
Abstract
Objective
To determine the relationship between cartilage lesion etiology and clinical outcomes after second-generation autologous chondrocyte implantation (ACI) in the patellofemoral joint (PFJ) with a minimum of 2 years’ follow-up.
Methods
A retrospective review of all patients that underwent ACI in the PFJ by a single surgeon was performed. Seventy-two patients with a mean follow-up of 4.2 ± 2.0 years were enrolled in this study and were stratified into 3 groups based on the etiology of PFJ cartilage lesions: patellar dislocation (group 1; n = 23); nontraumatic lesions, including chondromalacia, osteochondritis dissecans, and degenerative defects (group 2; n = 28); and other posttraumatic lesions besides patellar dislocations (group 3; n = 21). Patient’s mean age was 29.6 ± 8.7 years. Patients in group 1 were significantly younger (25.4 ± 7.9 years) than group 2 (31.7 ± 9.6 years; P = 0.025) and group 3 (31.5 ± 6.6 years; P = 0.05). Body mass index averaged 26.2 ± 4.3 kg/m2, with a significant difference between group 1 (24.4 ± 3.2 kg/m2) and group 3 (28.7 ± 4.5 kg/m2; P = 0.005). A clinical comparison was established between groups based on patient-reported outcome measures (PROMs) and failure rates.
Results
Neither pre- nor postoperative PROMs differed between groups (P > 0.05). No difference was seen in survivorship between groups (95.7% vs. 82.2% vs. 90.5%, P > 0.05).
Conclusion
Cartilage lesion etiology did not influence clinical outcome in this retrospective study after second generation ACI in the PFJ.
Level of Evidence
Level III, retrospective comparative study.
Introduction
The biomechanical complexity of the patellofemoral joint (PFJ) predisposes it to a variety of injuries, ranging from acute patellar dislocation to chronic cartilage degeneration and osteoarthritis. While a meta-analysis showed a 39% prevalence of patellofemoral arthritis in symptomatic patients aged 30 years or older, 1 a recent systematic review based on magnetic resonance imaging (MRI) findings suggests that even up to 52% of patients show cartilage defects within the PFJ. 2 Besides acute traumatic events such as patellar dislocation, repetitive microtrauma and chronic maltracking have also been described as possible etiologies of chondral injuries in the PFJ.3,4
Autologous chondrocyte implantation (ACI) has emerged as an excellent treatment option for PFJ chondral defects.5,6 It allows coverage of even large chondral defects and easily adapts to the complex contours of the PFJ articular surface. Moreover, the recent increase in understanding of the complex biomechanics of the PFJ made it possible to better determine diverse etiologies of PFJ cartilage defects. Thus, it allowed the correction of associated risk factors through concomitant procedures that ultimately led to better ACI outcomes in the PFJ.7-9
While appropriate PFJ biomechanics are of utmost importance, other variables have also been shown to affect ACI outcomes in the PFJ, including patient characteristics (age, body mass index [BMI], sex, etc.) and lesion characteristics (location, size, involvement of the subchondral bone, etc.).10-13 Yet few studies specifically investigated the impact of the specific etiology of cartilage defects on the postoperative clinical outcome after ACI to the PFJ. While there have been reports showing a tendency toward worse clinical outcomes in degenerative lesions,14,15 there is a lack of evidence specifically assessing “etiology” in relation to ACI outcomes in the PFJ. The purpose of this study was therefore to investigate the influence of cartilage lesion etiology on postoperative ACI clinical outcomes in the PFJ with a minimum of 2 years’ follow-up. Our hypothesis is that the etiology of cartilage lesions affects the clinical outcomes of ACI in the PFJ and lesions due to patellar dislocation lead to worse clinical outcomes.
Materials and Methods
Patient Selection
A retrospective review of prospectively collected data of all patients submitted to cartilage repair with ACI for focal cartilage defects in the PFJ between September 2007 and October 2015 by a single surgeon (senior author) was performed. Prior to any data collection, the study was approved by our institutional review board (IRB). Patient’s age at the time of surgery, BMI, sex, operated side, cartilage lesion etiology and whether the patient had concomitant procedures at the time of ACI on the index knee were reviewed. Cartilage defect morphology including size, number, and location (patellar surface, trochlear surface, or both) were collected from surgical notes. Inclusion criteria comprised (1) patients with acute and nonacute full thickness chondral lesion(s) in the PFJ (patella, trochlea, or bipolar) and (2) utilization of second-generation ACI—bilayer porcine collagen membrane (BioGide; Geistlich Biomaterials), which was fixed with multiple interrupted 6-0 resorbable sutures and watertight sealed with fibrin glue. Conversely, exclusion criteria included (1) patients with cartilage lesions in the tibiofemoral joint; (2) major concomitant procedures, including other cartilage procedures (osteochondral allograft transplantation [OCA], microfracture, osteochondral autograft transfer [OAT]), meniscal transplantation, trochleoplasty, and distal femoral or high tibial osteotomies (except tibial tubercle osteotomy [TTO]); (3) patients with incomplete data or without pre- or postoperative patient-reported outcome measures (PROMs); 4. presence of inflammatory diseases, unresolved or recent septic arthritis, metabolic arthropathies, and deficient soft tissue coverage; and (5) patients with less than 2 years of follow-up.
Anteromedialization (TTO) was routinely indicated for patients with distal or lateral cartilage defects on the patellar articular surface, in symptomatic cases of patellar maltracking or instability with a tibial-tubercle–trochlear-groove (TT-TG) distance greater than 15, and TT-TG distance greater than 20 mm regardless of the PFJ symptoms. At our institution, other procedures (medial patellofemoral ligament [MPFL] reconstruction or lateral retinacular release/lengthening) are routinely indicated for patellar maltracking or instability as a concomitant procedure with TTO and were not considered in the exclusion criteria.
A total of 190 patients underwent cartilage repair with ACI for focal cartilage defects in the PFJ within the study period. After applying the study’s exclusion criteria, 72 patients with a mean follow-up of 4.2 ± 2.2 years (range, 2-10 years) were eligible for final analysis. Patient’s mean age at the time of surgery was 29.6 ± 8.7 years.
Patient Stratification, Demographic Analysis, and Comparison
Based on the etiology of PFJ cartilage lesions, patients were stratified into 3 groups. Group 1 consisted of 23 patients with at least 1 episode of patellar dislocation, including patellar instability or traumatic dislocations. Group 2 comprised 28 patients with nontraumatic cartilage lesions due to chronic repetitive microtrauma, including patellar maltracking, osteochondritis dissecans, and PFJ degeneration. Group 3 included 21 patients with other posttraumatic cartilage lesions besides patellar dislocation, comprising previous patellar fracture, anterior knee contusions, or any other major knee trauma associated with the PFJ chondral lesion (anterior cruciate ligament rupture, meniscus tear, etc.). Thus, patients with preceding history of a major knee trauma or patellar dislocations were included in groups 3 and 1, respectively. Figure 1 displays patient inclusion and allocation process.
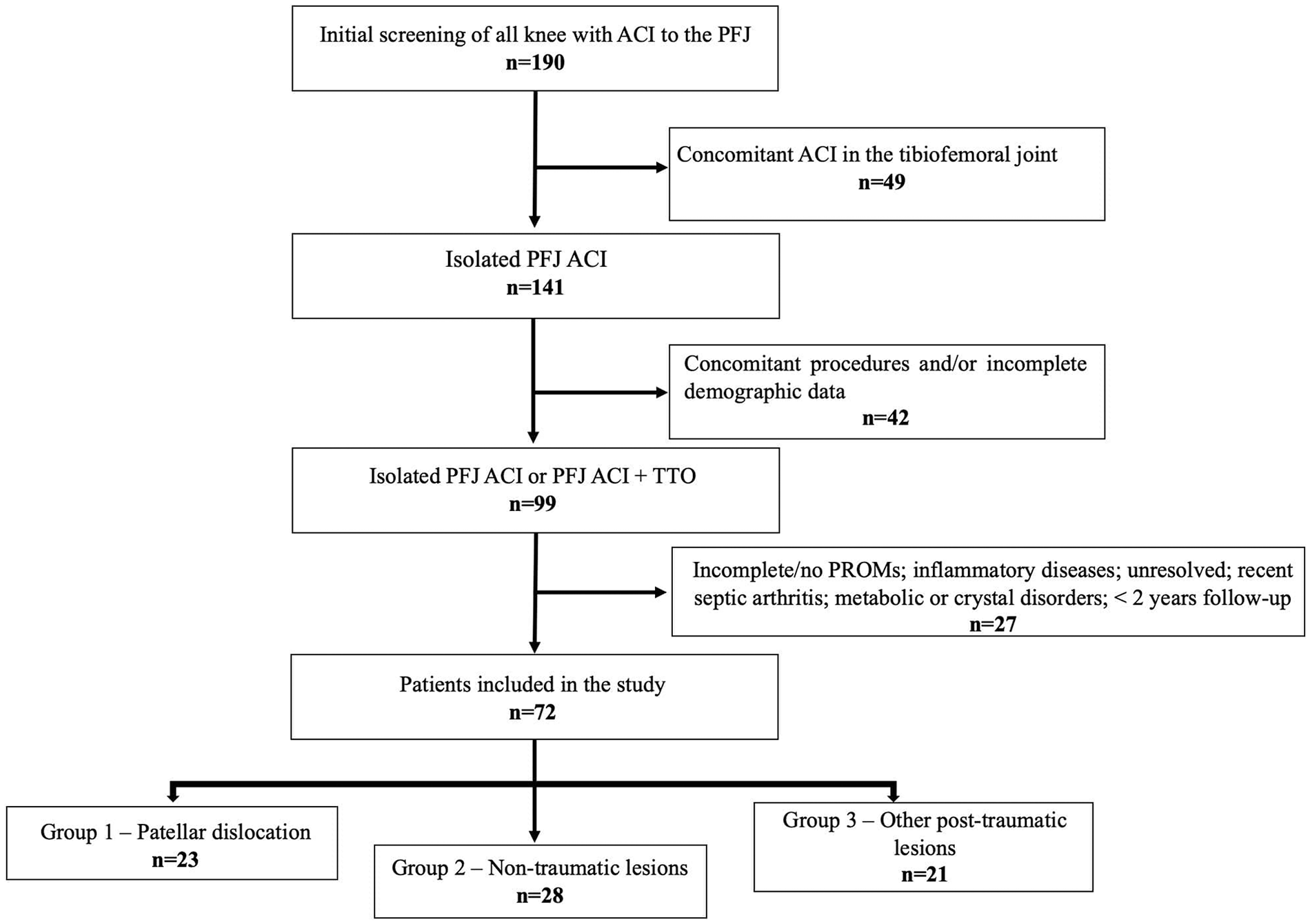
Flowchart showing patient selection and group allocation.
Patients in Group 1 were significantly younger (25.4 ± 7.9 years) than those in group 2 (31.7 ± 9.6 years) and in group 3 (31.5 ± 6.6 years) (P = 0.025 and P = 0.05, respectively). BMI averaged 26.2 ± 4.3 kg/m2, with a significant difference between group 1 (24.4 ± 3.2 kg/m2) and group 3 (28.7 ± 4.5 kg/m2) (P = 0.005). Patients in group 1 more often underwent concomitant procedures when compared with those in groups 2 and 3: TTO (P < 0.001 and P < 0.001, respectively), MPFL reconstruction (P < 0.001 and P < 0.001, respectively), and lateral release (P < 0.001 and P < 0.001, respectively). No differences were seen in the distribution of sex and operated side as well as mean follow-up time between groups ( Table 1 ).
Group Characteristics.
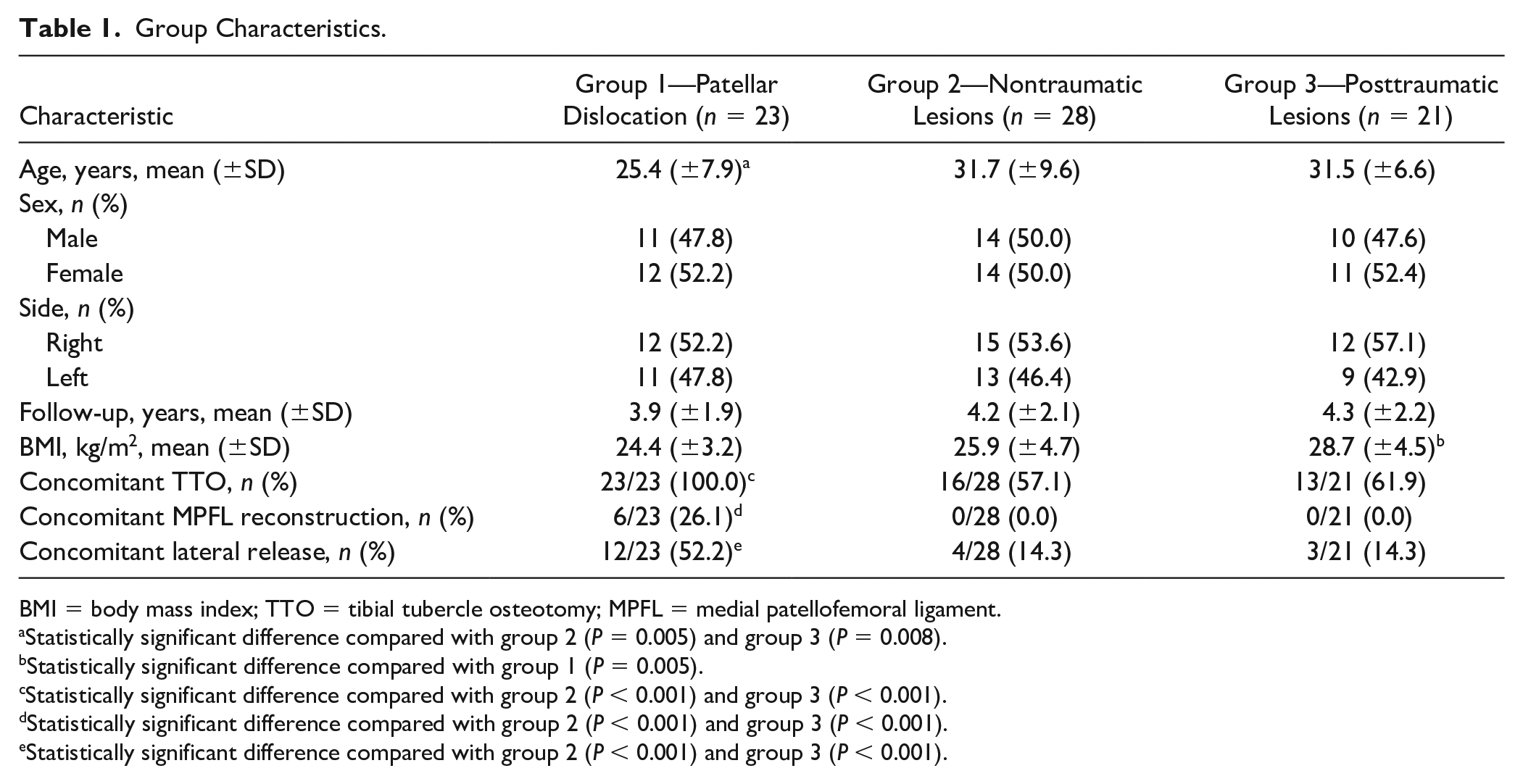
BMI = body mass index; TTO = tibial tubercle osteotomy; MPFL = medial patellofemoral ligament.
Statistically significant difference compared with group 2 (P = 0.005) and group 3 (P = 0.008).
Statistically significant difference compared with group 1 (P = 0.005).
Statistically significant difference compared with group 2 (P < 0.001) and group 3 (P < 0.001).
Statistically significant difference compared with group 2 (P < 0.001) and group 3 (P < 0.001).
Statistically significant difference compared with group 2 (P < 0.001) and group 3 (P < 0.001).
Patients in group 1 were more likely to have chondral lesions in the patellar surface when compared with groups 2 and 3 (P = 0.003 and P = 0.005, respectively), and less likely to present defects in the trochlear surface when compared with groups 2 and 3 (P < 0.001 and P < 0.001, respectively). There were no statistically significant differences in mean patellar or trochlear lesion size between the 3 groups ( Table 2 and Fig. 2 ).
Lesion Characteristics.
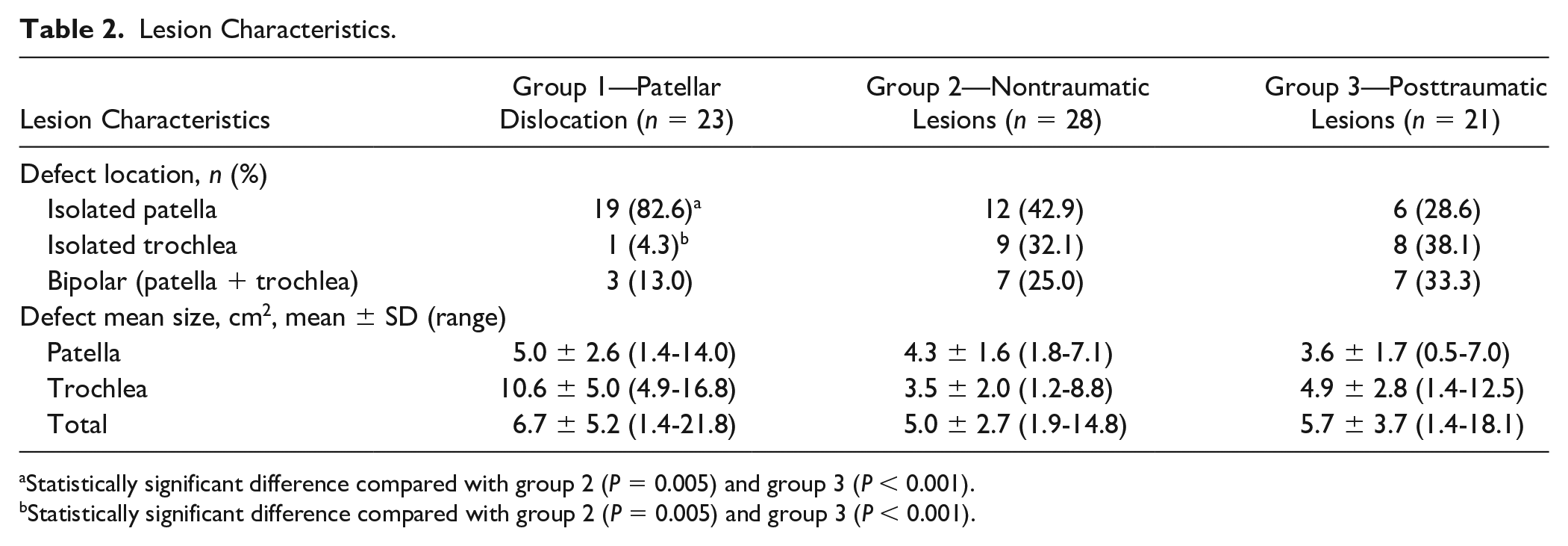
Statistically significant difference compared with group 2 (P = 0.005) and group 3 (P < 0.001).
Statistically significant difference compared with group 2 (P = 0.005) and group 3 (P < 0.001).
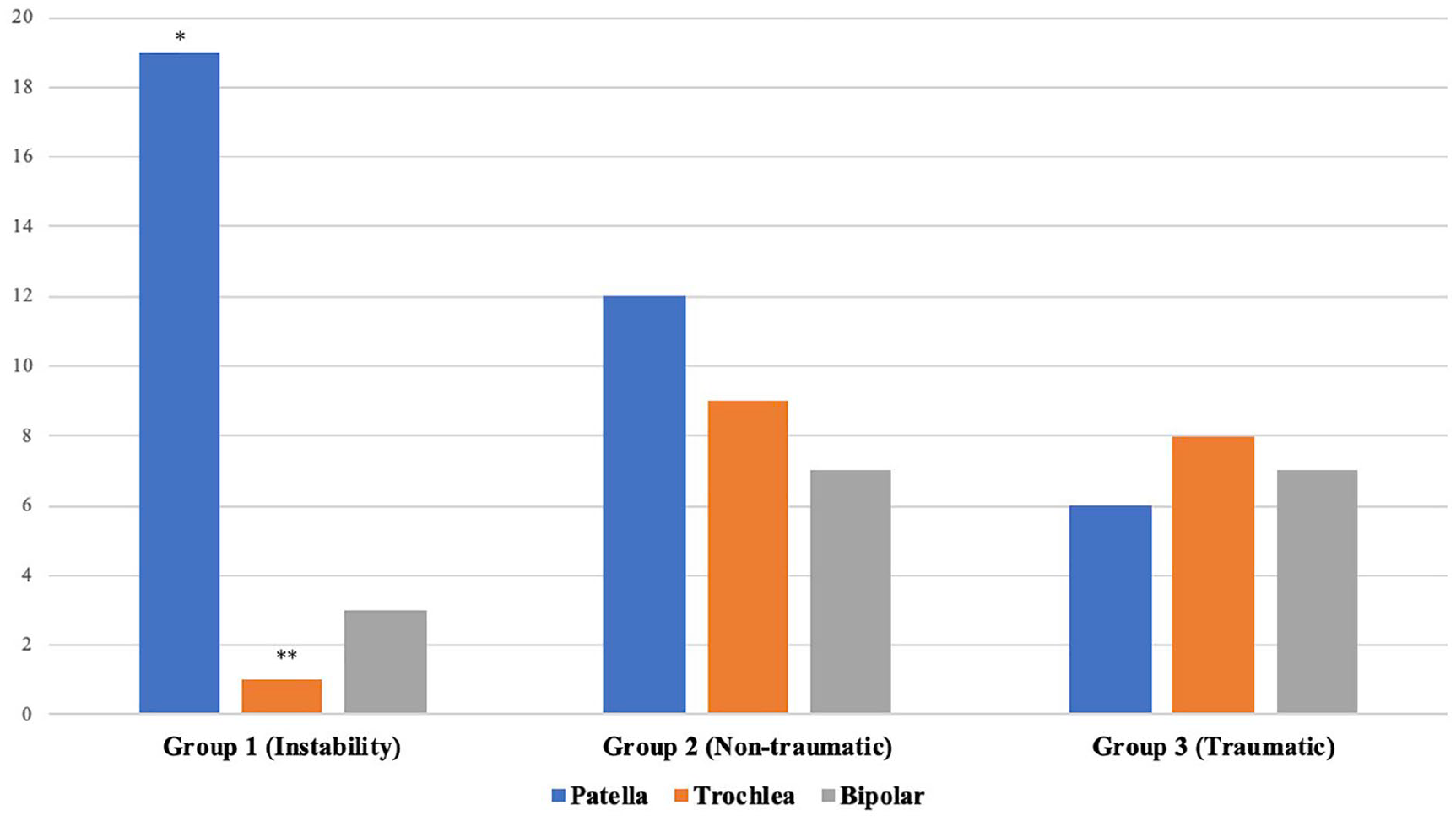
Chondral defects distribution.
After patient allocation, PROMs and failure rates were compared between all groups. Postoperative improvement was also analyzed and compared between groups based on previously published ACI-specific minimal clinically important difference (MCID) for each PROM. 16
Patient-Reported Outcomes Measures
Clinical outcome was evaluated utilizing commonly used PROMs in patients with cartilage lesions of the knee including the Knee Injury and Osteoarthritis Score (KOOS) to assess pain, symptoms, activities of daily living (ADL), sport/recreation, and quality of life (QOL); the Lysholm score evaluating pain, symptoms, and function; the Tegner Activity Scale measuring patient activity level; and the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form. 17 Data were prospectively collected and surveys were completed pre- and postoperatively through our IRB-approved electronic research data capturing (RedCAP) software.
Definition of Failure
The definition of failure for this study included any reoperation resulting from the removal of more than 25% of the graft, as well as revision procedures such as revision ACI, OCA, microfracture, osteochondral autograft transplantation, or arthroplasty. This failure definition was previously defined and utilized in the literature, and served to improve comparability with other studies.6,18,19
Statistical Data Analysis
Microsoft Excel was used for data entry and management. All statistical analyses were performed in SPSS for Mac (Version 23.0, IBM Corp., Armonk, NY). Sociodemographic and clinical characteristics of patients were determined using descriptive statistics. Postoperative self-assessed pain and functional scores between patients, as well as other numeric variables (age, follow-up, BMI, and lesion size) were compared between groups using analysis of variance (Kruskal-Wallis or 1-way analysis of variance) based on data distribution as determined by the Shapiro-Wilk test. Pre- and postoperative clinical outcomes were evaluated utilizing the Wilcoxon rank-sum test and the paired t test. Chi-square test was used to assess categorical variables distribution between groups (concomitant TTO and defect location). Significance was set at P < 0.05. With a total sample size of 72 patients, the study was adequately powered to detect a large effect (Cohen’s f of 0.4) 20 between postoperative PROMs with a power of 0.85 on a level of significance of 0.05. Post hoc power calculation was performed with G-Power version 3.1.
Results
Postoperatively, all 3 groups had statistically significant improvements in KOOS pain, KOOS ADL, KOOS sports/recreation, KOOS QOL, Lysholm, and IKDC scores, exceeding the ACI-specific MCID, determined previously by Ogura et al.16,17 KOOS symptom was the only score that did not reach statistically significant improvement in any of the 3 groups. Tegner Activity Scale reached statistically significant improvement only in group 2 ( Table 3 ).
Comparative ACI Clinical Outcomes Between Groups.
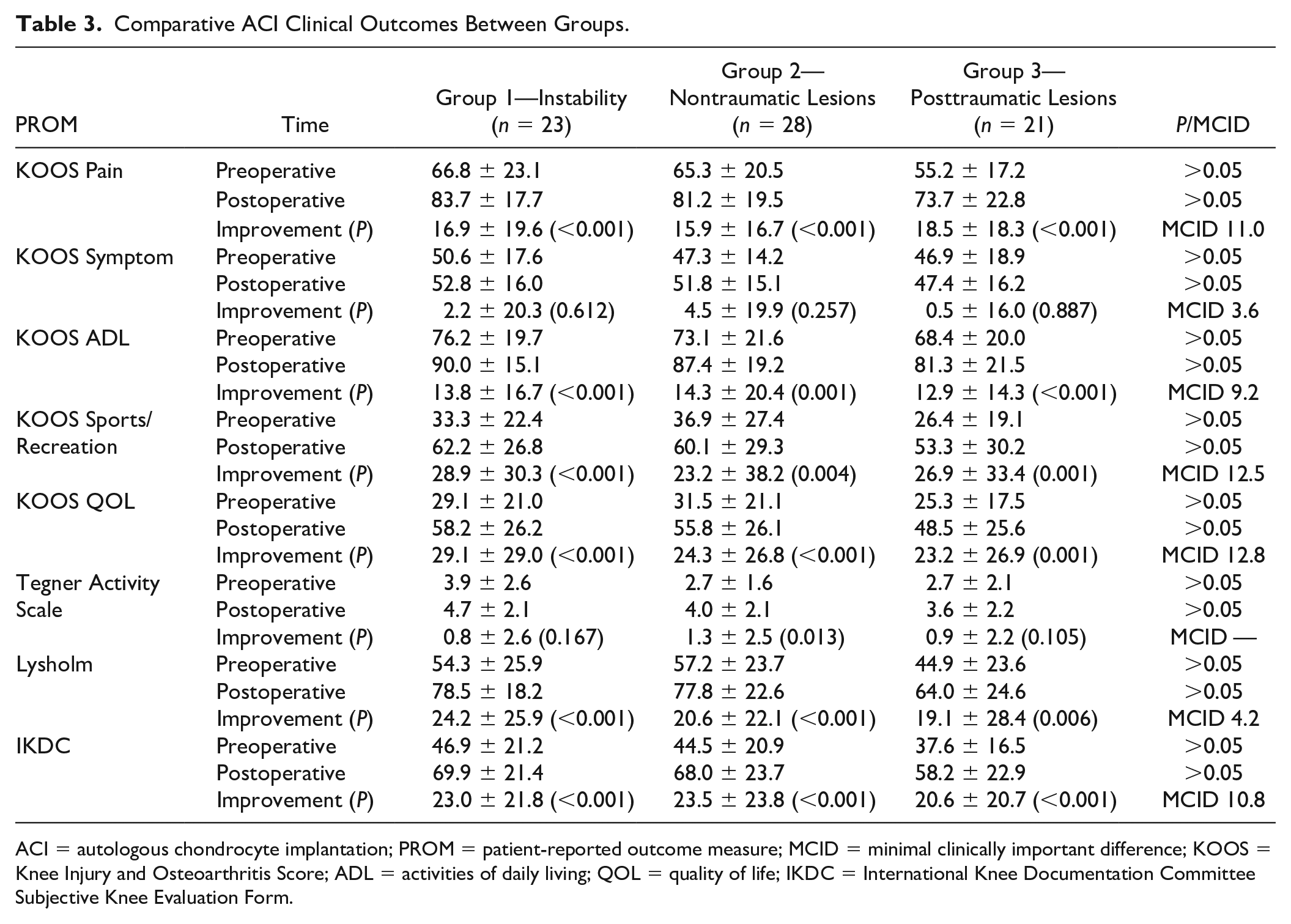
ACI = autologous chondrocyte implantation; PROM = patient-reported outcome measure; MCID = minimal clinically important difference; KOOS = Knee Injury and Osteoarthritis Score; ADL = activities of daily living; QOL = quality of life; IKDC = International Knee Documentation Committee Subjective Knee Evaluation Form.
No differences were found in any pre- or postoperative PROMs between the groups (P > 0.05) ( Table 3 ). Overall survivorship of ACI in the PFJ was approximately 88.9% at final follow-up, regardless of chondral lesion etiology. Group 1 presented with 1 failure (4.3%), group 2 with 5 failures (17.8%), and group 3 with 2 failures (9.5%), resulting in no statistically significant difference between groups (P > 0.05). Failure occurred at an average of 3 ± 1.3 years and all cases were surgically revised with revision ACI (3 patients), OCA (2 patients), debridement and chondroplasty (2 patients), or patellofemoral arthroplasty (1 patient). Overall survivorship free of revision with arthroplasty was 90.3%.
Discussion
The most important finding of this study was that the etiology of a cartilage lesion did not appear to significantly affect the clinical outcome after ACI in our PFJ patients at a minimum of 2 years of follow-up. Clinical comparison of 3 different major causes of cartilage lesions in the PFJ (patellar dislocation, nontraumatic and other posttraumatic lesions besides patellar dislocation) resulted in no statistical differences in PROMs or survival between groups. Postoperatively, all 3 groups significantly improved and exceeded the MCID for all PROMs but KOOS symptoms. In regard to the MCID between groups, Lysholm score fared slightly better in the patellar dislocation group (Group 1) when compared with the group of other posttraumatic lesions group (group 3) but did not reach statistical significance. Tegner Activity Scale showed a statistically significant postoperative improvement in patients with nontraumatic chondral lesions (group 2), but significance was not reached in its comparison between groups.
Initially, ACI to the PFJ demonstrated poorer outcomes when compared with defects in the tibiofemoral joint.21,22 With improvement in surgical technique, emergence of modern collagen membranes, and increased utilization of concomitant procedures for correcting and optimizing PFJ biomechanics, more recent studies demonstrated improved outcomes of ACI to the PFJ.5,23,24 Accordingly, the current study shows satisfactory outcomes with an overall survivorship of 88.9%% at a mean follow-up of 4.2 years, with no statistical differences between the etiologies analyzed.
Previous studies investigated the effect of numerous patient-specific variables on clinical outcome after ACI for PFJ chondral defects. However, few authors specifically assessed “defect etiology” as a potential factor. Gobbi et al. 14 evaluated 38 patients treated with ACI for full-thickness PFJ chondral lesions at a mean follow-up of 6.3 years. Among other variables analyzed, patients with degenerative lesions had worse postoperative IKDC scores when compared with traumatic lesions. 14 Jungmann et al., 15 in a cohort study with 413 patients, analyzed 12 variables to determine risk factors for reinterventions after ACI in the knee. Their results showed that female gender, previous surgeries, previous bone marrow stimulation and periosteum patch-covered ACI were among the risk factors for ACI failure, while lesion origin was not. 15 In contrast to these analyses, the present study solely focused on PFJ cartilage lesion etiology. Furthermore, it discriminates between traumatic lesions caused by patellar dislocation (group 1) and other traumatic etiologies (group 3). We believe that this is an important distinction as both groups present with distinct patient characteristics, ultimately requiring individualized surgical approaches to address the underlying cause of trauma. Last, a third group of nontraumatic lesions (group 2) was included to comprise all patients with lesions that knowingly had no acute trauma episode as the origin of the cartilage defect.
While the clinical comparison performed in this study found no statistical differences among the analyzed etiologies, the MCID found in Lysholm score between groups suggest slightly better clinical outcomes of the PFJ ACI in patients with patellar dislocations (group 1) when compared to patients with other causes of posttraumatic lesions (group 3). However, the inherent heterogeneity between group 1 and group 3 may be a reason for this finding. In the presented cohort, patients in group 1 were younger, thinner (lower BMI), more likely to have a chondral defect on the patellar rather than the trochlear surface, and presented with more concomitant procedures to correct for patellar malalignment. On the other hand, patients with nontraumatic chondral lesions (group 2) were the only ones showing a statistically significant Tegner Activity Scale improvement, though no differences were found in the comparison of postoperative Tegner scores between groups. However, with a smaller sample, it could not reach statistically significance. Nevertheless, patients on both groups 2 and 3 had lower preoperative Tegner score baseline in comparison with group 1, while, postoperatively, these patients appear to catch up with the rest of other patients showing a similarity of postoperative patients’ activity provided by the treatment. Conversely, none of the analyzed groups could demonstrate a postoperative improvement in KOOS symptoms scores. Yet treatment of PFJ conditions remains challenging and patients commonly experience residual postoperative symptoms such as clicking, swelling, and stiffness.25,26
The importance of patellofemoral realignment for the improvement of ACI to the PFJ has been extensively studied in the literature. Pascual-Garrido et al. 27 compared the outcomes of PFJ ACI in patients with or without concomitant TTO. With a mean follow-up of 4 years, patients that underwent ACI with concomitant TTO showed improved clinical outcomes. 27 Ogura et al. 23 evaluated graft survivorship after ACI for the treatment of bipolar chondral lesions in the PFJ. The overall survival rates were 83% and 79% at 5 and 10 years, respectively. The best survival rate was observed among patients who underwent ACI with concomitant TTO (91% at 5 and 10 years). 23 The results of the present study support the importance of patellofemoral realignment for ACI in the PFJ. All patients in the patellar dislocation group underwent at least 1 concomitant procedure for patellar stabilization and maltracking correction. This has to be considered when interpreting the results of the current study, especially the observed differences in postoperative Lysholm scores exceeding the MCID favoring the patellar dislocation group. Additionally, group 1 had a 4-fold lower failure rate when compared to group 2 (nontraumatic lesions), although no statistical significance was achieved.
Besides concomitant procedures, other demographic differences found between the groups—age, BMI and defect location—may also have impacted postoperative outcomes seen in the current study. However, literature remains controversial in quantifying the influence of such variables on PFJ ACI outcomes. Regarding defect location, 1 study reported better outcomes in patellar lesions than in trochlear lesions, 14 while 2 studies showed worse outcomes in bipolar lesions.8,10 Yet other studies found no clinical differences between defect locations at all.26,28 BMI is another variable with conflicting outcomes, with studies reporting better outcomes with lower BMI,12,29 while other reports show no correlation between BMI and ACI outcomes.11,15 Moreover, some studies found no influence of age on ACI outcomes.11,14,15 Yet patients older than 40 years who underwent ACI have an increased risk of a revision procedure as shown by Martincic et al. 30 and present with worse clinical outcomes as published by Krishnan et al. 13 In the present study, a small age difference was observed between patients in group 1 and group 3, yet all groups had a mean age far less than 40 years. Therefore, patient age was unlikely to have affected clinical outcomes.
Limitations
We acknowledge that the current study has some limitations. Though it is a retrospective analysis, all data were prospectively collected to minimize any potential recall bias. The substantial number of excluded patients also deserves attention due to the possibility of selection bias. However, a large number of patients (91 knees, 47.9% of the initially screened knees) had a concomitant ACI to other knee compartment besides PFJ, underwent other major concomitant procedures (i.e. meniscal transplantation, femoral or tibial osteotomies, etc.), required another cartilage procedure to the knee or had less than 2 years of follow-up. Inclusion of all these patients would have introduced major confounders to the analysis. Additionally, only the second generation ACI was analyzed. Yet, all patients that were submitted to the matrix autologous chondrocyte implantation (MACI, third-generation ACI) had a short follow-up, as MACI has become available in the United States not until 2017 and were consequently excluded from the analysis. Last, no specific PFJ score was used for the assessment of clinical outcomes. The Kujala patellofemoral pain scoring system was just recently implemented in our service and did not allow for an adequate follow-up. 31 Despite these limitations, however, the herein presented study adds valuable clinical information regarding the relationship of PFJ cartilage lesion etiology and clinical outcomes after the treatment with ACI.
Conclusion
Cartilage lesion etiology did not influence the clinical outcome after second generation ACI in the PFJ in a retrospective study of 72 patients in three different PFJ groups. This study underlines that one may obtain excellent outcome after ACI in the PFJ and thus supports ACI as preferable procedure for treating cartilage lesions in the PFJ, regardless of lesion etiology.
Supplemental Material
sj-pdf-1-car-10.1177_19476035211030991 – Supplemental material for Etiology of Cartilage Lesions Does Not Affect Clinical Outcomes of Patellofemoral Autologous Chondrocyte Implantation
Supplemental material, sj-pdf-1-car-10.1177_19476035211030991 for Etiology of Cartilage Lesions Does Not Affect Clinical Outcomes of Patellofemoral Autologous Chondrocyte Implantation by Alexandre Barbieri Mestriner, Jakob Ackermann, Gergo Merkely, Pedro Henrique Schmidt Alves Ferreira Galvão, Luiz Felipe Morlin Ambra and Andreas H. Gomoll in CARTILAGE
Supplemental Material
sj-pdf-2-car-10.1177_19476035211030991 – Supplemental material for Etiology of Cartilage Lesions Does Not Affect Clinical Outcomes of Patellofemoral Autologous Chondrocyte Implantation
Supplemental material, sj-pdf-2-car-10.1177_19476035211030991 for Etiology of Cartilage Lesions Does Not Affect Clinical Outcomes of Patellofemoral Autologous Chondrocyte Implantation by Alexandre Barbieri Mestriner, Jakob Ackermann, Gergo Merkely, Pedro Henrique Schmidt Alves Ferreira Galvão, Luiz Felipe Morlin Ambra and Andreas H. Gomoll in CARTILAGE
Supplemental Material
sj-pdf-3-car-10.1177_19476035211030991 – Supplemental material for Etiology of Cartilage Lesions Does Not Affect Clinical Outcomes of Patellofemoral Autologous Chondrocyte Implantation
Supplemental material, sj-pdf-3-car-10.1177_19476035211030991 for Etiology of Cartilage Lesions Does Not Affect Clinical Outcomes of Patellofemoral Autologous Chondrocyte Implantation by Alexandre Barbieri Mestriner, Jakob Ackermann, Gergo Merkely, Pedro Henrique Schmidt Alves Ferreira Galvão, Luiz Felipe Morlin Ambra and Andreas H. Gomoll in CARTILAGE
Supplemental Material
sj-pdf-4-car-10.1177_19476035211030991 – Supplemental material for Etiology of Cartilage Lesions Does Not Affect Clinical Outcomes of Patellofemoral Autologous Chondrocyte Implantation
Supplemental material, sj-pdf-4-car-10.1177_19476035211030991 for Etiology of Cartilage Lesions Does Not Affect Clinical Outcomes of Patellofemoral Autologous Chondrocyte Implantation by Alexandre Barbieri Mestriner, Jakob Ackermann, Gergo Merkely, Pedro Henrique Schmidt Alves Ferreira Galvão, Luiz Felipe Morlin Ambra and Andreas H. Gomoll in CARTILAGE
Footnotes
Authors’ Note
This study was presented at the ICRS World Congress 2019 (October 5, 2019 to October 8, 2019) in Vancouver, Canada (free paper presentation) and received the prize “Cum Laude”: ![]() . Investigation performed at the Cartilage Repair Center, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA.
. Investigation performed at the Cartilage Repair Center, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received grant support from Vericel Corporation (Grant No. 20180814)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by our institutional review board (IRB) Approval/Activation Protocol No. 2018P000180/PHS.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding was provided by Vericel Corporation (Grant Id 20180814).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.