
Abstract
Objective
To investigate the effects of exercise training alone and in combination with kinesio taping on pain, functionality, and circulating cartilage oligomeric matrix protein (COMP), and matrix metalloproteinase (MMP)-1, and -3 at rest and immediately after walking exercise in knee osteoarthritis (OA).
Design
A total of 22 female patients diagnosed with knee OA were randomly divided into the exercise training (ET) or exercise training plus kinesio taping (ET + KT) groups. The patients in the ET performed exercise training for 6 weeks. The patients in the ET + KT group were applied with kinesio tape in addition to the exercise training for 6 weeks. In both groups, 20 minutes of walking exercise were performed before and after the interventions. The pain and functional status of the patients were assessed using visual analogue scale (VAS) and Western Ontario McMasters Osteoarthritis Index (WOMAC) before and after the intervention at rest, respectively. Blood samples were taken at rest and immediately after the walking exercise before and after the interventions for the analysis of COMP, MMP-1, and MMP-3 levels.
Results
In both groups, pain and functionality scores were significantly improved after the interventions (P < 0.05). COMP, MMP-1 and MMP-3 levels were higher immediately after walking exercise when compared with rest in both groups before and after the intervention (P < 0.05).
Conclusions
Exercise training and exercise training plus kinesio taping improved pain and physical function; however, the COMP, MMP-1, and MMP-3 levels did not change.
Introduction
Osteoarthritis (OA) is a chronic, multifactorial, and degenerative disorder that mainly is seen in cartilage, subchondral bone, synovium, and muscles.1,2 It is characterized by the loss of joint space, articular cartilage disorders, subchondral bone destruction, and synovial membrane thickening.3,4 The knee is the most affected joint in OA, and knee OA patients experience inflammation, pain, stiffness, muscle atrophy, and functional disability. 5 Physical disability caused by pain and loss of functional capacity in knee OA reduce life quality. Interestingly, women are more affected by knee OA than men. 6 Although differences in knee anatomy, kinematics, previous knee injury, and hormonal influences have been shown to cause the disease, 7 the true cause and underlying cellular and molecular mechanisms are still unclear. Current knee OA treatments aim to alleviate these symptoms by a variety of methods such as pharmacological, nonpharmacological, surgical, and nonsurgical interventions. Among the nonpharmacological modalities, exercise training and kinesio taping have gained popularity in recent years. 8
There are no diagnostic tests that are routinely used to diagnose OA, but several biomarkers have been used to assess the severity of OA. 9 One of the possible biomarkers of OA are the products of bone and cartilage degradation,10,11 among which cartilage oligomeric matrix protein (COMP) and matrix metalloproteinases (MMPs) are the most studied biomarkers. 12 The fact that the levels of these markers are proportional to the degree of knee OA and that serum levels correlate with synovial fluid levels led to much work on them.13-15
COMP is a noncollagen protein found primarily in articular cartilage, 16 and plays a role for the maintenance of mature collagen network. 17 Its level in synovial fluid correlates with serum level, 18 and age, weight, and mechanical loading affect the serum COMP level in healthy individuals. 19 In addition, an increase in serum COMP level has been reported in patients with knee OA,19,20 and athletes after exercise. 21 Furthermore, serum COMP level reflects the severity of the disease in the early stage of knee OA. 22
MMPs are a group of extracellular enzymes responsible for extracellular matrix (ECM) degradation. 23 MMP-3 is produced mainly in synovial tissue and cartilage and is responsible for cartilage matrix degradation and joint inflammation 24 and activates proMMPs 1, 7, 8, 9, and 13. 25 MMP-1, -8, and -13 are members of the collagenases that are responsible for the degradation of intact collagen type II which is the main component of the articular cartilage. 23 However, MMP-7 and MMP-9 play an important role in ECM homeostasis and in joint disc remodeling. 26 Studies have shown that synovial fluid and circulating levels of MMP-1 and MMP-3 are higher in knee OA than healthy individuals, and MMP-1 and MMP-3 reflect the progression of joint disease.12,25,27,28
It is well known that exercise training improves strength, balance, range of motion, body coordination and reduces morbidity and pain in knee OA patients.20-30 In addition to aerobic and resistance exercises in different modalities such as water exercises, walking, Tai Chi and yoga; quadriceps and hamstring strength exercises are also recommended regardless of the patient’s age, gender, body mass index, radiographic status, and baseline status.31,32 In addition, circulating levels of COMP and MMPs have been reported to slightly decrease or not change in response to exercise training.17,33-35 However, acute loading, such as walking exercise, has been shown to cause a marked increase in serum COMP and MMPs levels 15, 30, 45, and even 60 minutes after exercise, but had returned to baseline within 24 hours.17,25,28,29,33 Erhart-Hledik et al. 36 found that serum COMP levels increased after 30 minutes of walking exercise, and this amount of increase was closely related to the 5-year rate of cartilage loss in participants with knee OA.
Kinesio taping is an alternative taping method that reduces pain and edema, induces functional and proprioceptive stimulation, improves muscle activity, and prevents and treats sports injuries.37,38 Number of studies37,39-42 have examined the effects of kinesio taping on knee OA, but conflicting results have been obtained on pain and functionality. However, to our knowledge, no study has so far investigated the effects of kinesio taping on COMP, MMP-1, and MMP-3 levels in knee OA.
Since exercise training reverses knee OA-induced pain and functional impairment, we assumed that the combination of exercise training and kinesio taping may have a synergistic effect on knee OA symptoms and treatment. Therefore, the primary objective of this study was to investigate the effects exercise training alone and in combination with kinesio taping could have on pain, functionality, and circulating COMP, MMP-1, and MMP-3 levels at rest in patients with knee OA. Additionally, since acute loading causes an increase in serum COMP and MMPs levels after exercise, exercise training alone and in combination with kinesio taping may prevent this elevation after exercise. Thus, our secondary goal was to examine changes in circulating COMP, MMP-1, and MMP-3 concentrations after 20 minutes of walking exercise before and after interventions.
Methods
Subjects
Study Sample
This study was a randomized, double-centered study. Participants were selected from the patients who applied to Konya Numune Hospital Physical Medicine and Rehabilitation Department outpatient clinic between June 2016 and November 2016. All measurements were performed in Selçuk University Faculty of Medicine Division of Sports Physiology Laboratory.
The study was approved by the Ethics Committee of Selçuk University (approval no. 2016/101, 30/03/2016) and all experiments were carried out in accordance with the Helsinki Declaration. All participants were given written and verbal information about the purpose, procedures, and potential risks of the study, and signed informed consent forms were obtained.
Inclusion and Exclusion Criteria
Inclusion criteria were patients between the ages of 38 and 60 years, having a knee OA diagnosis according to the American College of Rheumatology, 5 and Kellgren-Lawrence index II and III in class, and signing the informed consent form.
The exclusion criteria were rheumatoid arthritis, severe organ failure, previous joint replacement, osteoporosis, and diagnosis of any disease that could limit performance.
Study Design
Based on the inclusion and exclusion criteria 22 adult women were included in this study. The patients were randomly divided into the exercise training (ET, n = 11) and exercise training plus kinesio taping (ET + KT, n = 11) groups. Randomization was carried out using the sealed envelope method. In this method, an investigator gathered the 22 patients who met the inclusion criteria, and each patient was instructed to randomly select one of the sealed envelopes. There were 22 sealed envelopes, and 11 of these enveloped contained letter A, and 11 contained letter B. The patients in the group A performed exercise training for 6 weeks. The patients in the group B were applied kinesio taping in addition to the exercise training for 6 weeks. In both groups, 20-minute walking exercise was performed as an acute loading before and after the intervention ( Fig. 1 ).
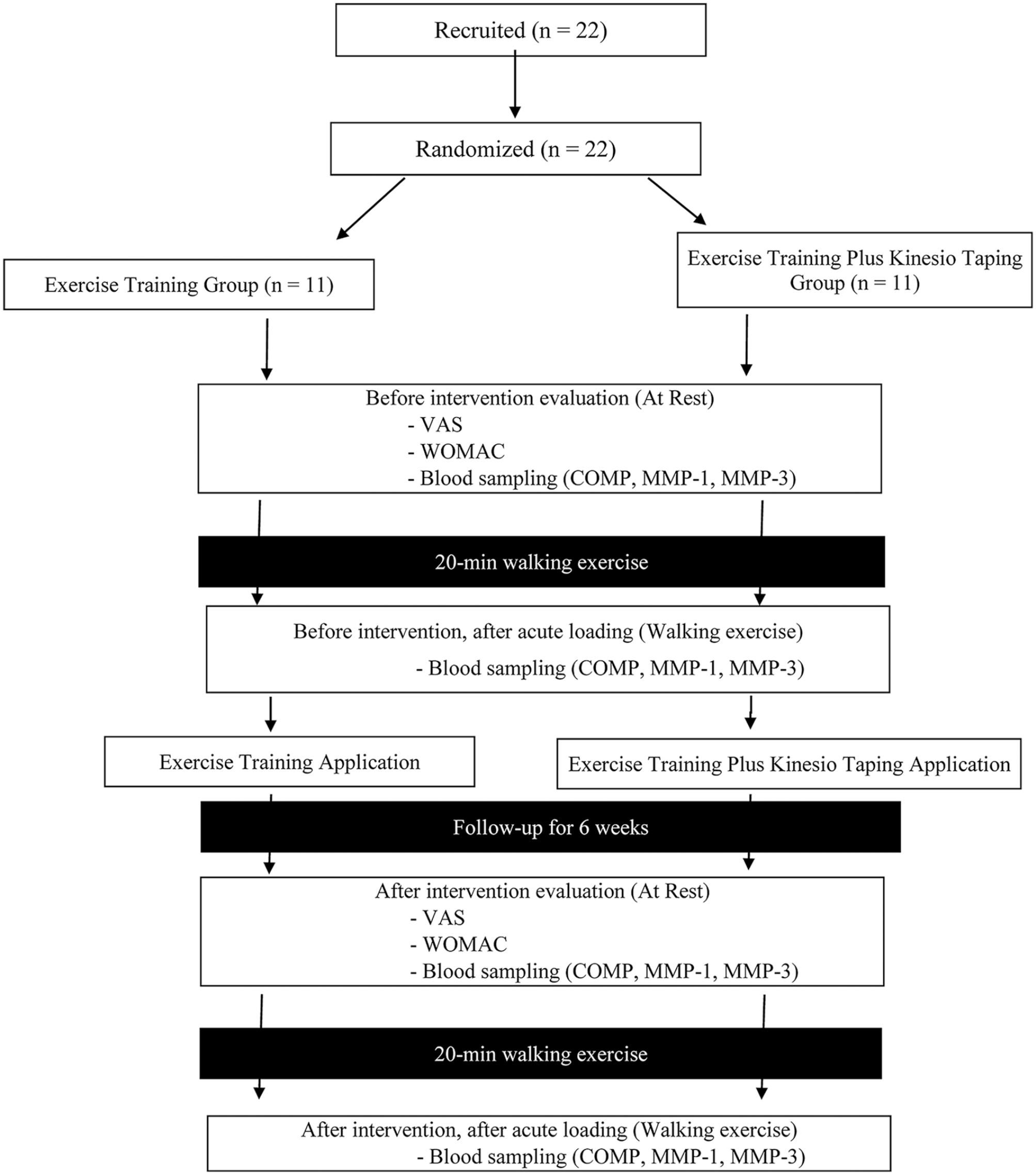
Flowchart of study design.
Interventions
Exercise Training Protocol
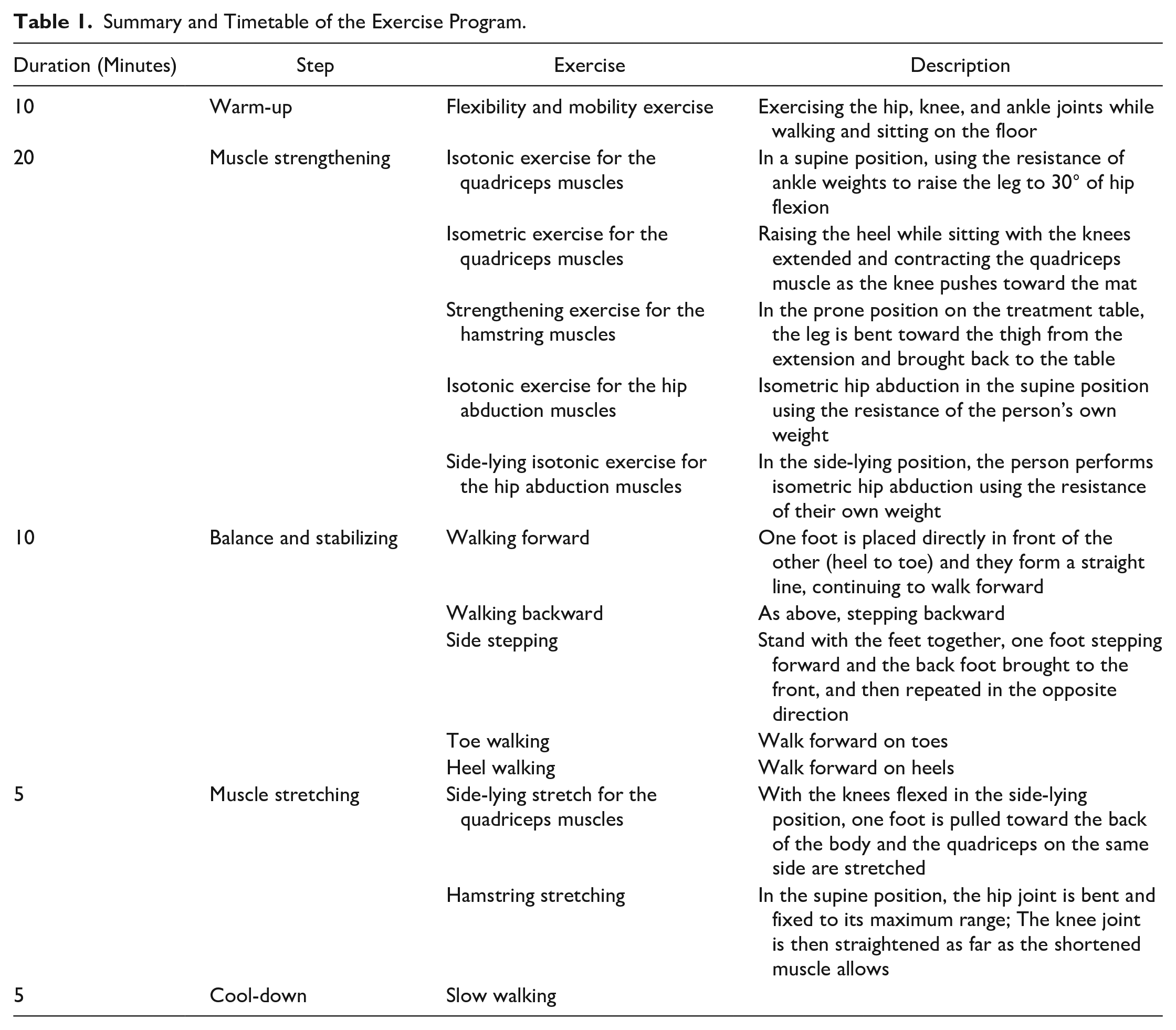
The exercise training consisted of 6 weeks of training with 3 days per week. This program was designed based on the recommendation of the American Geriatrics Society. 43 Each exercise session consisted of a total of 50-minute sessions of 10 minutes of warm-up, 20 minutes of resistance, 10 minutes of balance and stabilization, 5 minutes of lower limb stretching, and 5 minutes of cool-down exercises ( Table 1 ). All sessions were supervised by a trained physiotherapist (first author). The 20 minutes of walking exercise was done before and after the intervention at the participants’ own walking speed.
Summary and Timetable of the Exercise Program.
Kinesio Tape Application
Kinesio taping was applied 3 times per week over the study period of 6 weeks by the same experienced physiotherapist (first author). Before the kinesio taping, the skin surface was cleaned. Patients were positioned lying on their side, hip extended, and knee joint at 60° of flexion. The knee was taped with an I-shaped kinesio tape starting at the origin of the rectus femoris, and a Y-shaped kinesio tape proximal to the superior patellar border. The taping had no tension at its base, whereas the portion between the anchor and the superior patella was stretched ≈40% ( Fig. 2 ). After 48 hours, the kinesio tape was removed from the skin and each subject was examined for any skin sensitivity.

Kinesio taping applications used in the study.
Collection and Storage of Blood Samples
Blood samples were obtained 24 hours after the last training session at rest and immediately after the 20 minutes of walking exercise before and after the interventions using a standard venipuncture at a constant room temperature ( Fig. 1 ). While blood samples were transferred to nonadditive tubes to obtain serum, they were transferred to EDTA (ethylenediaminetetraacetic acid)-coated tubes to obtain plasma. Samples were centrifuged at 5000 × g at 4 °C for 15 minutes and stored at −80 °C until time of analysis.
Outcome Measures
Knee-Related Pain and Health Status
Pain and physical function outcomes were evaluated at the beginning and at the end of the intervention period by the visual analogue scale (VAS) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), respectively.
Pain intensity was evaluated by the VAS. In this test, each subject was asked to state her perceived pain at rest, during activity, and during the night. 44 The WOMAC is a reliable and valid functionality test commonly used in patients with knee OA. This scale contains 24 items and is assigned into 3 subunits: pain, stiffness, and physical function and a Likert-type scale was used for scoring each item. 45
Biochemical Analysis
Serum COMP and plasma MMP-1 and MMP-3 levels were measured blood samples obtained at rest and following 20 minutes of walking exercise before and after the interventions. The serum COMP level was quantified via enzyme-linked immunosorbent assay (ELISA) according to the manufacturer’s instructions (Cat. no: 201-12-1487, Sunred Biological Technology, Shanghai, People’s Republic of China). The minimum detection level was about 0.283 ng/mL. Intra- and interassay coefficient of variation (CV) were 10.0% and 12.0%, respectively. The COMP level was expressed as ng/mL. Plasma MMP-1 level was measured using commercial ELISA kit (Cat. no: 201-12-0917, Sunred Biological Technology, Shanghai, People’s Republic of China), according to the producer’s recommendations. The minimum detection level was about 0.207 ng/mL. The MMP-1 level was expressed as ng/mL. Plasma MMP-3 level was analyzed using commercially available ELISA kit (Cat. no: BMS2014/2, Affymetrix, eBioscience, BenderMed Systems GmbH, Germany), according to the manufacturer’s recommendations. The minimum detection level was about 0.008 ng/mL. Intra- and interassay CV of the kit were 5.8% and 3.0%, respectively. The MMP-3 level was expressed as ng/mL.
Statistical Analysis
Statistical analysis was performed with SPSS v.22.0 for Windows (IBM Corp., Armonk, NY, USA). Data expressed as mean ± standard deviation (SD). The normality of the distribution of the data was evaluated by the Shapiro-Wilk test and statistical difference between the groups was analyzed by Student t test for parametric data and Mann-Whitney U test for nonparametric data. Intragroup comparisons were evaluated with paired t test for parametric data and Wilcoxon signed rank test for nonparametric data. A P value of less than 0.05 was considered statistically significant.
Results
Participants’ Characteristics
All participants completed the study, and there were no participants who could not complete the study. The mean age of the participants in the ET and ET + KT groups were 51.00 ± 3.69 and 48.18 ± 7.56 years, respectively, and there was no difference between the groups (P > 0.05). The baseline characteristics of the groups are shown in Table 2 . No statistically significant differences were found regarding weight, height or body mass index between the groups before and after the intervention (P > 0.05).
Baseline Characteristics of Participants in This Study. a
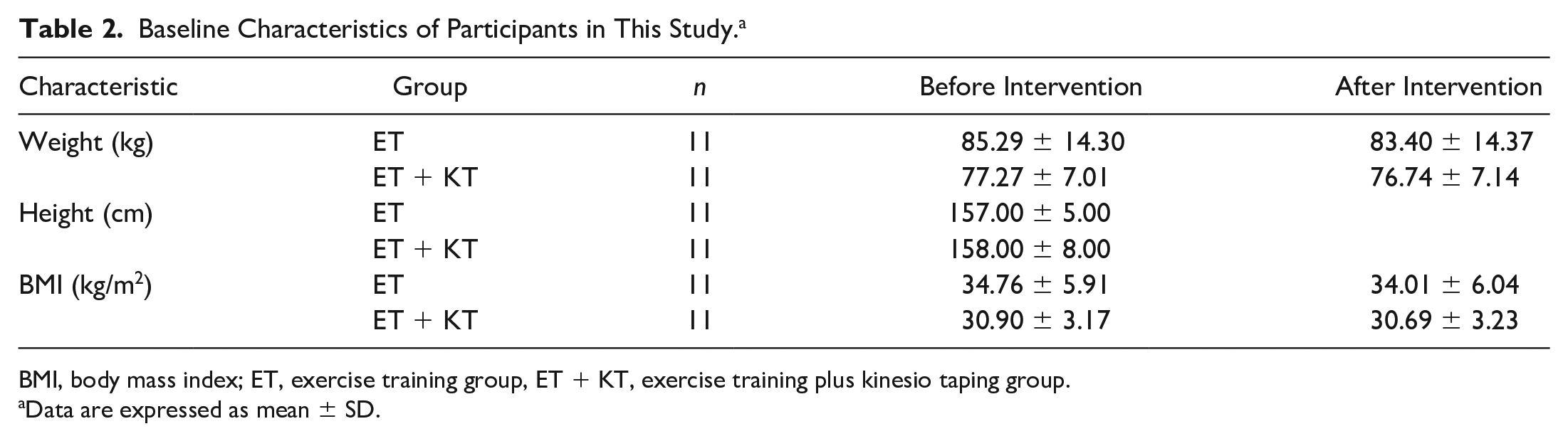
BMI, body mass index; ET, exercise training group, ET + KT, exercise training plus kinesio taping group.
Data are expressed as mean ± SD.
Changes in Pain and Functionality Scores
Intragroup comparison of the ET and ET + KT groups showed that the VAS and the WOMAC scores were lower after the intervention when compared with before the intervention in both groups (P < 0.05). However, there were no statistically significant differences between the groups before and after the intervention (P > 0.05) ( Table 3 ). These results indicate that there is no significant difference in pain and function following exercise training and exercise training plus kinesio taping.
Comparison of VAS and WOMAC Scores Between Groups.
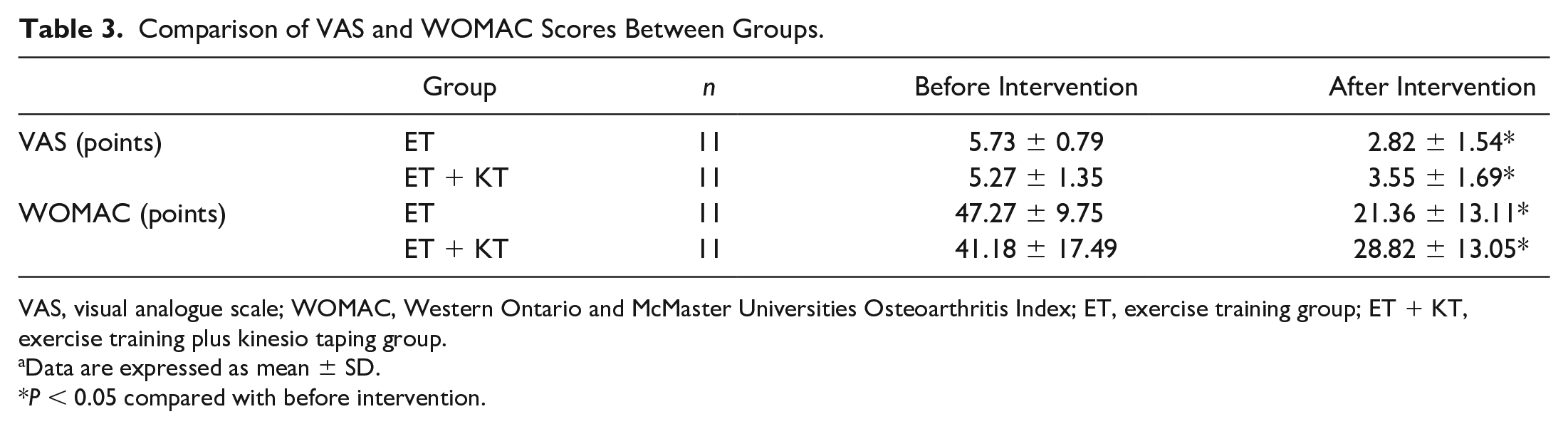
VAS, visual analogue scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; ET, exercise training group; ET + KT, exercise training plus kinesio taping group.
Data are expressed as mean ± SD.
P < 0.05 compared with before intervention.
Changes of Biochemical Markers at Rest Before and After Interventions
Table 4 presents the circulating COMP, MMP-1, and MMP-3 levels before and after the interventions. There was no statistically significant difference between before and after the intervention in regarding the resting serum COMP and plasma MMP-1 levels in both groups (P > 0.05). In the ET group, plasma MMP-3 level was lower after the intervention than before the intervention (P < 0.05), but in the ET + KT group there was no statistically significant change between before and after the intervention at rest (P > 0.05). However, there was no statistically significant difference between the groups before and after the intervention periods (P > 0.05). These data indicate that neither exercise training alone nor exercise training plus kinesio taping affected circulating COMP, MMP-1, and MMP-3 levels at rest.
Effects of Exercise Training Alone or in Combination With Kinesio Taping on Biomarkers of the Knee OA. a
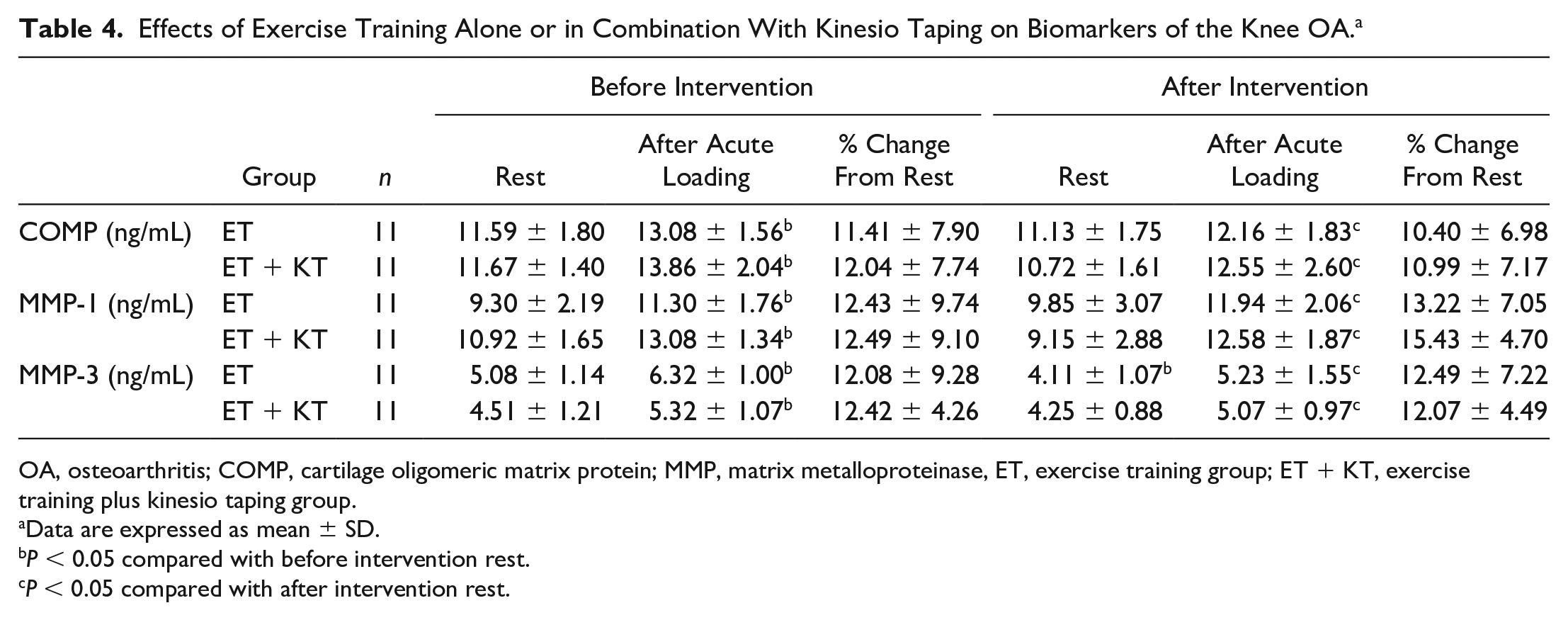
OA, osteoarthritis; COMP, cartilage oligomeric matrix protein; MMP, matrix metalloproteinase, ET, exercise training group; ET + KT, exercise training plus kinesio taping group.
Data are expressed as mean ± SD.
P < 0.05 compared with before intervention rest.
P < 0.05 compared with after intervention rest.
Changes in COMP, MMP-1, and MMP-3 Levels in Response to Acute Loading Before and After Interventions
Circulating COMP, MMP-1, and MMP-3 levels were higher immediately after the 20 minutes of walking exercise than at rest in the ET and ET + KT groups before and after the intervention (P < 0.05). Before intervention, COMP concentrations in the ET and ET + KT groups were elevated by 11% and 12%, respectively. However, after the intervention, COMP levels in the ET and ET + KT groups were increased by 10% and 11%, respectively. Before the intervention, in both groups, MMP-1 and MMP-3 concentrations were increased by 12%. However, after the intervention, MMP-1 levels in the ET and ET + KT groups were elevated by 13% and 15%, respectively, and MMP-3 levels in both groups were increased by 12% ( Table 4 ). These data show that COMP, MMP-1, and MMP-3 levels increased in response to acute exercise, but neither exercise training alone nor exercise training plus kinesio taping affected COMP, MMP-1, and MMP-3 levels in response to acute exercise.
Discussion
In this study, we sought an answer to the question that does exercise training alone and in combination with kinesio taping improve pain, functionality and circulating COMP, MMP-1, and MMP-3 levels in patients with knee OA. The straight answer to this research question based on the results of the study is partially yes. Our results did not show a significant difference between exercise training and exercise training plus kinesio taping groups in terms of parameters of pain and functionality namely, VAS and WOMAC and circulating COMP, MMP-1, and MMP-3 levels. Despite that some changes occurred in pain, functionality, and biochemical markers with exercise training and exercise training plus kinesio taping, no difference was evident between the groups.
In this study, pain was assessed by VAS and functional status by WOMAC, and exercise training caused a decrease in VAS and WOMAC scores. Consistent with our findings, quadriceps strengthening exercises alone 46 or in combination with different exercise training protocols such as hamstring strengthening47,48 and flexibility 49 exercise have been shown to be useful in improving pain and reducing functional performance limitations in patients with knee OA, as measured by VAS and WOMAC. In the present study VAS and WOMAC scores also decreased after the exercise training plus kinesio taping. There are conflicting findings regarding the effectiveness of kinesio taping on pain and functionality in knee OA. VAS and WOMAC scores have been reported to decrease39,41,50,51 or not change 42 in response to kinesio taping. These differences in results may be due to the evaluation time, duration of kinesio taping, differences in taping methods and characteristics of the patient group. In this study, we did not observe additional beneficial effect of kinesio taping on VAS and WOMAC scores. The possible explanation for the absence of any changes between the groups in this study may be due to the similar mechanism of action of exercise training and kinesio taping. During kinesio taping application, skin mobilization increases blood and lymph circulation and stimulates of cutaneous mechanoreceptors. 39 These mechanisms are also stimulated by exercise, and these factors are believed to directly affect pain perception and function. 52
One of the primary objectives of this study was to compare resting COMP level before and after interventions. In this study, exercise training and exercise training plus kinesio taping did not affect resting serum COMP level. There are conflicting findings suggesting that exercise training for 6 to 12 weeks increases34,53 or does not affect17,54 serum COMP levels in patients with knee OA. The differences between the results may be due to the type, duration, and intensity of exercise training programs and differences in patients’ characteristics. In this study, unchanged resting COMP levels in response to exercise training and exercise training plus kinesio taping suggest that these interventions are safe and do not cause any adverse changes on COMP turnover and cartilage metabolism. To our knowledge no study has so far investigated the effects of kinesio taping or exercise training plus kinesio taping on COMP level, and our study is the first in this regard. In this study, there was no difference between exercise training and exercise training plus kinesio taping groups, suggesting that kinesio taping did not have an additional effect on resting COMP level in these patients.
One of the secondary objectives of this study was to investigate the changes in circulating COMP level following acute loading in patients with knee OA. In this study, serum COMP level increased immediately after 20 minutes of walking exercise performed before and after the interventions. However, although the magnitude of the post-intervention increase was smaller, it was not statistically significant in either group. Consistent with our findings,17,33,49 it has been reported in many studies that serum COMP levels increase in patients with knee OA after 30 minutes to 1 hour of walking exercise. In this study, possible reasons for the increase in serum COMP levels during exercise are mobilization of COMP from cartilage or other pressure loaded tissues, and modifications to the extra cartilage cycle of COMP. In addition, high levels of COMP in serum samples may indicate evidence of cartilage damage. In the present study, no difference between exercise training and exercise training plus kinesio taping groups, which suggests that kinesio taping has no additional effect on resting COMP level in patients with knee OA.
In the knee OA, mild to moderate inflammatory reactions may occur in the synovial membrane. During synovial inflammation, synoviocytes produce cartilage-disrupting enzymes such as MMPs that reduce cartilage volume. 55 In this study, although exercise training and exercise training plus kinesio taping did not affect resting MMP-1 levels, plasma MMP-3 levels were decreased in the exercise training group. In addition, MMP-1 and MMP-3 levels increased immediately after 20 minutes of walking exercise compared with resting levels before and after the interventions. Consistent with our findings, knee flexion-extension and isometric quadriceps exercises have been shown to reduce MMP-3 levels in synovial fluid in patients with knee OA. 52 These data indicate that exercise training may prevent inflammatory reaction to chondrocytes and cartilage matrix, delay articular cartilage degeneration, and thus improve knee function. To the best of our knowledge, no studies have examined the effects of kinesio taping or exercise training plus kinesio taping on MMP-1 and MMP-3 levels at rest and after exercise in knee OA. Therefore, our study is a first in this regard. In this study, the lack of difference between exercise training and exercise training plus kinesio taping groups suggests that kinesio taping did not have additional effect on MMP-1 and MMP-3 levels in knee OA patients.
Although these results provide new information, this study has some limitations. First, biomarker concentrations were measured in serum and plasma samples representing systemic levels, not in knee synovial fluid. Second limitation is the absence of only kinesio taping group to better evaluate and compare the effectiveness of the interventions. Third, patients’ physical activity levels were not recorded before and during treatment. Fourth, in this study, we selected cartilage biomarkers that are considered potential biomarkers in knee OA, but other biomarkers such as pro- or anti-inflammatory cytokines can also provide us with useful information. Finally, muscle strength was not assessed before and after the intervention due to the technical difficulties.
This study has shown that exercise training and exercise training plus kinesio taping may improve pain and functionality independently of cartilage biomarkers such as COMP, MMP-1, and MMP-3. Exercise training and exercise training plus kinesio taping protocols have no detrimental effect on cartilage metabolism. However, acute exercise increases cartilage turnover and levels and activity of the proteolytic enzymes. As the clinical significance of the observed effects of the exercise training plus kinesio taping is questionable, more detailed future studies utilizing a longer period are required especially at the molecular level to explain the possible mechanism of actions.
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Selçuk University Scientific Research and Project Committee (Grant No. 16202028).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethics Committee of Selçuk University (approval no. 2016/101, 30/03/2016) and all experiments were carried out in accordance with the Helsinki Declaration.
Informed Consent
Signed informed consent forms were obtained from all participants.