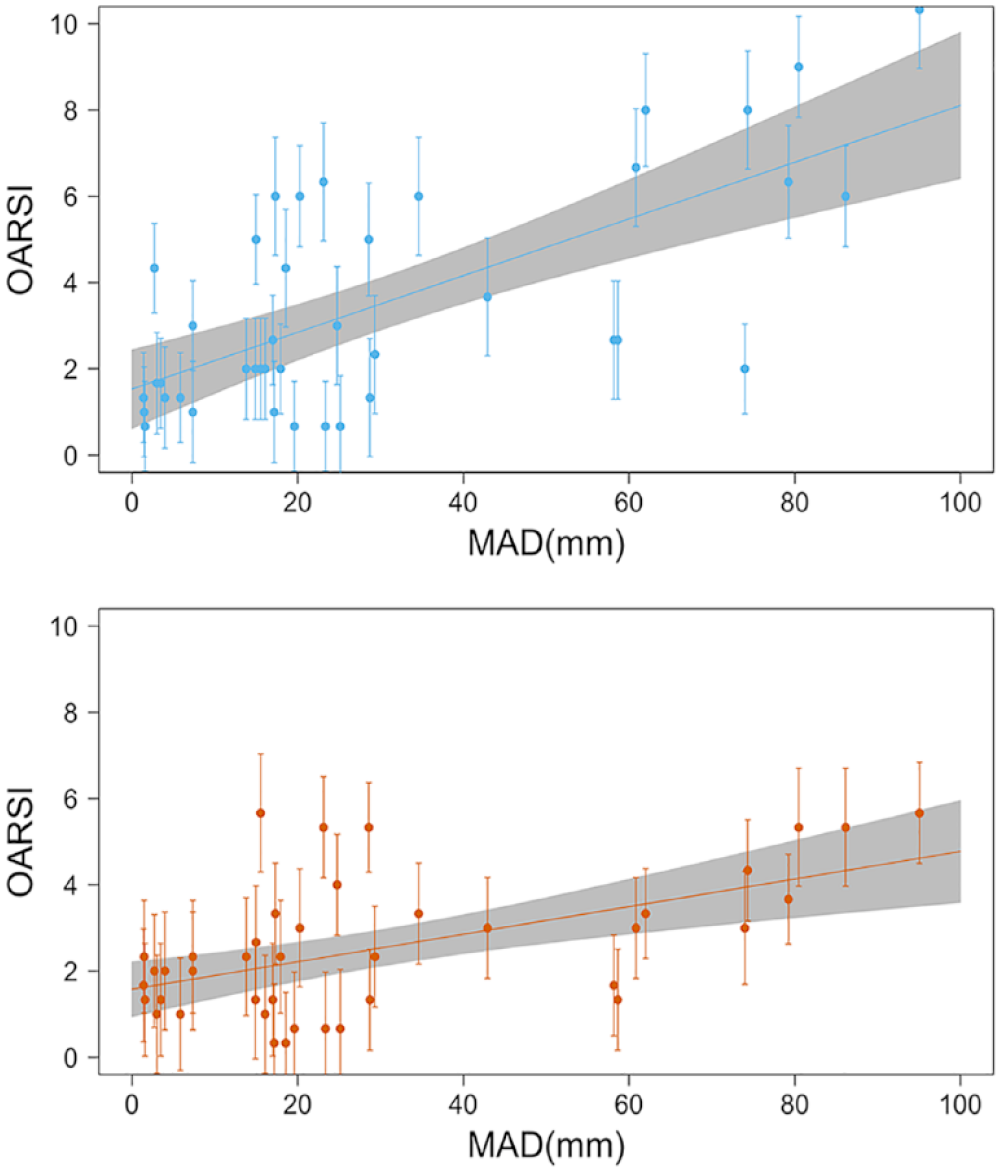
Comparison of OARSI arthritis grade (mean ± Standard Error of the Mean (SEM) for 3 reviewers) vs absolute MAD (mm) in affected compartment (blue) and theoretically spared (red). Trendlines with confidence interval (0.95). OARSI = Osteoarthritis Research Society International; MAD = mechanical axis deviation.
The OARSI arthritis score was clearly correlated with absolute MAD for the affected compartment with a regression coefficient of a=0.06 OARSI/mm|MAD| (SE
0.01; P <0.001) and with Time b=0.07 OARSI grades for every year since injury (SE 0.02, P = 0.01), the overall Rho was 0.77 and P < 0.001. In this study, only patients >2 years after injury were included, to ensure adequate time had elapsed to observe an effect; these results suggest that after that time for patients with malalignment, 0.6 OARSI grades in the affected compartment can be expected for every 10 mm axis deviation, with further deterioration of 0.7 grades per decade. The theoretically spared (unloaded) compartment was also positively correlated (Rho 0.43, P ≤ 0.001), but to a lesser degree with a =0.02 OARSI/mm|MAD| (SE 0.01; P = 0.002) and with less evidence for time 0.04 OARSI/year (SE 0.01, P = 0.003). A separate linear regression model with side (theoretically affected vs spared) as a factor demonstrated OARSI grade was positively correlated with MAD and was significantly greater in the theoretically affected compartment (blue) compared to the spared compartment (P ≤ 0.001).
A linear regression with interaction of terms was also considered, testing the interaction between malalignment (MAD) and time with deformity in relation to OARSI arthritis grade:

The independent variables (a = 0.02, SE = 0.01; P = 0.07) and b = 0.030, SE = 0.02, P = 0.10) had reduced contribution, but there was a significant effect (c = 0.0013, SE = 0.000, P = 0.004) for the terms with interaction, and the overall correlation was significant Rho 0.79 and P < 0.001. This model gives an alternative to the linear model without interaction, but is difficult to express as a simple generalization. The plotting of this linear model with interaction of terms, although based on a modest sample size, gives a rough guide to the effect of time and deformity to arthritis grade over time (
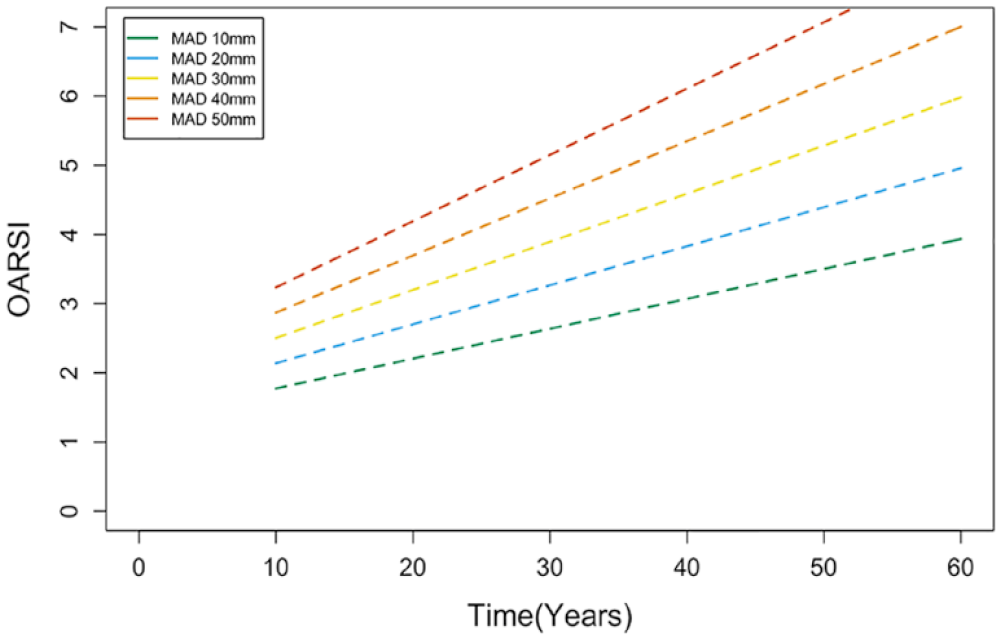
Line chart from results of a linear model with interaction terms that showed significant contributions of MAD and time with deformity to degree of osteoarthritis OARSI grade. MAD = mechanical axis deviation; OARSI = Osteoarthritis Research Society International.
The general correlation between OARSI rating for three reviewers 0.74-0.85 was good, and single score intraclass correlation (ICC) was moderate 0.63. Similarly, for KL correlation 0.73-0.80 and ICC 0.61. These correlations are similar to or better than those previously reported. 16
Discussion
The most important findings of this study all support the mechanical hypothesis, suggesting that the progression of post-traumatic degenerative arthritis is at least in part related to malalignment of the lower limb. The causes of arthritis are believed to be multifactorial, reflecting an interaction of genetic predisposition, environmental/sociodemographic factors, and internal joint pathology. 14 There is evidence to support contributions from the mechanical hypothesis from biomechanical, animal, and human studies. Biomechanical investigations have demonstrated varus/valgus deformity asymmetrically increases monolateral compartment joint pressure by 50%, 17 and rabbit studies have confirmed overloading and cartilage damage in the theoretically overloaded compartments. 18 Clinical studies of malunion have been less consistent, perhaps related to study design and flaws in the analysis of the associated deformities. 2
The results in this study of post-traumatic varus and valgus deformities demonstrated with clear confidence that malalignment was associated with more severe monocompartmental arthritis in the affected knee. The varus knees also demonstrated more advanced medial compartment arthritis compared to a post-traumatic cohort with normal alignment. In valgus knees, the lateral compartment exhibited more severe arthritis scores compared to the normal cohort, but this did not reach significance. This perhaps reflects the normal physiological alignment of the lower limb, in which the mechanical load still passes through the medial compartment, even when the limb is considered radiographically aligned resulting in higher rates of medial compartment degeneration. 19 The same angular malunion would cause a longer lever arm in varus malalignment than in valgus, and these results indicate that many of the patients had valgus malalignment magnitude <|16|mm. The normally higher rates of arthritis in the medial compartment makes it difficult to demonstrate a significant shielding effect. A power calculation was conducted to determine the sample size needed to detect as significant a difference as 0.95 OARSI score in the affected lateral compartment in valgus versus the normal group; the standardized effect size is 0.95 over 2.15 the pooled standard deviation 0.44. At a significance threshold of 0.05 and a desired power of 80%, a sample size of n = 64 in each group would be needed to detect an effect size of 0.44 standard deviations.
The past literature concerning clinical outcomes of arthritis following malalignment are inconsistent. An early study of 88 patients with tibial malunion at a mean of 8 years follow-up revealed greater radiographic degeneration of the knee with malalignment. 20 Among the 43 patients with malunion greater than 5 degrees, almost a third had developed arthritic changes at the knee. Palmu et al. 21 in 2013 conducted a long-term follow-up of pediatric femoral fractures, where almost half (21/52) healed with >10 degrees malunion. Subsequently, more than a third (6/15) of patients with long-term follow-up developed arthritis by the mean age of 32 years. In contrast, a follow-up of 64 femoral shaft fractures at an average of 22 years measured long-leg tibiofemoral angle using the Milner method to determine the malunion angle. 15 10/64 had >10 degrees malunion, and they reported 31 patients outside of normal mechanical axis (distribution and magnitude not specified). There were only 5/31 cases with ipsilateral osteoarthritis at follow-up, and this was not significantly associated with malalignment; however, a third of patients had mild symptoms that may suggest early degeneration.
In this study the severity of arthritis score was shown to correlate both with time since injury, and the degree of deformity, supporting the mechanical hypothesis. The linear model that intuitively supports an interaction of time and degree of deformity contributing to arthritis was used to make a line chart that can be used for reference (
There are three sources of deformity that can contribute to lower limb malalignment: extra-articular deformity of the femur, extra-articular deformity of the tibia, or internal joint deformity from ligamentous laxity or asymmetric cartilage loss. 24 In malalignment after malunion, the primary initial deformity is static and extra-articular, making malunion an excellent case study for the mechanical hypothesis. In the absence of a specific known intraarticular derangement of the knee (a confounder we made a concerted effort to avoid), the cause of compartmental arthritis compared to the contralateral knee could reasonably be assumed to be degeneration due to malalignment. This is in contrast to the general population with osteoarthritis, where much of the deformity is intra-articular, with cartilage and bone loss and pseudo-laxity that causes gradually increasing (usually varus) malalignment. This has led some to consider malalignment exclusively as a sign of arthritis progression, rather than a factor that may cause arthritis.11,13,14 We recognize that there may be contributions from sagittal, and perhaps more importantly rotational, malalignment in these complex cases of malunion, but these could not be reliably measured from the data available and so were beyond the scope of this study. Other potentially important contributors such as BMI and smoking status were also not able to be compared as they were not reliably documented. The potential contributions of these factors to arthritis have been highlighted in epidemiological studies. 14
It is difficult to draw evidence from much of the past literature which used varying measures of malalignment which could be inaccurate. The Framingham study used local anatomical tibiofemoral alignment,
11
which is not an accurate representation of the mechanical forces acting at the knee, and this method can lead to the misclassification of neutral mechanically aligned (and mildly varus) legs as valgus knees (
Nevertheless, larger cohort studies of osteoarthritis have provided some evidence in support of the mechanical hypothesis. A large observational study of 2958 knees without osteoarthritis at baseline, based on long-leg tibiofemoral angle, demonstrated an increased 1.5 odds ratio of incidence of medial compartment arthritis in varus alignment; there was not significant evidence for the same incident risk in lateral valgus knees, although these had higher risk of progression and reduced risk of medial progression. 26
The most important limitation of this study was its retrospective nature, and it is therefore potentially susceptible to selection bias which may have influenced the results reported here in a manner difficult to predict. Measurement bias could have occurred, but having multiple observers independently assess all radiographs minimized this possibility. The small sample size of the definitive study cohort is an obvious limitation, with the exclusion of 92.3% of the 1,160 long standing radiographs that were identified and screened. However, this is also a strength of the study, as the rigorous selection criteria excluded intra-articular fractures, those with ligamentous instability, and evidence of meniscal pathology that would have been confounding factors. Long-term follow-up of post-traumatic patients is notoriously difficult, leading to relatively low patient numbers. The patients who do follow up are often complex with concomitant ipsilateral or contralateral injuries that would confound comparison of knee arthritis, and were also excluded from review. The rigor with which the study was conducted extends the generalizability of the findings, and limits the possibility that these outcomes would not be replicated in a larger sample from a different population. The potential limitations in this study as a retrospective analysis, are common across most of the studies of malunion. This study serves as a framework for future work, perhaps involving a higher volume of patients with a multi-center retrospective review.
Conclusion
Monocompartmental post-traumatic arthritis correlates closely with lower limb coronal plane malalignment in this study of patients after traumatic malunion. This is likely related to the implicit increased mechanical load and subsequent accelerated wear in the overloaded compartment. These results suggest the development of arthritis is closely related to both time with deformity and the severity of the deformity. This supports the mechanical hypothesis, providing evidence that could not be obtained from cohort studies of osteoarthritis. Based on a linear model with interaction a MAD of 20 mm predicts an OARSI score of 2 after a decade, and a patient with MAD of 40 mm may reach an OARSI score of 3 within 15 years. This topic is of importance both in the study of associated risk factors of, and interventions for, the treatment of osteoarthritis in the general population, and specifically malalignment for fracture malunion.
Supplemental Material
sj-docx-1-car-10.1177_19476035231186688 – Supplemental material for Asymmetric Post-Traumatic Knee Arthritis Is Closely Correlated With Both Severity and Time for Lower Limb Coronal Plane Malalignment
Supplemental material, sj-docx-1-car-10.1177_19476035231186688 for Asymmetric Post-Traumatic Knee Arthritis Is Closely Correlated With Both Severity and Time for Lower Limb Coronal Plane Malalignment by Luke E. Visscher, Cathal McCarthy, Jordy White and Kevin Tetsworth in CARTILAGE
Supplemental Material
sj-pdf-2-car-10.1177_19476035231186688 – Supplemental material for Asymmetric Post-Traumatic Knee Arthritis Is Closely Correlated With Both Severity and Time for Lower Limb Coronal Plane Malalignment
Supplemental material, sj-pdf-2-car-10.1177_19476035231186688 for Asymmetric Post-Traumatic Knee Arthritis Is Closely Correlated With Both Severity and Time for Lower Limb Coronal Plane Malalignment by Luke E. Visscher, Cathal McCarthy, Jordy White and Kevin Tetsworth in CARTILAGE
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the institutional ethics committee (Metro North Health HREC/17/QRBW/495), with a waiver for consent to access retrospective data.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.