
Abstract
Background
Full-depth cartilage lesions do not heal spontaneously and may progress to osteoarthritis (OA). Treatment for these lesions is warranted when symptomatic. At younger age, biological treatment remains the gold standard, but treatment in the middle-aged patient remains a clinical challenge and focal metal implants have been proposed. We aim to present the subjective outcome at 2 years and the risk of reoperation for any reason at midterm after surgery with a novel customized implant for focal femoral chondral lesions in the knee.
Methods
In a prospective cohort study, 30 patients were included between January 2013 and December 2017 at 9 different clinics in Sweden. The primary outcome was subjective outcome measurements (Visual Analogue Scale [VAS], EuroQoL [EQ5D], Knee injury and Osteoarthritis Outcome Score [KOOS]) at a minimum of 2 years. The secondary outcome was reoperations for any reason during the follow-up period until December 2019 (mean of 55 months) studied retrospectively by analyzing medical records.
Results
The VAS, EQ5D, and all the KOOS subscales showed significant improvements from preoperatively to the 2-year follow-up. The VAS showed the greatest improvement at the early (3 months) postoperative stage (P < 0.001). Five (7%) patients underwent reoperations and one of these was revised to hemiarthroplasty due to OA progression. No implant loosening was detected in any of the cases.
Conclusions
This customized resurfacing metal implant showed good safety and patient satisfaction. The risk of OA progression and implant loosening is low. Subjective function and pain improved significantly.
Keywords
Introduction
The main function of articular cartilage is to provide a bearing surface that permits almost frictionless movement.1,2 Patients with focal cartilage defects often have functional impairments and pain that significantly affects their quality of life and socioeconomic situation.3-5 Cartilage lesions constitute a pathology on the rise, due to the increased activity level in an aging population, as well as their association with sports injuries. 6
Epidemiological studies show that chondral lesions, of any type, are present in about 60% of all knee arthroscopies.3,7-9 Focal knee cartilage lesions, International Cartilage Research Society (ICRS) grades 1-2, are superficial and often do not require surgical treatment. 8 Deep knee cartilage lesions, ICRS grades 3-4, are thought to precede osteoarthritis (OA) and are therefore potential candidates for surgery. In patients over 40 years of age, full-depth single lesions with an area of 1 cm2 or more are encountered in about 9% to 13% of all arthroscopies performed for any reason.3,7-9
For the last 30 years, biological treatment strategies have aimed to regenerate durable knee cartilage repair tissue.10-12 Unfortunately, the healing power of articular cartilage is remarkably limited due to its avascular nature. 13 Nonetheless, there is scientific evidence that transplanted chondrocytes, growth factors, and artificial matrices are able to stimulate the neoformation of cartilaginous tissue. 12 However, biological treatment is less effective with increasing age, and the repair tissues degenerate with time. 14 Unicompartmental or total knee arthroplasties could be considered, but they are known to impose a high risk of early failure in the middle-aged patient. 15
Managing focal cartilage injuries in these patients therefore poses a challenge. 12 For this reason, there is a treatment gap for the middle-aged patient with symptomatic full-depth focal knee cartilage lesions.16,17
In the last decade, a novel treatment strategy has been proposed. It involves surgically replacing the void of the cartilage defect with a focal metal implant. This treatment modality has shown promising results in terms of improved pain and function.18-20 Nevertheless, a worrying revision rate of 28% has been reported, caused primarily by OA progression.21,22 Patient selection and accurate implant positioning are crucial for a satisfactory clinical outcome in the midterm and long term.23,24
A second-generation metal implant featuring patient-specific articulating surface and guide instruments based on magnetic resonance imaging (MRI) images, including a careful MRI assessment of the entire knee, has been developed and has shown promising initial results.25-27
The primary objective of this prospective consecutive cohort study was to assess the subjective outcome in the short term and the risk of new surgical interventions in the midterm for the first 30 patients. We hypothesize that this novel focal resurfacing implant is an option for the treatment of symptomatic knee cartilage lesions in the middle-aged patient, with a good subjective outcome and a low risk of early revision surgery.
Materials and Methods
Patients
This is a retrospective analysis of a prospectively collected cohort. The study was approved by the local ethics committee (2019-03204). Patients from 9 different clinics in Sweden were identified and informed consent was obtained. Thirty patients who underwent surgery with the Episealer implant (Episurf Medical, Stockholm, Sweden) between 2012 and 2018 and with a minimum of 2 years of follow-up were included. The inclusion criteria for surgery were patients aged 30 to 65 years with symptomatic focal chondral defects in the trochlea, or on the medial or lateral femoral condyles ≤2 cm diameter. The patients had had activity pain on the Visual Analogue Scale (VAS; 0-100 mm) >40 mm for more than 6 months. The patients had previously experienced the failure of conservative treatment or surgical interventions such as abrasions, drilling, or microfracture. In some cases, partly regenerated cartilage lesions ICRS grade 2 occurred after previous surgery, but the patients were still symptomatic. The exclusion criteria considered for this implant were unaddressed instability or other concomitant knee injuries such as meniscal injuries, apart from small flap lesions with an intact rim and intact meniscal anterior and posterior horn insertions. Patients undergoing surgery for anterior cruciate ligament injuries with no remaining subjective instability or objective laxity were regarded as eligible. Further exclusion criteria to consider are established OA (Kellgren-Lawrence >1), malalignment, metabolic disorders which may impair osseointegration, smoking, metal allergies, inflammatory joint diseases, and the systemic administration of corticosteroids, anti-neoplastic drugs, and immune-stimulating or immunosuppressive agents. 27
Implant
The implant is a monobloc focal Cr-Co femoral condyle or trochlear prosthesis where the articulating surfaces are patient specific and manufactured by computer-aided design/computer-aided manufacture (CAD/CAM) from MRI images. The fixation surfaces facing cartilage and bone are double coated with hydroxyapatite (HA) on top of titanium, resulting in osseo- and chondrointegration. 28 The implants are configured as either a circle (Solo) or a figure of eight (Twin) as needed, depending on the size of the lesion. Correct positioning is aided by patient-specific guide instruments. The specific design of the implant, preoperative planning, surgical technique, and postoperative rehabilitation regimen have been previously described. 27
Outcomes
Primary outcome assessments were prospectively collected patient-reported outcome measurements (PROMs): the Knee injury and Osteoarthritis Outcome Score (KOOS), 29 the EuroQoL (EQ5D), and the Visual Analog Scale (VAS pain) preoperatively, at 3 and 6 months, and 1 and 2 years. The secondary outcome was complications such as implant loosening, deep venous thrombosis, or infection and the need for revision surgery during the follow-up period until December 2019, studied retrospectively by analyzing medical records.
Statistical Analysis
All the data were analyzed using IBM SPSS Statistics for Mac, version 23 (IBM Corp, Armonk, NY). Data for patient demographics and PROMs are expressed as the mean, standard deviation, and range. Differences in outcome from preoperatively up to 2 years were analyzed using a paired sample t test, 2-tailed. A P value of less than 0.05 was considered to be statistically significant.
Results
Demographics, Subsequent Surgery
Thirty patients from 9 clinics that underwent surgery from 2012 to 2018 were included. The mean follow-up period was 55 months (SD 20; range 24-86). For 15 (50%) patients, there was a well-described acute knee trauma related to the start of symptoms, while for 7 (23%) patients there was no clear trauma of this kind. For 8 (27%) patients, no reliable data regarding the start of symptoms were registered in the patient charts. All the patients had previously experienced failed conservative treatment for at least 6 months and 23 (77%) patients had previously experienced failed cartilage surgery such as a microfracture and/or debridement prior to the index surgery with an Episealer implant. Demographic, injury, and surgical data are listed in Table 1 . Body mass index (BMI) was not available for 1 patient, the ICRS grade was missing in 4 patients.
Demographic, Injury, and Surgical Data a .
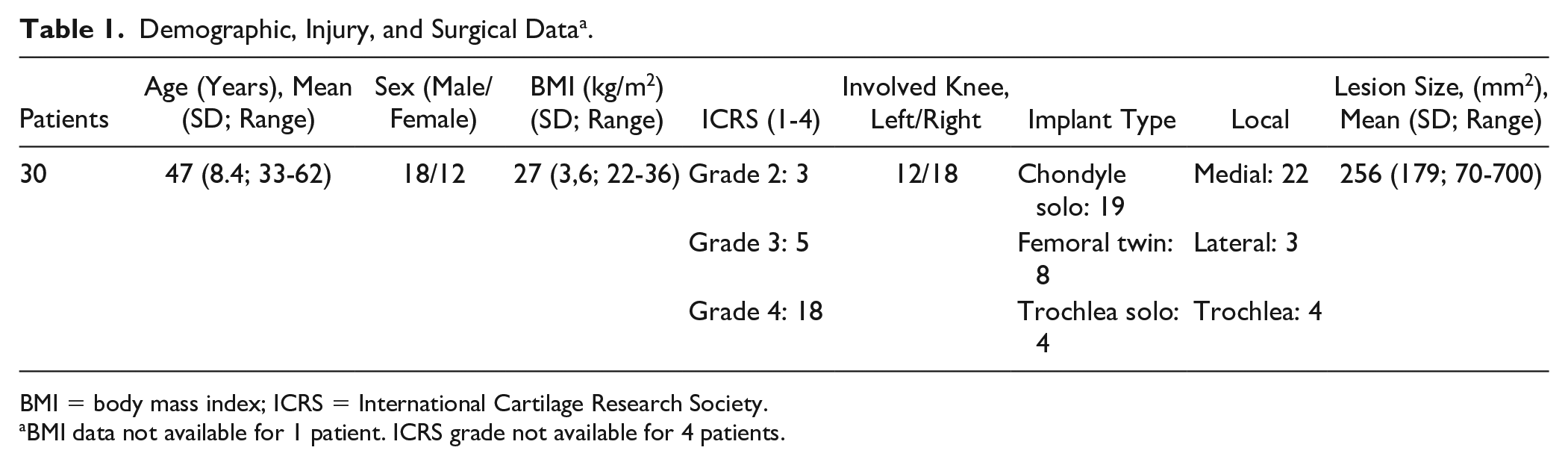
BMI = body mass index; ICRS = International Cartilage Research Society.
BMI data not available for 1 patient. ICRS grade not available for 4 patients.
In the medical records, no infections or deep venous thromboses were diagnosed. Five (17%) patients had a new operation during the follow-up. For 22 (73%) patients, PROMs were available at preoperative and 24 months. Of the 22 patients with available PROMs, 2 (7%) patients had a new operation on the same knee during the follow-up period. In one patient, a diagnostic second-look arthroscopy was performed 10 months after the index surgery due to persistent anterior knee pain. The focal knee prosthesis was placed on the medial femoral condyle. The arthroscopy showed slight patellofemoral OA, ICRS 1-2, and slight synovitis locally in the medial capsule. The implant was well fixed with cartilage growth over the edges. The second patient underwent an arthroscopy 8 months after index surgery due to pain and swelling. The index surgery was a trochlear implant that was found to be well incorporated and positioned. The arthroscopy showed slight synovitis in the lateral compartment of the knee.
Of the 8 patients without available PROM data, another 3 (10%) patients had subsequent surgery during follow-up. One had a revision to an Oxford unicompartmental knee prosthesis about 10 months after index surgery. The tibial joint surface was worn down to the bone. Slight cartilage degeneration of the tibial joint surface was also noted at index surgery. The implant was firmly attached to bone and it was removed by chiseling around the periphery, gripping it with a pair of tongs, twisting it loose, and pulling it out. The insertion of the Oxford unicompartmental knee prosthesis went well and no further complications have been noted. Another patient had an arthroscopy 8 months after index surgery with an implant on the medial femoral condyle. The implant was well positioned with cartilage growth over the edges and a clear thinning of the opposing cartilage on the medial tibial condyle was found. No further surgery has been performed in this patient, followed-up for 54 months. The third patient had a complex patellofemoral instability and pain syndrome at index surgery with a trochlear implant. At the time of index surgery, a concomitant patella-stabilizing Krogius-Lecene procedure was performed, and 8 months after surgery, a suture anchor was removed, followed 6 months later by the lateral release of the patella.
In all, of 30 patients, 5 (17%, median 8 months after index surgery) underwent subsequent surgery. In 2 cases of 30 (7%), progression of OA on the opposing tibial cartilage was found, and in 1 case, the extraction of the implant and conversion to a unicompartmental knee prosthesis were performed. No implant loosening was detected in any of the cases.
Patient-Related Outcome Measurements
At 2 years, all the follow-up scores, the EQ5D VAS, VAS, and all the KOOS subscales, showed significant improvements compared to presurgery ( Table 2 and Fig. 2 ). The improvement on all the subscales exceeds the minimal important change as defined by Ingelsrud et al. 30 The VAS showed the greatest improvement at an early stage, with a significant decrease between preoperative and 3 months (P < 0.001), after which it was steady ( Fig. 1 ). Some residual pain and impairment of function were however still noted at the 2-year follow-up.
Patient-Related Outcome Scores, Preoperative, and at 2 Years a .
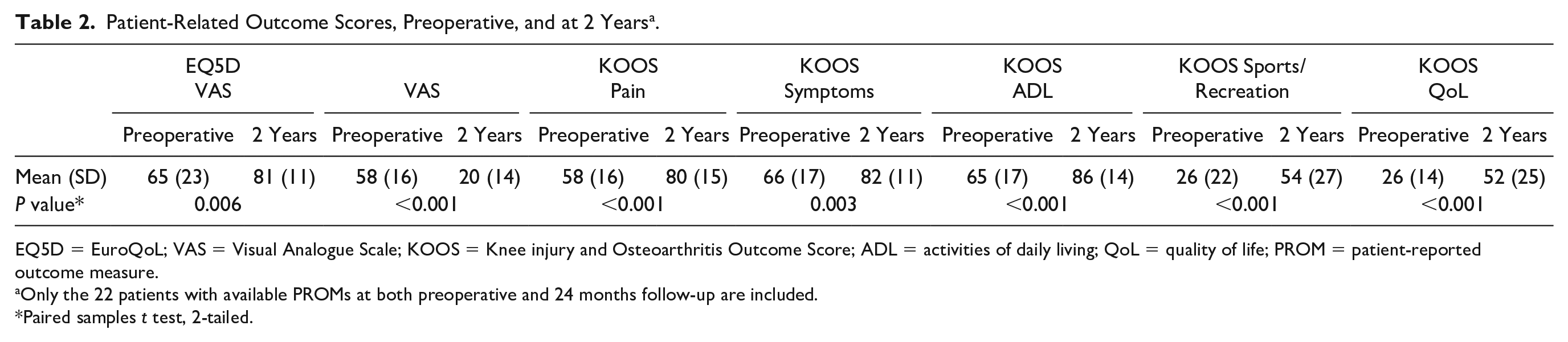
EQ5D = EuroQoL; VAS = Visual Analogue Scale; KOOS = Knee injury and Osteoarthritis Outcome Score; ADL = activities of daily living; QoL = quality of life; PROM = patient-reported outcome measure.
Only the 22 patients with available PROMs at both preoperative and 24 months follow-up are included.
Paired samples t test, 2-tailed.
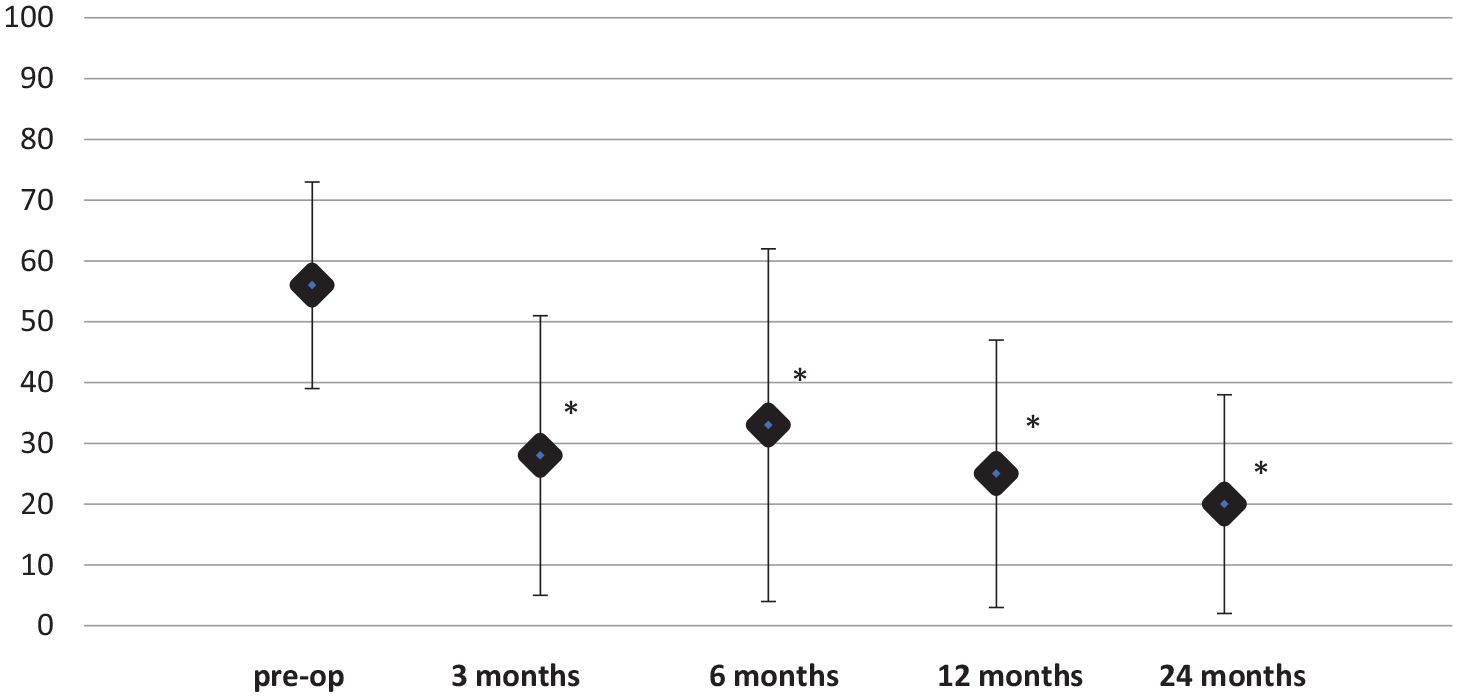
Visual Analogue Scale (VAS). VAS at preoperative, 3, 6, 12, and 24 months. VAS improved at 3 months and maintained significantly improved in comparison with preoperative over 24 months (3 months P = <0.001, 6 months P = 0.006, 12 months P = <0.001, 24 months P = <0.001).
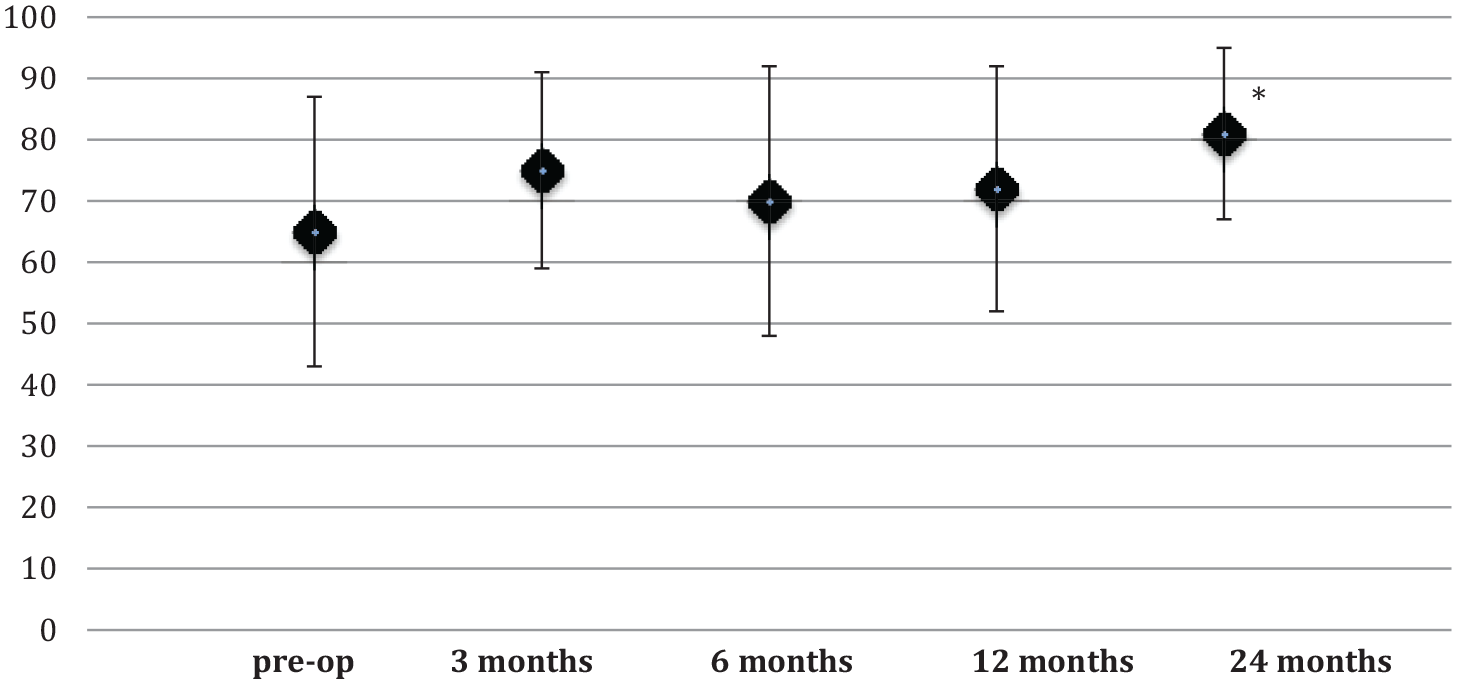
EuroQoL (EQ5D) Visual Analogue Scale (VAS) at preoperative, 3, 6, 12, and 24 months. The improvement was significant only from preoperative to 24 months (65-81, P = 0.006).
Discussion
The most important finding in this study is that treatment of symptomatic femoral knee cartilage lesions with this customized metal implant shows improvement in patient outcome measures and low risk of revision surgery.
Single focal knee cartilage and osteochondral defects are very common and can also cause great functional impairment to the same extent as in patients with OA. 4 Osteochondral defects are also considered to be a factor predisposing to the development of knee OA perhaps due to impairment of the incongruity of the joint surfaces that induces stress in adjacent regions.31,32 The healing capacity of articular cartilage injuries is poor and biological treatment less effective with increasing age. 14 Unicompartmental or total knee arthroplasties could be considered but implant survivorship is limited in the active young and middle-aged patient, which explains why this patient group poses a great challenge.31,32 A treatment gap exists for the middle-aged patient with symptomatic focal knee cartilage lesions. There is a need for a solution for this patient group that could effectively relieve pain and improve function but still be less surgically aggressive than a conventional arthroplasty. The concept should also be able to permit subsequent revision to an arthroplasty if needed. Focal knee resurfacing techniques have evolved and have been proposed to be the bridge between biological treatment and arthroplasty in the middle-aged patient. 33
However, previous studies of focal knee resurfacing implants have reported a high risk of progression to OA and risk of revision to knee arthroplasty.21,22 In the Australian knee prosthesis registry a revision rate of 24% can be seen at a 5-year follow-up for partial knee resurfacing methods with 57% revised to total knee replacement and 22% to unicompartmental knee replacement. 21 In studies by Laursen et al., a 23% to 47% conversion to total knee replacement was seen at a 7-year follow due to the progression of cartilage lesions, OA, or increased knee pain using different types of focal knee implants.22,33 The risk of subsequent surgery during the follow-up period was in this study lower than previously described for other focal knee resurfacing systems. Five patients (17%) had new surgery for any reason during the follow-up but in only one of those cases a revision to a unicompartmental knee was made. It has been questioned whether the opposing tibial plateau cartilage is able to endure the possible stress from the focal femoral implant. Experimental animal studies have shown the importance of correctly positioning the implant to reduce the risk of increased contact pressure. 24 The lack of patient-adapted implants and instruments in previous reports could have had a detrimental effect on the opposing cartilage. It is mandatory for long-lasting function to avoid any increase in contact pressure on the opposing cartilage. The rate of revision to knee prosthesis in this study (1 case) is significantly less, and it is reasonable to attribute this to the patient specificity of implants and instruments, but it could also be an effect of better patient selection.
In several cases, arthroscopy was performed during the first year. Except for one case with opposing cartilage wear, the common findings were problems in other parts of the joint, often the patellofemoral joint. Notably, all these secondary procedures were performed during the first postoperative year, and once this has passed, longevity may be good. This long lack of secondary interventions after the first year is of particular interest since it is known that a focal cartilage injury predisposes to the development of generalized OA.34,35
Previous reports on this customized focal knee resurfacing system are limited to a study with a small number of participants, 10 patients. 27 That study revealed good implant safety and improved subjective outcome but was underpowered to find any significant improvement for the EQ5D VAS and the KOOS subscales of pain and symptoms. With this larger study, improvements in the EQ5D VAS and all the subscales of the KOOS were noted at the same 2-year follow-up. The decisive impact on experienced VAS pain early in the postoperative course despite the surgical trauma is noteworthy. It is known that a focal cartilage injury, due to either trauma or avascular necrosis, can be very painful. 4 It is obvious that the procedure is pain relieving. This can probably be attributed to the loss of high pressure on the subchondral bone following the surgery. It should, however, be noted that some residual pain was still present at the 2-year follow-up and a patient with a focal cartilage injury treated with a focal knee implant can expect some remaining morbidity, which is important to know when advising the patients before considering surgery.
One limitation of this study is that, although the follow-up period is a mean of 55 months and up to 86 months, PROMs are only available for 24 months. We state that damage to the opposing cartilage was only seen in 2 patients but no X-ray evaluation was done and a second-look arthroscopy was done in only 5 patients. No control group was available and it should be noted that the patients were still experiencing some pain and an impairment of function at the latest, 2-year, follow-up. Another limitation is the 27% loss of follow-up in PROMs, especially for the group requiring revision surgery.
From this study, it is not possible to say whether this metal implant will reduce the risk of the long-term development of OA. At this point, this would be pure speculation and further studies are mandatory, but considering the improvements in PROMs and the low risk of conversion to arthroplasty surgery focal femoral resurfacing with this implant could be an option for the challenging middle-aged patient with symptomatic cartilage injuries with failed biological treatment or a lack of suitability for this treatment. More studies with a long-term follow-up are needed, but in the event of failure, the method does not seem to compromise potential future arthroplasty surgery.
Conclusion
This customized focal knee resurfacing implant showed good implant safety and an improvement in patient outcome measurements. The risk of revision surgery was low.
Footnotes
Authors’ Note
All the authors have read and participated in the data analysis and writing of this article.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AS has received research funding from Episurf AB.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the local ethics committee Karolinska Institutet (2019-03204).
Informed Consent
Verbal informed consent was obtained from all subjects before the study.