
Abstract
Purpose. The aims of this study were to (1) examine the timeline of return to sport (RTS) following isolated lateral opening wedge distal femoral osteotomy (DFO), (2) evaluate the degree of participation on RTS, and (3) identify risk factors for failure to RTS. Methods. Nineteen consecutive patients undergoing isolated lateral opening wedge DFO were reviewed retrospectively at a minimum of 2 years postoperatively. Patients completed a sports questionnaire, visual analogue scale for pain (VAS-Pain), Single Assessment Numerical Evaluation (SANE), and a satisfaction questionnaire. Results. Seventeen patents (89.5%; age 32.1 ± 10.1 years; gender 9 males, 52.9%) were contacted at 7.3 ± 4.4 years (range 2.0-13.8 years). Twelve patients (70.6%) resumed playing ≥1 sport at an average time of 9.5 ± 3.3 months (range 3-12 months). Of these 12 patients, 6 returned to a lower level of participation (50.0%). Seven patients (41.2%) had returned to the operating room for further surgery, which included removal of hardware (5.9%) and total knee arthroplasty (5.9%). The average VAS-Pain, SANE, and Marx scores were 3.4 ± 2.6 (range 0-8), 56.2 ± 18.7 (range 20-85), and 5.0 ± 5.3 (range 0-16), respectively. Fourteen patients (82.4%) were at least somewhat satisfied with their procedure. Conclusion. In patients with isolated lateral compartment osteoarthritis and valgus deformity, lateral opening wedge DFO allows 70.6% of patients to RTS by 9.5 ± 3.3 months. However, most patients may be unable to return to their presymptomatic level of function. Patient expectations regarding RTS can be appropriately managed with adequate preoperative patient education. Level of Evidence. IV, case series.
Introduction
Knee osteoarthritis is a leading cause of global disability and its incidence is continually growing among young, active patients.1,2 Due to multifold increased risk of revision and heightened expectations in young patients, total knee arthroplasty may not be the optimal treatment modality in this population. 3 Patients in this cohort may expect to participate in recreational activities at a high level which may increase the risk of failure of total knee arthroplasty. Therefore, in patients with isolated lateral compartment osteoarthritis with valgus deformity, distal femoral osteotomy (DFO) represents an alternative treatment option that preserves the native joint space while offloading the lateral compartment.4,5 By reducing the contact pressure on the lateral tibiofemoral joint, DFO aims to reduce pain, improve function, and delay knee deterioration—which may reduce the need for eventual knee arthroplasty.6,7
Following isolated DFO, patients demonstrate a significant improvement in patient-reported outcome measures (PROMs), high rate of satisfaction, and low rate of conversion to total knee arthroplasty. 8 However, in young, active patients, return to sport (RTS) and the degree of participation may represent an important outcome metric. It has previously been shown that 77% to 100% of patients are able to RTS within a year following isolated DFO.9,10 Despite a high rate of RTS, these investigations are limited by small sample sizes as well as heterogeneous indications and patient populations that included derotational osteotomies, opening and closing wedge DFO, medial and lateral approaches, and cases with concomitant high tibial osteotomy.
As preoperative patient expectations are a significant predictor of postoperative outcomes,11,12 it is imperative to appropriately educate patients in order to establish manageable goals prior to operative intervention. The purpose of this investigation is to (1) examine the timeline of RTS following isolated opening wedge DFO, (2) evaluate the degree of participation and function on RTS, and (3) identify risk factors for failure to RTS.
Methods
Prior to the start of this investigation, approval was obtained from the local institutional review board. A retrospective review was performed on a prospectively collected patient database. The registry was queried for patients who underwent lateral opening wedge DFO from 2004 to 2015 by the senior author. Indications for DFO include age less than 65 years and evidence of isolated lateral compartment osteoarthritis (Kellgren-Lawrence ≥1). At the time of surgery, all patients included in the investigation had at least mild osteoarthritis. Inclusion criteria for this study were patients who received an isolated lateral opening wedge DFO with a minimum 2-year follow-up. Patients were excluded if they were 18 years or younger at the time of surgery or underwent bilateral DFO within 3 years of each other. Patients who underwent concomitant osteochondral allograft (OAG), meniscal allograft transplant (MAT), or autologous chondrocyte implantation (ACI) were excluded from this investigation. Patients who underwent prior meniscectomy or anterior cruciate ligament reconstruction on the ipsilateral knee were included in the investigation. Furthermore, patients who underwent previous cartilage/meniscal procedures (microfracture, MAT, OAG, osteoarticular transfer system [OATS], or ACI) on the ipsilateral knee that were not a part of a staged procedure were also included. A single patient (5.9%) underwent previous OATS procedure with an outside physician that was not a part of a planned staged procedure and no patients returned to the operating room for cartilage/meniscal regeneration procedures.
Fifty-four patients underwent lateral opening wedge DFO by the senior author from 2004 to 2015. Of these, 40 patients had a minimum of 2-year follow-up. Twenty-one patients underwent concomitant meniscal allograft transplantation and were excluded from this study. The remaining 19 patients received isolated lateral opening wedge DFO and 17 patients (89.5%) were contacted to complete a sports questionnaire postoperatively. Patients with a functional telephone number or email address were contacted. Those who were not contacted for follow-up had a disconnected phone number or did not respond to attempts to have the questionnaire mailed to their home. This sports questionnaire has been used previously to describe sport-related outcomes following knee osteotomies.13-15 Patient-reported activities were stratified into low-, medium-, and high-intensity lower-extremity demands ( Table 1 ).13-15 Information regarding preoperative sports participation was not collected prior to surgery; however, this information was collected postoperatively at final follow-up as a part of the sports questionnaire. In addition to this questionnaire, patients were asked to complete a Single Assessment Numerical Evaluation (SANE), Marx Activity Scale, and visual analogue scale (VAS) for pain. Preoperative diagnosis, demographic information, intraoperative variables, complications, and surgical history were collected from patient records. Additionally, preoperative radiographs were assessed for the degree of osteoarthritis by the Kellgren-Lawrence grading system. Operative reports were reviewed for the degree of correction of valgus malalignment.
Sports Stratified by Demand Level.
Surgical Technique
Preoperatively, the degree of correction was determined by calculating the angle between a line extending from the center of the femoral head to the center of the medial tibial spines, and a line from the center of the talus through the center of the tibia. 16 The goal was to record a degree of correction that achieved a neutral mechanical axis. A 4- to 6-cm lateral incision is made along the midline of the lateral femur. The iliotibial band is incised, and the vastus lateralis is elevated from the intermuscular septum. With the knee flexed to 10° of flexion, guide pins are inserted into the lateral femoral cortex and advanced until it contacts the medial cortex. Osteotomy guides (Arthrex, Naples, FL) are inserted over the guide pins and adjusted to achieve the appropriate degree of correction. With the use of a reciprocating saw and osteotomes, the lateral, anterior, and posterior cortices of the distal femur are cut, leaving the medial cortex intact. A DFO wedge plate (Arthrex Opening Wedge Femoral Osteotomy Plate; Arthrex, Naples, FL) is inserted and secured with 4.5-mm threaded cortical screws proximally, and 6.5 mm cancellous screws distally. Cancellous bone chips or harvested bone autograft (distal femur, proximal tibia, or iliac crest) was then packed into the osteotomy site.
Rehabilitation Protocol
Patients were limited to heel-touch only and allowed to progress to full weightbearing 6 weeks following operative intervention. Patients were advised to use a knee brace at all times for the first 2 weeks following surgery. After which, the brace was removed at night until 6 weeks postoperatively. After which, the brace was permanently discontinued. Patients were allowed range of motion as tolerated, but an emphasis was made on maintaining full extension during the first 2 weeks by sleeping in a locked knee brace at full extension.
Statistical Analysis
Statistical analysis was conducted using Microsoft Excel (Microsoft, Seattle, WA). Descriptive analysis of continuous variables included means and standard deviations, while frequencies and percentages were used to report discrete variables.
Results
Nineteen patients met inclusion criteria; of whom, 17 patients (89.5%) were contacted at an average follow-up of 7.3 years (SD, 4.4) (range: 2.0-13.8 years). Patient demographics and characteristics are provided in Table 2 . Sixteen patients (94.1%) underwent at least 1 previous operation on the same knee prior to isolated lateral opening wedge DFO. No patient had previously received an osteotomy for alignment correction and 3 patients (17.6%) previously had surgery on their contralateral leg. The most commonly patient-reported reason to pursue isolated lateral opening wedge DFO were to relieve pain (82.4%), stay active (70.6%), improve motion (64.7%), and to relieve arthritis (29.4%).
Patient Variables and Characteristics.
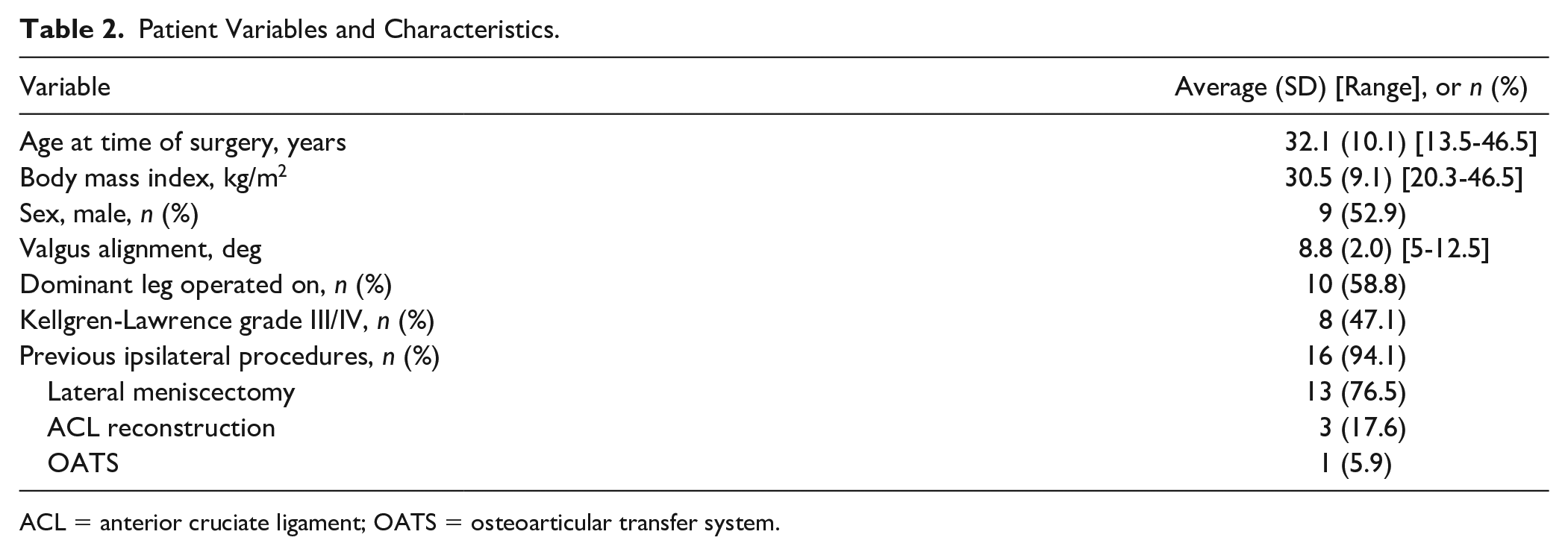
ACL = anterior cruciate ligament; OATS = osteoarticular transfer system.
At the time of final follow-up, 7 patients (41.2%) returned to the operating room for further surgery, which included meniscal debridement/meniscectomy (17.6%), and 1 patient each underwent anterior cruciate ligament reconstruction, removal of hardware, and manipulation under anesthesia (5.9% each). A single patient (age 40.0 years; body mass index [BMI] 30.7 kg/m2) underwent total knee arthroplasty at 6.8 years following the primary DFO.
Outcome Scores
Preoperative outcome scores were available for less than 30% of the patient cohort; thus, these values were not reported. At the time of final follow-up, the average VAS-Pain score was 3.4 ± 2.6 (range 0-8), the average SANE score was 56.2 ± 18.7 (range 20-85), and the average Marx Activity Level was 5.0 ± 5.3 (range 0-16). Fifteen patients (88.2%) in this group stated that in retrospect, they would have this operation again and 14 patients (82.4%) were at least somewhat satisfied with their procedure. Fourteen patients (82.4%) reported at least one complaint with their knee, which included: stiffness (70.6%), chronic pain (41.8%), catching and locking symptoms (35.3%), and frequent swelling (23.5%).
Sports-Related Outcomes
All 17 patients (100.0%) included in this study participated in sports within 3 years prior to their surgery. Twelve patients (70.6%) resumed playing ≥1 sport postoperatively at an average time of 9.5 ± 3.3 months (range 3-12 months). Of these 12 patients, 6 had returned to a lower level of sports participation (50.0%). Eleven patients (64.7%) stopped playing ≥1 sport they previously had participated in, after their procedure. Twelve patients reported being at least somewhat satisfied with their ability to play sports after their operation (70.6%). Table 3 contains the sports-related outcomes for all patients at the time of final contact.
Sports-Related Outcomes.
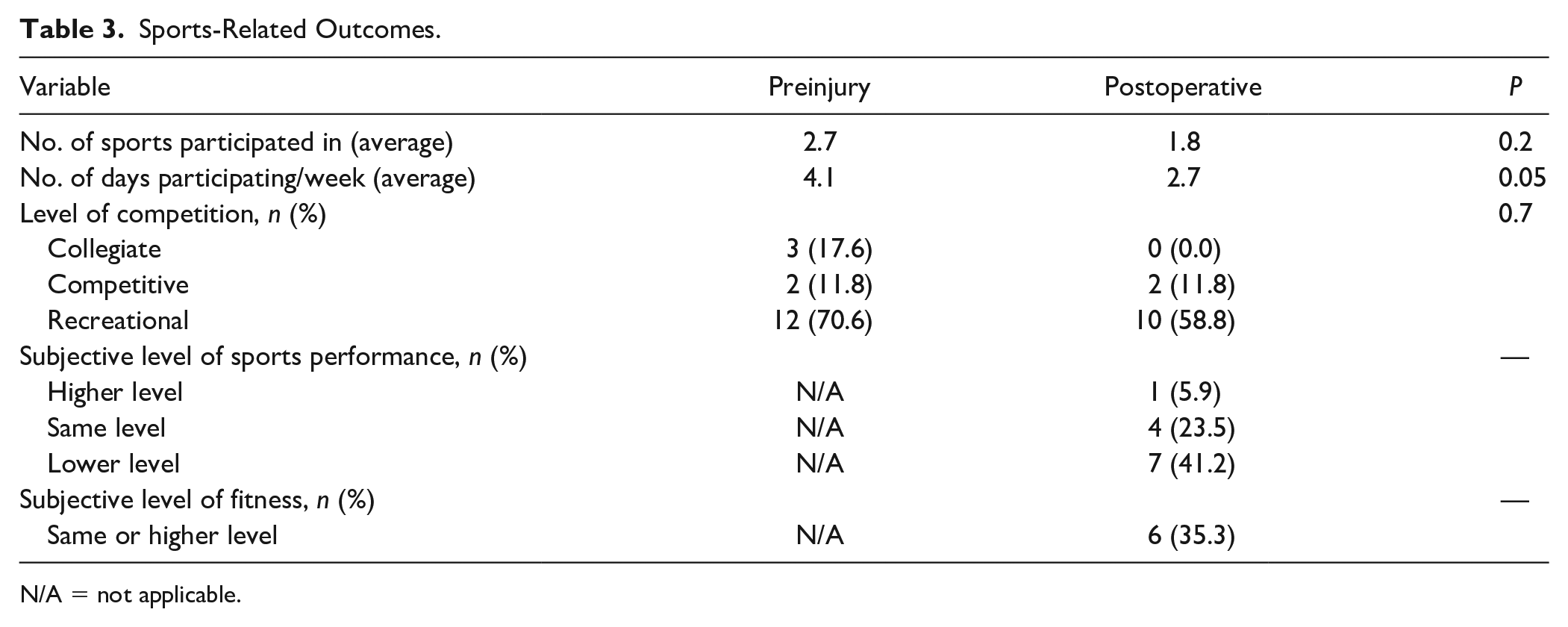
N/A = not applicable.
The direct rate of return to the most commonly reported sports was 100% for baseball (1/1), 57.1% for cycling (4/7), 55.6% for weightlifting (5/9), 40.0% for running (2/5), 33.3% for golf (1/3), and 20.0% for basketball (1/5) (
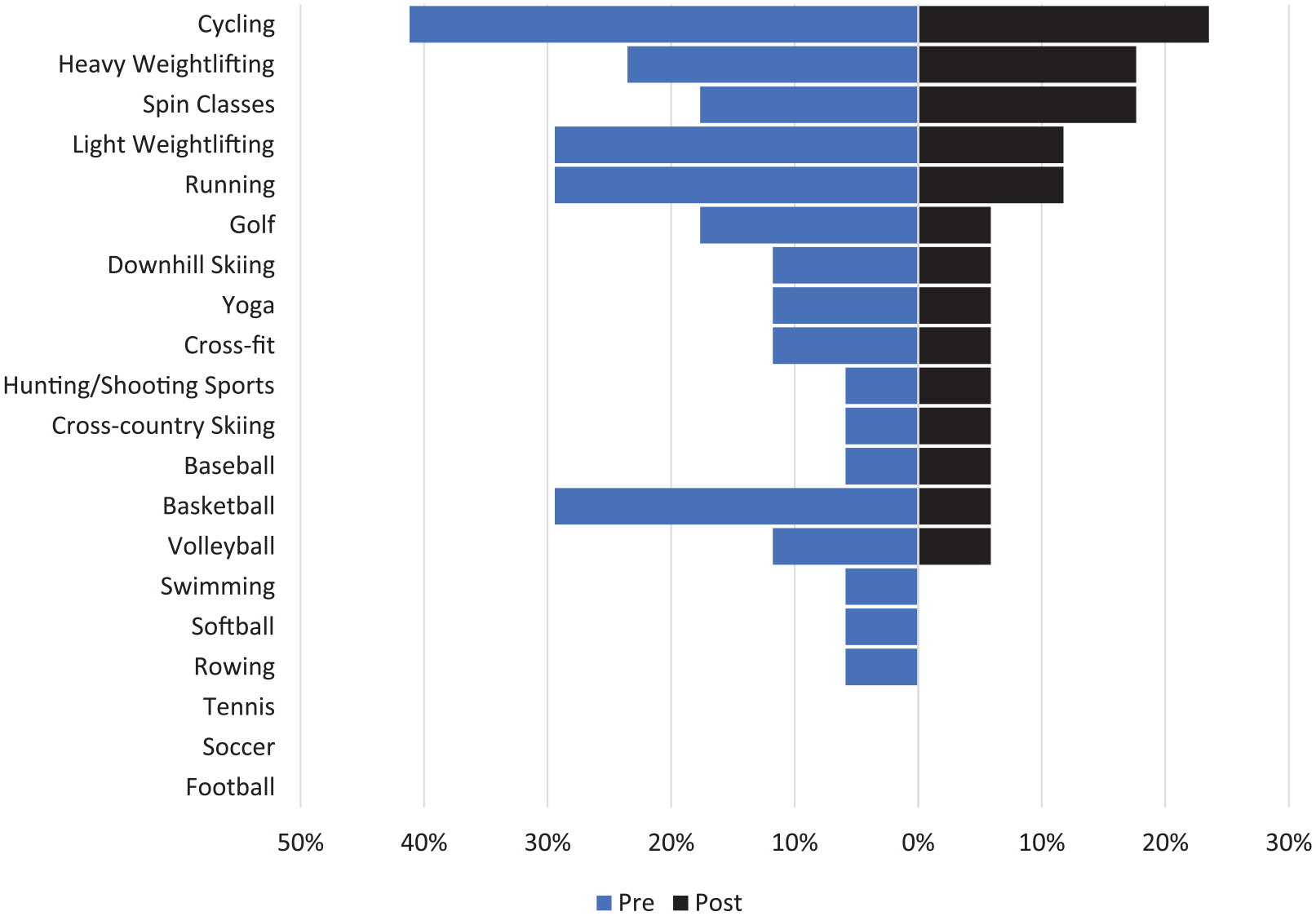
Direct rate of return to sport following isolated distal femoral osteotomy.
Discussion
In this investigation, we demonstrated that 70.6% of patients resumed playing at least 1 sport at an average of 9.5 ± 3.3 months following isolated lateral opening wedge DFO. However, on returning to sport, most patients were unable to return to their previous level of function. This investigation also reports sport-specific rates of return for patients undergoing isolated lateral opening wedge DFO for lateral compartment osteoarthritis with valgus malalignment. Since preoperative patient expectations influence postoperative outcomes, the results of this investigation are critical for appropriately counseling patients in order to manage postoperative expectations.
The rate of RTS in the present investigation is lower than what has been previously reported following DFO (71% vs. 77%-100%).9,10 Voleti et al. 10 investigated 13 patients who underwent opening or closing wedge DFO and demonstrated that 100% of patients returned to sport by 11 months postoperatively. In this cohort, patients were younger (age 24 vs. 32 years), had a lower BMI (27.4 vs. 30.5 kg/m2), lower degree of correction (7.0° vs. 8.8°), and the majority of patients (69%) underwent concomitant procedures on the ipsilateral knee than patients in the present investigation. In a cohort of 126 patients, Hoorntje et al. 9 demonstrated that 77% of patients are able to RTS within 6 months of surgery. Although this cohort of patients were older (age 41.2 vs. 32 years), higher proportion of females (62% vs. 47.1%), and had a lower BMI (27.3 vs. 30.5 kg/m2), the majority of patients (57%) had closing wedge DFO and a significant proportion of patients (35%) had either concomitant high tibial osteotomy or derotational femoral osteotomy. Differences in the rate of RTS is likely attributed to variations in patient populations. Including patients who possess varus or valgus deformity, concomitant osteotomies, meniscal allograft transplantations, or osteochondral allograft transplantations imply varying indications for operative management. These patients may have had a higher baseline function than patients included in the present investigation, which may have allowed them to RTS. However, the authors of the present investigation were unable to compare patients baseline function since preoperative patient function was not reported in this investigation. Furthermore, varying operative techniques, such as opening or closing DFO and V-shaped osteotomy, further contributes to a heterogeneous patient population. Since DFO is an uncommon procedure, it is not unreasonable to pool patients with varying concomitant procedures or techniques. However, comparing the rate and duration of RTS to previous investigations is inherently flawed as heterogeneous patient populations limits the interpretation and clinical applicability of the findings.
In the present investigation, patients who underwent isolated lateral opening wedge DFO due to isolated lateral compartment osteoarthritis with valgus deformity by a single surgeon were included in the analysis. This creates a homogenous patient population that can be used to provide a realistic timeline for RTS following isolated lateral opening wedge DFO. However, it is important to note that there was variability in baseline patient demographics, such as age (range 33 years), BMI (range 26.2 kg/m2), and varus alignment (range 7.5°). This variability may influence the overall rate and duration of RTS following isolated lateral opening wedge DFO. Additionally, only 50% of patients in the present investigation were able to return to their previous level of function on RTS. Similarly, Hoorntje et al. 9 found that patients had a significantly lower Tegner Activity Level following DFO, while de Carvalho et al. 17 demonstrated that 57.7% of patients returned to their preoperative level of sport participation. Therefore, evaluating RTS at the same level of function likely provides a more accurate evaluation of surgical outcomes—especially in young, active patients.
The goals of high tibial osteotomy and DFO are to offload the medial and lateral compartments by shifting the mechanical axis. 18 Therefore, it is important to compare the results of this investigation with the treatment of isolated medial compartment osteoarthritis. In a series of 38 patients (average age 42.7 ± 7.2 years; average follow-up of 9.0 ± 3.3 years), Liu et al. 14 demonstrated that 88.2% of patients returned to sport following high tibial osteotomy for isolated medial compartment osteoarthritis, while only 41.2% of patients returned to their previous level of function. On the other hand, 70.6% of patients returned to sport following isolated DFO while only 50% of patients were able to return to their previous level of sport. High-intensity activities, such as volleyball, basketball, and soccer, had lower rates of RTS than lower intensity activities across both types of osteotomies. Last, a higher proportion of patients underwent conversion to knee arthroplasty following high tibial osteotomy than DFO (38.2% vs. 5.9%). 14 Patients undergoing DFO and high tibial osteotomy had similar baseline BMI, degree of correction, and proportion of previous operations; however, patients undergoing DFO were younger (age 32.1 vs. 42.7 years) and had a lower proportion of preoperative Kellgren-Lawrence grade III/IV osteoarthritis (47.1% vs. 91.2%). Directly comparing patient populations may be limited; however, patients included in the present investigation and those of Liu et al. 14 were operated on by the same senior author. This enables a more direct comparison than other case series would allow. Patients undergoing high tibial osteotomy may have experienced a greater degree of symptom relief which may have allowed a higher proportion of patients to RTS. However, due to increased age and a higher grade of baseline osteoarthritis, more patients may have had to undergo eventual conversion to knee arthroplasty despite similar duration of follow-up (7.3 vs. 9.0 years). Patients may be preoperatively counseled that isolated DFO and high tibial osteotomy may allow patients to RTS; however, these procedures may only be a temporizing measure as patients may require eventual arthroplasty for continued compartment degeneration.
In this investigation, 41.2% of patients returned to the operating room following the index DFO and 82.4% of patients reported at least 1 complaint with their knee in the postoperative period. The most common complaints were stiffness, chronic pain, and catching and locking symptoms. These symptoms were likely due to progression of osteoarthritis, which were treated nonoperatively with activity modification, physical therapy, and pain management. The rate of return to the operating room following DFO ranged from 54.8% to 76.2%, which was mostly secondary to hardware pain.19,20 However, in this investigation, the most common secondary operative procedure was meniscal debridement/meniscectomy. Variation in the cause of the secondary procedure may be due to differences in implants during the initial procedure, degree of baseline osteoarthritis, as well as differing indications for further operative management. Furthermore, only a single patient (5.9%) in the present investigation underwent total knee arthroplasty at 6.8 years following the primary DFO. The survivorship of DFO has been previously reported to be between 78% and 92%.19,20 Differences in the survivorship may be attributed to differing duration of follow-up, variation in baseline osteoarthritis, as well as preoperative patient education. Young, active patients who may have heightened expectations or motivation to participate in higher intensity activities should be appropriately counseled that this may lead to further disease progression and subsequent operative management.
The results of this investigation must be interpreted within the context of its limitations. The retrospective nature of this investigation yields the risk of recall bias which may influence the results of RTS and satisfaction. However, the design of this investigation has previously been implemented for RTS following osteotomies around the knee.13-15 Although this investigation yields a homogenous patient population with a singular indication and operative technique, the same size is limited. Therefore, the generalizability of the results of this investigation may be limited and not applicable to all populations. A multivariate binomial regression was attempted in this investigation to limit the impact of baseline demographics on RTS. However, due to a low sample size, this analysis was not feasible. Additionally, the decision to RTS may be independent of symptom resolution. An additional limitation of this investigation is that postoperative radiographs and clinical assessment was not performed to assess the progression of lateral compartment osteoarthritis. Furthermore, legacy patient-reported outcome measures, such as International Knee Documentation Committee (IKDC), Knee Injury and Osteoarthritis Outcome Score (KOOS), and Lysholm were not assessed as these questionnaires are lengthy. Including these questionnaires in our investigation may have caused respondent fatigue as the RTS questionnaire includes approximately 50 items. Preoperative patient-reported outcome measures or sport participation was not collected. Therefore, the authors were unable to make comparisons of postoperative outcomes. Respondents were queried regarding preoperative sport participation as part of the questionnaire; however, this is subject to recall bias. The clinical significance of our results could not be directly assessed and its impact on patient care can only speculated upon.
Conclusion
In patients with isolated lateral compartment osteoarthritis and valgus deformity, lateral opening wedge DFO allows 70.6% of patients to RTS by 9.5 ± 3.3 months. However, most patients may be unable to return to their presymptomatic level of function. Patient expectations regarding RTS can be appropriately managed with adequate preoperative patient education.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained for this study (19111206-IRB01).
Informed Consent
Informed consent was not sought for the present study.
Trial Registration
Not applicable.