
Abstract
Objective
The purpose of this study was to compare the results of a biphasic synthetic scaffold (TruFit, Smith & Nephew) to microfracture for the treatment of knee cartilage defects and identify patient- and lesion-specific factors that influence outcomes.
Design
Prospectively collected data from 132 patients (mean age, 41.8 years; 69% male) with isolated chondral or osteochondral femoral defects treated with biphasic synthetic scaffolds (n = 66) or microfracture (n = 66) were reviewed. Clinical outcomes were evaluated longitudinally over 5 years with the Short Form–36 (SF-36), Activities of Daily Living of the Knee Outcome Survey (KOS-ADL), International Knee Documentation Committee (IKDC), and Marx Activity Scale. Cartilage-sensitive magnetic resonance imaging (MRI) was performed to evaluate osseous integration and cartilage fill in a subgroup of patients. Multivariate regression analysis was used to identify predictors of clinical outcomes within the scaffold group.
Results
Both groups demonstrated clinically significant improvements in knee clinical scores over 5 years (P < 0.01). There were no significant differences in KOS-ADL and IKDC scores between groups up to 5 years postoperatively. Marx activity level scores in the microfracture group declined over time, while significant improvements in activity level scores were observed in the scaffold group over 5 years (P < 0.01). Good-quality tissue fill and cartilage isointensity were more often observed in the scaffold group compared with the microfracture group, particularly with longer time intervals. Increasing age, high body mass index, prior microfracture, and traumatic etiology were predictors for inferior outcomes in the scaffold group.
Conclusions
Activity level and MRI appearance following treatment of cartilage lesions with the biphasic synthetic scaffold were superior to microfracture over time in this nonrandomized, retrospective comparison.
Introduction
Biphasic synthetic scaffolds offer a surgical approach for repair of focal chondral and osteochondral defects in the knee, which can be a significant source of morbidity for active individuals. These scaffolds support local migration of chondrogenic and osteogenic cells that facilitate formation of favorable reparative tissue.1,2 The TruFit plug (Smith & Nephew, Andover, MA) is a biphasic, acellular, synthetic polymer scaffold composed of poly(
Microfracture is still one of the most widely utilized cartilage repair techniques performed and is largely favored because it is an inexpensive, simple, single-stage procedure that can yield good clinical results in the short term.9-13 Although the strength and durability of mature fibrocartilage produced by the procedure remains a genuine concern, 14 microfracture still remains the standard to which most cartilage repair techniques are compared. To date, comparison of outcomes between treatment of cartilage defects with biphasic synthetic scaffolds and microfracture have not been reported. 6
The purpose of this study was to compare the outcomes of patients treated with the biphasic synthetic scaffold versus microfracture for femoral cartilage defects according to (1) patient-reported clinical outcomes and (2) quality of the cartilage repair tissue as measured by cartilage-sensitive magnetic resonance imaging (MRI). Additionally, patient- and lesion-specific factors that may contribute to clinical outcomes after treatment with the synthetic scaffold were identified. The study’s hypothesis was that patients would have better clinical outcomes and superior cartilage tissue fill after treatment with the synthetic scaffold compared to microfracture with longitudinal follow-up.
Methods
An institutional registry that prospectively collects clinical outcomes of any patient who undergoes a cartilage procedure at the Hospital for Special Surgery (New York, NY) was utilized for this study. The institutional review board approved the cartilage registry (#2013-024), and informed consent was obtained from all patients prior to enrollment. All patients were evaluated preoperatively and prospectively followed at 1, 2, 3, 4, and 5 years postoperatively.
Inclusion/Exclusion Criteria
Patients were included in the study if they met the following demographic or surgical criteria: (1) skeletally mature; (2) a single symptomatic cartilage lesion of the medial femoral condyle, lateral femoral condyle, or trochlea that was classified as Outerbridge grade III or IV at the time of diagnostic arthroscopy; (3) no significant osseous deficiency in the area of the lesion requiring additional bone grafting; (4) a lesion area of 1 to 6 cm2; and (5) minimum 2-year follow-up. Exclusion criteria were generalized osteoarthritis, inflammatory arthritis, osteonecrosis, multiple chondral lesions, and ligamentous instability of the knee. Patients were also excluded if meniscal deficiency was present requiring meniscal allograft transplantation in the affected compartment, treated patellar lesions, patellofemoral maltracking requiring proximal or distal realignment in the affected knee, malalignment requiring osteotomy of the affected compartment, or knee instability requiring concomitant ligament reconstruction. Of the 1,580 registry patients screened from 1999 to 2014, a total of 490 patients (211 synthetic scaffold, 276 microfracture) were identified. Among those treated with synthetic scaffold plugs, 127 were excluded due to concomitant procedures (1 osteotomy, 126 ligamentous reconstruction). Among those treated with microfracture, 87 were excluded due to concomitant procedures (4 osteotomy, 99 concomitant ligamentous reconstruction). An additional 18 and 47 patients from the synthetic scaffold and microfracture groups, respectively, were excluded due to lack of minimum 2-year patient-reported outcome measure (PROM) follow-up. This resulted in 66 patients who were treated with synthetic scaffolds. An equal number of microfracture patients were matched by including patients treated consecutively during the same time period (2005-2013) the synthetic scaffold was utilized at the institution. Therefore, a total of 132 patients were analyzed for this study (66 with biphasic synthetic scaffolds, 66 with microfracture).
Surgical Technique
Surgical procedures were performed by sports medicine fellowship-trained orthopedic surgeons that were familiar with use of the biphasic synthetic scaffold delivery system and microfracture technique. A diagnostic arthroscopy of the knee was performed in each patient to identify any additional intra-articular pathology. For each case, any concomitant procedures were recorded.
Surgical treatment with the synthetic scaffold was performed utilizing the technique described by Bedi et al. 15 Following diagnostic arthroscopy to characterize the lesion and address concomitant pathology, the medial or lateral portal incision was extended proximally and distally to create a mini-arthrotomy. In some cases, a portion of the patellar fat pad was excised to facilitate adequate visualization. With complete exposure of the lesion, the articular surface defect size was measured and the appropriate number of plugs needed to fill the lesion was determined. Using a commercially available trephine and coring reamer (Smith & Nephew, Andover, MA), individual plug host sites were created. Each plug site was drilled to a depth of approximately 8 mm below the surrounding normal articular surface. The area was then adequately cleared of bone debris to facilitate easy delivery of the scaffold and ensure a flush surface interface when inserted into place. The delivery device was then utilized to measure the precise depth of the defect. The plug was then manually trimmed to an appropriate length. Utilizing the same delivery device, the plug was gently impacted into place until it was fully seated within the defect. Slight adjustments with tamps were then made to ensure that the plug was flush with the surrounding hyaline cartilage. The mean plug diameter used was 10 mm (range, 5-11 mm). When multiple plugs were utilized, each successive plug was completely seated prior to preparation of the residual lesion area with the core reamer. The mean number of plugs used per case was 2.5 (range, 1-5), with a single plug used in 11 cases (17%), 2 plugs in 26 cases (39%), 3 plugs in 18 cases (27%), 4 plugs in 5 cases (8%), and 5 plugs in 6 cases (9%).
Microfracture was performed utilizing the surgical technique described by Steadman et al. 12 Using arthroscopic techniques, each femoral cartilage lesion was debrided to ensure the presence of stable margins and adequate removal of the calcified cartilage layer. Commercially available pick instruments (Conmed Linvatec, Largo, FL) were then used to penetrate the subchondral bone to an adequate depth in order to facilitate communication with the marrow. Subchondral bone bridges (approximately 3-4 mm wide) were left intact to preserve the integrity and function of the subchondral plate. In each case, adequate communication with the marrow was confirmed by decreasing the arthroscopic pump pressure and observing the release of blood and marrow elements from the microfracture channels.
Postoperative Rehabilitation
Postoperative rehabilitation was similar for both the synthetic scaffold and microfracture cohorts. Any patient with a medial or lateral femoral condyle lesion was immediately treated with continuous passive motion (CPM) starting at 0° to 60° for 6 hours per day with advancement of the flexion angle to tolerance. Passive range of motion was gradually increased, as the patient utilized the CPM machine over a 6-week time period. Synthetic scaffold and microfracture patients were allowed to begin weightbearing at 3 and 6 weeks after surgery, respectively. In both groups, patients treated for a trochlear lesion underwent continuous passive motion from 0° to 80° for 6 hours per day over a 6-week time period. Active flexion was limited from 0° to 40° and early weightbearing activity was allowed with the knee in full extension.
Assessment of Clinical Outcomes
For each patient, validated PROMs were obtained preoperatively and at 1, 2, 3, 4, and 5 years postoperatively. An independent observer performed pre- and postoperative data collection for all validated clinical outcome instruments. In order to assess the general health of each patient, the physical component summary of the Short Form–36 physical component summary (SF-36 PCS) (version 1.0) was utilized. 16 Knee function was assessed with the Activities of Daily Living of the Knee Outcome Survey (KOS-ADL) 17 and the International Knee Documentation Committee (IKDC) subjective score.18,19 Both of these instruments have been utilized to assess clinical outcomes in patients that have undergone cartilage restoration procedures with high reliability, validity, and responsiveness.18,19 Finally, patient activity level was assessed with the Marx Activity Rating scale. 19 Data attrition was observed in both groups with longitudinal collection of PROMs. In the scaffold group, there were 30 (45%), 54 (82%), 33 (50%), 23 (35%), and 13 (20%) patient responses at 1, 2, 3, 4, and 5 years, respectively; in the microfracture group, there were 34 (52%), 42 (64%), 25 (38%), 18 (27%), and 14 (21%) patient responses at 1, 2, 3, 4, and 5 years, respectively.
Assessment of MRI Outcomes
MRI outcomes were assessed on small subsets of patients in both groups that had MRI studies performed beyond 2 years from the index operation for the investigation of nonspecific knee symptoms. In the synthetic scaffold group, 15 cases (23%) were reviewed, and in the microfracture group, 16 cases (24%) were reviewed.
The cartilage assessment protocol for biphasic synthetic scaffolds has been previously described. 20 All MRI images were obtained on a clinical 3.0-T MRI unit (Signa HDx, General Electric Healthcare, Milwaukee, WI) using a standard 8-channel phased array knee coil (InVivo extremity coil; InVivo Corporation, Orlando, FL). Cartilage-sensitive morphologic MR images were obtained using a previously validated fast-spin echo pulse sequence.21,22 The cartilage morphological characteristics were graded using a previously reported series of imaging parameters, including signal intensity of the repair cartilage relative to the surrounding cartilage (hypointense, isointense, or hyperintense), gross appearance (depressed, flush, or proud), the presence or absence of hypertrophy or displacement, subchondral edema (mild [<1 cm2], moderate[1-2 cm2], or severe [>2 cm2]), bony overgrowth (absent, mild, severe), percentage of fill based on both coronal and sagittal images (0%-33%, 34%-66%, or 67%-100%), and integrity of adjacent cartilage (modified International Cartilage Repair Society [ICRS] classification).23,24 Osseous incorporation of the plug into the native trabecular architecture was graded as poor, partial poor, partial, or complete. The cartilage pulse sequences used to evaluate these repairs have been previously validated based on a suitable standard of arthroscopy. 21
Statistical Methods
Descriptive statistics are reported in means and standard deviations for continuous variables and frequencies and percentages for discrete variables. All continuous variables were tested for normality using the Shapiro-Wilks test and all were found to be normally distributed. Univariate analyses compared group differences between continuous variables using independent-samples t tests, while group differences in categorical variables were evaluated using chi-square or Fisher’s exact test.
Two-way mixed models with maximum likelihood estimates were used to account for data attrition of longitudinal collection of PROMs. Longitudinal assessment of all PROMs was analyzed within each study group as were between group comparisons at each time point. Bonferroni technique was used to adjust all P values for multiple comparisons. A post hoc power analysis showed that 66 patients in each group testing for a minimal clinically important difference (MCID) of 10 (±4) points for the KOS-ADL and 17 (±4) points for the IKDC achieved at least 80% power. 25
Multivariate linear regression models were created to quantify the relationship between all predictor variables and the clinical outcomes in the synthetic scaffold group while controlling for any potential confounding factors. Power analysis demonstrated that a sample size of 41 patients achieves 80% power to detect an R2 change of 0.20 in a model that contains 6 independent variables with statistical significance set to alpha equal to 0.05. The 2-year time point was the only time point (other than baseline) where more than 41 patients had available clinical data; therefore, only this time point was analyzed in the multivariate regression model.
All patient and surgical variables collected in the study were included as candidates in the regression model (age, sex, body mass index [BMI], etiology, previous microfracture, concurrent meniscal tear, location of lesion, number of plugs, and average plug size). Because of the exploratory nature of this analysis, a threshold of P = 0.15 was chosen as the threshold for retention in the final model. Using backward stepwise procedure, variables that failed to achieve a P value of ≤0.15 were removed from the final model. Variables that achieved a P value ≤0.05 were called statistically significant predictors. For all regression models, regression coefficients (B) and their respective 95% confidence intervals (95% CI) are reported. All analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY).
Results
The mean duration of follow-up was 3.4 years (range, 2-8 years) in the synthetic scaffold group and 3.6 years (range, 2-7 years) in the microfracture group. Patient demographics and baseline knee-specific clinical scores were similar between the 2 groups. The proportion of males to females (P < 0.01), mean preoperative SF-36 PCS score (P = 0.05), and mean preoperative Marx activity rating score (P < 0.01) were higher in the microfracture group ( Table 1 ). Mean lesion size was smaller in the microfracture group (2.2 vs. 3.0 cm2, P = 0.02). Among the 66 synthetic scaffold cases analyzed, there was 1 failure (1.5%) due to persistent pain and progressive osteoarthritic change. This patient underwent a medial unicompartmental knee replacement 3 years postoperatively. Additionally, there were 2 perioperative complications that were treated with reoperation; 1 deep infection at 3 months was treated with irrigation and debridement, and 1 case of arthrofibrosis at 1 year was treated with arthroscopic lysis of adhesions and manipulation.
Patient Demographics, Intraoperative Data, and Preoperative Outcome Scores. a
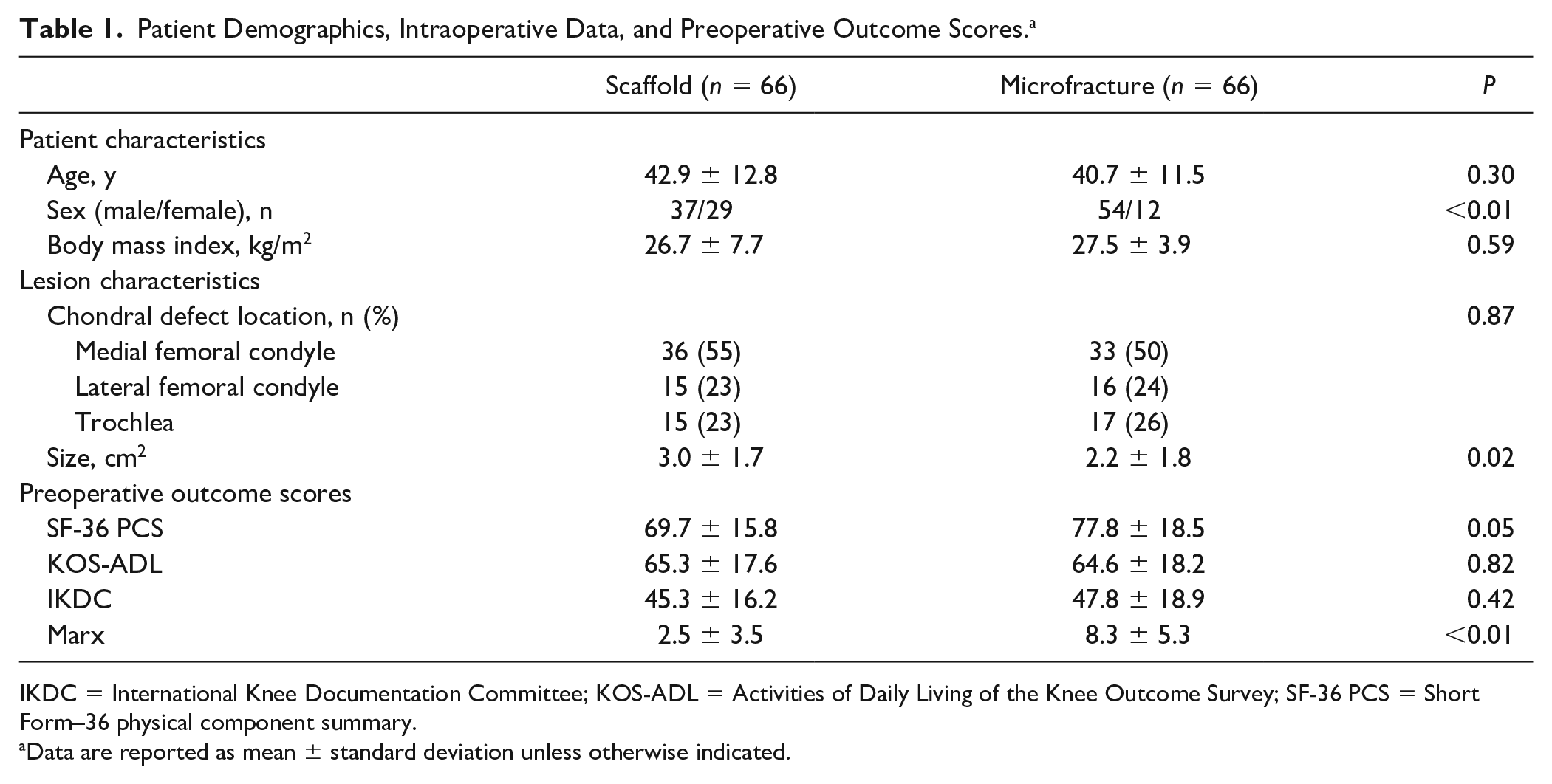
IKDC = International Knee Documentation Committee; KOS-ADL = Activities of Daily Living of the Knee Outcome Survey; SF-36 PCS = Short Form–36 physical component summary.
Data are reported as mean ± standard deviation unless otherwise indicated.
Patient-Reported Clinical Outcomes
Mean postoperative SF-36 PCS scores significantly improved in the synthetic scaffold group from baseline to all postoperative time points (P < 0.01 for all). In contrast, mean postoperative SF-36 PCS scores in the microfracture group were not significantly different from baseline to any postoperative time point (P = 1.00). At all postoperative times, SF-36 PCS scores were not significantly different between the scaffold and microfracture groups ( Fig. 1 , Supplemental Table).
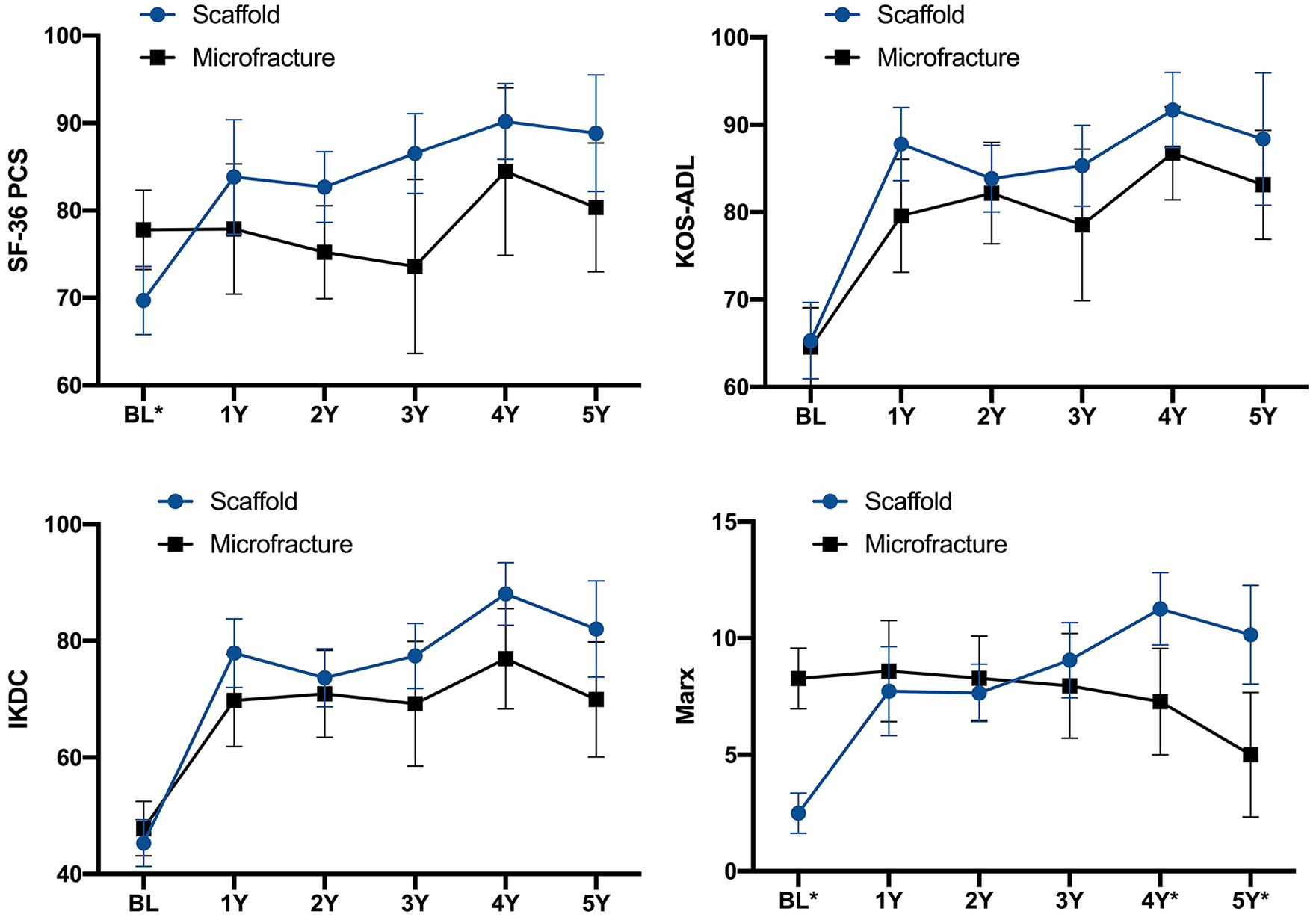
Patient-reported outcome scores at baseline (BL) and 1, 2, 3, 4, and 5 years postoperative for the SF-36 PCS, KOS-ADL, IKDC, and Marx Activity Rating Scale. *Indicates significant difference (P < 0.05) between synthetic scaffold and microfracture groups. Error bars indicate 95% confidence intervals. IKDC, International Knee Documentation Committee; KOS-ADL, Activities of Daily Living of the Knee Outcome Survey; SF-36 PCS, Short Form–36 physical component summary.
Mean postoperative KOS-ADL and IKDC scores significantly improved in both groups from baseline to 1, 2, 3, 4, and 5 years postoperatively (P < 0.01), with scores in both groups meeting the MCID threshold (10 points for the KOS-ADL, 17 points for the IKDC) at all postoperative time points. KOS-ADL and IKDC scores were higher in the scaffold group compared with microfracture group at all postoperative time points, although these differences were not significant ( Fig. 1 , Supplemental Table).
Mean postoperative Marx Activity Rating Scale scores steadily declined over time in the microfracture group, with 5-year scores being significantly lower than baseline scores (P < 0.01). In contrast, mean postoperative Marx Activity Rating Scale scores significantly improved in the scaffold group at every postoperative time point compared with those at baseline (P < 0.01). At 4 and 5 years, postoperative Marx Activity Rating Scale scores were significantly higher in the synthetic scaffold group compared with the microfracture group (P < 0.01) ( Fig. 1 , Supplemental Table).
MRI Outcomes
There were no significant differences between the 2 groups in signal intensity of the repair cartilage, gross appearance, percentage fill, integrity of the adjacent cartilage, or presence of synovitis ( Table 2 ). The microfracture group showed significantly more bony overgrowth (9/16) of the cartilage repair tissue compared with the synthetic scaffold group (1/15) (P = 0.01) ( Figs. 2 and 3 ). The synthetic scaffold cases demonstrated native cartilage isointensity in a majority of cases (67%, 10/15), including the majority of cases at greater than 4-year follow-up (71%, 5/7) ( Figs. 4 and 5 ). The microfracture group showed isointensity of the repair cartilage in approximately 50% of analyzed patients, with no trend in signal intensity over time ( Figs. 4 and 5 ). Furthermore, the majority of the synthetic scaffold cases had a flush cartilage surface (60%, 9/15), in contrast to the microfracture group, of which the majority had recessed cartilage surfaces (63%, 10/16). All synthetic scaffold cases with a follow-up of greater than 4 years (n = 7) had complete cartilage fill, whereas several (5/13, 38%) microfracture cases with similar long-term follow-up had <33% cartilage fill ( Figs. 2 and 5 ). In 3 of the 16 microfracture cases (19%), there was a complete absence of any cartilage repair tissue. Regarding bony incorporation in the scaffold group, only 1 patient (7%) showed poor bony incorporation. The majority of patients treated with synthetic scaffolds demonstrated complete (53%, 8/15) or at least partial bony incorporation (40%, 6/15).
Qualitative MRI Assessment Results. a
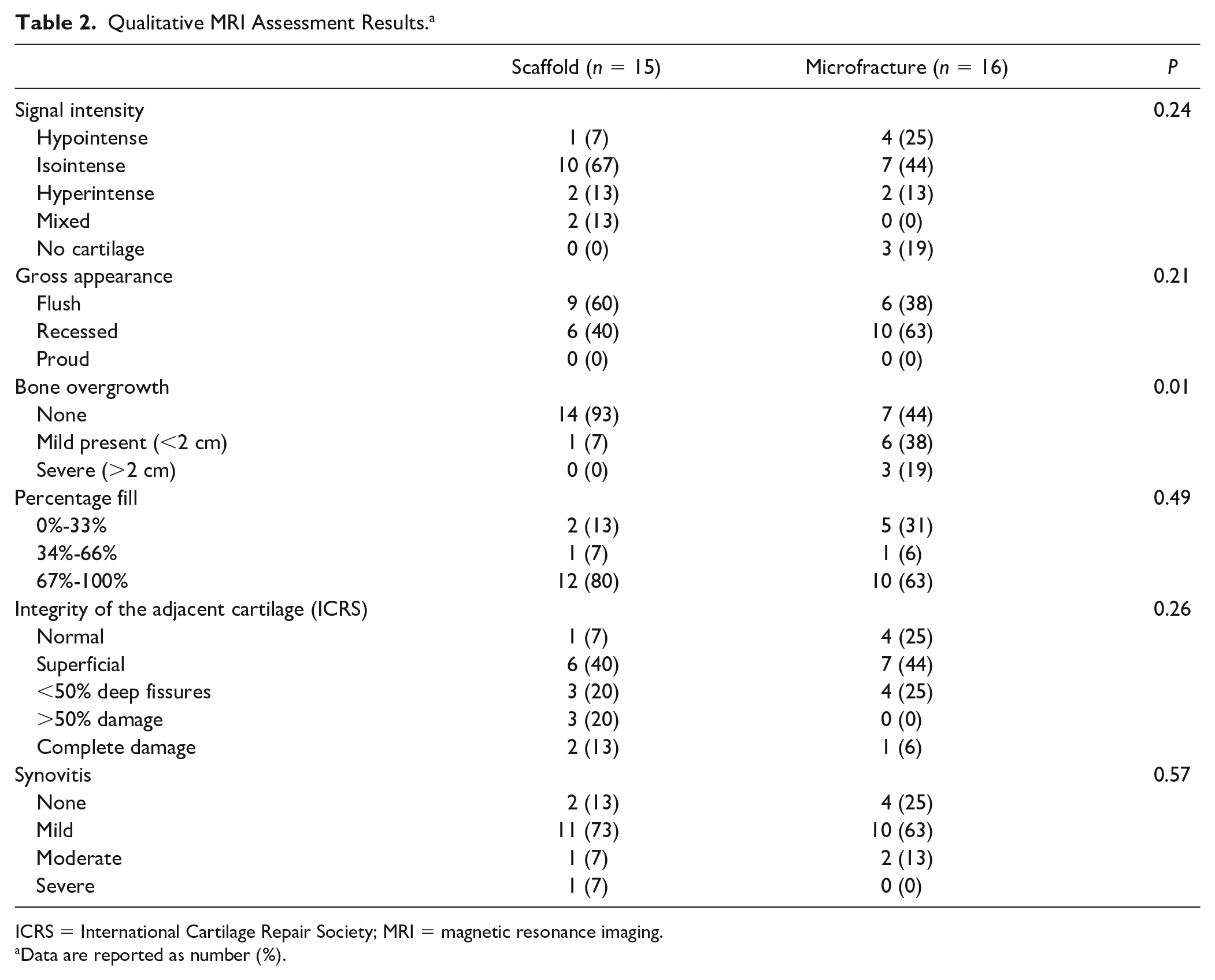
ICRS = International Cartilage Repair Society; MRI = magnetic resonance imaging.
Data are reported as number (%).
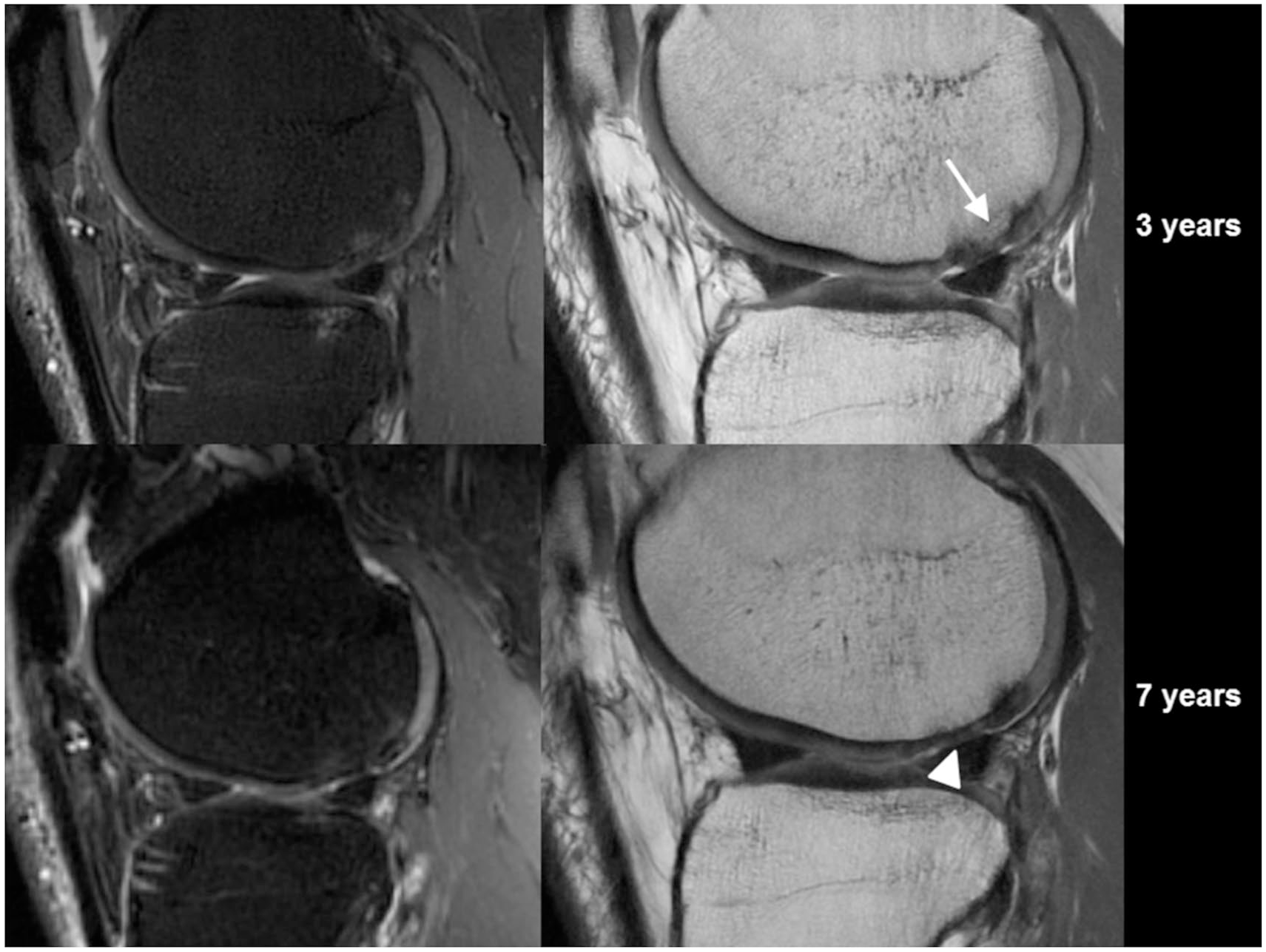
Serial magnetic resonance images (MRIs) of a single microfracture case. At 3 years, sagittal T2-weighted fast spin echo (FSE) MRI scan (left) and a sagittal proton-density FSE scan (right) showed partially recessed cartilage with bony overgrowth (arrow) at 3 years and recessed cartilage (arrowhead) at 7 years.
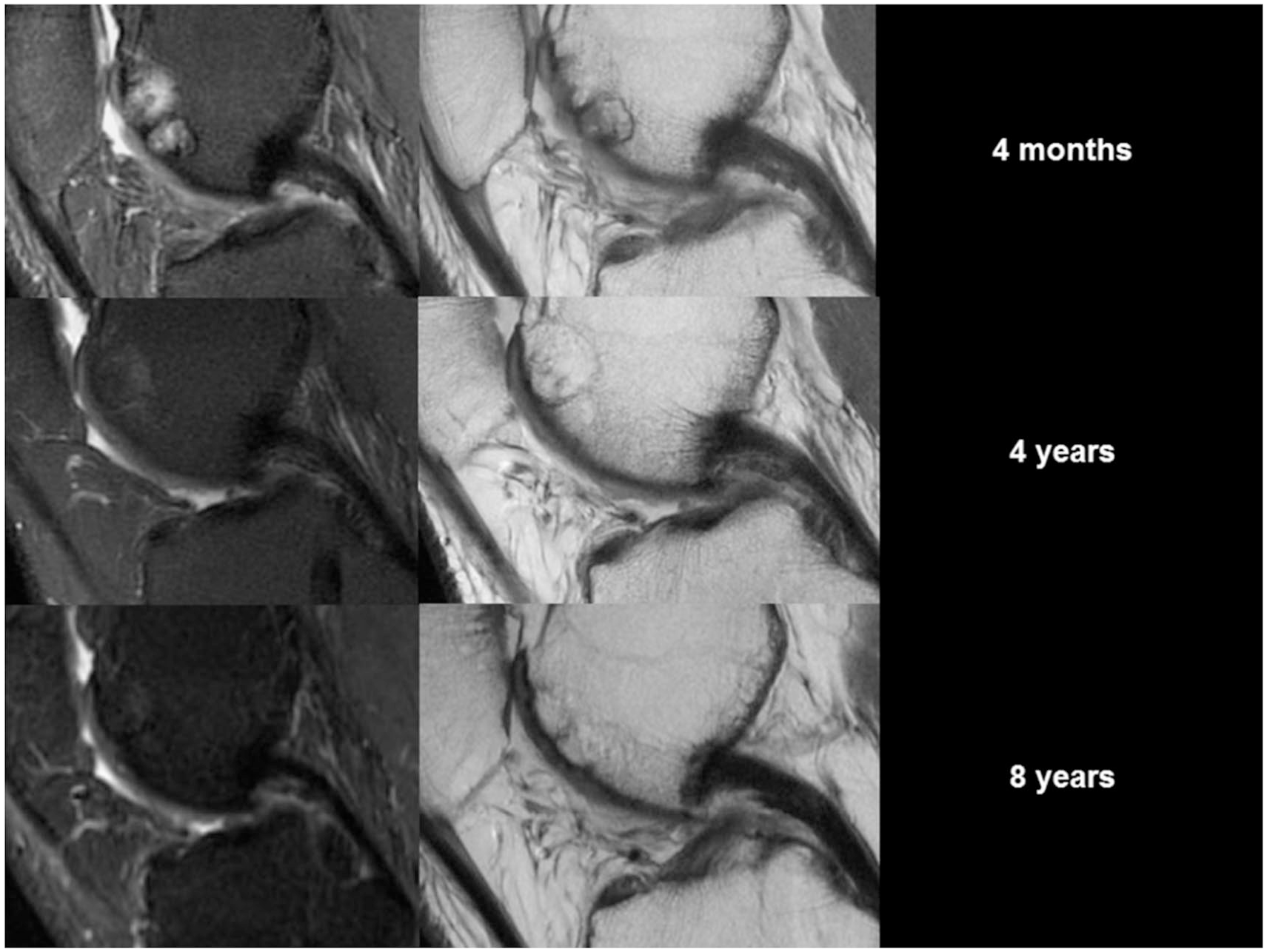
Serial magnetic resonance images (MRIs) of a single biphasic synthetic scaffold case. At 4 months, a sagittal T2-weighted fast spin echo (FSE) MRI scan (left) showed high signal, and a sagittal proton-density FSE scan (right) showed a perifocal sclerotic rim around the plug with poor bone incorporation. At 2 years, the signal reduced (left), and there was partial bone incorporation and isointensity of the repair cartilage (right). At 8 years, there was no high signal in the bone (left) and excellent cartilage fill and bony incorporation (right).
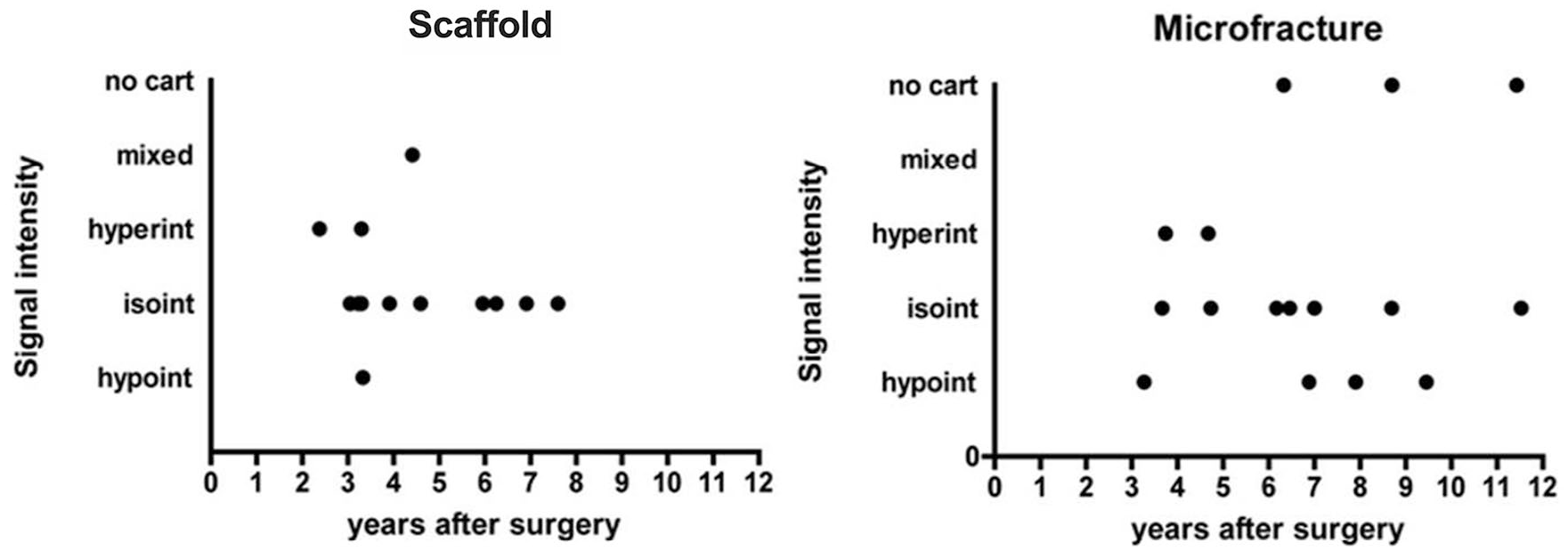
Biphasic synthetic scaffold cases demonstrated native cartilage isointensity in the majority of cases (67%, 10/15), particularly with the majority of cases at greater than 4-year follow-up (71%, 5/7), whereas the microfracture group showed isointensity of the repair cartilage in approximately 50% of analyzed patients, with no specific pattern over time.

Representative magnetic resonance images at 6-year follow-up showing good (left column) and bad (right column) cartilage repair after synthetic scaffold (top row) and microfracture (bottom row) treatment.
Multivariate Linear Regression
Results from the multivariate regression model indicated that increased age, BMI, a traumatic etiology, and a previous microfracture procedure were all predictors of clinical outcomes after treatment with biphasic synthetic scaffolds at 2-year follow-up after adjusting for all other potential confounders in the model ( Table 3 ). Increases in age and BMI were significant predictors for worse scores at 2-year follow-up, with 1 year and 1-unit increases associated with approximately half-point decreases in IKDC scores (B = −0.6 and −0.7, respectively; P < 0.01 for both). Additionally, patients with traumatic chondral lesions and those treated previously with microfracture had worse KOS-ADL and IKDC scores ( Table 3 ). Increased age and higher BMI were significant predictors of lower Marx activity levels at 2-year follow-up, whereas male sex was significantly associated with higher Marx activity levels ( Table 3 ).
Multivariate Regression Analysis for Predictors of Patient-Reported Outcomes after Synthetic Scaffold Treatment at 2-Year Follow-up.
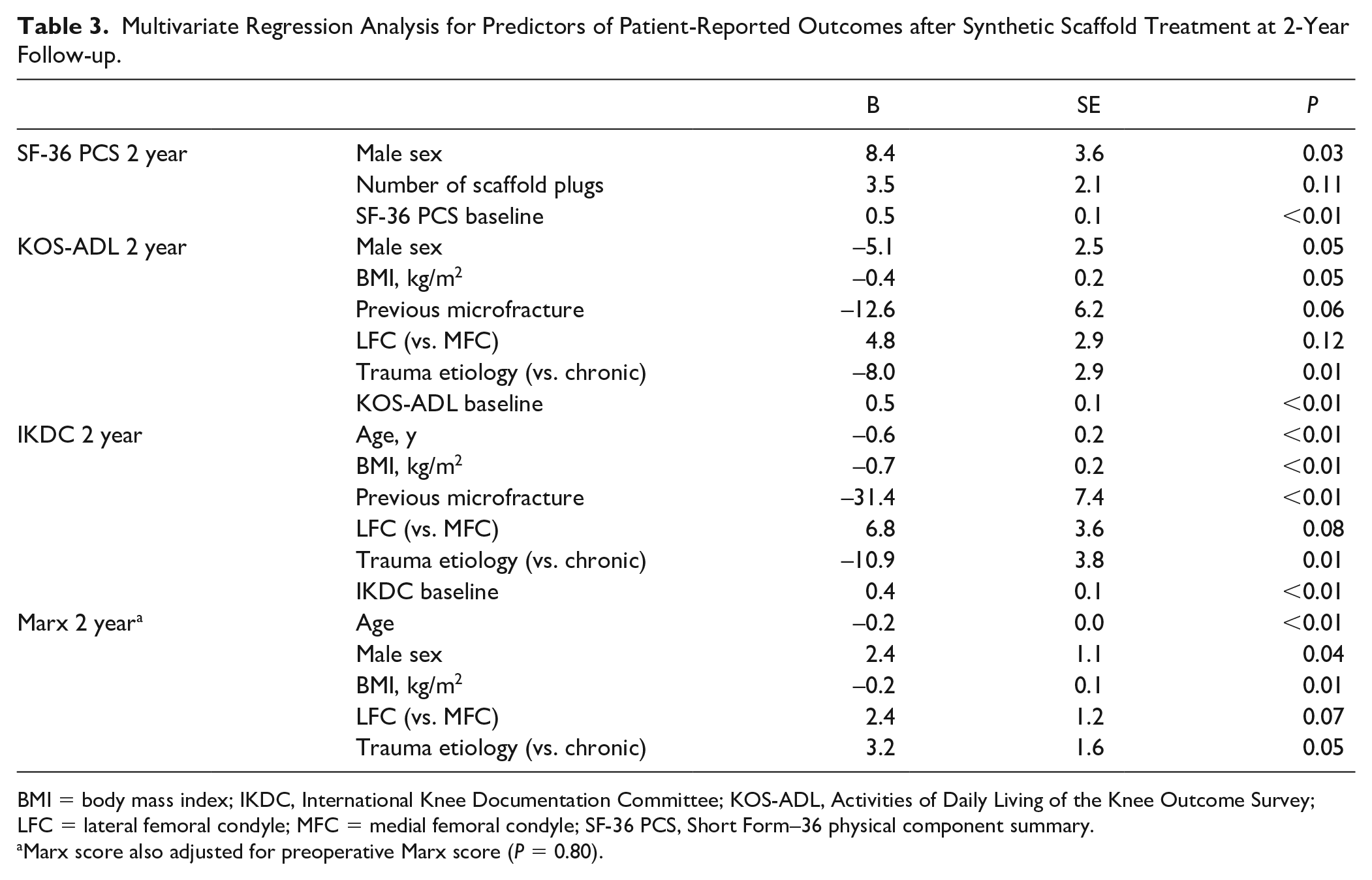
BMI = body mass index; IKDC, International Knee Documentation Committee; KOS-ADL, Activities of Daily Living of the Knee Outcome Survey; LFC = lateral femoral condyle; MFC = medial femoral condyle; SF-36 PCS, Short Form–36 physical component summary.
Marx score also adjusted for preoperative Marx score (P = 0.80).
Discussion
The main study finding was that patients treated with biphasic synthetic scaffolds demonstrated clinically significant improvements in outcome scores out to 5 years postoperatively, with superior activity level scores compared to microfracture after 3 years. Qualitative MRI assessment showed that the quality of the cartilage repair tissue was better in the synthetic scaffold group and also matured over time. Increasing age, BMI, previous microfracture, and traumatic etiology were identified as negative predictors factors for outcomes following synthetic scaffold implantation.
Animal studies using the biphasic synthetic scaffold for osteochondral defects of the medial femoral condyle and lateral trochlea have demonstrated excellent tissue fill, host incorporation, and formation of a hyaline-like cartilage repair tissue with more favorable histological and biomechanical characteristics than microfracture repair tissue.21,26 The majority of studies reporting clinical outcomes of the same synthetic scaffold have been positive, although most have been small case series with short- to mid-term follow-up. Several clinical studies examining use of the synthetic scaffold for cartilage defects have demonstrated similar trends to the current study. D’Ambrosi et al. 8 examined 21 patients treated with biphasic synthetic scaffolds arthroscopically for grade IV lesions in the knee. At a final follow-up of approximately 8 years, patients had maintained high Knee Injury and Osteoarthritis Outcome Scores (KOOS) and Hospital for Special Surgery (HSS) scores (81.9 and 83.7, respectively) that were similar to 3-year postoperative scores and significantly improved compared with baseline scores. This is in contrast to the deterioration of outcomes of microfracture at mid-term follow-up. 10 Another retrospective study comparing 35 patients treated with synthetic scaffolds to 31 with autologous osteochondral mosaicplasty demonstrated similar reoperation rates between groups at a mean follow-up of 22 months. 27 However, return to sport was significantly lower in the synthetic scaffold group, as were pain and functional outcome scores, although they did not reach statistical significance.
On MRI, native cartilage isointensity was more often observed in the synthetic scaffold group (67%, 10/15), particularly with increasing time after surgery. Furthermore, only 1 patient showed poor bony incorporation (40 months after surgery). In a study of 57 patients treated with synthetic scaffolds, in which the majority (75%) of patients had MRIs at 24 months, Gelber et al. 28 found good cartilage layer integration but high heterogeneity and no filling of the subchondral bone layer. Subsequent published studies examining the MRI appearance of the synthetic scaffold plug have reported increased maturation and defect fill at longer postoperative intervals,5,7,20,29 consistent with the findings of this study. Bugelli et al. 29 reported progressive healing and graft integration on MR images from 1 to 5 years, with maintenance of articular surface congruency and osseous integration past 5 years. It should be noted that MRI appearance of the subchondral bone and clinical outcomes do not always correlate after osteochondral treatment, as this has been demonstrated for both synthetic scaffolds and fresh osteochondral grafts.28,30
The multivariate regression analysis in this study found that predictors of inferior clinical outcomes after synthetic scaffold treatment included increasing age, BMI, and previous microfracture, all of which are consistent with trends identified in prior studies evaluating cartilage repair.13,31-34 The trend toward better scores in patients who were younger may be attributed to the degenerative processes and declining healing potential that progress with age. Higher BMI is a logical negative risk factor due to greater loading conditions in the knees of heavier patients, which would predispose the cartilage repair tissue to early breakdown. Similarly, alteration of the subchondral bone from prior microfracture may compromise the potential of osseous integration and creeping substitution after implantation with the synthetic scaffold. The multivariate analysis also found that traumatic etiology was associated inferior clinical outcomes after treatment with scaffolds. The effect of etiology on outcomes after osteochondral restoration is not well known. Oftentimes, the line between traumatic and degenerative lesions is not well defined, and traumatic cartilage lesions often present with concomitant ligamentous injuries, which can make this question difficult to study. Rather, age of the defect and duration of symptoms seem to be more important predictors of outcomes for focal traumatic cartilage lesions. 32
There are several limitations with this study. Prospectively collected data were retrospectively reviewed, and patients were not randomized to the treatment groups. As such, biphasic synthetic scaffolds may have been utilized for the treatment of osteochondral lesions, whereas microfracture treatment may have limited for chondral lesions, although these data were not available. Data attrition from longitudinal collection of PROMs was observed in both groups. Although 2-way mixed models with maximum likelihood estimates were used to account for this limitation, the data was likely underpowered at longer-term follow-up to detect any significant differences between treatment groups. Preoperative differences in sex and activity level between groups may have confounded the results. However, many large studies have not found any difference in outcomes between males and females after cartilage surgery.35-37 Additionally, although microfracture patients reported higher preoperative Marx activity scores, subsequent postoperative scores fell below preoperative levels, while scaffold patients exhibited improving Marx scores over time that were significantly higher than scores from the microfracture group at years 4 and 5. Another limitation of this study was that postoperative MRIs could only be obtained for a subset of our study group, which may incur selection bias.
In conclusion, biphasic synthetic scaffolds are an effective treatment option for the treatment of articular cartilage defects of the knee. This study demonstrated good, durable clinical results with 5-year longitudinal follow-up. The synthetic scaffold system is a simple, single-step, off-the-shelf option that is easier to execute compared to other cell-based approaches. Further research and development of synthetic scaffold technology, through the enhancement of the biomaterial or augmentation with other factors such as cells or bioactive anti-inflammatory agents, could allow the potential of this promising surgical approach to further improve the treatment of cartilage defects in the knee.
Supplemental Material
Supplemental_Table_v2 – Supplemental material for Synthetic Biphasic Scaffolds versus Microfracture for Articular Cartilage Defects of the Knee: A Retrospective Comparative Study
Supplemental material, Supplemental_Table_v2 for Synthetic Biphasic Scaffolds versus Microfracture for Articular Cartilage Defects of the Knee: A Retrospective Comparative Study by Dean Wang, Danyal H. Nawabi, Aaron J. Krych, Kristofer J. Jones, Joseph Nguyen, Ameer M. Elbuluk, Nadja A. Farshad-Amacker, Hollis G. Potter and Riley J. Williams in CARTILAGE
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The institutional review board approved the cartilage registry (#2013-024).
Informed Consent
Informed consent was obtained from all patients prior to enrollment.
Trial Registration
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.