
Abstract
Objective
The objective of this study was to determine the level of disease severity in a pilot cohort of temporomandibular joints (TMJs) and compare them to the pathology findings previously characterized in cadaveric knee joints.
Design
Thirty-one intact TMJs from 17 cadaveric donors were harvested and arthritic lesioning seen in the knee joint was investigated on the condyle and the fossa of the TMJ. Prevalence of gross alterations was equated and disease severity was determined for sex- and age-based donor pools using a validated, osteoarthritis (OA) disease severity scale (DSS). Knee joint DSS scores were also compared to the TMJ condyle and fossa DSS scores and a case study was carried out on a male donor that demonstrated severe OA in the both joints.
Results
The mandibular fossa demonstrated an increase in disease severity compared to the mandibular condyle in a mixed sex donor pool (P = 0.035). It was discovered that the younger females demonstrated statistically more pathological condyles compared to the older half of the female subgroup (P = 0.02). TMJ fossa and knee joints demonstrated comparable OA severity and similar signs of cartilage disease in a single donor highlighting the systemic nature of OA.
Conclusions
This study demonstrates that gross signs of OA in the TMJs of cadavers are comparable to pathology found in the knee. The mandibular fossa appears to be the site of more profound disease, implying translational movements may be more likely to induce biomechanically abnormal movement, loading, and OA.
Introduction
Osteoarthritis (OA) is the most common degenerative joint disease that affects over 300 million people worldwide and more than 32.5 million adults in the United States.1,2 OA is characterized by chronic degeneration of hard and soft tissues associated with synovial joints. OA was long believed to be exclusively related to cartilage “wear and tear,” but the pathogenesis is now better understood to be multifactorial and related to altered inflammatory signaling and remodeling processes.3,4 All or most structures of the synovial joint may be affected by these processes, but the articular cartilage demonstrates some of the most pronounced signs of pathology including linear cracks, fibrillations, erosions, stellate fractures, and gross degeneration to exposure and damage underlying cortical bone.5,6 In principle, any synovial joint can be affected by OA pathogenesis to produce pain, joint stiffness, functional impairments, and reduced quality of life. 7
The temporomandibular joint (TMJ) is a bilateral synovial joint between the condyle of the mandible and the mandibular fossa of the temporal bone. The joint space is composed of an upper and a lower synovial cavity that are separated by a fibrocartilaginous articular disk. The joint is capable of sliding/translational movements in the looser upper joint compartment and rotational/hinge-like movements in the tighter lower compartment.8,9 The TMJ is a vital structure to the health and vitality of all individuals and is of crucial importance in the practice of dentistry. Temporomandibular disorders (TMDs) are fairly common pathologies and are estimated to affect between 5% and 12% of Americans; in 2022, this may represent as many as 40 million people. 10 A systematic review that assessed 2,741 articles on TMDs estimated that as many as 31% of adults or elderly patients have a form of these disorders. 11 Symptoms of TMDs include joint pain, pain in the muscles of mastication, decreased range of mandibular motion, abnormal joint noises, and other various functional deviations. TMDs encompass a variety of acute and chronic diseases and can be classified into 3 subgroups, muscular disorders, disk disorders, and joint disorders. 10 Plain film radiology and computed tomography (CT) are often utilized in the clinic to assess patients for bony alterations of the TMJ; osteophytes are easily visualized. Cone-beam computed tomography systems (CBCT) has been shown to be superior in visualizing the mandibular condyle and cortical erosions, whereas magnetic resonance imaging (MRI) is the gold standard for evaluating soft tissue changes at the TMJ. 9 OA in the TMJ is relatively under studied and the current body of evidence is profoundly reliant on radiology to draw conclusions. Research on pathogenesis of TMJ OA is in its very early stages and a cadaveric approach to study helps advance understanding of cartilage degeneration in a way that is unobtainable through imaging, even CBCT.
The objective of this study was to determine the level of disease severity in a pilot cohort of TMJs. A validated scale for disease severity of OA in the knee joint was utilized to interpret pathology in the TMJs while statistically validating the scale’s usage in the new joint. In the knee joint, it was demonstrated that there were no statistically significant differences in disease severity on the femoral condyles between the sexes but disease severity did demonstrate significant increases with aging (Immonen 2020). Gross alterations to the cartilage of the TMJ were assessed for prevalence and specific location and frequency data was generated; disease severity was correlated to age and sex. This study also aims to help advance the knowledge of TMJ OA in the field of dentistry as dental considerations related OA are researched less regularly compared to OA and its effects on mobility, obesity, and lower extremity joint pain. There are few osteoarthritis investigators that work in cadaveric models and examination of arthritic TMJs is an even rarer pursuit. This pilot body of work represents the development of a new specific aim within an osteoarthritis research program. This work intends to incorporate pathology examined and treated by dentistry and maxillofacial surgery to better interpret holistic osteoarthritis presentation and management.
Methodology
Cadaveric Dissection and Accrual
Thirty-one intact TMJs from 17 cadaveric donors were harvested from skull dissections. Donor sex, age at death, and primary cause of death are provided in Table 1 . Mandibles were disarticulated from the skull by transversely cutting the neck of the mandible and opening the lateral side of the TMJ capsule. The zygomatic arch and calvaria were removed using an autopsy saw. The dura and brain were then removed from the cranial cavity and 2 frontal plane cuts were created to the anterior and posterior aspect of the mandibular fossa of the temporal bone. The posterior cut was placed just anterior to the tragus, and the anterior cut was aligned with the removal of the zygomatic arch. Frontal plane cuts were made to the depth of the foramen spinosum in the middle cranial fossa. Donors were acquired from the University of California Irvine Body Donation Program and the University of California San Diego Body Donation Program. This project (IRBNet ID 1681548-1) was reviewed by University of Nevada Las Vegas’ Institutional Review Board in Las Vegas, NV, and was determined to be research not involving human subjects.
Identifying Number, Sex, Age of Death, and Primary Cause of Death for the 16 Cadaveric Donors Composing the Specimen Pool.
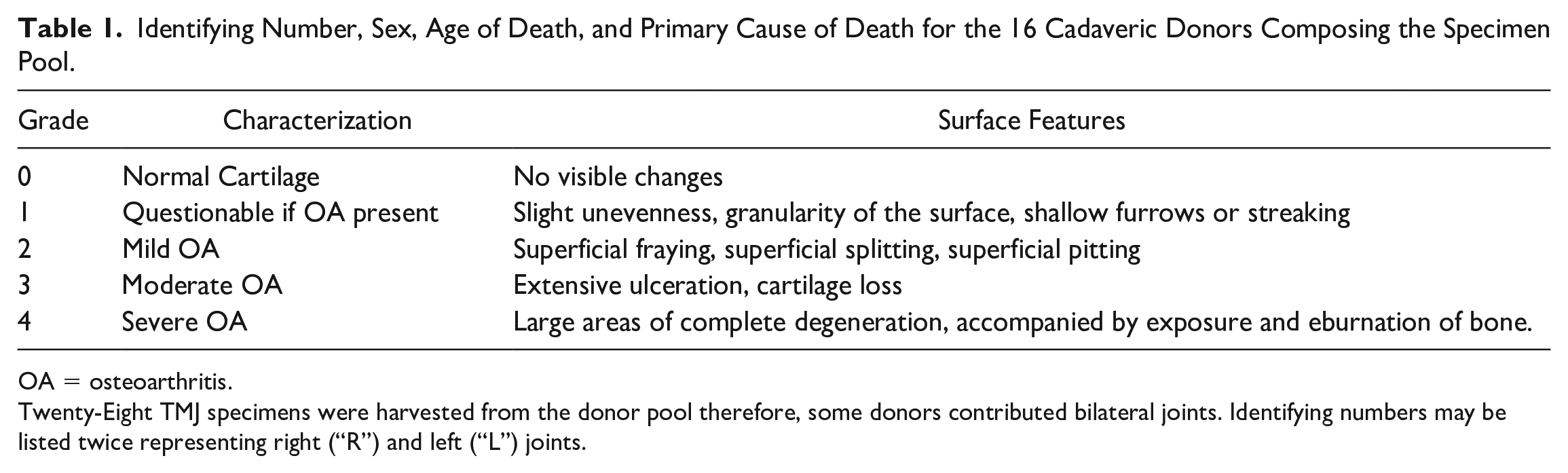
OA = osteoarthritis.
Twenty-Eight TMJ specimens were harvested from the donor pool therefore, some donors contributed bilateral joints. Identifying numbers may be listed twice representing right (“R”) and left (“L”) joints.
TMJ Photography
The anatomy of the TMJ was photographed using a 12-megapixel iPhone 13 Pro camera. All photographs included a drafting ruler for calibration. The condyle of the TMJ was photographed from the anterior, medial, lateral, and posterior views on 2 different backgrounds to allow for better interpretation of gross signs of OA. The disarticulated mandibular fossa was placed on the benchtop and photographed with calibration from above on 2 different backgrounds.
Gross Signs of OA
Specific types of lesioning seen in arthritic knee joint cartilage were investigated on the condyle of the mandible and the mandibular fossa of the temporal bone using the Kovler et al. 2014 validated, OA disease severity scale (DSS) described in the following section. This scale was validated in other synovial joints, most recently in the knee joint.12,13 Superficial pitting, fraying, or splitting would be indicative of Mild OA. Fibrillations are a specific type of focal, superficial damage that is a classical presentation of Mild OA. Fibrillations are early degenerative changes in osteoarthritis, marked by softening of the articular cartilage due to superficial proteoglycan losses and collagen disorganization, water retention, and cleft formation between groups of cartilage cells.14-16 Investigators who have long been involved with this OA research program describe these pathologies as “fuzzy” in appearance. Extensive ulceration or cartilage loss would be indicative of Moderate OA. When a specimen demonstrates large areas of complete chondral degeneration accompanied by exposure or eburnation of bone it is indicative of Severe OA. Eburnation is a degenerative process of bone commonly found in patients with osteoarthritis or non-union of fractures. Altered inflammatory signaling seen with OA will cause bone thickening and reactive conversion of the sub-chondral bone to an ivory-like sclerosis at the site of the cartilage erosion. 17 Visible, gross alterations to the cartilage such as linear cracks or articular cartilage erosions could be signs of mild, moderate, or severe OA depending on the depth of damage.6,14-16
Rating of Disease Severity
Cadaveric dissection and deep visual assessment of the intracapsular anatomy of the TMJ is not widely carried out in educational labs. Due to this lack of educational emphasis, cadaveric research involving the regional anatomy and gross signs of OA is even more rare. This considered, there were no known anatomical or clinical regional experts on cadaveric TMJ OA.
A validated tool developed to describe knee joint OA disease severity was utilized in this assessment. 12 This scale classes a synovial joint between Grade 0 OA, demonstrating no visible changes, to Grade 4 OA which represents severe OA. Specific gross surface features of the cartilage are listed as criteria to be classified as “No OA” (Grade 0), “Questionable OA” (Grade 1), “Mild OA” (Grade 2), “Moderate OA” (Grade 3), and “Severe OA” (Grade 4) and detailed in Table 2 . Sample images of Grades 1 to 4 OA on the TMJ are demonstrated in Figure 1 and are further discussed in the results. Currently, there are no specimens in the donor pool classified as Grade 0 OA likely, based on the fact we have not had the opportunity to assess any donors below the age of 69 years old. The histologic/histochemical grading system (MANKIN scale) and the OARSI (Osteoarthritis Cartilage Histopathology Assessment System) scales may be more familiar to some investigators but were not utilized in this assessment based on the absence of histological assessment completed.
Scale Modified From Kolver et al. (2004) to be Implemented in the Knee Joint and the TMJ.
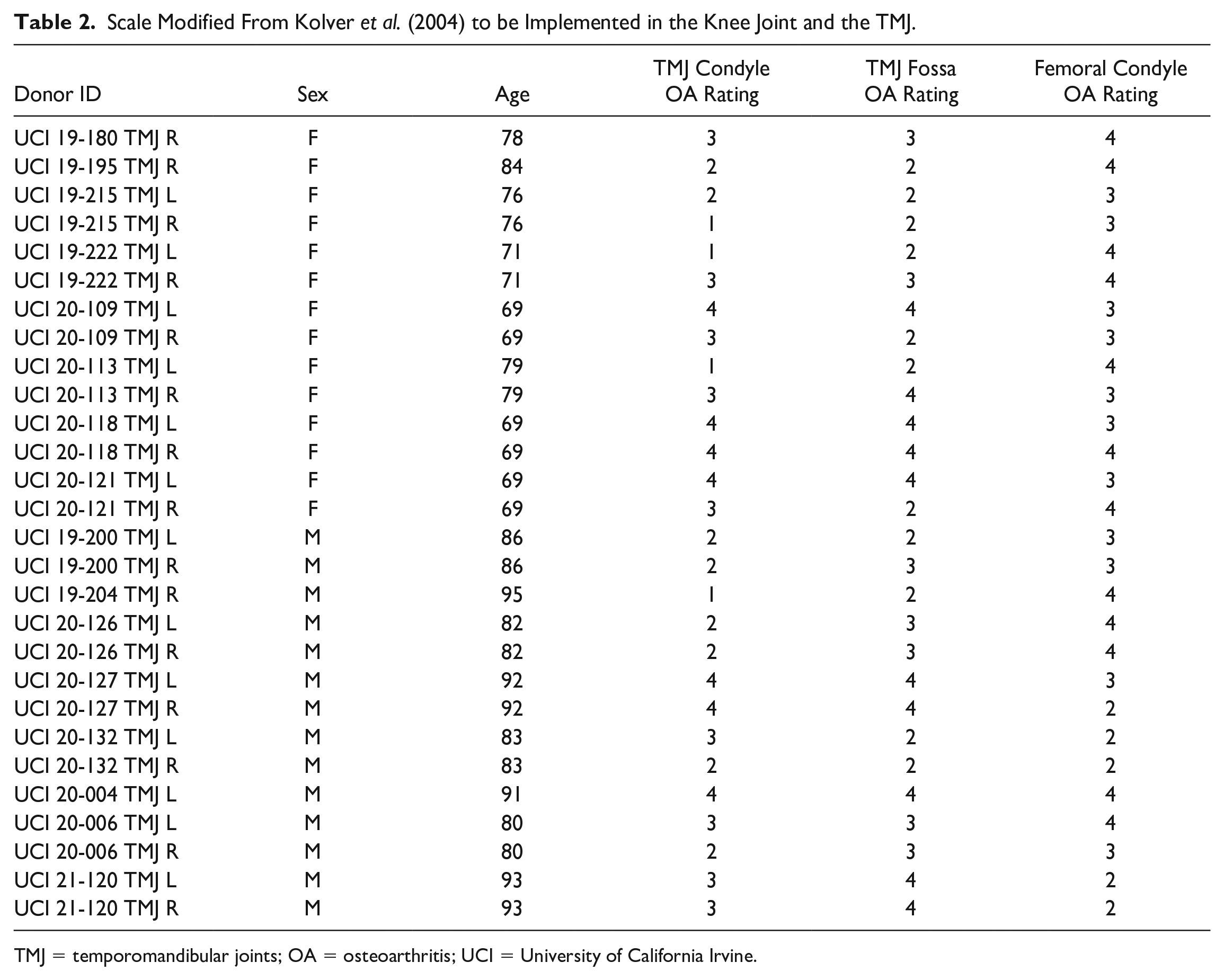
TMJ = temporomandibular joints; OA = osteoarthritis; UCI = University of California Irvine.
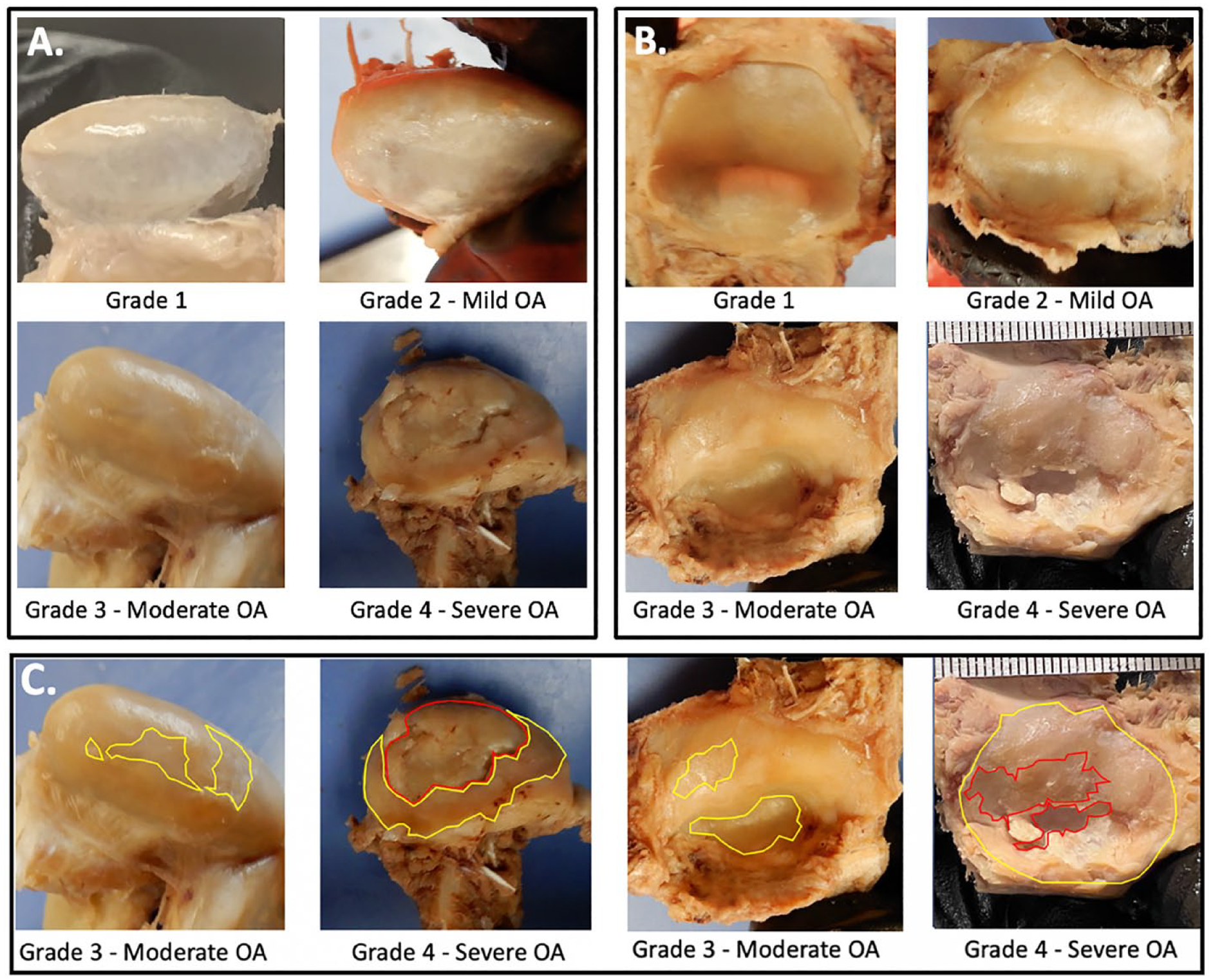
This figure represents sample images for Grade 1-Grade 4 OA disease severity on the TMJ condyle
Two blinded raters assessed the 31 TMJs for disease severity using the scale. A brief calibration session was carried out to clearly demonstrate examples of the surface feature irregularities seen with each grade of OA severity. This calibration session was carried out using knee joint images as to not use specimens included in the study at hand or bias the raters. Site of most profound disease (condyle or fossae) was noted for each TMJ specimen.
Additional anatomical information was collected for each TMJ specimen including condylar variation and state of articular disk degeneration. Condylar variation was based on the anatomical types discussed in Hegde 2013; the condyles were classed as Angled, Flat, Convex or Round on the frontal plane. 9 Disks were classed to have mild, moderate, or severe wear based on the presence of transparency, small holes, or large erosions. Many disks did not demonstrate visible wear.
Statistics
Statistical analyses were ran using SPSS statistics software. Krippendorff’s alpha (Kα) test 18 was used to estimate the interrater reliability of 2 OA raters’ condyles and fossae DSS scores. Assessments were ran using SPSS v27 (IBM Corp); an alpha of 1 to 0.8 represents strong interrater reliability. Condyle and fossae cartilage DSS ratings were compared using a 2-sample t-test with equal variance. This test was also utilized to determine if there was a statistically significant difference in the DSS scores for the TMJ condyle and the fossae between the sexes and in the older compared to the younger subgroups.
Case Study: 91-Year-Old Male Demonstrating OA in Multiple Joints
Severe gross signs of osteoarthritis appeared to present comparably in the TMJ and knee joint of a single, 91-year-old male donor. This led investigators to thoroughly assess this specific donor’s knee joints in addition to the TMJ. Severity of OA findings related to disease progression were evaluated in the right knee and the left TMJ. The left knee joint presented with a total joint replacement and the right TMJ was damaged in student dissection. The validated disease severity scale was used to assess the joints and significant signs of disease such as osteophytes, deep cartilaginous damages, and fibrocartilage damages were noted.
Donor Assessment for Knee Joint OA
Of the 31 TMJs that were harvested from this donor pool, 28 had available knee joints for inclusion in this study. In a previous study, the disease severity scale at hand was utilized and validated on a larger pool of knee joint specimens that included this subgroup. 12 DSS ratings for the 28 femoral condyle specimens were identified from this previous analysis where interrater reliability was demonstrated; these ratings were utilized in this novel comparison to the TMJ condyle and fossa DSS scores. Final statistical analysis involved comparing DSS scores for the TMJ condyle, TMJ fossa, and femoral condyles of a single donor.
Results
Superficial pitting and fibrillations were the most common form of degeneration in specimens with mild TMJ OA in this donor pool. Mild signs of OA often accompanied more pathological signs of OA on donors that were classed to have moderate or severe OA based on the disease severity scale. Donors with severe TMJ OA demonstrated extensive cartilage loss and cortical bone exposure. The mandibular fossa was more prone to demonstrate OA pitting (58%) and cartilage loss (46%) compared to the condyle (38%, 23%).
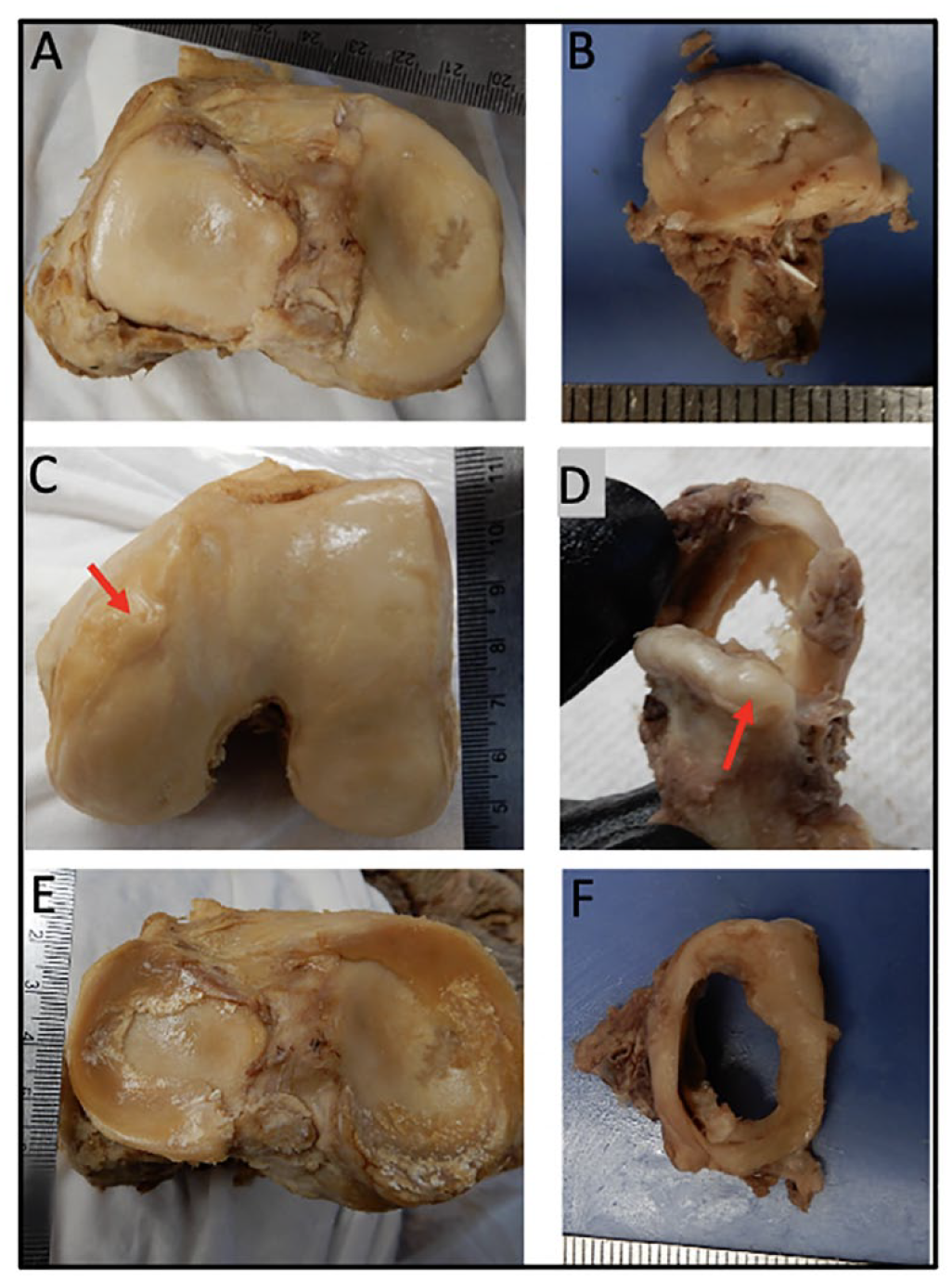
This study established that the validated scale for disease severity utilized in the hip, wrist, and knee joint of previous studies is an appropriate tool to utilize in disease severity assessment of the TMJ. Superficial pitting, fibrillations, articular cartilage erosions, and gross degeneration of the articular cartilage surfaces were all exhibited on a subset of TMJ specimens included in the study. Superficial pitting is a key element to be classed as Grade 2 OA based on this scale whereas cartilage erosion is a key element to be classed as Grade 3 or 4 (contingent on depth of erosion). Given these are requirements to be scored a Grade 2, 3, or 4 using this scale it was critical that investigators identified these gross signs of OA in the donor pool to justify the utilization of this tool. Both findings were regularly demonstrated on the mandibular fossa as well as on the mandibular condyle. Representative specimen images are included in
Figure 1A
Figure 1C demonstrates moderate and severe TMJ condyles and fossae. Specimens with severe OA demonstrate multiple depths of damage with large surface areas of cortical bone exposure and/or cortical bone damage (red). Specimens with Moderate OA demonstrate substantial areas of cartilage erosion (yellow); depth of damage tends to be more uniform with Moderate OA with less damage to the underlying bone. Stellate fractures, a common finding in the knee joint, were not demonstrated in this donor pool of TMJs ( Fig. 2 ). The validated scale does not specifically address stellate fractures as a specific requirement to be classed as a 0 to 4 Grade. Given these results, it was concluded that this scale for OA disease severity could be effectively used to class disease in arthritic TMJs.
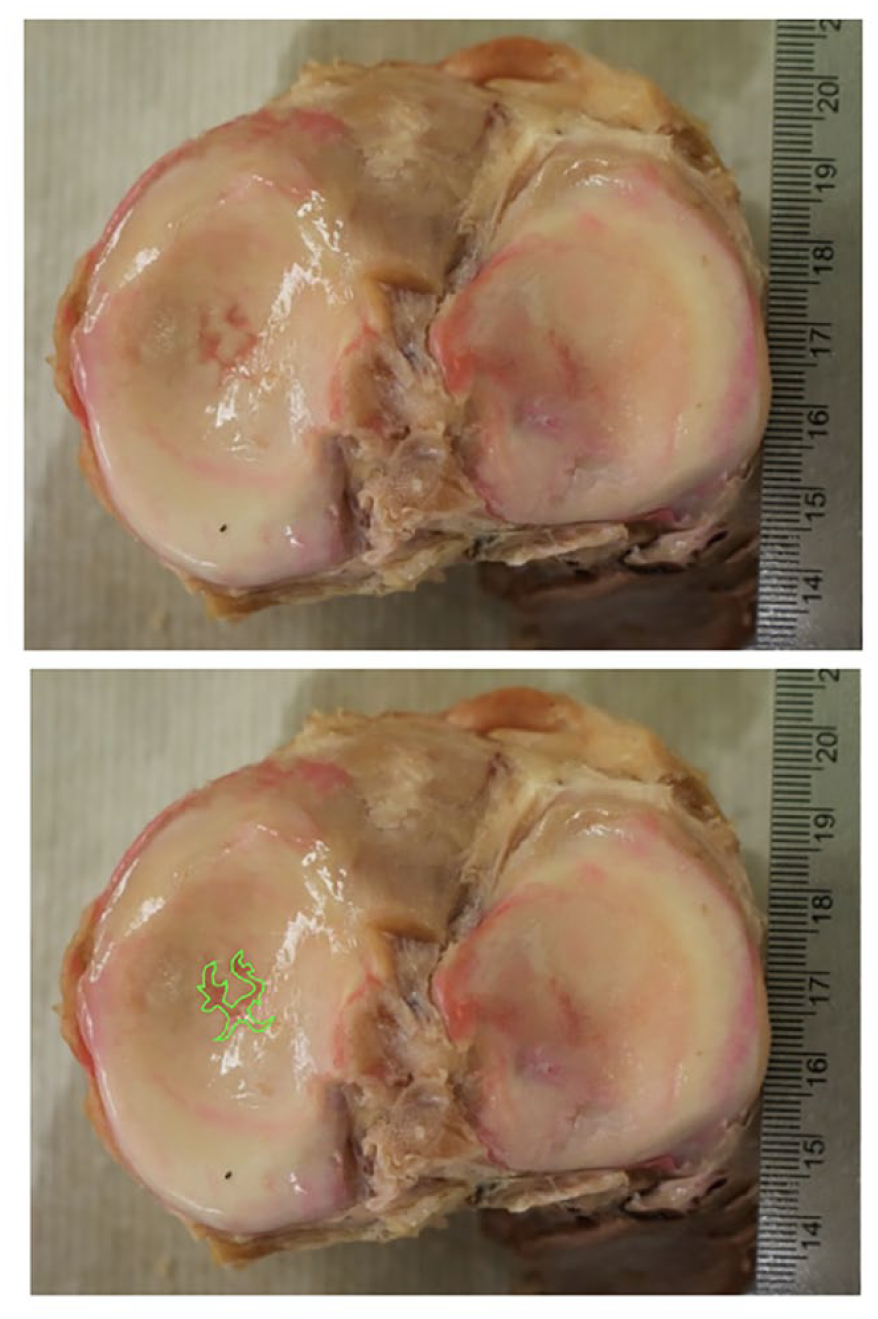
Sample image of a stellate fracture on the medial tibial plateau. Lower image is a duplicate of the above knee with the stellate fracture highlighted. Stellate fractures are often visible on specimens demonstrating moderate or severe OA. Pink coloration to the stellate fracture is an artifact of the embalming process.
The mandibular fossa demonstrated a statistically significant increase in disease severity compared to the mandibular condyle in the mixed sex donor pool (P = 0.035). The condyle scored an average score of 2.68 ± 0.96 on the OA DSS and the mandibular fossa scored an average of 2.90 ± 0.76 on the DSS. There was no statistically significant difference in the disease severity scoring of condyle or fossa specimens based on sex. The average DSS rating for the subgroup of female condyles was 2.73 ± 1.21 and 2.63 ± 0.78 for the male condyles. The average DSS rating for the subgroup of female fossae was 2.87 ± 0.84 and 2.94 ± 0.73 for the male fossae. The Kα results show high interrater reliability between the 2 raters of the condyles (α = .9353) and of the fossae (α = .9816). Based on the scoring provided by the most experienced rater, it was determined that the condyle and fossa of a single donor demonstrated equivalent disease severity in 58% (18/31 TMJs) of the donor pool. The fossa was the most degenerated in 29% (9/31) of specimens. The condyle was the most degenerated in 13% (4/31 TMJs) of specimens. Most importantly with respects to the biomechanical discussion to come, the fossa was most degenerated or equivalently degenerated as the condyle in (27/31) 87% of the donor pool at hand.
When the specimens were broken up into age groups 75 years old and below (youngest), 76 to 80 years old (middle), and 80 years old and above (oldest) there was no statistically significant difference in the disease severity scoring of specimens based on age for the condyle or the fossa (DSS score for condyles: youngest 3.25 ± 1.07, middle 2.3 ± 0.68, and oldest 2.62 ± 0.92. DSS score for fossae: youngest 3.13 ± 0.98, middle 2.6 ± 0.49, and oldest 3.00 ± 0.83). The sample was also divided in half by age, representing age groups of 69 to 79 years old and 80 to 95 years old. There was also no statistically significant difference in the disease severity scoring of specimen condyles or fossae based on this age breakdown (DSS score for condyles: youngest 2.75 ± 1.13 and oldest 2.6 ± 0.83. DSS score for fossae: youngest 2.81 ± 0.83 and oldest 3.00 ± 0.71).
The donor pool was also divided by sex and split into age subgroups for statistical analysis (male = 16; younger = 8, older = 8 / female = 15; younger = 8, older = 7). The subgroups were compared for disease severity on the condyle and the fossa. There was no statistically significant difference in disease severity on the TMJ fossa between the younger (69-71 years old; N = 8) and older (76-84 years old; N = 7) and females. There was a statistically significant difference in the disease severity on the TMJ fossa between the younger (78-83 years old; N = 8) and older (86-95 years old; N = 8) males; older male TMJ fossae demonstrated more severe OA findings (DSS score for younger males 2.5 ± 0.29, DSS score for older males 3.38 ± 0.84; *P = 0.02). When statistically comparing the younger and older female condyles for disease severity, it was discovered that the younger females demonstrated more pathological condyles compared to the older half of the female subgroup (DSS score for younger females 3.25 ± 1.07, DSS score for older females 2.14 ± 0.81; *P = 0.02). There was no statistically significant difference in disease severity on the TMJ condyle between the younger and older males.
The pathology of the articular disk was not statistically assessed with the validated scale for disease severity but obviously provided investigators with information on a specimen’s disease progression. Only 30 of the 31 total specimens had appropriate photography of the articular disk for this assessment; 17 of the 30 specimens (57%) of the articular disks demonstrated visible wear. Of those 17 specimens, 35% (6/17) demonstrated severe degeneration, 18% (3/17) demonstrated moderate degeneration, and 47% (8/17) demonstrated mild degeneration. It was hypothesized that condyle variation may affect the degree of degeneration present on a specimen.
This study demonstrates that gross signs of OA in the TMJs of cadavers are comparable to pathology found in the knee based on qualitative disease observations in addition to the previously mentioned nonparametric statistics. Similar articular cartilage and fibrocartilage disease findings presented on the TMJ and knee joint of a 91-year-old donor highlighting the systemic nature of OA. Osteophyte development and fibrocartilage damages occurred on both of the joints in the same donor. The right knee of a 91-year-old male donor demonstrated osteophyte growth on the anteromedial femoral condyle and extensive cartilage loss of the femoral condyles and the tibial plateau. The left knee joint was a total replacement so it can be inferred the OA disease progression was severe. The contralateral (left) TMJ was harvested from the same donor and also demonstrated severe cartilage erosion and linear cracking of the articular cartilage. A sizeable osteophyte was found on the superolateral aspect of the mandibular condyle. The menisci and the articular disks are fibrocartilaginous structures of the knee and TMJ, respectively. These structures appeared to wear in a similar fashion in the donor. The articular disk was completely worn through centrally and a fibrocartilaginous ring was the only persisting remnant of the articular disk ( Fig. 3 ).
This figure represents similar signs of OA in the knee joint and the TMJ on a single 91-year-old donor. (
There appears to be a correlation in the degenerative processes seen on the femoral condyles and the mandibular fossa. The mandibular condyle demonstrated significantly less severity in OA presentation compared to the femoral condyles (*P = 0.04) in the mixed sex donor pool (N = 28), whereas the fossa was comparably pathological to the knee (Average DSS score for mixed sex TMJ condyles 2.68 ± 1.00, DSS score for TMJ fossae 2.96 ± 0.87, DSS score for femoral condyles 3.25 ± 0.74). When OA signs were assessed in same sex donor groups (female N = 14, male N = 14) the mandibular fossa and the knee joint were consistently comparable, whereas the mandibular condyle was statistically less pathological compared to femoral condyles from the same donor (*P = 0.05 for male and female comparisons).
Discussion
The literature pool related to the study of osteoarthritis in the TMJ is limited compared to other synovial joints in the body that regularly experience the inflammatory condition. An even fewer number of research teams are investigating TMDs in a cadaveric model making these findings quite novel. Prior to analysis, there were 2 potential hypotheses related to disease severity in the TMJs compared to disease severity that has previously been assessed on the femoral condyles. 12 One plausible hypothesis was that the femoral condyles may demonstrate greater disease severity compared to TMJs of similar age due to the fact they are weight-bearing joints. The TMJ is not a weight-bearing joint along the line of gravity but Zhao and Ye 19 demonstrated that the maximum male bite force of the first molar was 120.66 kg or approximately 266 pounds. 19 These findings make hypothesizing greater or equivalent disease severity in the TMJs compared to the knee joints also reasonable. Human bite force data highlights how understandable it is to see such a large percentage of the population experience TMDs and gross alterations to the TMJ articular cartilage regardless of its stronger, fibrocartilage phenotype. Knee joints from donors that were 80 years old and above showed the highest disease severity scores whereas this study showed that the greatest average disease severity for the TMJ condyles and fossae were seen in the youngest donors. 12 This comparison emphasizes the complexity of TMDs and the plethora of physical and mental influences that may lead to degeneration of TMJ anatomy.
Similar to findings in knee joint OA cadaveric donors, superficial pitting and fibrillations were the most common form of degeneration associated with mild disease and accompanied more exacerbated findings such as extensive craters and bone exposure in donors with moderate and severe disease. Unlike the knee joint, linear cracks were quite uncommon on TMJ condyles and fossae, presenting on only a single severely arthritic TMJ condyle. In this donor pool, there were no discernible stellate fractures, a manifestation of OA commonly seen as a central deformity of the medial or lateral compartment of the tibial plateau. As far as disease presentation on the articular disk, the findings in this donor pool were very polarized. Disks were most regularly classed as mildly or severely degenerated indicating that once the pathogenesis and formation of a perforation begins it progresses quickly. The least prevalent anatomical variants of the TMJ condyle, the angled and rounded morphologies, all accompanied joints expressing moderate and severe disease with full-thickness holes in the articular disk. This may relate to classical explanations on evolution and natural selection; a disadvantageous feature may be breed out of a population to produce a stronger future generation. Sample images of the variations of mandibular condyles are included in Figure 4 and are listed from most common to least common based on the current literature. 9 The greater severity of pathology on the condyles of the Angled and Rounded variant representative images compared to the Convex and Flat variants is apparent.
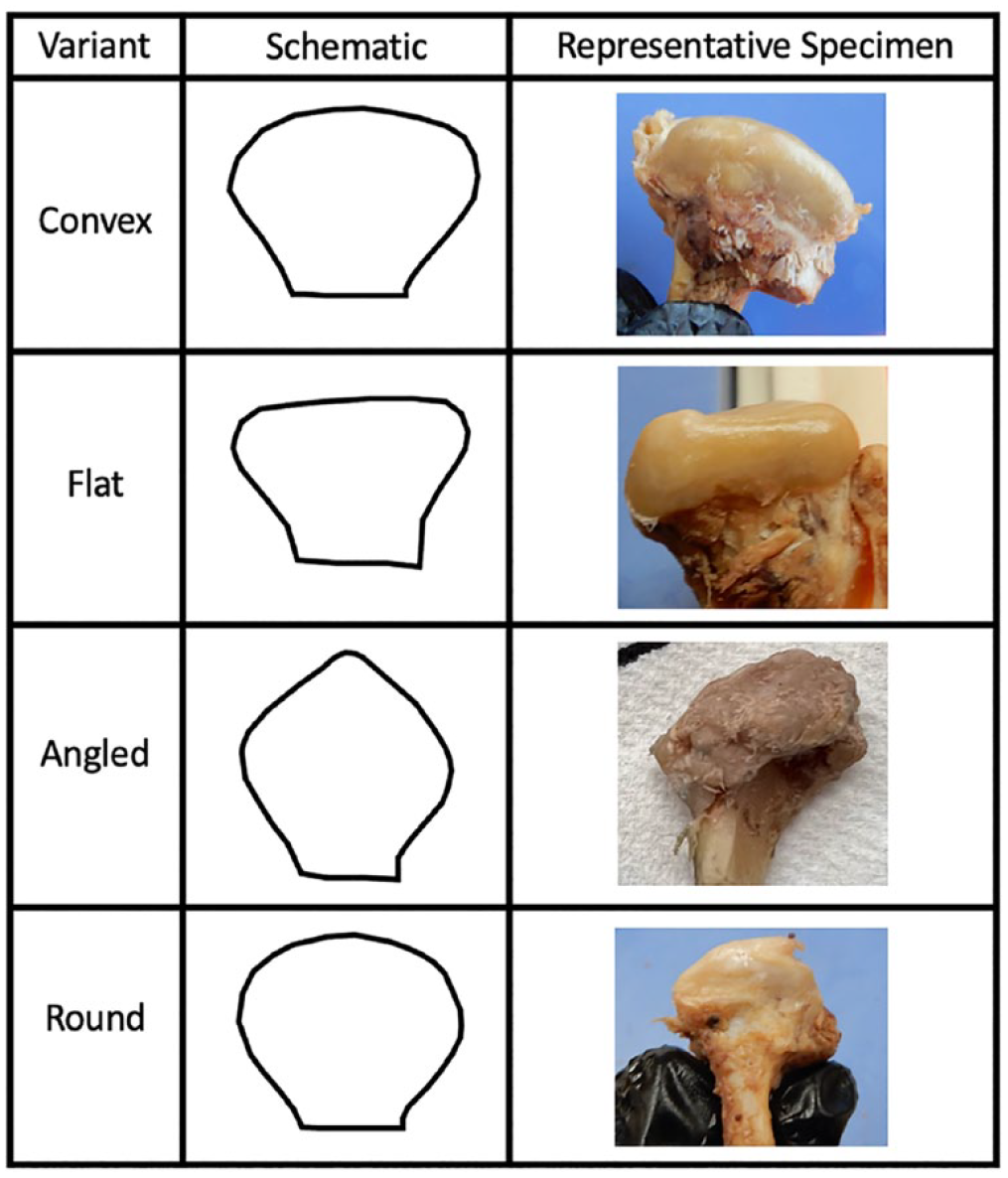
Figure demonstrates the variations of the mandibular condyle drawn in schematic and by representative photographs from the donor pool. Variants are listed from least common to most common in a recently assessment population (Hegde 2013). More severe signs of OA on the Angled and Rounded condyles are apparent in the representative photographs.
Assessing disease severity in the TMJs was more challenging compared to the assessment of the femoral condyles for several reasons. It is difficult to identify investigators with expertise in arthritic cadaver joints, especially TMJs. Many investigators that implement cadaveric dissection in their research are affiliated with biomedical sciences education in medical programs and these programs typically do not have a strong dissection emphasis on structure pertinent to dentistry such as the TMJ. Precuring specimen raters that have dissected TMJs, let alone had assessed TMJs for signs of disease, was regionally impossible so a calibration protocol for interpreting gross signs of cadaveric osteoarthritis was developed. Other limitations in this study warrant mentioning such as the minor degree of shadowing generated with the selected camera. This shadowing was offset but the substantially better quality of defect visualization seen with the iPhone 13 compared to a single-lens digital camera. All and all, the results of this assessment are to be considered with the context of a pilot population that heavily draws on case report data and future studies with a greater population size should be carried out.
This calibration protocol utilized arthritic knee joint specimen photographs from previous studies to highlight sample images of mild, moderate and severe osteoarthritis, Grades 2 to 4 on the disease severity scale. The calibration protocol also provided examples of superficial pitting and fraying, fibrillations and extensive cartilage loss. Moderate disease severity was described to demonstrate extensive cartilage loss on less than half of the specimen condyle or fossa. Severe OA was described to demonstrate extensive cartilage loss over more than half of the specimen. Often, specimens with severe OA demonstrated complete cortical bone exposure with potential damages to the underlying bone.
Once specimens were scored it was determined that there was strong interrater reliability using this assessment tool previously validated in the knee, hip and wrist joints. Separate disease severity scoring for a single TMJ specimen’s fossa and condyle allowed investigators to determine that the mandibular fossa appears to regularly be the site of more profound disease or equivalently profound disease as the condyle. This suggests the upper joint compartment laxity of the TMJ and the translational movements occurring there may be more likely to induce biomechanically abnormal movement, loading and OA compared to the hinging movements generated in the lower joint compartment.
There was no statistically significant difference in the disease severity scoring of the condyles or the fossae within this donor pool based on sex or age. The only comparisons that generated statistical significance were when the younger half of the female or male subgroups was compared to the older half of the female or male subgroups. Age groups were determined by splitting the donors in half; for the female subgroup, the younger specimens represented donors 69 to 71 years old and the older specimens represented donors 76 to 84 years old. Interestingly, younger females demonstrated more profound disease than older females (P = 0.02). Aging has a chief role in onset of disease findings and severity of degeneration in the knee joint12,17,20-22 but the aging process is seemingly a lesser factor compared to other influences that propel TMJ OA pathogenesis in women. For example, American women who experience a younger age of death may often be less healthy with accompanying comorbidities. Four out of the 8 female donors included in this donor pool had documented causes of death, such as atherosclerotic vascular disease and hypertensive heart failure, that could theoretically be prevented or reduced based on lifestyle choices. Age may be a lesser factor in the development of TMJ OA if systemically the patient is unhealthy. Additionally, social psychology and mental health research emphasize that a greater mental load is often put on women in heterosexual relationships, especially during child-bearing years, and substantial stress may be present from this potential unequal distribution of effort.23,24 TMDs are known to have a strong correlation with mental health diseases, anxiety disorders and stress and as many as 75% of TMD patients have a significant psychological abnormality. 25
These findings have importance in the dental clinic. It is reasonable to anticipate that the greater mobility and translational movements in the upper joint compartment would manifest more pathology. Normal chewing, and to a greater degree in cases of bruxism, significant lateral translational movements at the TMJ occur. In patients with bruxism, these lateral excursions can become exceptionally pronounced and would predominantly or solely alter the integrity of the upper joint compartment. It has been documented that when patients chewed increasingly harder foods, the masticatory width or lateral movement of chewing increased to increase the bite force. 26 From a dentistry perspective, one of the first recommendations given to TMD patients is to begin a soft food diet for 2-4 weeks to reduce chewing and allow for healing in the joint space. A bite splint is also a common approach to treating TMD patients because it protects the teeth during nighttime grinding and props the bite slightly open. This encourages healing in the joint space as the mandibular condyle is not capable of pressing on the articular disk and mandibular fossa as forcefully. As minor mouth opening is predominantly hinge movement and translational movements occur secondarily to allow for greater mouth opening, patients with severe TMD can experience a limited ability to depress the mandible. These patients face difficulty maintaining weight and adequate nutrition due to limited mouth opening, chewing motion, and generation of substantial bite force. 27
The case study on the 91-year-old male donor is a perfect example of the systemic nature of osteoarthritis. Similar articular cartilage disease findings such as osteophytes, extensive erosions and linear cracking presented on the TMJ and knee joint whereas there were also similar damages to the fibrocartilage structures. The menisci and the articular disk both demonstrated notable wear, especially at the sites of greatest intracapsular contact. Interestingly, the articular surfaces in the knee joint are lined with hyaline cartilage whereas the TMJ articular surfaces are lined with stronger fibrocartilage. Similar findings appear in both cartilage types implying the cartilage breed isn’t a limiting factor to disease progression. It could be questioned as to whether cadaveric signs of pathology in the TMJ are as assured to be osteoarthritis as they are in the knee joint. This cadaveric case report suggests dysregulated inflammatory signaling is a likely culprit for the gross alterations to the joint given the multiple pathology correlations to the patient’s knee joint and the high prevalence of osteoarthritis in the United States. From a patient care perspective, it is important to consider these common OA manifestations based on systemic inflammatory and metabolic alterations when educating patients on their joint dysfunction and pain, highlighting other joints are likely to become affected without lifestyle alterations.
Footnotes
Acknowledgments and Funding
The authors wish to thank individuals who donate their bodies and tissues for the advancement of education and research. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This project (Protocol 1681548-1) was reviewed and approved by the University of Nevada Las Vegas Institutional Review Board in Las Vegas, NV. This project was determined to be research not involving human subjects.