
Abstract
Objective
To assess the clinical and radiological results of patellofemoral osteochondral lesions treated with microfractures associated with a chitosan scaffold.
Design
A retrospective observational analytical study was performed. Fifteen patients with full-thickness patellofemoral osteochondral lesions were included. Quantity and quality of the reparation cartilage was assessed with the MOCART 2.0 score on a postoperative magnetic resonance imaging (MRI), and clinical outcomes were evaluated with pre- and postoperative Kujala score tests. Shapiro-Wilk test for normality was applied as well as Wilcoxon’s signed rank test and Kruskal-Wallis H test for clinical scores within subjects and patella versus trochlea subgroups comparisons. Analysis of variance test was used for imaging subgroups comparison, with P < 0.05 defined as statistical significance.
Results
Mean follow-up was 33.36 months (range 24-60 months). Postoperative Kujala scores improved an average of 19 points compared with the preoperative state (SE = 17.6; P < 0.001). No statistical difference was found through the clinical location assessment (P = 0.756), as well as the cartilage imaging assessment (P = 0.756). The mean MOCART 2.0 scale was 67.67 (range 50-85).
Conclusions
Treating full-thickness patellofemoral osteochondral lesions with microfractures associated with a chitosan scaffold proved to be effective regarding defect filling and symptomatic improvement.
Introduction
Articular cartilage injuries represent a significant challenge. 1 Prevalence studies indicate that chondral injuries of varying severity are found in 60% to 72% of knee arthroscopies.2-5 Although most of these lesions are found in the medial femoral condyle, chondral lesions of the patellofemoral compartment are the second most frequent location.3,4 Many surgical treatments have been described, most of them achieving inferior results compared with the other compartments of the knee6,7 due to the complex biomechanical environment and the transmission of substantial load through the patellofemoral joint during weightbearing and flexion activities. 8
The most widely used surgical technique for cartilage defects is microfracture, based on stimulation of the bone marrow. 9 The success of this procedure depends on the stability of the newly formed clot. To improve this factor, different techniques has been described in the past years. CarGel (Smith & Nephew, Andover, MA), a natural biological chitosan scaffold, 10 is a product developed to stabilize the clot produced by microfractures by mixing a buffer with a chitosan solution and autologous blood to create a liquid bio-scaffold. This allows stability of the progenitor mesenchymal cells from the subchondral bone, thus forming a repair cartilage of better quality and theoretically similar in structure to hyaline cartilage. 11 Different studies using this scaffold, focused on femoral condyle lesions have shown superiority over microfractures in the repair tissue quality and quantity, and several technical advantages compared to other cartilage repair techniques.12,13 To date, there is limited evidence regarding the management of patellofemoral chondral lesions using this scaffold.
The purpose of this study was to evaluate the clinical, functional, and imaging results obtained in full-thickness chondral lesions of the patellofemoral compartment treated with microfractures and the application of a chitosan scaffold.
Methods
An analytical retrospective study was conducted in a private health care center. The medical records of 27 patients who underwent arthroscopic knee surgery as a treatment for full thickness, symptomatic osteochondral lesions of the patella and trochlea from January 2016 to December 2018 were evaluated.
The inclusion criteria were patients with grade IV, symptomatic osteochondral lesions according to the International Cartilage Repair Society (ICRS) scale, diagnosed by magnetic resonance imaging (MRI; General Electric resonator 3.0 T, GE Medical Systems, Milwaukee, WI) in the patellofemoral compartment refractory to more than 6 months of conservative treatment, who have received treatment with microfractures in addition to a chitosan scaffold, without associated alignment surgery, postoperative MRI performed between 6 and 12 months after surgery. Exclusion criteria were presence of osteochondral lesions in other compartments, associated realignment surgery, MRI performed before 6 months or after 12 months after surgery.
Of the total of 27 patients initially evaluated, 15 met the inclusion criteria. Mean follow-up was 33.36 months (range 24-60 months). The average age was 33.8 ± 9.9 years, with 86.7% of male patients. Mean body mass index was 25.23 kg/m2 (range 17-31.5 kg/m2). The location of the lesion was in the trochlea in 5 cases (33.3%), patella in 4 cases (26.7%), and patella plus trochlea in 6 cases (40%). The mean preoperative area of the lesions was 1.99 cm2 (range 1.1-3.8 cm2), mean area for trochlear lesions was 1.6 cm2 (range 1.1-2.3 cm2), mean area for patellar lesions was 1.7 cm2 (range 1.2-2.1 cm2), and the mean area for combined lesions was 2.5 cm2 (range 1.3-3.8 cm2). Every patient received previously to surgical indication at least 6 months of conservative treatment consisting in activity modifications (avoiding deep knee flexion and patellofemoral loading exercises such as squats and lunges) and routine physiotherapy appointments twice a week.
Surgical technique was the same in every patient. After careful evaluation of the patient MRI ( Figs. 1 and 2 ), a diagnostic arthroscopy was performed, and microfractures were done during this part of the procedure. If the injury was located on the patellar surface, a medial or lateral parapatellar approach with patellar eversion was performed according to the side of the lesion to place the chitosan comfortably ( Figs. 3 and 4 ). After the chitosan scaffold was stable (15 minutes), closure was performed and the patient was put on a hinged knee brace, locked in 0° to 30° of range of motion for 3 weeks. After that term, full range of motion was permitted and rehabilitation started. Patients were allowed to perform unsupervised sports from the fourth month after surgery depending on their muscular improvement. A follow-up MRI ( Figs. 5 and 6 ) was performed after 6 months from the procedure.
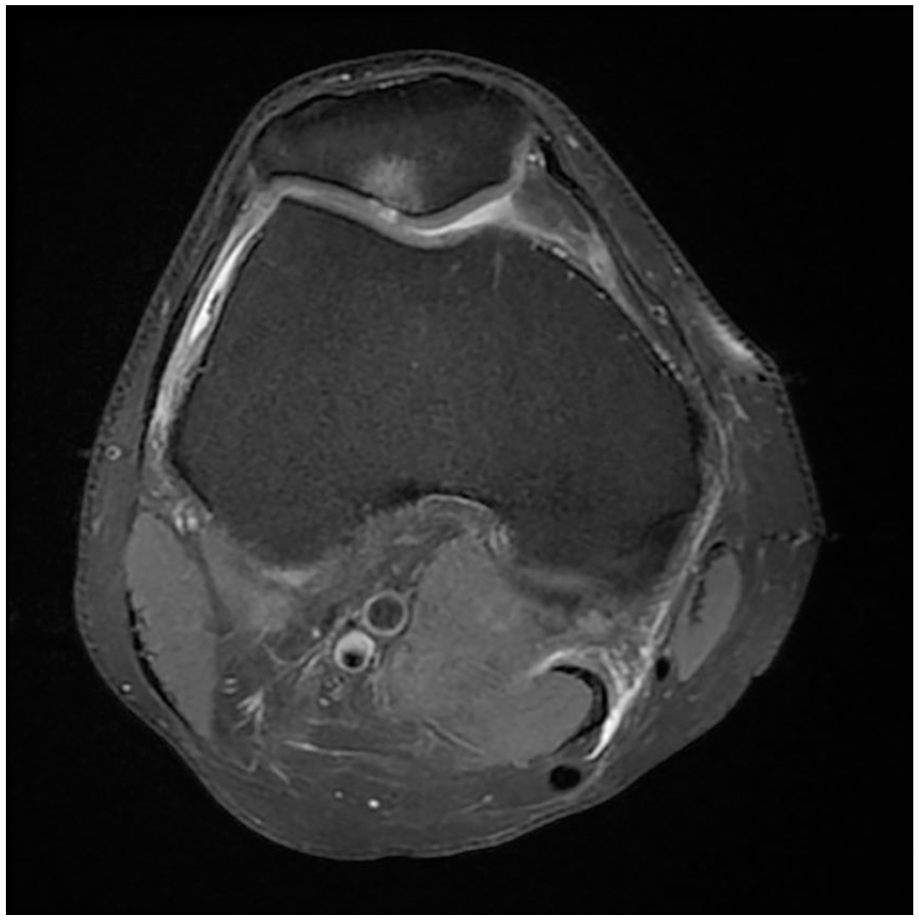
Axial magnetic resonance imaging cut showing a full-thickness patellar chondral lesion.
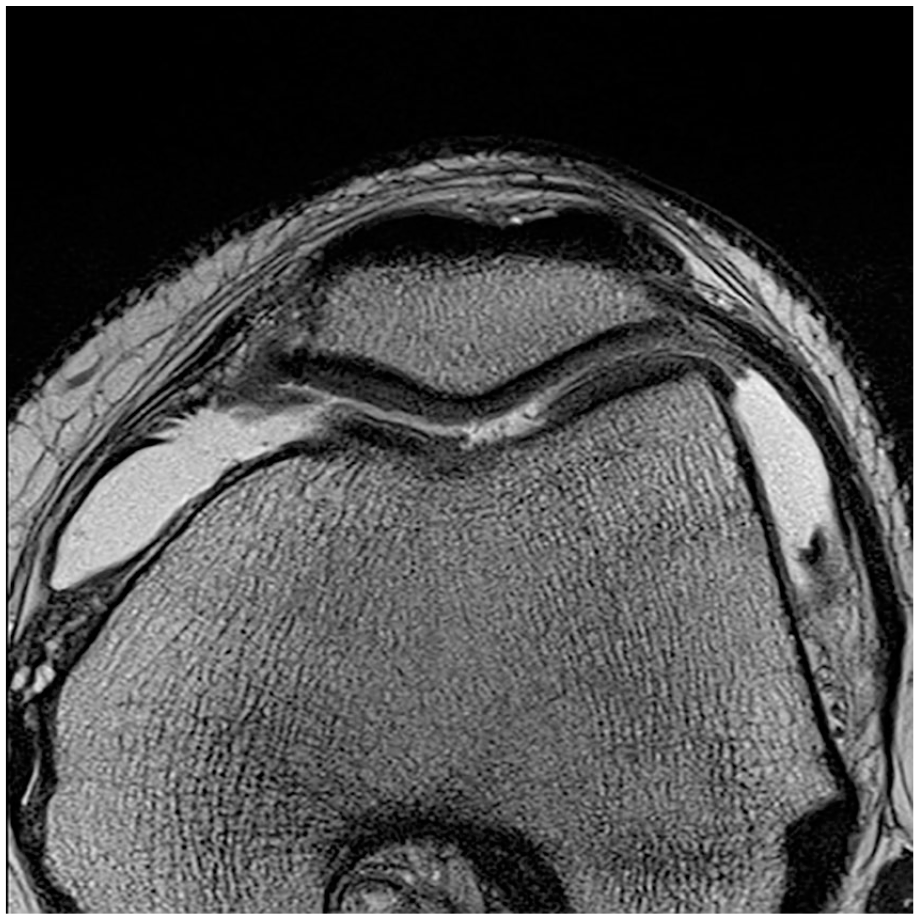
Axial magnetic resonance imaging cut showing a full-thickness trochlear chondral lesion.

Intraoperative image showing a diffuse full thickness patellar chondral lesion.

Intraoperative image showing filling of the full thickness patellar chondral lesion with chitosan.
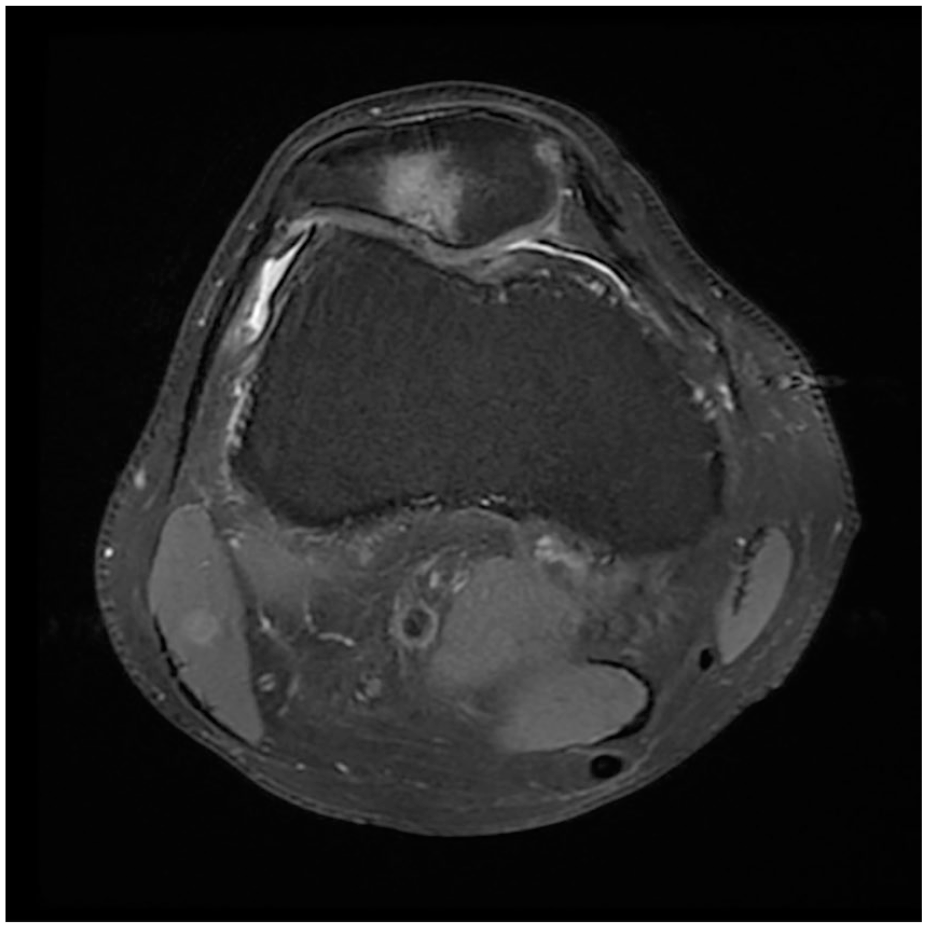
Axial postoperative magnetic resonance imaging cut showing complete filling of the cartilage lesion seen in Figure 1 .
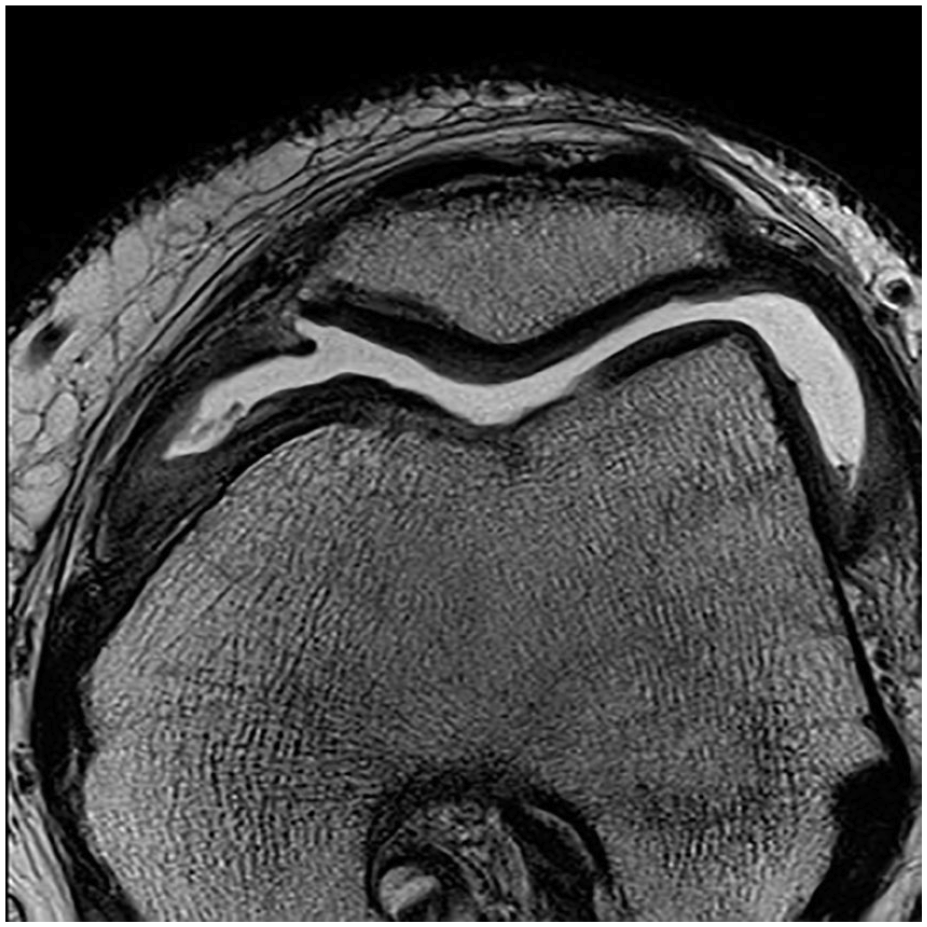
Axial postoperative magnetic resonance imaging cut showing partial filling of the cartilage lesion seen in Figure 2 .
Clinical history, surgical reports, and the pre- and postoperative MRI of the patients were evaluated. The images were evaluated by a single musculoskeletal radiologist experienced in the field to determine the volume of filling (complete, hypertrophied, or incomplete in different percentages), integration to the adjacent cartilage (complete or with different size defects), cartilage surface (intact or with irregularities), structure of the repair tissue (homogeneous or heterogeneous), signal of the repair tissue, bone defect or growth, and subchondral changes (no changes, signs similar to edema, cyst or signs of osteonecrosis). These 7 measurements allowed the calculation of the MOCART 2.0 (magnetic resonance observation of cartilage repair tissue) score (range 0-100), 14 indicating the quality of the cartilage repair.
For the clinical evaluation, the Kujala score 15 was evaluated pre- and postoperatively associated with a single question of self-reported satisfaction regarding the result of the surgery through telephone calls. Both measurements were done at final follow-up.
Nonparametric Wilcoxon and Kruskal-Wallis H tests were used for the comparison analysis between preoperative and total postoperative clinical scores (Kujala), as well as the comparison of postoperative clinical scores and filling volume by subgroups, given the abnormal distribution evaluated by Shapiro-Wilk test. For comparison by subgroups of imaging results, the one-factor analysis of variance (ANOVA) test was used because of its normal distribution and its homogeneity of variances without performing post hoc analysis given the results, with P < 0.05 defined as statistical significance.
This study received the approval of the local ethics committee.
Results
Regarding clinical evaluation ( Table 1 ), 81.25% of the patients reported feeling satisfied with the result of their surgery. The Kujala score described a preoperative median of 68 (interquartile range [IQR] = 58-74) points and a postoperative median of 87 (IQR = 79-93) points, with a mean improvement of 19 points, being statistically significant, P < 0.001.
Clinical Evaluation Summary.

SD = standard deviation; IQR = interquartile range; SE = standard error.
All subgroups by location of the lesion showed improvement in the clinical scores, without observing statistically significant differences in the medians of the 3 groups; P = 0.756 ( Table 2 ).
Clinical and Imaging Evaluation by Location.
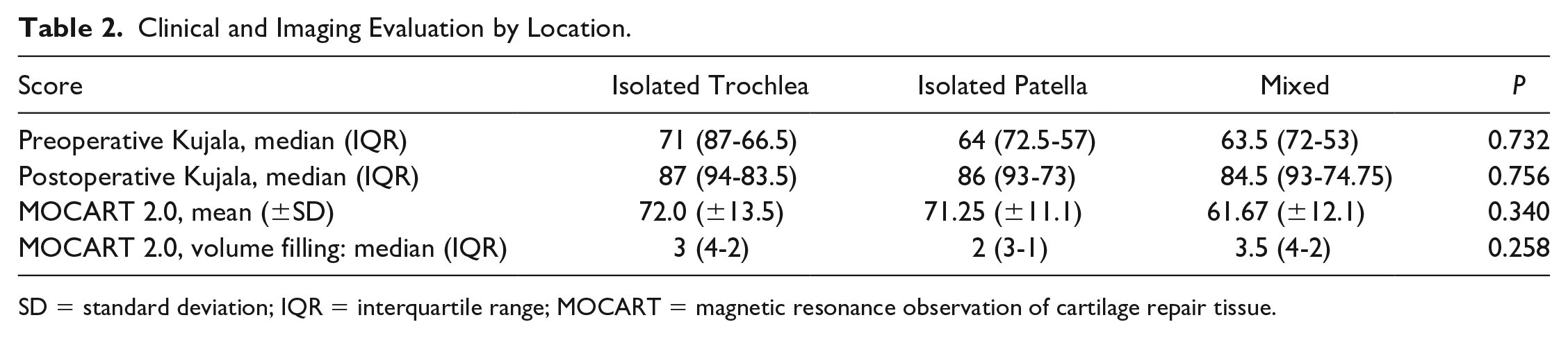
SD = standard deviation; IQR = interquartile range; MOCART = magnetic resonance observation of cartilage repair tissue.
When the patients were consulted regarding their satisfaction with the surgical procedure at the end of the follow-up, 80% reported being satisfied.
Regarding the imaging results, the mean MOCART 2.0 scale was 67.67 (50-85). Sixty-six percent presented a filling volume larger than 50%, as well as 80% showed a favorable integration to the adjacent cartilage ( Figs. 7 and 8 ). The structure of the repair cartilage was observed to be mainly homogeneous, as well as the surface had irregularities in less than 50% of the tissue. The intensity of the tissue signal obtained only normal responses, while the bone evaluation did not present significant defects or overgrowth. Finally, the most important subchondral changes were signs similar to edema in less than 50% of the tissue, with no evidence of cysts or osteonecrosis.
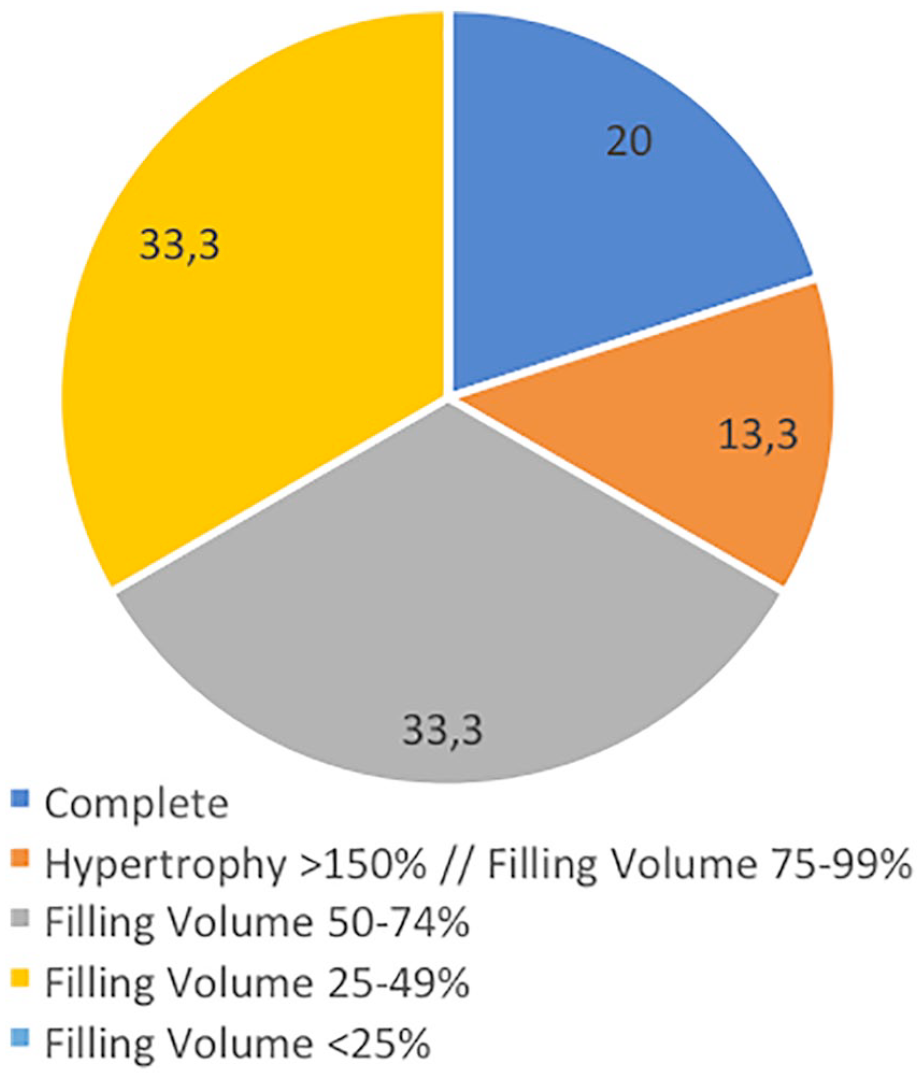
Repair cartilage filling volume results.
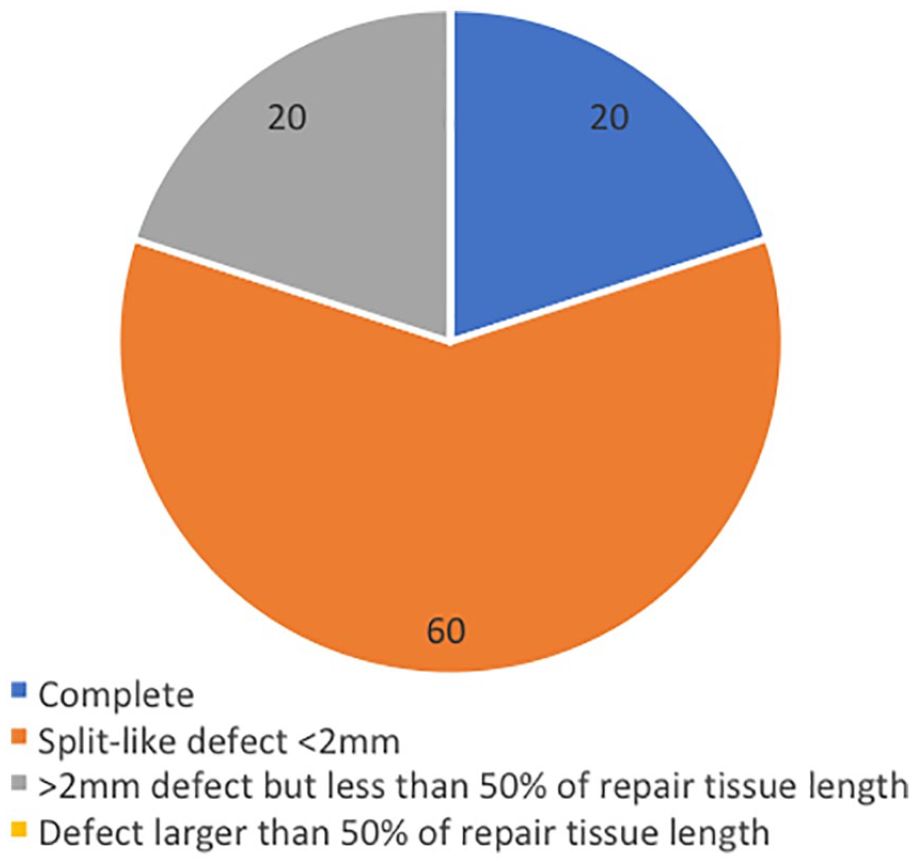
Integration of the repair cartilage with adjacent cartilage results.
When analyzing the results of the MOCART 2.0 score by location, no statistically significant differences were observed between the means, P = 0.340 ( Table 2 ). Similarly, when analyzing the filling volume, no statistical differences were found among subgroups (P = 0.258) ( Table 2 ).
Discussion
The present study showed that using microfractures in addition to a chitosan scaffold is a good surgical alternative for the treatment of full thickness patellar or trochlear cartilage lesions, obtaining good imaging results in the short-term follow-up and favorable clinical results in the mid-term follow-up.
Full-thickness articular cartilage injuries represent a challenge for the surgeon in their treatment, especially those located at the patellofemoral level.2,5 Although there are various surgical techniques, undoubtedly those that determine bone marrow stimulation, such as microfractures, are the most widely used given their simplicity and cost-effectiveness. The controversy is established in its worst results in the mid- to long-term follow-up16,17 especially in young and active patients.
However, promising results in patellofemoral lesions have been found with various cartilage repair techniques. Ebert et al. 18 found out in their series of patellofemoral chondral lesions treated with autologous chondrocyte implantation (ACI), improvements in all areas of the KOOS (Knee Injury and Osteoarthritis Outcome Score) questionnaire at 2 years. Similarly, Figueroa et al., 19 in a series of patellofemoral chondral lesions treated using osteochondral autograft transplantation (OAT) found promising results in the Kujala and WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores. It is important to remark, that unlike ACI, OAT has a size limitation because of donor-site morbidity. In a long-term study including lesions in femoral condyles, patella, and trochlea, Gobbi et al. 20 demonstrated good to excellent clinical outcomes using a hyaluronic acid–based scaffold embedded with bone marrow aspirate concentrate for the treatment of full-thickness cartilage injuries.
Regarding isolated microfractures, Mithoefer et al. 21 indicated in its systematic review that 67% to 86% of patients reported improvement in the functionality of the operated knee in the medium- and long-term follow-up. However, a progressive deterioration over time with regard to the initial postoperative function has been described. 22 Some authors attribute this to incomplete filling of the defect and poor integration with the surrounding normal articular cartilage after microfractures, while others point to the inferior characteristics of the fibrocartilaginous repair tissue resulting from bone marrow stimulation.23-27
The concept of “enhanced” microfractures has been developed, including the chitosan scaffold among others, in an attempt to resolve this issue. There are studies describing how microfractures associated with chitosan promotes the filling of the lesion, increases the stability of the clot, and promotes the growth of repair fibrocartilage with superior results when compared with the one generated by isolated microfractures.12,28-30 To date, there is limited evidence regarding the management of patellofemoral chondral lesions using this scaffold.
Previous studies have shown favorable results in the filling and quality of the repair cartilage with the MOCART 2.0 score using the chitosan scaffold. 27 The results of this study showed that microfractures associated with the chitosan scaffold provides in the short-term a cartilage of good quality and filling repair based on the measurement with the MOCART 2.0 score, similar to the results in the study by Steinwachs et al. 31 in its patellar subgroup. Similarly, their study indicated that the patients treated with the chitosan scaffold did not require second operations due to complications in relation to the applied product, as there were no reports of infections or allergic reactions, confirming the safety of the bio-scaffold. On the same direction, this study did not present the need to perform complementary procedures such as arthroscopic fibro-arthrolysis, manipulations under anesthesia or other surgical reinterventions, differing from the rates of reoperations reported in the literature for chondral regeneration techniques. 32
Despite the favorable results, it is necessary to point out that the study has certain limitations, the main one being the low number of cases; however, this corresponds to the same number as the patellar subgroup evaluated by Steinwachs et al., 31 without existing publications with longer series. On the other hand, as the present study is retrospective, it is not exempt from the biases inherent in its design.
Regarding the strengths of this study, it should be noted that the group of chondral patellar and trochlear lesions was specifically isolated, without including other compartments or other associated knee surgeries, avoiding the mixing of groups and possible confounding variables.
In the future, prospective randomized studies are needed using microfractures in addition to chitosan as a scaffold in patellofemoral lesions, evaluating long-term results, and permitting the correlation of the results of this technique with others for the treatment of full-thickness patellofemoral cartilage lesions.
Conclusion
In conclusion, microfractures associated with a chitosan scaffold is a valid surgical alternative for the treatment of full thickness patellar and trochlear cartilage lesions, obtaining favorable imaging results in the short-term follow-up and clinical results in the mid-term follow-up.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study received the approval of the local ethics committee (ID 2013-01).