
Abstract
Objective
The purpose of this study is to assess if incident radiographic osteoarthritis (OA) is associated with clinical OA symptoms at midterm follow-up after arthroscopic partial medial meniscectomy (APMM).
Design
A total of 44 patients (43% females, mean age 50.1 ± 2.8 years, minimum 5.6-year follow-up) with isolated medial meniscal tears and no-to-mild preoperative radiographic OA underwent APMM. Incident radiographic OA was assessed using the modified Kellgren-Lawrence (K-L) classification. Patients completed the Knee Injury and Osteoarthritis Outcomes Score (KOOS), and subscale thresholds for assessment of a symptomatic knee (KOOS OA criteria) and for Patient non-Acceptable Symptom State (PASS-N) following anterior cruciate ligament reconstruction (ACL-R) were calculated.
Results
Incident medial compartment OA occurred in 50% of patients. Morbidly obese patients (body mass index ≥35 kg/m2) were more likely to demonstrate incident radiographic OA (100% vs. 41%, P = 0.002). Forty-three percent of patients met KOOS OA criteria, while 77% were PASS-N. Females were more likely to meet KOOS OA criteria (73% vs. 21%, P = 0.009). Patients with incident radiographic OA in any compartment were more likely than those without radiographic OA to meet KOOS OA criteria (71% vs. 17%, P = 0.008). Patients with preoperative K-L grade 2 changes in any compartment were more likely to meet KOOS OA criteria than those without K-L grade 2 changes in any compartment (83% vs. 35%, P = 0.037).
Conclusions
Roughly half of APMM patients will have incident radiographic OA within 6 years of APMM, and this risk increases with obesity. Females and patients with incident radiographic OA are more likely to meet clinical thresholds for OA.
Introduction
Arthroscopic partial medial meniscectomy (APMM) is the most commonly performed orthopedic procedure in the United States.1-3 However, APMM does not slow the progression of osteoarthritis (OA).4-6 OA following meniscectomy has been reported in 30% to 75% of patients at mid- to long-term follow-up.4-7 Previous studies have investigated the relationship between radiographic OA and clinical symptoms following meniscectomy at mid- to long-term follow-up.8-10 However, there remains limited information to date on the association between the radiographic progression of OA and clinical symptoms following APMM.
Englund et al. 8 performed a case-control study to determine the impact of meniscus tear type on symptomatic and radiographic OA in patients largely undergoing open subtotal meniscectomy, demonstrating a high risk of radiographic and symptomatic tibiofemoral OA at mean 16-year follow-up. In another study using the same research database, this group evaluated the influence of various risk factors on the development of symptomatic OA following meniscectomy at 15- to 22-year follow-up. 10 They reported an association of obesity and female sex with symptomatic radiographic OA. More recently, Longo et al. 9 corroborated the above findings, reporting a high prevalence of radiographic OA at 5 to 12 years following APMM, with worse outcomes associated with lateral meniscectomy. In addition, these authors reported a correlation between radiographic and clinical OA. 9 However, the studies cited above each included patients with meniscal tears in both compartments and contained a relatively high proportion of patients with preoperative OA within the meniscectomized compartment.8,9
In this study, we aim to determine if incident radiographic OA is associated with the development of a symptomatic knee consistent with clinical OA at midterm follow-up following APMM. Secondarily, we aim to determine the association of demographic factors with radiographic and clinical OA. We hypothesize that patients undergoing APMM are likely to go on to incident radiographic OA at midterm follow-up, and patients with incident radiographic OA are likely to have clinical symptoms of a symptomatic knee.
Methods
Patients
A retrospective review was performed of all patients presenting to a single surgeon’s practice in the Midwest United States who prospectively consented to participate in this research study between May 1, 2010 and December 1, 2011. Patients eligible for inclusion had a painful knee, a magnetic resonance imaging demonstrating isolated medial meniscus tear and underwent APMM for symptomatic isolated medial meniscus tear. Patients were excluded if they had Kellgren-Lawrence (K-L) grade 3 or higher OA within any knee compartment (medial, lateral, or patellofemoral), focal ICRS (International Cartilage Repair Society) grade 3 or higher chondral injury, varus or valgus deformity of more than 5°, cruciate ligament injury, age greater than 70 years at the time, or surgery or history of contralateral knee meniscectomy. Mean follow-up was (±95% CI) 6.2 ± 0.4 years (range 5.6-8.0 years). All patients underwent a single series of knee radiographs (standing AP, Rosenberg, lateral and merchant views) at the time of the initial preoperative clinic visit and at final follow-up. Baseline age, sex, and body mass index (BMI) were collected and recorded.
Radiographic Evaluation
A musculoskeletal-trained academic radiologist, blinded to clinical follow-up data graded the preoperative and final follow-up radiographs of the operative and contralateral knee according to the modified K-L classification system of OA ( Fig. 1 ).11,12 The modified K-L classification allows for patients to be dichotomized as having “incident OA,” defined as joint space narrowing and an osteophyte, with at least one of these being new, 12 or “no incident OA.” A K-L grade was assigned to each knee compartment (medial, lateral and patellofemoral). Patients were dichotomized as having “incident OA” or “no incident OA” within the medial compartment. Patients were also dichotomized as having “incident OA” or “no incident OA” within any knee compartment. There were no differences in preoperative K-L grade according to age, sex, or BMI.
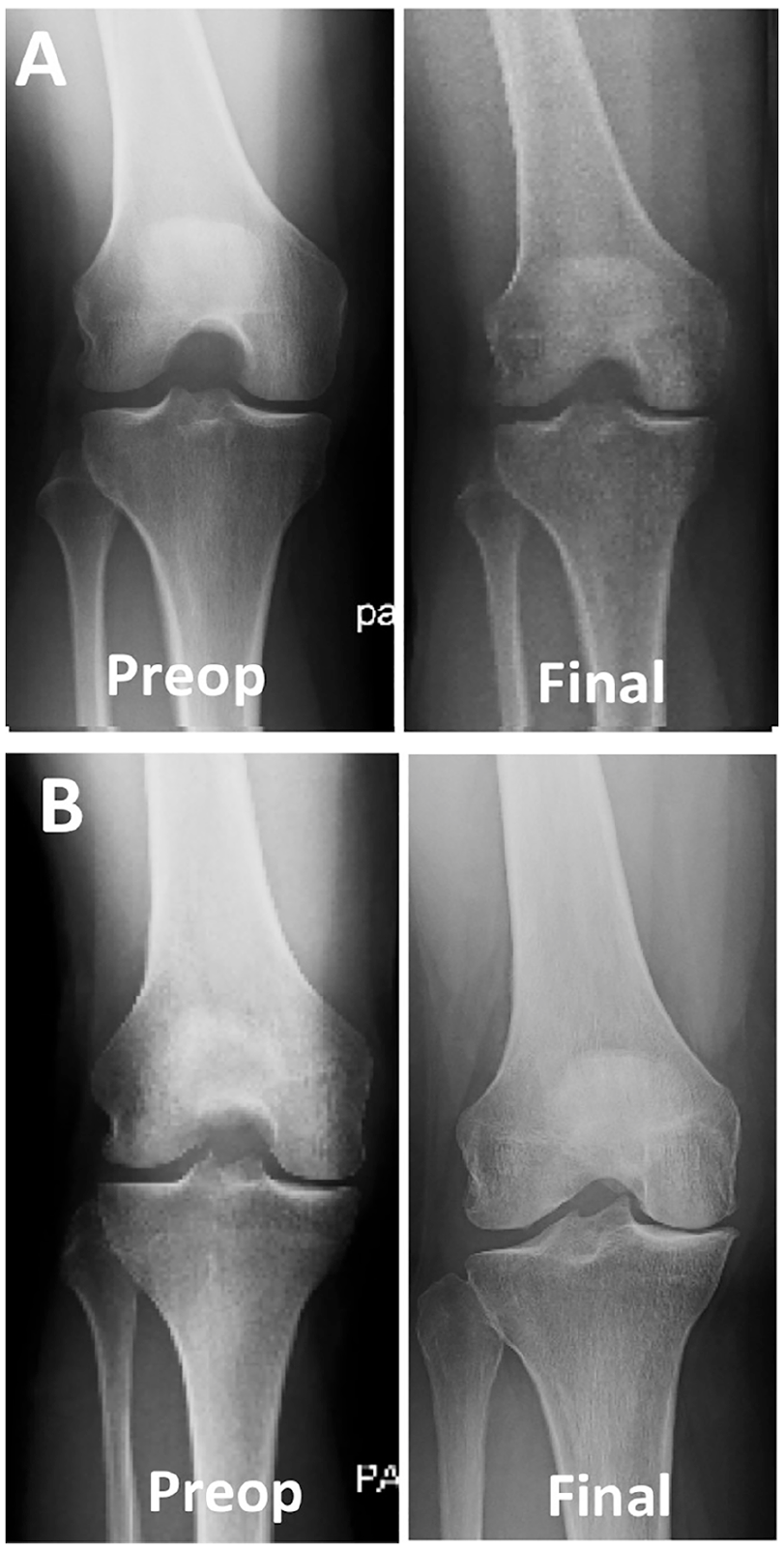
Preoperative and final follow-up radiographs of 2 patients. (
Clinical Evaluation
At final follow-up, patients completed the Knee Injury and Osteoarthritis Outcome Score (KOOS). 13 Patients were categorized as having “clinical OA” if they met the clinical definition of a symptomatic knee based on KOOS subscale thresholds as previously described. 8 Clinical OA has previously been defined 8 as the score for the KOOS subscale quality of life (QOL) ≤87.5 and 2 of the 4 additional subscales should be equal to or less than the score obtained as follows: Pain ≤86.1, Symptoms ≤85.7, Activities of Daily Living (ADL) ≤86.8, Sport/Recreation ≤85.0. Established KOOS subscale thresholds for the Patient Acceptable Symptom State (PASS) after ACL reconstruction (ACL-R) were also determined. Muller et al. 14 previously defined an acceptable symptoms state (PASS-Y[yes]) as KOOS subscale QOL ≥ 62.5, Pain ≥ 88.9, symptoms ≥ 57.1, ADL ≥ 100 and Sport/Recreation ≥ 75.0. Patients not meeting these thresholds were considered not in an acceptable symptoms state (PASS-N[no]).
Research Ethics and Patient Consent
Written and signed informed consent was obtained from all study participants. The study was approved by the Washington University Institutional Review Board (IRB #201509165).
Statistics
The primary outcome measures were incident radiographic OA within the medial compartment and clinical OA based on postoperative KOOS scores. Secondary outcome measures included incident radiographic OA within any compartment and PASS based on postoperative KOOS scores. Continuous variables are reported as means and standard deviations in the descriptive analysis. Frequencies and percentages are used to report descriptive statistics of discrete variables. McNemar’s tests were used to evaluate the differences on dichotomous dependent variable of incident OA between the operated knee and the paired contralateral knee. Similar tests were done compare the percentage of incident OA on the medial, lateral, and patellofemoral components. Nonparametric Mann-Whitney U tests were used to compare the continuous variables between all outcomes. Chi-square analyses (or Fisher’s exact tests when sample sizes were appropriate) were used to analyze discrete variables between outcomes. Multivariable logistic regression models were generated to assess the risk factors of age, sex, and BMI with the outcome of incident OA and all other secondary outcomes. Odds ratios and 95% confidence intervals were used to report the magnitude (and precision) of the association with the outcomes. Statistical significance was defined as P values of 0.05 or lower. All analyses were conducted using SPSS version 23.0 (IBM Corp., Armonk, NY).
Results
Forty-four patients with an isolated medial meniscal tear and no to mild preoperative OA (K-L grade 0, 1, or 2) consented for the study and underwent APMM ( Table 1 ). Twelve patients (21.4%) were lost to follow-up.
Characteristics of Study Patients.
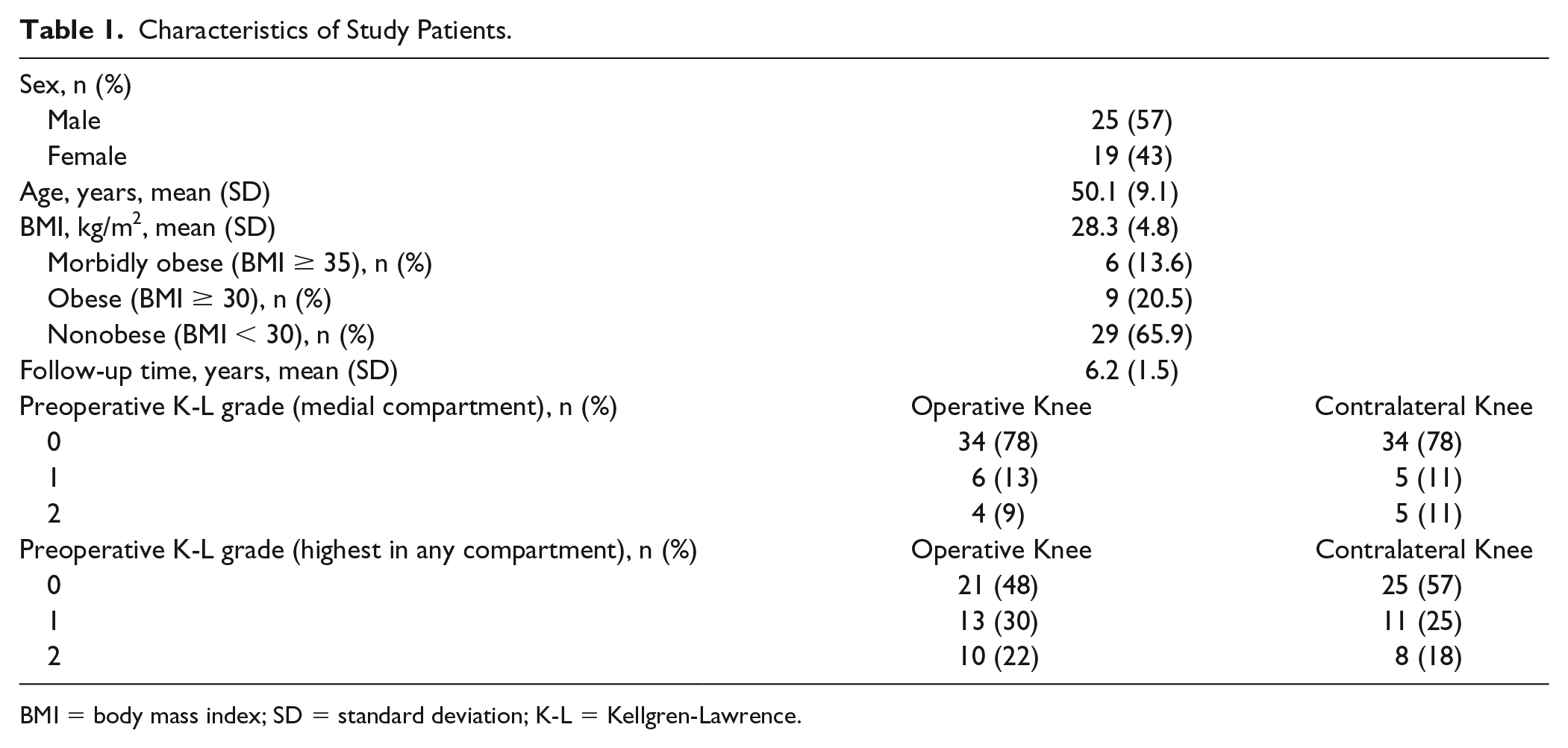
BMI = body mass index; SD = standard deviation; K-L = Kellgren-Lawrence.
Fifty percent of patients had incident radiographic OA in the medial compartment, significantly higher than the incident radiographic OA observed in the contralateral knee ( Table 2 ).
Incident Radiographic OA and Clinical Outcomes by Knee Compartment.
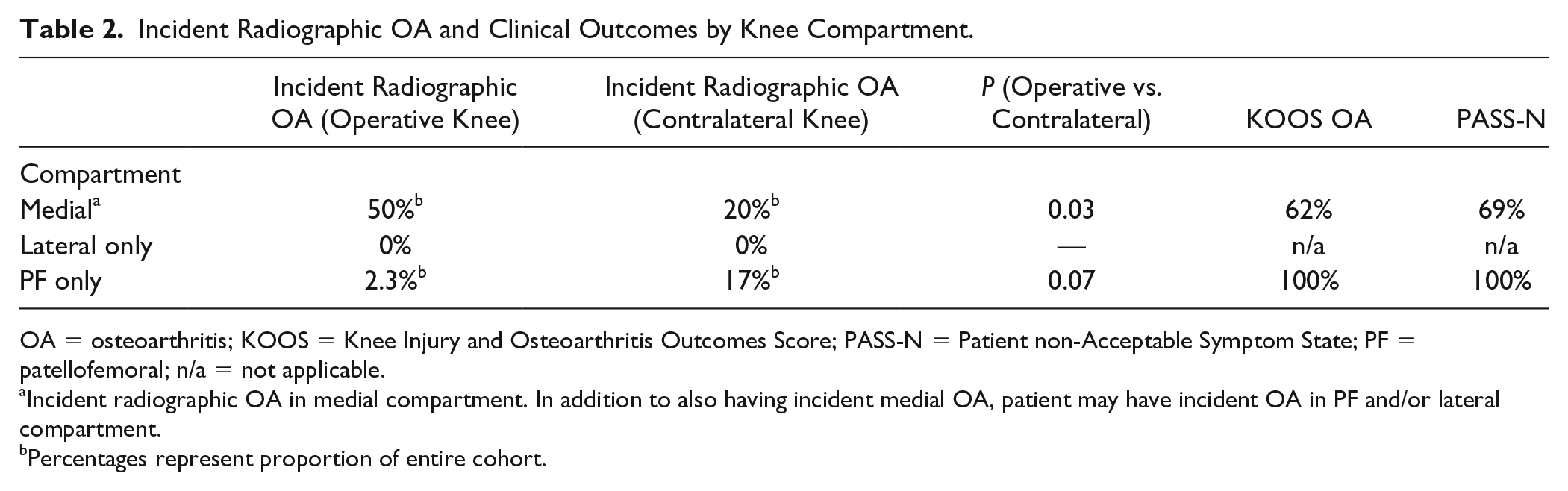
OA = osteoarthritis; KOOS = Knee Injury and Osteoarthritis Outcomes Score; PASS-N = Patient non-Acceptable Symptom State; PF = patellofemoral; n/a = not applicable.
Incident radiographic OA in medial compartment. In addition to also having incident medial OA, patient may have incident OA in PF and/or lateral compartment.
Percentages represent proportion of entire cohort.
Association between Clinical and Radiographic OA
Of all patients with clinical OA, 83% had incident radiographic OA in any compartment, and 75% had incident radiographic OA in the medial compartment. Patients with incident radiographic OA in any compartment or in medial compartment were more likely than those without incident radiographic OA in any compartment (67% vs. 18%, P = 0.021) or in medial compartment (62% vs. 18%, P = 0.047) to have clinical OA. Patients with preoperative K-L grade 2 changes in any compartment were more likely to have clinical OA at follow-up than those without K-L grade 2 changes in any compartment (83% vs. 35%, P = 0.037).
Association of Patient Characteristics with Outcomes
Females were more likely than males to have clinical OA (73% vs. 21%, P = 0.009), with a substantial trend toward females being more likely to develop incident radiographic OA in any compartment (67% vs. 40%, P = 0.10). There was no significant difference between obese patients (BMI ≥30 kg/m2) and nonobese patients (BMI <30 kg/m2) in developing incident radiographic OA in any compartment (60% vs. 44%, P = 0.33). However, there was a difference between morbidly obese patients (BMI ≥35 kg/m2) and nonobese patients (100% vs. 44%, P = 0.02) and between morbidly obese patients and all other patients (100% vs. 41%, P = 0.02) in developing incident radiographic OA in any compartment. We did not find any association between obesity and clinical OA or between age, sex, or obesity and PASS thresholds.
Multivariable logistic analysis demonstrated that females were more likely than males to have clinical OA at follow-up (OR 9.1, 95% CI 1.3-50).
PASS Criteria
Of all patients meeting PASS-N criteria, 55% had incident radiographic OA in any compartment, and 50% had incident radiographic OA in the medial compartment. Among patients with incident radiographic OA in any compartment 73% met PASS-N criteria, and among patients without incident radiographic OA in any compartment, 82% met PASS-N criteria.
Discussion
At mid-term follow-up following APMM, half of patients developed incident radiographic OA, and greater than two thirds of these patients also had clinical evidence for OA. Females were more likely than males to have clinical OA. Morbidly obese patients were more likely to develop incident radiographic OA. Patients who developed incident radiographic OA, whether in the medial compartment or in any knee compartment, were also more likely to have clinical OA than patients who did not develop incident radiographic OA. Patients with preoperative OA in any compartment were more likely to have clinical OA at final follow-up than those without preoperative radiographic OA. To our knowledge, this is the first study to demonstrate that the development of incident radiographic OA within the medial compartment, or any compartment of the knee, following APMM is associated with clinical symptoms of OA at mid-term follow-up.
A recent review discussed the biomechanical consequences and clinical outcomes following APMM 15 and it is well known that meniscal resection results in increased tibiofemoral contact pressures, with progressively larger amounts of resection resulting in further increases in contact pressures. 16 Predictors of poor clinical outcome include female sex, increased BMI, focal chondral injuries, ACL insufficiency, and tibiofemoral malalignment. 15 A systematic review of outcomes following APMM found increased joint space narrowing at 4.5 years after surgery among patients older than 40 years compared with those younger than 40 years, but no correlation was found between radiographic OA severity and clinical outcomes.17,18 A systematic review of relatively younger patients (mean age 19-38.5 years) undergoing APM found that the operative knee had earlier radiographic signs of OA compared with the contralateral knee, but again clinical symptoms did not correlate with radiographic OA severity. 19 The findings of the current study corroborate several of the above findings, including a higher incidence of clinical symptoms among female patients and obese patients. However, contrary to previous studies, we demonstrate that the development of radiographic OA following APMM is associated with more significant clinical symptoms at intermediate follow-up. This suggests that minimizing resection at the time of APMM15-17 can, by decreasing the radiographic progression of OA, have a clinical benefit.
Previous studies have investigated the association of radiographic OA and clinical symptoms following meniscectomy. Englund et al. 8 reported on patients who underwent medial or lateral meniscectomy at mean 16-year follow-up, and of note only 17% were female. Nearly 70% of patients underwent open meniscectomy, with 60% undergoing subtotal meniscectomy. 8 Preoperative radiographic changes were not reported, but up to 1/3 of patients had cartilage changes at the time of surgery involving of at least one knee compartment. 8 Similar to the present study, the authors utilized KOOS subscale thresholds for clinical OA. 8 The authors reported a prevalence of radiographic OA in 41.6% of patients following medial meniscectomy, with 24.9% meeting criteria for both clinical and radiographic OA. In the study by Englund et al., 8 the authors defined radiographic OA in a fundamentally similar manner as in the present study, approximating K-L grade 2 OA. 11 We report a similar incidence of radiographic OA at midterm follow-up; however, a markedly higher number of patients with incident radiographic OA also had clinical OA (67%) than in Englund et al. 8 Additionally, Englund et al. 8 had 20% obese patients while the present study had a higher proportion (35%). The authors did not investigate the association between morbid obesity and clinical or radiographic outcomes. In another study using the same research database, 8 the same group 10 evaluated the influence of various risk factors on the development of symptomatic OA following meniscectomy at 15- to 22-year follow-up. Symptomatic radiographic OA was evident in 27% of patients, with a higher incidence of radiographic OA among obese patients. 10 The authors also reported an association of obesity and female sex with symptomatic radiographic OA. Despite these observations, the findings from the above 2 studies are likely less generalizable to all populations, as they were performed about 45 years ago, with a predominately male population in a specific region (Sweden), and most patients underwent open subtotal meniscectomy. Similar to previous studies, we demonstrate a higher incidence of clinical symptoms among female patients post meniscectomy and an association of elevated BMI with radiographic OA. 10 However, interestingly, we found a higher incidence of symptomatic radiographic OA following APMM compared with previous reports following open subtotal meniscectomy.8,10
In a recent study, Longo et al. 9 reported a relatively high incidence of preoperative radiographic OA (8% to 27% depending on preoperative weight and location of tear) in a retrospective case series of patients undergoing APMM at 5- to 12-year follow-up. Rates of radiographic OA following APM were similar to the present study, ranging from 42% to 100% depending on sex, BMI, and knee compartment. While the authors did not utilize KOOS thresholds for clinical OA, they reported significant correlations between patient-reported clinical outcomes scores (KOOS and WOMAC [Western Ontario and McMaster Universities Osteoarthritis Index]) with radiographic OA, also reporting a higher incidence of radiographic OA progression among obese patients compared to non-obese patients. The authors did not investigate the association between morbid obesity and clinical or radiographic outcomes.
The association of radiographic knee OA and clinical symptoms of knee pain remains poorly characterized. Numerous studies have suggested that the severity of a patient’s radiographic OA correlates poorly with symptoms.20-26 Bruyere et al. 27 investigated the association of radiographic OA severity and progression on pain and disability, finding that baseline radiographic degenerative changes were weakly correlated with WOMAC scores. While the authors demonstrated a small but statistically significant relationship between joint space narrowing and WOMAC pain subscale scores, they concluded that radiographic features poorly predict clinical outcomes in the setting of knee OA. 27 On the contrary, Fukui et al. 28 found that patients with progressive medial joint space narrowing had more severe symptoms, compared with those without medial joint space narrowing as assessed by the Japanese Knee Osteoarthritis Measure (JKOM) and visual analogue scale pain scores. While it remains unclear whether radiographic OA is associated with clinical symptoms in the setting of knee OA, the findings of the present study, consistent with other studies.8,10 suggest that radiographic OA progression following meniscectomy is correlated with symptomatic OA. We specifically demonstrate that radiographic OA progression following APMM is associated with clinical symptoms of OA at midterm follow-up.
Since there was no consensus on the definition of a symptomatic knee, the use of specific KOOS subscale score cutoffs has been established and validated, making it a reliable method for defining symptomatic OA.8,10,29 Moreover, other authors 14 have defined KOOS subscale score thresholds for the PASS for patients following ACL-R. In the present study, we sought to determine how these validated clinical outcome measures are associated with radiographic progression of OA specifically following APMM. We demonstrate that the previously established thresholds for clinical OA are significantly associated with radiographic OA progression, 8 while PASS thresholds are not useful in the setting of APMM. It warrants mention that the definition of a symptomatic knee created by Englund et al.,8,10 was initially established by author consensus, which is somewhat arbitrary in nature. Furthermore, the cutoffs used in this definition of a symptomatic knee are similar to subsequently described population-based reference KOOS scores. 30 Nonetheless, our findings suggest that a high proportion of patients with incident radiographic OA following APMM also meet criteria for a symptomatic knee. These results may be used to counsel patients preoperatively and in approaching symptomatic patients following APMM.
Limitations include the retrospective nature of the study without a control group. Additionally, baseline KOOS scores were only obtained at final follow-up. Although the cohort was not large, we were still able to report a significant associations of incident radiographic OA with clinical OA. Although we utilized both univariable and multivariable testing in our data analysis, the use of multiple univariable tests increases the risk of chance findings and is a limitation of the study. However, multivariable testing did confirm an association of female sex with clinical OA. In this study, we did not consider tear types (degenerative vs. traumatic), as it is often difficult to ascertain, particularly in a middle-aged patient cohort whether the etiology was truly degenerative, traumatic, or a combination.
In conclusion, greater than two-thirds of patients who developed incident radiographic OA also had clinical symptoms of OA. Females were more likely than males to have clinical OA at final follow-up, and morbidly obese patients were more likely to develop incident radiographic OA after APMM. PASS thresholds do not appear to be useful in assessing the clinical symptoms state following APMM. These results may be helpful when counseling patients who are considering or have undergone APMM to guide expectations regarding the development of OA and emphasize the importance of minimizing resection at the time of APMM. While there is a significant association between KOOS thresholds for OA and radiographic progression of OA following APMM, there is a need for improved patient-reported outcome measures that better correlate radiographic progression with clinical symptoms following APMM. Further studies with larger cohorts and longer-term follow-up can help better define the relationship between the progression of radiographic OA and clinical symptoms.
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Orthopaedic Research and Education Foundation (OREF) Resident Clinician Scientist Training Grant (grant number 18-014).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Washington University Institutional Review Board (IRB #201509165).
Informed Consent
Written and signed informed consent was obtained from all study participants.
Trial Registration
Not applicable.