
Abstract
Objectives
We aimed to compare the outcomes of exercise rehabilitation and conventional treatment in patients with knee osteoarthritis.
Methods
This trial included a total of 166 patients diagnosed with knee osteoarthritis; they were randomly divided into groups. The experimental group underwent systematic exercise rehabilitation, while the control group received naproxen (n = 28), diclofenac (n = 27), or celecoxib (n = 19). Improvement in symptoms, knee function, and quality of life were compared. SPSS Statistics 24.0 was used for the data analysis.
Results
The mean age of patients was 56.0 ± 10.5 years, and the average follow-up time was 12 ± 2.3 weeks. No statistically significant differences were seen in age, body mass index, and sex (P > 0.05) between the groups. The average Western Ontario and MacMaster Universities (WOMAC) scores after treatment were 84.4 ± 15.2, 108.3 ± 3.9, 107.4 ± 5.4, and 107 ± 6.0 in the exercise rehabilitation, diclofenac, naproxen, and celecoxib groups, respectively. The mean Lysholm scores were 60.3 ± 14.9, 41.0 ± 0.1, 43.5 ± 5.3, and 41.7 ± 3.6 in the exercise rehabilitation, diclofenac, naproxen, and celecoxib groups, respectively. The mean SF-36 (Short Form-36 Survey) scores were 105.4 ± 21.5, 82.5 ± 3.7, 84.2 ± 3.5, and 83.7 ± 5.0 in the exercise rehabilitation, naproxen, celecoxib, and diclofenac groups, respectively. The average ranges of knee motion were 125.0 ± 6.2°, 116.4 ± 1.4°, 114.7 ± 1.1°, and 115.7 ± 0.8° after exercise rehabilitation, diclofenac, naproxen, and celecoxib treatments, respectively. These data presented statistical differences between the groups.
Conclusion
Exercise better improved symptoms and quality of life in patients with knee osteoarthritis over a 12-week follow-up period than that achieved with nonsteroidal anti-inflammatory drugs and COX-2 inhibitors.
Introduction
The general aim of treatment in patients with knee osteoarthritis is to relieve pain, improve joint movement, and find nontargeted strategies to treat knee osteoarthritis. 1 During the last decade, clinical practices included the use of nonsteroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase-2 inhibitors (COX-2 inhibitors), and intraarticular injection of hyaluronic acid to reduce inflammation and relieve pain. 2 However, these conventional treatment methods have limitations, such as gastrointestinal side-effects. Moreover, their effectiveness in protecting the cartilage and delaying disease progression is controversial. 3 Some studies have suggested that regular exercise may help patients with knee osteoarthritis by reducing articular cartilage breakdown, relieve pain, and improve knee function and quality of life. 4
However, it remains unclear whether exercise rehabilitation can improve outcomes of patients with knee osteoarthritis under clinical conditions. Furthermore, the specific exercises that are suitable for patients with knee osteoarthritis are yet to be determined.
In this study, we hypothesized that exercise rehabilitation is better than treatment with conventional drugs in patients with knee osteoarthritis. In this study, we compared the outcomes of exercise rehabilitation and conventional treatment in patients with knee osteoarthritis. We also compared the outcomes achieved with naproxen, diclofenac, and celecoxib.
Methods
Patients and Study Design
The study was approved by The Second Hospital of Hebei Medical University Ethics Committee.
The inclusion criteria were as follows: (1) age 50 to 70 years, (2) diagnosis of knee osteoarthritis, (3) classified as Kellgren-Lawrence grades I to III with obvious symptoms ( Table 1 ), 5 and (4) patients who provided signed informed consent for inclusion into the clinical trial and agreed to comply with the protocol requirements of this study.
The Kellgren-Lawrence Classification of Osteoarthritis.
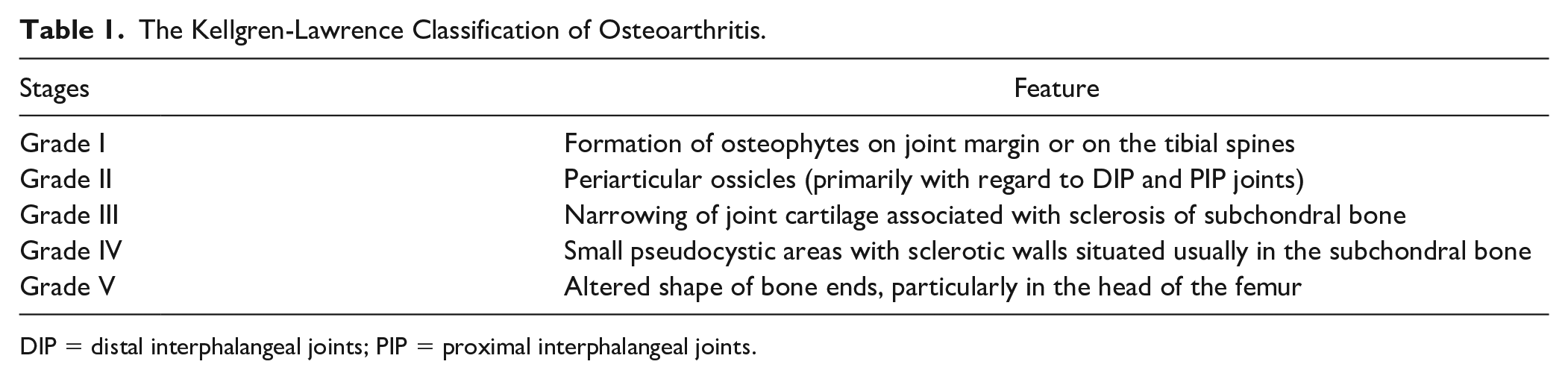
DIP = distal interphalangeal joints; PIP = proximal interphalangeal joints.
The exclusion criteria were as follows: (1) rheumatoid arthritis; (2) previous joint replacement; (3) severe organ failure, specifically patients with cardiovascular diseases, classified as New York Heart Association (NYHA) class III or IV, chronic kidney disease (CKD), classified as stage ≥3, and liver disease, with a Model of End-stage Liver Disease (MELD) score of ≥20; and (4) patients with severe mental illness.
Based on the inclusion and exclusion criteria, 185 patients diagnosed with knee osteoarthritis who were treated at The Second Hospital of Hebei Medical University between October and December 2018 were included.
Patients were randomly divided into 2 medication groups and an exercise rehabilitation group. As there were significant differences in the treatment among these 3 groups, no blinding was followed in this trial.
Intervention Methods
Generally, conventional treatment includes the administration of NSAIDs and COX-2 inhibitors. In this trial, naproxen and diclofenac were administrated to the patients, respectively. All patients in the conventional treatment group received the same drug dosage, while patients in the exercise rehabilitation group underwent the same physical therapy by the same physiotherapist.
The systematic exercise rehabilitation program mainly included lower limb static, dynamic, and flexibility exercises; exercises targeting the gluteus muscles; and core strength training for 20 minutes per day ( Table 2 ).
The Exercise Rehabilitation Training Plan for Patients With Knee Osteoarthritis.
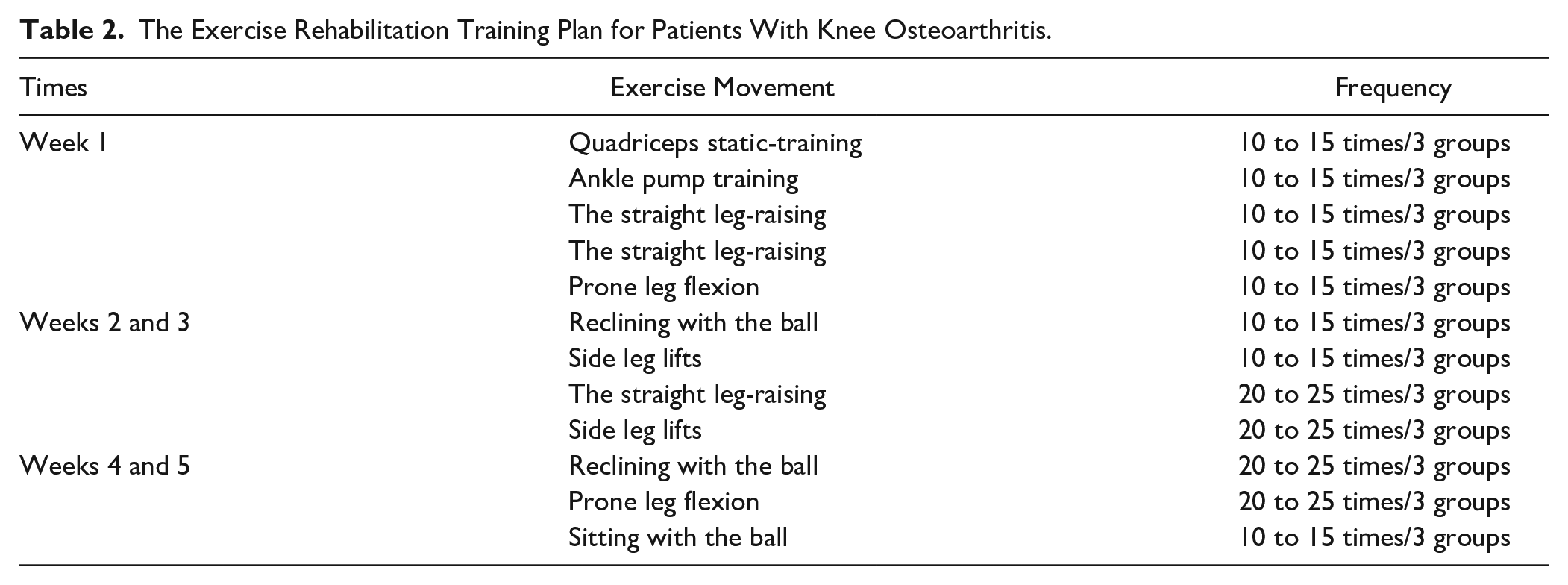
The patients were required to attend follow-up visits at weeks 1, 3, 5, 7, and 12 during the rehabilitation program, where the effect of the rehabilitation was recorded. No NSAIDs or other analgesics were used during the study period in the exercise rehabilitation group.
Assessment of Outcomes
In this study, the outcomes evaluated were improvement in symptoms, knee function, and quality of life of patients with knee osteoarthritis. All patients were assessed using the Lysholm Knee Score, Western Ontario and MacMaster Universities (WOMAC) Osteoarthritis Index Score, and SF-36 (Short Form-36 Survey) health questionnaire before and after treatment. Knee range of motion before and after treatment was evaluated. This study compared the outcome measures among patients who were administered naproxen, diclofenac, and celecoxib.
Statistical Analysis
We used SPSS version 24.0 (IBM Corp, Inc., Chicago, IL) for the statistical analyses. Data were recorded as percentage (n). All the measurement data (age, body mass index [BMI], Lysholm score, WOMAC scores, and SF-36 scores) and knee range of motion were analyzed using paired sample t tests. The data from the 3 groups were analyzed using chi-squared tests. Between-group differences in sex were evaluated. An alpha level of 0.05 was used. Statistical significance was considered as P < 0.05.
Results
A total of 166 patients with knee osteoarthritis were included in this randomized controlled trial. Nineteen patients (11.4%) were lost to follow-up ( Fig. 1 ). The mean age of patients was 56.0 ± 10.5 years, and 77.7% were women. The average follow-up was 12 ± 2.3 weeks. There was no significant difference with respect to age, BMI, and sex between the study and control groups (P > 0.05), as shown in Table 3 .
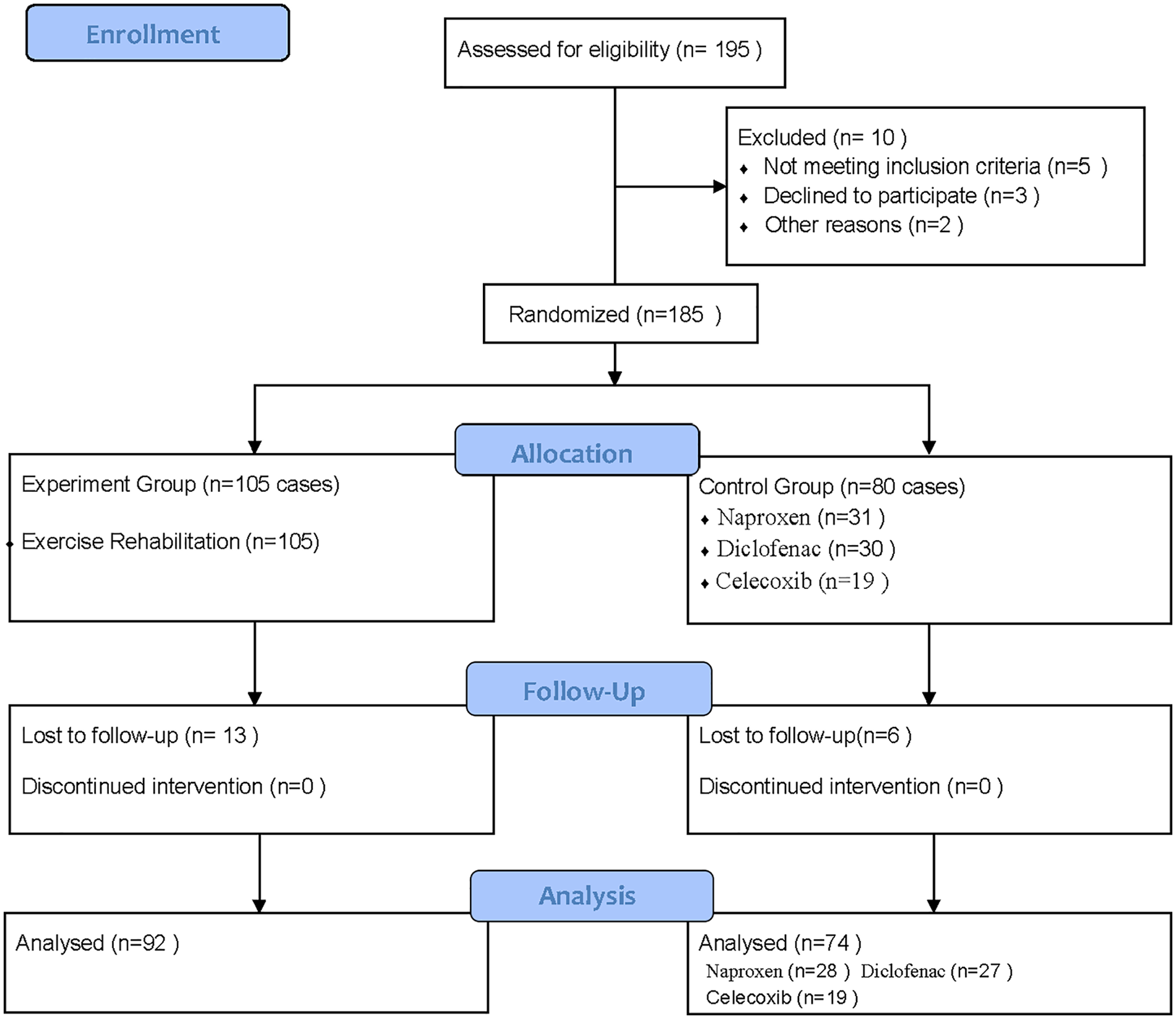
Flow diagram of randomized controlled trial. In this study, we assessed for eligibility 195 cases in enrollment, and finally included 166 cases in analysis; the experiment group included 92 cases, and the control group included 74 cases.
Baseline Characteristics of Patients in This Study.
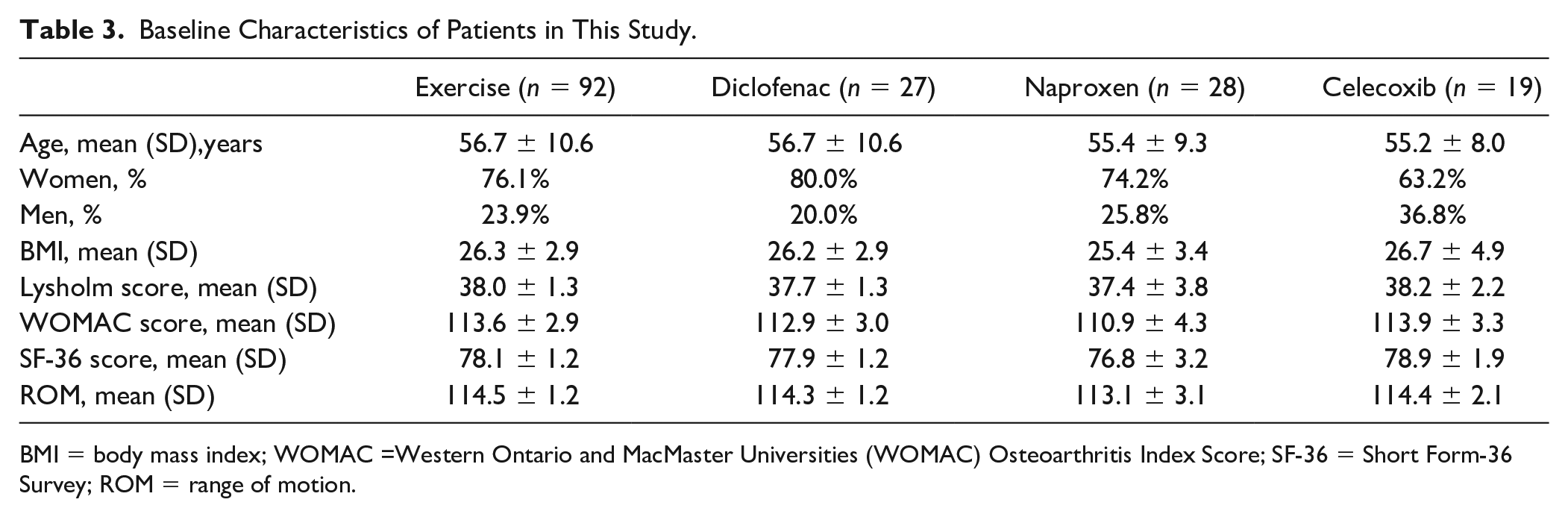
BMI = body mass index; WOMAC =Western Ontario and MacMaster Universities (WOMAC) Osteoarthritis Index Score; SF-36 = Short Form-36 Survey; ROM = range of motion.
The average WOMAC score in the exercise rehabilitation and diclofenac groups were 84.4 ± 15.2 and 108.3 ± 3.9, respectively, after treatment (P = 0.009). The mean Lysholm score in the exercise rehabilitation and diclofenac groups were 60.3 ± 14.9 and 41.0 ± 0.1, respectively, after treatment. These results showed a significant difference in scores between groups, which indicates that exercise rehabilitation can relieve pain and other symptoms more effectively than diclofenac. In the exercise rehabilitation group, the mean SF-36 score was 105.4 ± 21.5, and the average knee range of motion was 125.0 ± 6.2° after treatment. The average SF-36 score in the diclofenac group was 83.7 ± 5.0, and the average knee range of motion was 116.4 ± 1.4° after treatment. There were significant between-group differences (P = 0.043 and 0.017, respectively), showing that exercise rehabilitation achieved a greater improvement in quality of life than that achieved with diclofenac ( Table 4 ).
Comparison of the General Condition of Patients in the Exercise Rehabilitation and Diclofenac Groups.
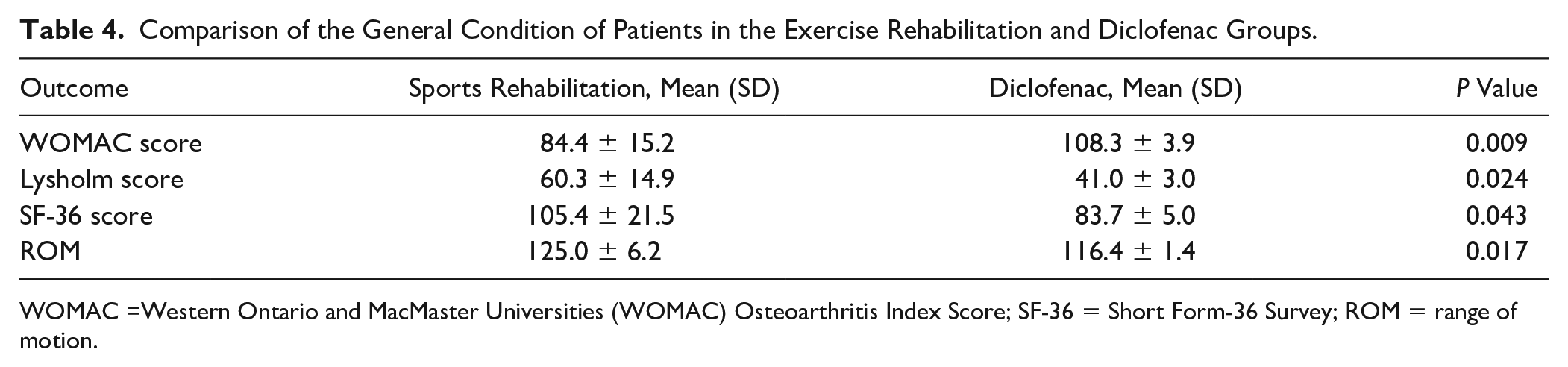
WOMAC =Western Ontario and MacMaster Universities (WOMAC) Osteoarthritis Index Score; SF-36 = Short Form-36 Survey; ROM = range of motion.
In the naproxen group, the average WOMAC score was 107.4 ± 5.4, and the average Lysholm score was 43.5 ± 5.3, after treatment. The results of the exercise rehabilitation and naproxen groups were significantly different (P = 0.006 and 0.020, respectively), which indicated that exercise rehabilitation was better at treating pain and other related symptoms than naproxen. Taking into account the quality of life, it was found that the naproxen group had an average SF-36 score of 82.5 ± 3.7 and an average knee range of motion of 114.7 ± 1.1°, while the exercise rehabilitation group had a score of 105.4 ± 21.5 and range of motion of 125.0 ± 6.2° (P = 0.046 and 0.011, respectively). Thus, exercise rehabilitation had an advantage over naproxen in improving patients’ quality of life and recovery ( Table 5 ).
Comparison of the General Condition of Patients in the Exercise Rehabilitation and Naproxen Groups.
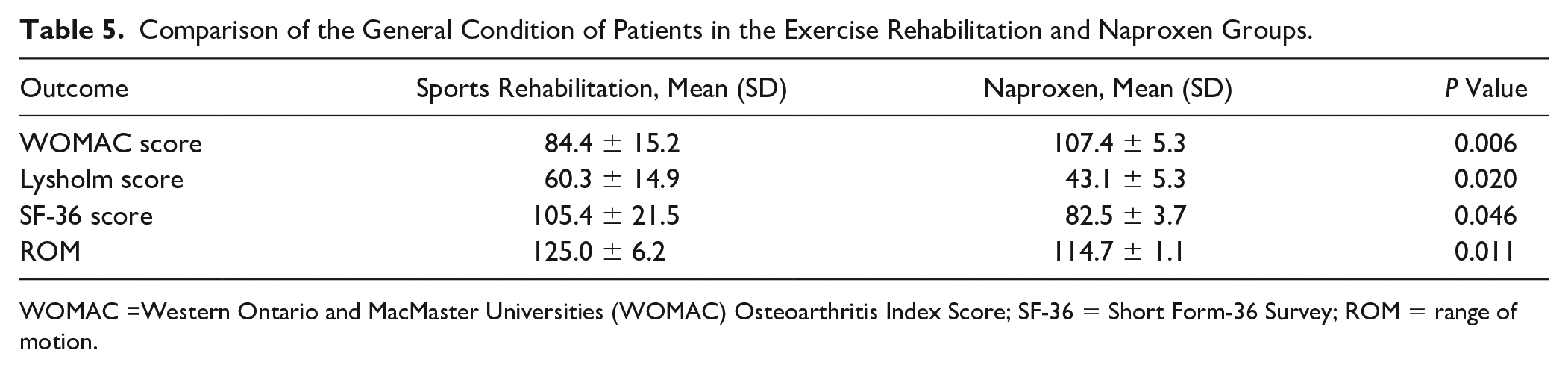
WOMAC =Western Ontario and MacMaster Universities (WOMAC) Osteoarthritis Index Score; SF-36 = Short Form-36 Survey; ROM = range of motion.
As shown in Table 6 , we also compared the outcomes of the exercise rehabilitation group with that of the celecoxib group with respect to differences in short-term prognosis of patients. In the celecoxib group, the average WOMAC score was 107 ± 6.0, the average Lysholm score was 41.8 ± 3.6, the average SF-36 score was 84.2 ± 3.5, and the average knee motion range was 115.6 ± 0.8°. The statistically significant difference between the 2 groups (P < 0.05) validated the ascendency of exercise rehabilitation on prognosis and quality of life improvements. Figure 2 shows that there was no statistically significant improvement in the WOMAC, Lysholm, or SF-36 scores, or knee range of motion in the diclofenac, naproxen, or celecoxib groups after treatment (P > 0.05).
Comparison of the General Condition of Patients in the Exercise Rehabilitation and Celecoxib Groups.
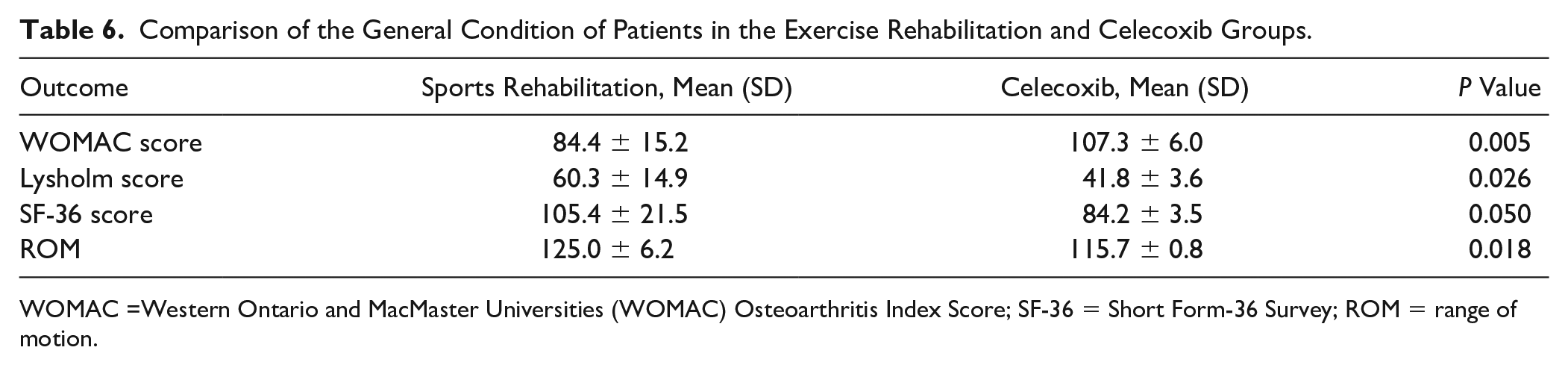
WOMAC =Western Ontario and MacMaster Universities (WOMAC) Osteoarthritis Index Score; SF-36 = Short Form-36 Survey; ROM = range of motion.
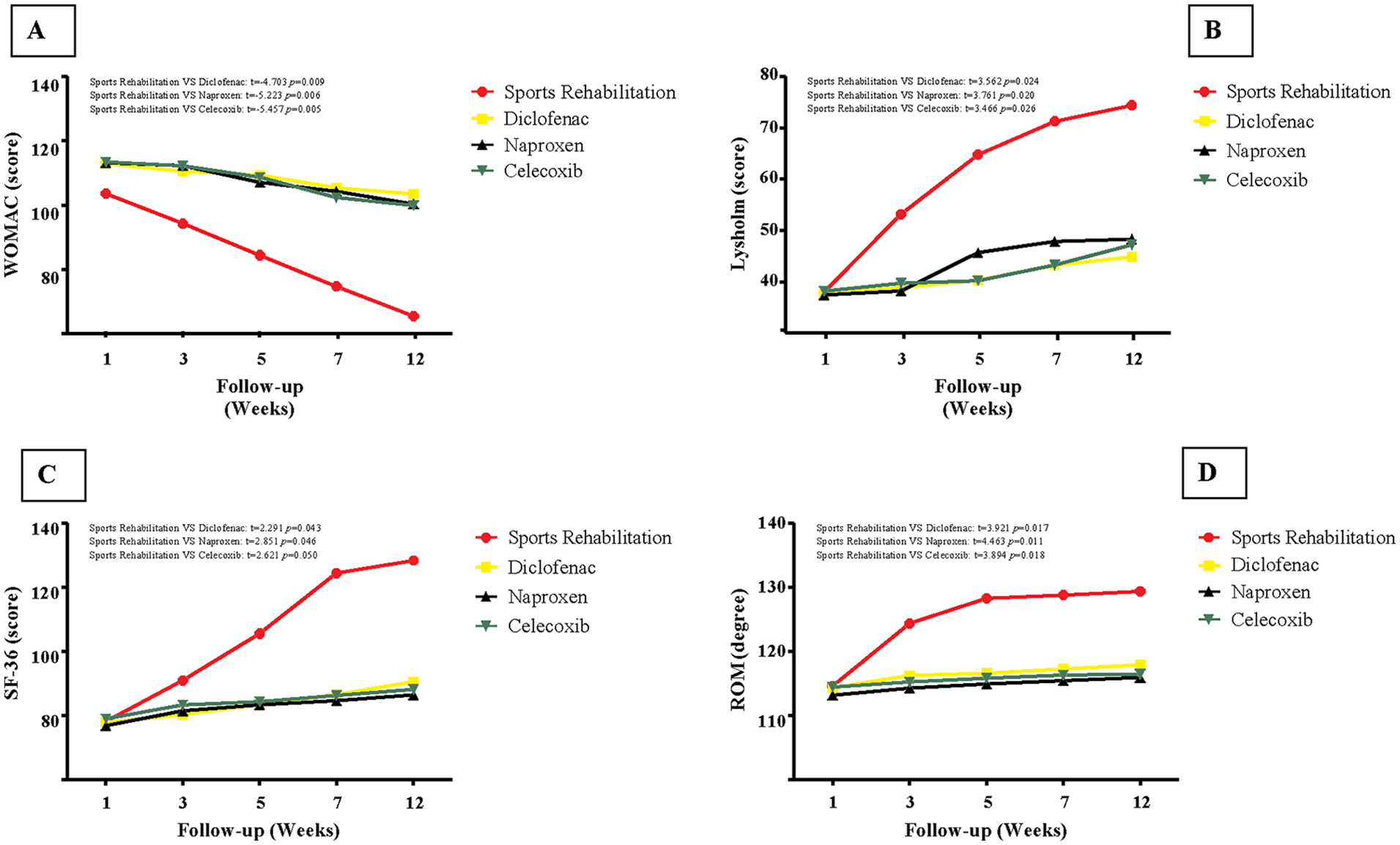
Comparison of outcomes experimental group and control group. (
Discussion
The trial showed that the WOMAC scores, Lysholm scores, SF-36 scores, and average ranges of motion after treatment were significantly better for the exercise rehabilitation group than those for the medication groups.
We still currently lack an effective disease-modifying therapy for osteoarthritis. Many professional societies suggest the use of NSAIDs for primary pharmacologic management of knee osteoarthritis. In England, 5.8 million prescriptions were dispensed for topical NSAIDs in 2014, mainly including formulations of ibuprofen and diclofenac. Some studies suggest the use of conservative treatment with exercise rehabilitation, which is considered to be one of the important and basic methods for the treatment of knee osteoarthritis.6-9 However, some studies have expressed concern as to whether exercise rehabilitation can surpass conventional treatment methods. 10
A total of 166 patients with knee osteoarthritis were included in this randomized controlled trial, and the mean follow-up period of the 2 groups was 12 ± 2.3 weeks. This study shows that exercise rehabilitation provides significant improvements in pain, other symptoms, and quality of life compared to that achieved by conventional treatments.
A British primary care center and Keele University conducted a systematic review and meta-analysis that showed that exercise programs that include muscle strength, flexibility, and aerobic training could improve the prognosis of patients by improving joint function. When compared to the control group, 11 the degree of pain was also significantly reduced. Japanese researchers conducted an 8-week randomized controlled trial, including patients with knee osteoarthritis who received home rehabilitation and those who received NSAIDs. It was found that quadriceps muscle strength training relieved pain as much as NSAIDs. Furthermore, it allowed patients to have a normal life, and even provided patients with a greater ability to perform social activities in contrast to using NSAIDs. 12 This result is consistent with the conclusion of this study.
In this study, we compared the outcomes of exercise rehabilitation with that of treatment with naproxen, diclofenac, and celecoxib, because these treatments form the basis of standard treatment recommended by most clinical practice guidelines for knee osteoarthritis.13,14 Diclofenac is the most commonly prescribed drug by primary care physicians. Naproxen is one of the most highly prescribed drugs worldwide for treatment of knee osteoarthritis 15 and is also the cheapest generic NSAID available to health insurance providers. 16 Celecoxib is a COX-2 inhibitor, which is widely prescribed in this group of patients. 17 A systematic review and network meta-analysis demonstrated that naproxen, diclofenac, and celecoxib provided significantly greater improvement in joint function, stiffness, and pain compared to acetaminophen in patients with knee osteoarthritis. 18
Certain studies have found that some inappropriate exercise patterns can adversely affect the prognosis of patients with knee osteoarthritis. 19 Thorstensson et al. found that high-intensity knee joint resistance exercise had no effect on pain relief or functional recovery of patients and even led to aggravation of pain. 20 Therefore, selecting the appropriate type of exercise and intensity level play an important role in the treatment of patients with knee osteoarthritis.
In this study, we evaluated the use of a systematic exercise rehabilitation program to ensure that the suitable type, intensities, and frequencies of exercise were provided to patients with knee osteoarthritis. Previous trials only focused on the effectiveness of muscle strength training or dynamic balance for patients with knee osteoarthritis.7,20,21 This exercise rehabilitation program includes lower limb muscle strength training, proprioception training, and core muscle stability exercises, focusing on the quadriceps and other peripheral muscles that strengthen the knee. Using movement, the combination of open-chain training and closed-chain training was adopted. Each training session lasted for 20 minutes. During the early stage of training, the horizontal position was used for open-chain training to minimize joint pain caused by excessive knee load, increase muscle strength of patients, and ensure patient compliance. During the middle and later stages of training, sitting and standing positions were used to gradually increase the load on the knee joint. Finally, a certain amount of heel lift and core training were provided to increase the lower limb and core strength of patients.
The limitations of this study include small sample size, short follow-up time, and the lack of blinding. Because of significant differences in treatment methods used between conventional treatment and exercise rehabilitation, a blinded method could not be used. Thus, there may have been a placebo effect, as well as a more subjective evaluation in the observation of any improvements, which may have resulted in evidence bias.
The follow-up period of this trial was 12 weeks, and thus, the data collected can be used to analyze the short-term effects of the exercise rehabilitation program in patients with knee osteoarthritis. This study demonstrated that the progressive muscle rehabilitation program resulted in significant improvement in strength, endurance, and speed of muscle contraction. The improvement seen after 3 months was approximately double that seen after 2 months; however, some studies suggest that this improvement may not be significant after more than 4 months of follow-up.22,23 Future studies should focus on long-term follow-up of patients, larger sample sizes, and increasing the use of functional and serological examinations. Studies should further explore the effect and mechanism of exercise on patients with knee osteoarthritis. In addition, the corresponding training intensity should be tailored for patients with varying degrees of knee osteoarthritis, and more appropriate exercise programs should be developed to improve patient compliance and prognosis.
Footnotes
Acknowledgments and Funding
We thank all participants of this trial. We thank the Lee Yaqian and Liang Wenjie for helping improve the study. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
JC and YPL designed the study; ZJ acquired the data; BXH and GQ designed the systematic exercise rehabilitation program. All authors drafted the manuscript and critically revised and approved the final version of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by The Second Hospital of Hebei Medical University Ethics Committee (2017023919).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Trial Registration
ChiCTR1800019208.