
Abstract
Objective
Focal cartilage injuries are debilitating and difficult to treat. Biological cartilage repair procedures are used for patients younger than 40 years, and knee arthroplasties are generally reserved for patients older than 60 years. Resurfacing implants are well suited for patients in this treatment gap. The objective was to investigate the 10-year survival of resurfacing implants in the Danish Knee Arthroplasty Registry.
Design
In this retrospective cohort study, patients treated with resurfacing implants were followed longitudinally in the Danish Knee Arthroplasty Registry from 1997 to 2020. The primary endpoint was revision surgery. The survival of the resurfacing implants was analyzed by Kaplan-Meier method.
Results
A total of 379 resurfacing implant procedures were retrieved from the Danish Knee Arthroplasty Registry. The mean age and weight of patients were 50 years (SD = 11) and 84 kg (SD = 17), respectively. The indications for surgery were as follows: secondary osteoarthritis (42%), primary osteoarthritis (32%), and osteochondral lesions (20%). Within the follow-up period, 70 (19%) of the implants were revised to arthroplasties. The 1-, 5-, and 10-year revision-free survival estimation was 0.95 (95% CI 0.93-0.97), 0.84 (95% CI 0.80-0.88), and 0.80 (95% CI 0.75-0.84), respectively. The median time to revision was 2 years.
Conclusion
The 10-year revision-free survival rate for resurfacing implants was 80%. Based on the revision rates, this treatment offers a viable alternative to biological cartilage repair methods in patients aged 40 to 60 years with focal cartilage pathology. Improved patient selection could further improve the implant survival rate. Further studies are needed to investigate this treatment method.
Introduction
Focal cartilage defects in the knee are frequent1,2 and the quality of life impairment is comparable to patients scheduled for total knee replacement due to osteoarthritis. 3 Despite decades of research, no study has successfully regenerated hyaline cartilage and no gold standard treatment for focal cartilage injuries exists. 4 The most widely used treatment is microfracture introduced by Steadman et al. 5 Treatment with microfracture results in fibrous or fibrocartilaginous repair tissue,6-8 and the short-term clinical improvements tends to deteriorate after 2 to 5 years.9-11 More advanced cartilage repair procedures such as autologous chondrocyte implantation (ACI) and osteochondral autograft transfer (OAT) seem superior in long-term studies,7,12-14 but common for all cartilage repair procedures is that advanced age leads to poorer outcome.15,16 Consequently, cartilage repair procedures are often exclusively offered to patients younger than 40 years.
Total knee arthroplasty (TKA) is a cost-effective treatment for severe osteoarthritis. Patients treated with TKA experience reduced pain, improved function, and improved quality of life. 17 The average age of patients undergoing TKA in Denmark is 68 years, 18 but currently the number of TKAs performed in patients younger than 60 years is rising. 19 The lifetime risk of revision surgery for patients older than 70 years treated with TKA is a mere 5%; however, in patients in their 50s, the lifetime revision risk is as high as 35%. 20
As a result, there is a treatment gap for patients aged 40 to 60 years with cartilage lesions and an estimated 3.6 million Americans are in this treatment gap—too old for biological cartilage treatments and too young for TKA. 21
These patients are left with few options other than corticosteroid injections, weight loss, and physiotherapy. One alternative is a resurfacing implant such as the HemiCap, the UniCap, or the Episealer. These implants consist of a rounded cap-like top, made from cobalt chromium, which is fastened to a titanium screw. The HemiCap (Ø15 mm and Ø20 mm) is available in 16 different contours in order to match the shape of the condyle or the trochlea. The Unicap is in principle the same product but is intended for defects sized 20 × 35 mm. The Episealer is a patient-specific implant created through a computer-aided design/manufacturing process using magnetic resonance imaging (MRI) data. Resurfacing implants can potentially fill the treatment gap between biological cartilage surgery and knee arthroplasty. Clinical studies on resurfacing implants report high patient satisfaction at short-term follow-up; however, the implant survival beyond this point is currently unknown. In addition, some studies report a relatively high revision rate.22-24 Therefore, our objective was to investigate the 10-year survival of resurfacing implants from a nationwide cohort registered in the Danish Knee Arthroplasty Registry.
Methods
The study was designed as a retrospective cohort study and reported in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement. 25 Prior to data collection and analysis, the study was approved by the Danish Data Protection Agency through the Central Denmark Region and Aarhus University Hospital (ID: 1-16-02-152-20).
Data Source
Data were retrieved from the Danish Knee Arthroplasty Registry, which longitudinally collects data on knee implants, including resurfacing implants, inserted in Denmark (estimated population of 5.6 million). Reporting is mandatory for both public and private hospitals and data are collected directly by the surgeon through standardized forms. 26 The Danish Knee Arthroplasty Registry is linked to the Danish Civil Registration Registry, which collects residential and vital status on all Danish citizens and thus, the Danish Knee Arthroplasty Registry enables complete follow up in a population-based cohort. 27
Study Cohort
Resurfacing implants was defined as UniCap, HemiCap, and Episealer. Implants from January 1, 1997 to June 30, 2020 were retrieved from the Danish Knee Arthroplasty Registry. Based on the unique patient identifier variable and the side of surgery, the resurfacing implants were linked with the study outcome defined as later revisions of any kind. In this study, we considered each knee as a single observation, enabling one patient to contribute with two observations. Each observation was longitudinal followed until revision, death, emigration, or end of study period at June 30, 2020.
Variables from the Danish Knee Arthroplasty Registry
Patient demographics included age, sex, and weight (in kilograms). The functional level of the patients was depicted by Charnley class defined as class A (unilateral knee degeneration), class B1 (bilateral knee degeneration), class B2 (implant in the opposite knee), and class C (other condition affecting walking capacity), and the American Knee Society Score (AKSS) divided in a clinical and functional subscore each ranging from 0 (worse) to 100 (best).28,29 Surgical data included prior knee surgeries, indication for condylar implant, type of implant, duration of surgery and reported complications during index surgery. Within the registry, prior knee surgeries were defined as arthroscopy, microfracture procedures, knee ligament reconstruction, osteosynthesis, osteotomy, and undefined, if the prior surgery was not described in detail. Similarly, the indications for resurfacing implants were defined as primary osteoarthritis, secondary osteoarthritis (e.g., following meniscectomy), osteochondral lesions, postfracture arthritis, inflammatory arthritis, recurrent patella dislocations and/or trochlea dysplasia, or undefined, when the indication was not specified.
Statistics
Based on their distribution, numeric variables were depicted by either mean and standard deviation (SD) or median and interquartile range (IQR). Categorical variables were depicted by their number and percentage. The survival of the resurfacing implants was primarily analyzed by Kaplan-Meier method with observations included at the date of index surgery and with date of revision surgery as endpoint. Unrevised observations were censored at the date of death, emigration, or by the end of study (June 30, 2020). Missing datapoints were imputed by multiple imputation with chained equations. 30 Data were sorted in STATA 16 (Stata Corp LLC, College Station, TX, USA) and analyzed using R version 3.5.1 (R foundation for Statistical Computing, Vienna, Austria).
Results
A total of 379 resurfacing procedures from 22 different institutions were retrieved from the Danish Knee Arthroplasty Registry ( Fig. 1 ). Of these, 375 were from patients with unilateral resurfacing implants and 4 observations originated from 2 patients with bilateral resurfacing implants. In total, 0.2% of the datapoints were missing with missing data points in AKSS clinical score (n = 4), Charnley class (n = 3), duration of surgery (n = 2), weight (n = 2), and AKSS functional score (n = 2). The missing data were considered missing at random and imputed by multiple imputation with chained equations.
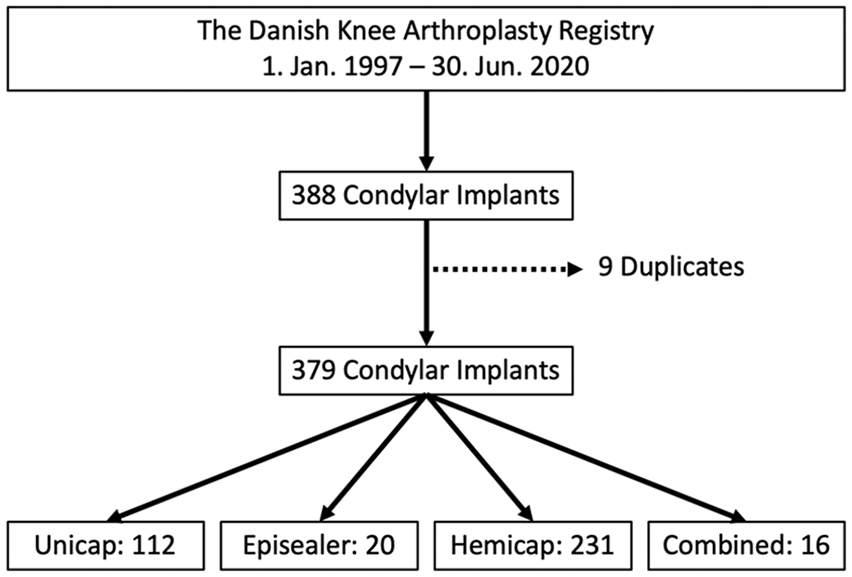
Flowchart: 388 condyle resurfacing implants were registered in the Danish Knee Arthroplasty Registry. Of these, 9 were duplicates and the remaining 379 implants were defined by type of implant in HemiCap, UniCap, Episealer, and combined when more than one implant was inserted.
Baseline Characteristics
As presented in Table 1 , the mean age and weight of patients receiving resurfacing implants were 50 years (SD = 11) and 84 kg (SD = 17), respectively, with a slightly higher frequency of females (57%). Mostly, patients in Charnley class A (87%) received surgery and in only 8 observations the patients’ suffered from another condition limiting their walking capability (Charnley class C). At the time of receiving a resurfacing implant the patients had limited knee function with a mean AKSS clinical score of 55 (SD = 12) and a mean AKSS functional score of 50 (SD = 22).
Patient Demographics and Function Scores from Index Condyle resurfacing Implant Surgery.
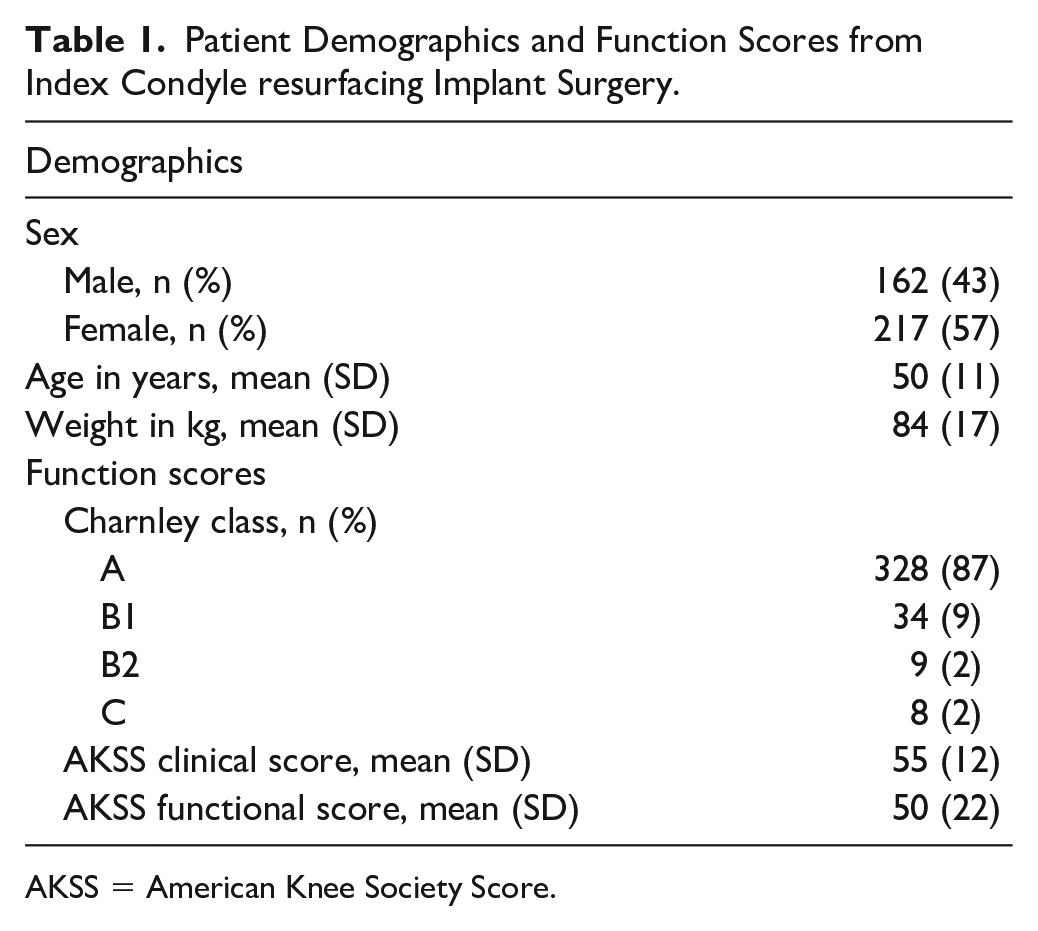
AKSS = American Knee Society Score.
The predominant indication for resurfacing implants was secondary osteoarthritis (42%), followed by primary osteoarthritis (32%), and osteochondral lesions (20%) as presented in Table 2 . Most of the observations had prior knee surgery in the affected knee with arthroscopy (60%) and microfracture procedures (22%) being the most frequent. In this study cohort, isolated HemiCaps (HemiCAP Focal Femoral Condyle Resurfacing Prosthesis, Arthrosurface Inc., Franklin, MA, USA) (61%) were predominantly used. The remaining observation consisted of isolated UniCaps (UniCap Focal Femoral Condyle Resurfacing Prosthesis, Arthrosurface Inc., Franklin, MA, USA) (30%), isolated Episealer (Episealer, Episurf Medical, Stockholm, Sweden) (5%), or more than 1 implant in combination (4%). The combinations were UniCap/HemiCap PF (n = 12) and HemiCap/HemiCap PF (n = 4).
Surgical Information from Index Condyle Resurfacing Implant Surgery.
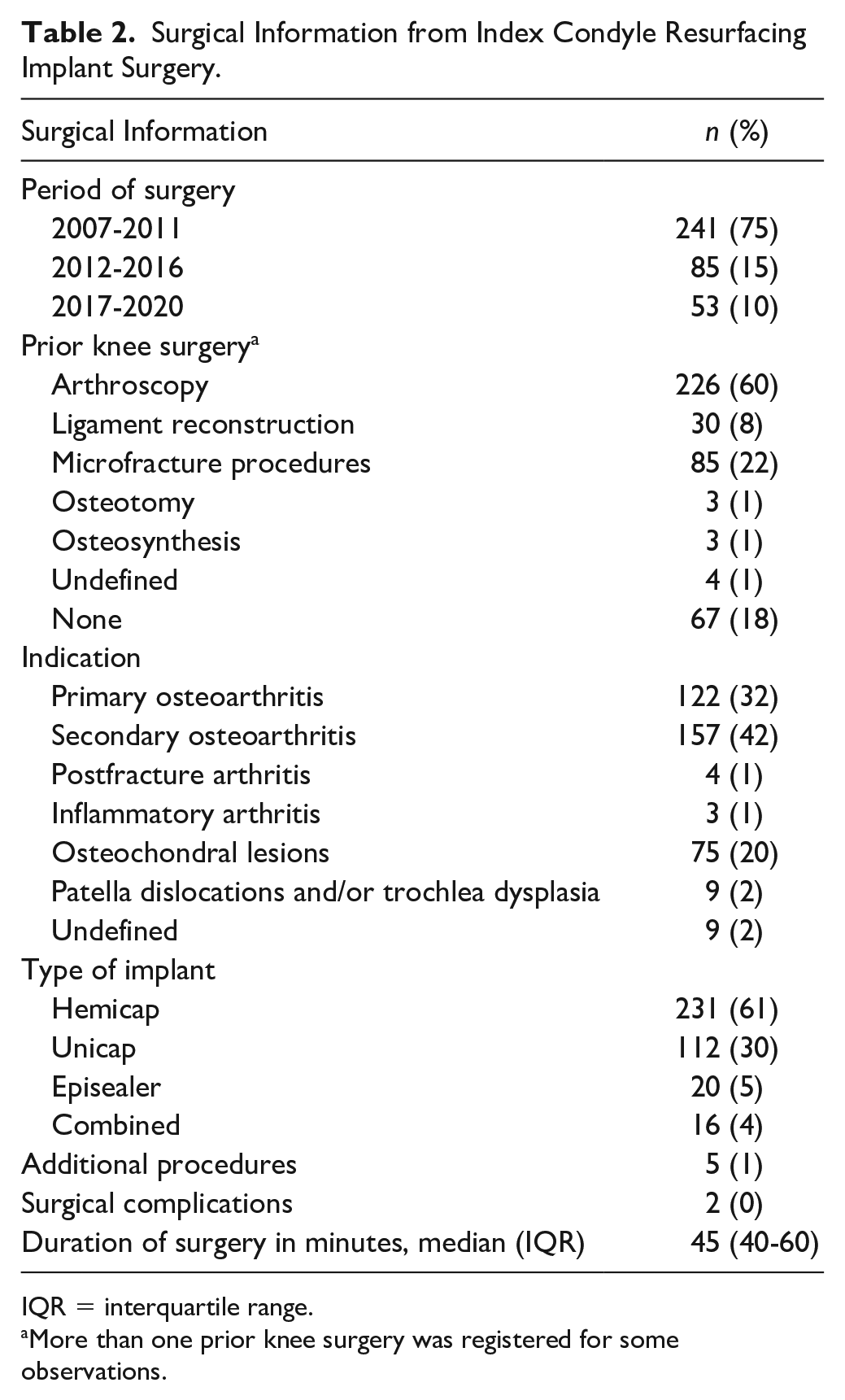
IQR = interquartile range.
More than one prior knee surgery was registered for some observations.
Survival of Condyle Resurfacing Implants
The median follow-up for the 379 resurfacing implants was 8 years (IQR 3-10) and within the follow-up, 70 (19%) of the implants were revised to arthroplasties. This corresponded to a 1-, 5-, and 10-year revision-free survival estimation of 0.95 (95% CI 0.93-0.97), 0.84 (95% CI 0.80-0.88), and 0.80 (95% CI 0.75-0.84), respectively, as seen in Figure 2 . The revised implants were mainly UniCap (n = 35, 50%) and HemiCap (n = 33, 47%) followed by Episealer (n = 1, 1.5%) and combined implants (n = 1, 1.5%). A total of 61 (87%) of the revised resurfacing implants were converted to cruciate-retaining TKAs, 5 (7%) to unicompartmental knee arthroplasties, 1 (2%) to posterior-stabilized TKA, and 3 (4%) had other revision surgery, including replacement of the resurfacing implant. The median time to revision was 2 years (IQR 1-4).
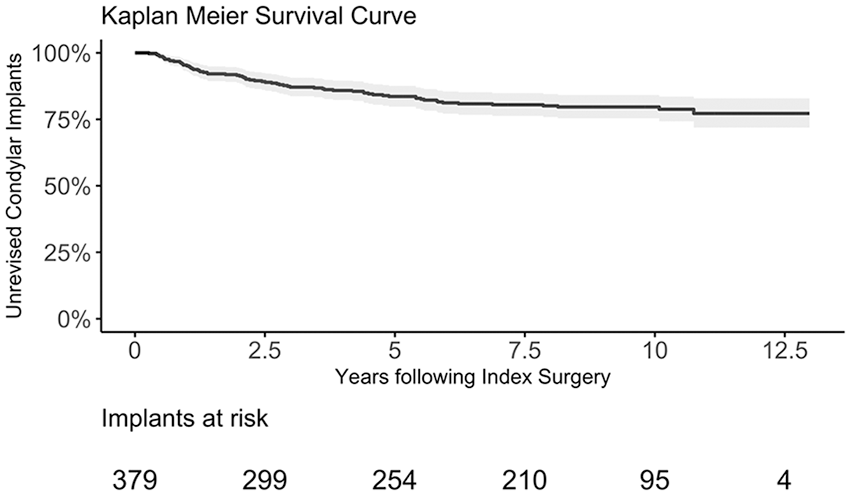
Kaplan-Meier survival estimate for the survival of condyle resurfacing implants with 95% confidence interval. Implants at risk describe the number of condyle resurfacing implants still at risk beyond that time in follow-up.
Discussion
In this study of 379 resurfacing implants, the 10-year revision free survival rate was 80%.
This is well below the 95% 10-year revision-free survival rate for TKAs in Denmark. 18 However, since the indication for treatment with resurfacing implants are focal cartilage injuries and not osteoarthritis, it is more relevant to compare resurfacing implants with biological cartilage repair procedures. In a 15-year randomized controlled trial, Knutsen et al. 13 followed 40 ACI patients (mean age 33 years) and 40 microfracture patients (mean age 31 years). The treatment survival after 15 years was 67.5% in the ACI group and 57.5% in the microfracture group. 13 Minas et al. 14 followed 210 patients treated with ACI (mean age 36 years) for an average of 12 years. The authors reported a 10- and 15-year survival of 71%. Of note, prior microfracture treatment lowered the survival rate of subsequent ACI to 44%. 14 The 10-year survival rate of 80% in the present study includes 21% of the patients with prior microfracture treatment, and a substantially higher average patient age of 50 years.
Pareek et al. 31 did a systematic review of 610 patients treated with OAT across 10 studies. The authors found a 10-year survival rate of 81%, and a failure rate (clinical failure, but no reoperation) of 28%. The authors found a negative correlation with advanced age, previous surgery, and large defect size. 31 While the survival rate of 81% matches the survival found in the present study, the average age of the patients treated with OAT was only 27 years versus 50 years in the present study.
Only limited data exist on resurfacing implants. Çepni et al. 32 reviewed 73 patients treated with HemiCap and found significant clinical improvements and a revision rate of only 6% after 2 years. Similarly, Holz et al. 33 evaluated 75 patients 2 years after treatment with the Episealer implant and found a 2.5% revision rate as well as improvements in the Knee Injury and Osteoarthritis Outcome Score (KOOS). Becher et al. 24 treated 21 patients with HemiCap and followed them for 5 years. The authors reported that 76% of the patients were satisfied with a procedure, and there was only 1 reoperation (4.7%). 24 In a 682-patient study on the Episealer implant, Ryd et al. 34 found a 96% survival after 7 years. The authors concluded that most of the 14 revisions in the study were caused by improper patient selection 34 .
The 2020 annual report from the Australian Arthroplasty Registry reported less favorable results of 245 “partial knee resurfacing procedures.” Of these, 49.5% has been revised after 12 years. 35 Differences in patient selection might be a cause of the high revision rate compared with the results reported in the present study. In an interesting study, Bollars et al. 36 reviewed 27 patients treated with HemiCap. Eight patients were excluded due to high body mass index, kissing lesion, inadequate defect coverage, or ACL instability. Of the 19 remaining patients, 83.4% had normal or near normal clinical scores and there were no revisions, but 7 of the 8 excluded patients had revision surgery. 36
Laursen et al. 22 have published a series of studies on HemiCap and UniCap. The authors followed 62 patients with 64 HemiCap prosthesis for 7 to 10 years and found a revision rate of 42%. 22 Studying the HemiCap Wave for patellofemoral defects, the authors found a revision rate of 28% after 6 years in 18 patients 22 and in 64 patients treated with UniCap (designed for larger defects), the authors found a revision rate of 56%. 23 Laursen et al. 22 reported that the subgroup of patients who did not require early revision had lasting clinical improvements, and no progression of osteoarthritis was seen, while patients suffering from osteoarthritis and patients who did hard, manual labor had a significantly higher risk of revision. This indicates that patient selection is of great importance.
In the present study, 70 revised implants were found. Even though only 112 (30%) of the 379 studied implants were UniCap, 50% of all revised implants were UniCaps. UniCap is designed for larger cartilage lesions and a possible explanation for the higher revision rate for these implants is that they have been used in patients with more extensive cartilage lesions. Lesions that are more likely to represent an osteoarthritic pathology where the joint is undergoing more generalized degenerative changes not addressed adequately with an isolated resurfacing implant.
This study has some limitations to address. Although the use of a nationwide registry adds the external validity of this study, the Danish Knee Arthroplasty Registry does not collect patient-reported outcome measurements. As a consequence, this study solely addresses the survival of resurfacing implants and cannot be used to conclude on the subjective and functional clinical outcome of these implants. Important clinical information, such as size of the cartilage defect or comorbidities, could not be reported as these are not registered in the Danish Knee Arthroplasty Registry. The registry only codes resurfacing implants as HemiCap, UniCap, or Episealer and thus does not allow for analysis the survival of subtypes of these implant designs (e.g., Hemicap Wave). Furthermore, all implant designs were grouped in this study due the relative low number of resurfacing implants. Therefore, the results cannot be used to conclude on the survival of individual implant designs. Finally, there is some uncertainty concerning the indication for surgery. The indications for surgery are predefined in the registry. If the indication is “osteochondral lesion,” the surgeon must check “other” and type the information manually. Therefore, the surgeon could be compelled to check a predefined box with primary or secondary osteoarthritis instead.
Conclusion
A 10-year revision-free survival rate of 80% was found for patients treated with resurfacing implants in the Danish Knee Arthroplasty Registry. Based on the revision rates, the treatment method offers a viable alternative to biological cartilage repair methods in patients aged 40 to 60 years with focal cartilage pathology. Improved patient selection could further improve the implant survival rate. Further studies are needed to investigate this treatment method.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Danish Data Protection Agency through the Central Denmark Region and Aarhus University Hospital (ID: 1-16-02-152-20).