
Abstract
Objective
Distal femoral varus osteotomy (DFVO) is an effective treatment for unloading valgus knee malalignment; however, there is limited evidence on the ability for patients to return to athletics following this procedure. The purpose of this study is to report the functional outcomes and rate of return to sport for athletes that underwent DFVO.
Design
A consecutive series of athletes that had undergone DFVO were retrospectively reviewed. Radiographs were assessed to determine preoperative and postoperative alignment. Institutional registries were used to collect preoperative and postoperative Marx Activity Scale, International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form scores, and return to sport.
Results
Thirteen patients (8 males, 5 females) with a mean age of 24 years (range 17-35 years) and a mean follow-up of 43 months (range 24-74 months) were included in the study. Six patients underwent medial closing wedge DFVO versus 7 patients who underwent lateral opening wedge DFVO. Nine of 13 had concomitant chondral, meniscal, or ligamentous procedures performed. The mean alignment correction was 8° (range 5°-13°). All patients were able to successfully return to sport at a mean of 11 months (range 9-13 months). Furthermore, all 13 patients demonstrated an improvement in both Marx Activity Scale (4-11; P < 0.01) and IKDC scores (53-89; P < 0.01) after surgery.
Conclusions
Correction of valgus knee malalignment through DFVO—either medial closing wedge or lateral opening wedge—can reliably result in improvement in function and return to sport. Concomitant chondral, meniscal, and ligamentous pathology should be addressed.
Keywords
Introduction
Valgus knee malalignment can lead to symptomatic lateral compartment overload, resulting in chondral and meniscal damage and further progression of angular deformity. 1 Distal femoral varus osteotomy (DFVO) can effectively correct valgus knee malalignment and unload the lateral compartment. 2 In fact, biomechanical analysis has demonstrated that the elevated contact pressures seen in the lateral compartment with valgus malalignment are normalized with corrective DFVO. 2 Good to excellent clinical results in nonathletes with symptomatic lateral compartment gonarthrosis have been reported with both medial closing wedge3-16 and lateral opening wedge17-22 DFVO.
While several studies have established the effectiveness of DFVO in relieving pain and improving function,3-22 there is limited available evidence on the ability for patients to return to athletics following this procedure. In their series of patients undergoing DFVO, de Carvalho et al. 23 reported that 58% had resumed physical activities, such as hydrotherapy, swimming, and muscle building exercises, at preoperative levels. However, none of the patients in their series had entered into physical competitions of any type either before or after surgery. 23 Therefore, the question of whether athletes can return to sport after DFVO still remains. The purpose of this study is to report the functional outcomes and return to sport for athletic patients who underwent DFVO for symptomatic lateral compartment overload and valgus knee malalignment.
Methods
This retrospective study was conducted at 2 institutions and approved by both institutional review boards prior to commencement. Institutional medical records databases were queried to identify all patients that underwent varus-producing distal femoral osteotomy between 2005 and 2015. The senior authors (RJW and AJK) performed 31 DFVOs during this time period. All patients had signs, symptoms, and imaging consistent with symptomatic lateral compartment overload and valgus knee malalignment. Surgical intervention was indicated for failure of nonoperative management, including activity modification, anti-inflammatory medications, and physical therapy. In some cases, preoperative unloader braces were used. Concomitant procedures, such as cartilage restoration and meniscus transplantation, were permitted. Patients were included in the present study if they participated in competitive sporting activity prior to the DFVO procedure. Details regarding sport of interest, ability to return to sport, and timing of return were obtained directly from the patients. Patients were classified as athletes if they endorsed participating in sporting activity at least 4 days out of every week. Activity level was also assessed for each patient before and after surgery using the Marx Activity Scale for disorders of the knee. 24 All patients were required to have minimum 2 years of follow-up.
Preoperative Planning
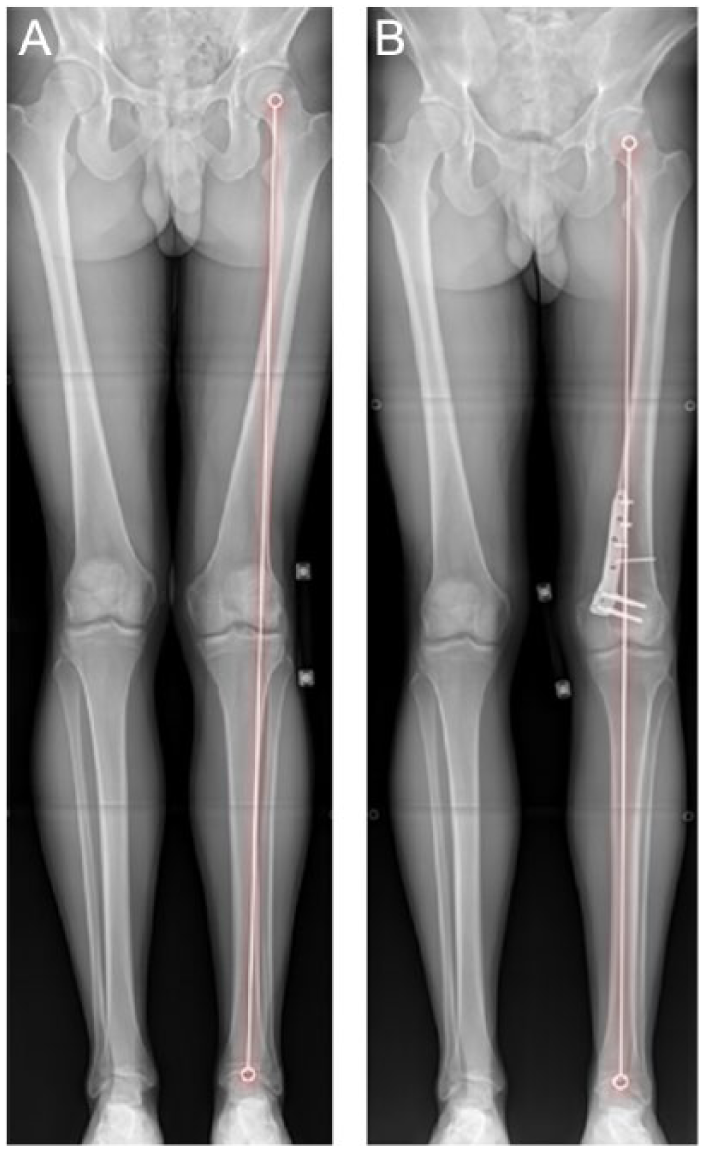
For all patients, preoperative anteroposterior weightbearing hip-to-ankle radiographs were evaluated to determine the angle formed between the mechanical axis of the femur and the tibia. This tibiofemoral angle was then used to calculate the amount of correction needed to achieve the goal of neutral alignment along the mechanical axis.
Patient Positioning and Surgical Technique
The patient is positioned supine with the operative limb raised on a foam ramp as necessary to allow adequate biplanar intraoperative imaging without manipulation of the osteotomy before fixation. A diagnostic arthroscopy is performed prior to the osteotomy to assess the cartilage and address any meniscoligamentous pathology. The authors prefer to first perform any concomitant procedures before the osteotomy.
Medial Closing Wedge Osteotomy
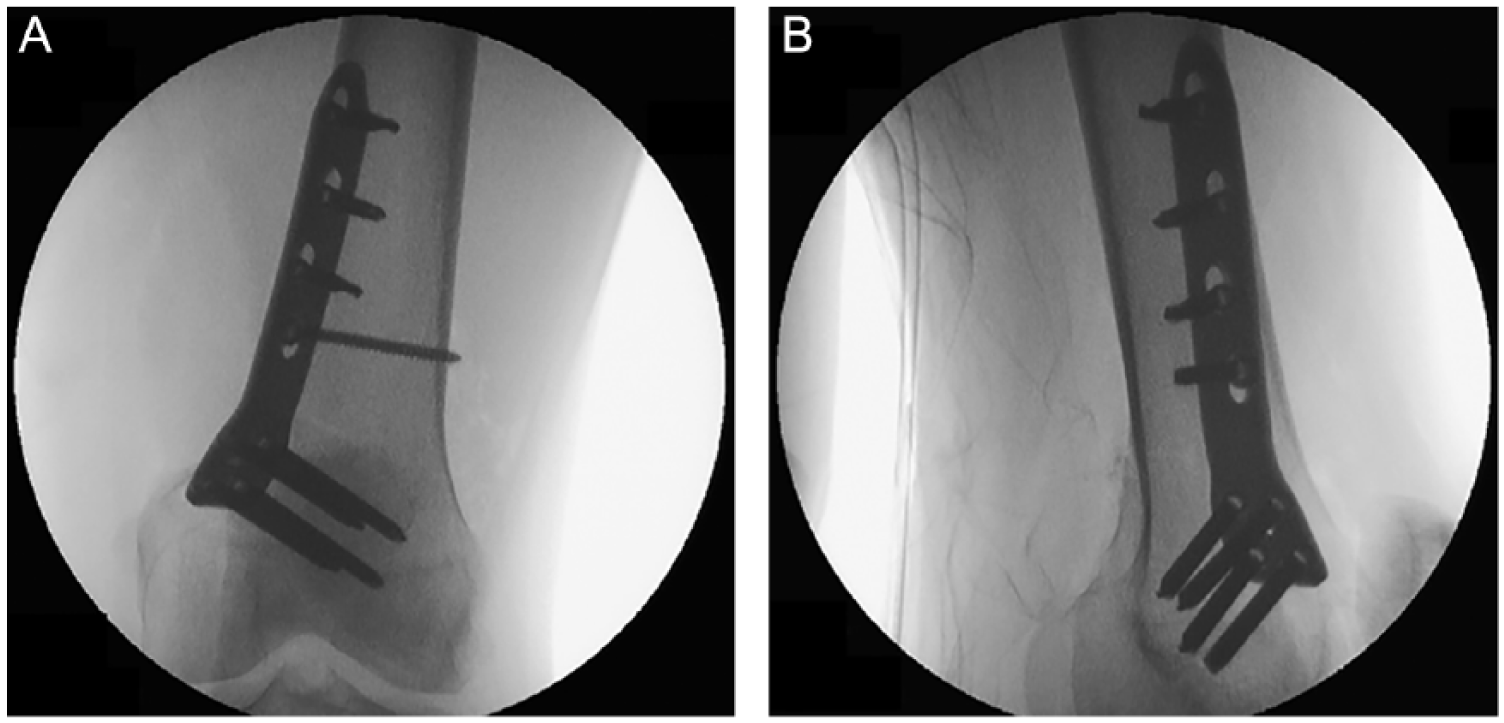
A 10-cm longitudinal incision is made over the medial epicondyle of the knee extending to the joint line distally. Dissection is carried down to the level of the periosteum, being careful to preserve the neurovascular structures of the distal femur. The implant of choice is positioned; the authors prefer a pre-contoured TomoFix Medial Distal Femur Plate (DePuy Synthes, Zuchwil, Switzerland). To avoid rotational deformity when closing the osteotomy, the osteotomy site is marked via electrocautery or marking pen, or by placing Kirschner wires (K-wires) proximally and distally (

Kirschner wires are placed under direct imaging establishing the desired amount of medial bone wedge removed per the preoperative plan.

A nonlocking bicortical screw has been placed in compression mode to compress the osteotomy site.
(
Lateral Opening Wedge Osteotomy
Two options exist for the approach to a lateral opening wedge osteotomy: a true extra-articular approach or an extended lateral peripatellar approach. The former is preferred unless concomitant intra-articular procedures will be performed. After obtaining adequate exposure using one of these approaches, a metadiaphyseal guide pin is placed to establish the trajectory of the osteotomy, and a parallel pin or markings can be used to preempt rotational deformity from the procedure. The knee is flexed to decrease tension on the neurovascular bundle and to increase the distance to the posterior cortex, in order to avoid iatrogenic injury. An oscillating saw begins the osteotomy along the guide pin, and thin osteotomes are used to complete the cut within 1 cm of the medial cortex. The jack opener is placed and opened, and the osteotomy is carefully hinged at the medial cortex over time. The osteotomy site is filled according to the preoperative plan, using corticocancellous wedges of femoral head allograft. This stabilizes the osteotomy while fluoroscopic images are taken to ensure proper mechanical axis alignment. Then the TomoFix Lateral Distal Femur Plate (DePuy Synthes, Zuchwil, Switzerland) is applied. Unicortical locking screws are placed in the distal holes, followed by a kickstand nonlocking screw in compression mode, and finally proximal unicortical locking screws.
Postoperative Care and Rehabilitation
For the first 6 weeks after the procedure, patients are restricted to partial weightbearing with the knee locked in full extension. Knee range of motion is allowed as tolerated. After 6 weeks, the patient may start quad-strengthening, progressive weightbearing, and full range of motion at the knee with no loading beyond 90° of flexion. The brace is weaned and the patient returns at 3 months for standing radiographs (
(
Data Collection and Statistical Analysis
Prospective institutional registries were used to collect preoperative and postoperative Marx Activity Scale and International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form scores. Preoperative versus postoperative outcome scores and tibiofemoral alignment were assessed using paired t tests. Changes in outcome scores were compared between groups using independent-samples t tests assuming unequal variances. All statistical analyses used 2-tailed tests with a critical α of 0.05, and were performed using JMP Pro 10 (SAS Institute Inc., Cary, NC).
Results
A total of 13 athletic patients underwent DFVO by 1 of the 2 senior authors ( Table 1 ). The series included 8 males and 5 females with a mean age at surgery of 24 years (range 17-35 years). The average body mass index was 27.4 kg/m2 (range 23-31 kg/m2). Six patients underwent medial closing wedge osteotomy, and 7 underwent lateral opening wedge osteotomy. Nine of 13 (69%) had one or more additional procedures at the time of osteotomy: 6 had lateral femoral condyle osteochondral allografts, 2 partial lateral meniscectomies, 1 lateral meniscus allograft transplantation, and 1 revision anterior cruciate ligament reconstruction, 1 lysis of adhesions and patellar tendon debridement, and 1 loose body removal. Distal femoral osteotomy significantly decreased the mean preoperative valgus deformity (tibiofemoral angle) from 7° (range 5°-13°) to a mean postoperative deformity of 0° (range 0°-2° varus) (P < 0.0001). The mean alignment correction was 8° (range 5°-13°). No patients were lost to follow-up. The mean postoperative follow-up time was 43 months (range 24-74 months).
Surgery Details, Sport Participation, and Clinical Outcomes for Athletes Who Underwent Distal Femoral Varus Osteotomy.
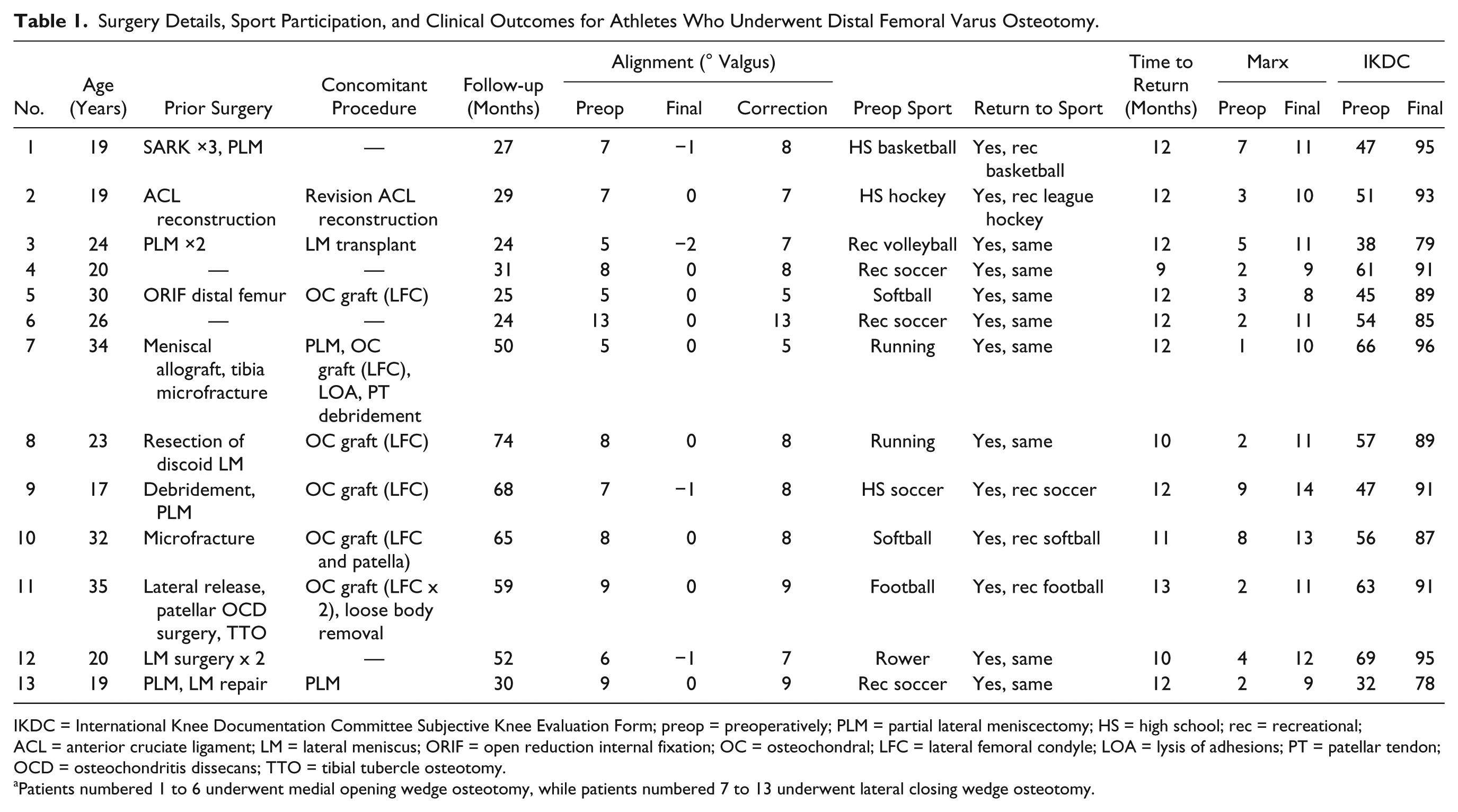
IKDC = International Knee Documentation Committee Subjective Knee Evaluation Form; preop = preoperatively; PLM = partial lateral meniscectomy; HS = high school; rec = recreational; ACL = anterior cruciate ligament; LM = lateral meniscus; ORIF = open reduction internal fixation; OC = osteochondral; LFC = lateral femoral condyle; LOA = lysis of adhesions; PT = patellar tendon; OCD = osteochondritis dissecans; TTO = tibial tubercle osteotomy.
Patients numbered 1 to 6 underwent medial opening wedge osteotomy, while patients numbered 7 to 13 underwent lateral closing wedge osteotomy.
The primary sport of participation before surgery was: 4 soccer, 2 softball, 2 running, 1 football, 1 basketball, 1 ice hockey, 1 volleyball, and 1 rowing. All 13 patients were able to successfully return to their sport of choice at a mean of 11 months (range 9-13 months). Return to sport was defined as returning to athletic activity at least 4 days a week. Furthermore, all 13 patients demonstrated an improvement in both Marx Activity Scale and IKDC scores after surgery. The mean improvement in Marx Activity Scale was 7 ± 2 points (P < 0.0001) with a mean final score of 11 (range 8-14). The mean improvement in IKDC score was 36 ± 8 points (P < 0.0001) with a mean final IKDC score of 89 (range 78-96). Between patients who received lateral femoral condyle osteochondral allografts and those that did not, there were no significant differences in the changes in Marx Activity Scale (P = 0.90) or IKDC scores (P = 0.53).
No major complications, including thrombosis, arthrofibrosis, nonunion, and infection, occurred in any of the patients. One patient that underwent a lateral opening wedge DFVO had symptomatic plate irritation underneath the iliotibial band, with subsequent hardware removal 2 years after surgery. Following plate removal, the patient was recommended not to participate in high-demand cutting and pivoting activities for 6 weeks. The patient’s symptoms were relieved with hardware removal. There were no other reoperations or subsequent surgeries at the time of last follow-up.
Discussion
Valgus knee malalignment often leads to symptomatic lateral compartment overload, which in turn may result in chondral and meniscal damage and further progression of angular deformity. 1 Participation in athletics may worsen the pain from overload of the lateral compartment and contribute to the progression of intra-articular pathology. In the present series, 13 competitive athletes underwent DFVO for these indications. All patients were able to return to sport at a mean of 11 months after surgery. Furthermore, they all demonstrated improved Marx Activity Scale and IKDC scores. 8 out of 13 patients did require concomitant procedures to treat focal cartilage deficits and meniscus insufficiency, and one additional patient also had revision anterior cruciate ligament reconstruction.
DFVO is a viable option for surgically correcting valgus knee malalignment and unloading the lateral compartment. Good-to-excellent clinical results in patients with symptomatic lateral compartment gonarthrosis have been reported with both medial closing wedge3-16 and lateral opening wedge osteotomies.17-22 Systematic reviews published by Chahla et al. 25 and Wylie et al. 26 in 2016 described consistently improved patient-reported outcomes at mid- to long-term follow-up for both approaches, although the scoring system used to measure these outcomes varies widely between studies.25,26 The overall complication rate was 9%, with a 34% reoperation rate. 26 Survivorship with arthroplasty as the endpoint was comparable between the 2 approaches; the lateral opening wedge studies reported lower rates of conversion to arthroplasty, but were also limited by shorter follow-up periods.25,26 For lateral opening wedge osteotomy, mean survival rates ranged from 84% to 100% at 6- to 8-year follow-up.18,20-22 For medial closing wedge osteotomy, mean survivorship has been reported as 64% to 89.9% at 10 years,5,11,12,16 45% to 78.9% at 15 years,12,14,16 and 21.5% at 20 years. 16
We believe the athletes in the present series were able to return to competitive sport due to correction of their alignment to neutral and addressing of concomitant pathology. However, no previous studies to our knowledge have focused on assessing the ability for patients to return to athletic activity after DFVO. A study by de Carvalho et al. 23 evaluated the physical activity and functional outcome of patients presenting with lateral compartment osteoarthritis before and after DFVO. Of the 26 patients enrolled in their study, none had entered into physical competitions of any type either prior to or after surgery. Fifteen of 26 (57.7%) were able to resume other physical activity, such as hydrotherapy, swimming, and muscle building exercises, at preoperative levels, with some patients demonstrating increased number and type of exercises. Twenty-two of 26 (84.6%) were very satisfied or satisfied and 23 (88.5%) returned to normal work duties without limitation or decline in performance. Mean Lysholm scores improved from 53.1 ± 16.2 preoperatively to 77.3 ± 16.7 (P < 0.05) postoperatively, while mean Tegner activity level was 3 both before and after surgery. In another case series by Saithna et al. 17 of 21 knees (18 patients) that underwent opening wedge DFVO, 1 patient did return to competitive Sunday league football, achieving a postoperative Tegner activity level of 9. The overall study found no significant improvements in Knee injury and Osteoarthritis Outcome Score (KOOS) Sport or Tegner scores after DFVO. However, the KOOS Pain and IKDC scores demonstrated clinically and statistically significant improvements. 17
Return to sport has been studied for other types of osteotomy around the knee, yielding promising results. After valgus-producing high tibial osteotomy (HTO), 92.3% of patients in a study by Faschingbauer et al. 27 resumed at least 1 sports activity. Participation in high-impact activities such as jogging, tennis, and soccer decreased more than participation in low-impact activities such as swimming, cycling, and hiking. 27 However, the cohort participated in sports activities for an average of 2.14 ± 0.67 times per week before surgery, which would not have met the criteria for athletic performance used in our study. In another study by Saragaglia et al. 28 that examined return to sport after valgus-producing HTO as well as double-level osteotomy, 86% of patients resumed physical activity after surgery. The majority (73%) engaged in a recreational or occasional level of activity preoperatively, while 4 patients (4.8%) were considered competitive athletes. Both studies demonstrated no significant decrease in the weekly frequency of athletic activity after valgus-producing osteotomy, but the duration of activities was decreased.27,28 In a systematic review of 19 studies that examined return to work and sport after HTO, including the 2 mentioned previously, there were 13 studies that reported on return to the same or greater level of sport in 378 patients. 29 The authors identified only 13 patients in the review as competitive athletes: 7 of 13 (54%) returned to “elite-level competition” and 6 did not. The lower rate of return may reflect more stringent criteria for classification as a competitive athlete than the requirement used in our investigation.
The present study has several notable limitations. As a case series with no control group, we are unable to compare the results of DFVO with other treatment measures. However, it should be noted that all patients enrolled in our study had failed conservative management prior to being indicated for surgery. The interpretation of the results may not be widely generalizable as there was surgeon bias in the selection of these athletes. We are also limited in the size of our study population and the duration of follow-up. Simply stated, the procedure is inherently not that common. A larger study with longer follow-up may be needed to further elucidate the outcomes for athletes following DFVO. We hope that this study will encourage surgeons to consider this treatment in athletes with valgus knee malalignment and symptomatic lateral compartment overload who have failed conservative treatment measures.
In conclusion, correction of valgus knee malalignment through DFVO—either medial closing wedge or lateral opening wedge—can reliably result in improvement in function and return to sport, provided that concomitant chondral, meniscal, and ligamentous pathology is addressed. Therefore, DFVO should be considered in the athletic population for correction of symptomatic valgus knee malalignment.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Riley J. Williams III: Arthrex, Inc.—IP royalties, paid consultant; Cymedica Inc.—stock or stock options; Histogenics Inc.—research support; JRF Ortho—paid consultant R2T2 Laboratories Inc.—stock or stock options; R2T2 Labs Inc.—unpaid consultant; RecoverX—stock or stock options; Springer—publishing royalties, financial or material support; Stryker—paid consultant. Aaron J. Krych: Aesculap/B.Braun—research support; American Journal of Sports Medicine—editorial or governing board; Arthrex, Inc.—IP royalties, paid consultant; Arthritis Foundation—research support; Ceterix—research support; Histogenics—research support; International Cartilage Repair Society—board or committee member; International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine—board or committee member; Minnesota Orthopedic Society—board or committee member; Musculoskeletal Transplantation Foundation—board or committee member; Vericel—paid consultant.
Ethical Approval
Ethical approval for this study was obtained from the HSS and Mayo Clinic Institutional Review Boards.
Informed Consent
Verbal informed consent was obtained from all subjects before the study.
Trial Registration
Not applicable (as this study was not a randomized controlled trial).