
Abstract
Objective:
The purpose of this systematic review was to compare activity-based outcomes after microfracture, autologous chondrocyte implantation (ACI), and osteochondral autograft (OAT).
Design:
Multiple databases were searched with specific inclusion and exclusion criteria for level III and higher studies with activity outcomes after microfracture, OAT, osteochondral allograft, and ACI. Activity-based outcomes included the Knee Injury and Osteoarthritis Outcome Score (KOOS), the Tegner Score, the Cincinnati Knee scores, the International Knee Documentation Committee (IKDC) subjective knee score, the Marx activity score, and/or the rate of return-to-sport.
Results:
Twenty studies were included (1,375 patients). Although results were heterogeneous, significant advantages were seen for ACI and OAT as compared with microfracture in Tegner scores at 1 year (ACI vs. microfracture, P = 0.0016), IKDC scores at 2 years (ACI vs microfracture, P = 0.046), Lysholm scores at 1 year (OAT vs microfracture, P = 0.032), and Marx scores at 2 years (OAT vs microfracture, P < 0.001). The only score or time point to favor microfracture was Lysholm score at 1 year (ACI vs microfracture, P = 0.037). No other standardized outcome measures or time points were significantly different. Several studies demonstrated significantly earlier return to competition with microfracture. Overall reoperation rates were similar, but of reoperations, a higher proportion of those following ACI were unplanned with the majority of performed for graft delamination or hypertrophy.
Conclusions:
ACI and OAT may have some benefits over microfracture, although return-to-sport is fastest following microfracture. Heterogeneity in technique, outcome measures, and patient populations hampers systematic comparison within the current literature.
Introduction
Injuries to the articular cartilage are common among those with knee pain, identified in up to 63% of arthroscopies.1,2 The incidence is also high in active populations, with MRI studies demonstrating signal abnormalities in 40% to 50% of asymptomatic collegiate and professional athletes.3,4 A variety of etiologies contribute to the development of these lesions in active patients including repetitive microtrauma from high axial and shear stresses at the articular surface with sporting activity. In addition, acute traumatic injuries can cause chondral damage, with an incidence up to 47% in anterior cruciate ligament (ACL) tears. 5 Ligamentous instability, malalignment, and meniscal insufficiency may lead to formation or progression of a chondral defect. 6 These defects do not reliably heal and can progress to degenerative joint disease.7-9 Although articular cartilage is an aneural structure, these defects may cause pain and symptoms similar to patients scheduled to undergo knee osteotomy or arthroplasty. 10
A minority of these lesions require surgical treatment. However, because of poorly understood factors, some patient may develop pain and swelling with a diagnosis of a chondral defect and can be considered for operative treatment.11-16 The most durable treatment that provides the highest likelihood of return to high level activity with a symptomatic chondral defect remains unknown.11-16
The purpose of this study is to compare activity-based outcomes and rate of return-to-sport after articular cartilage surgery in the knee in prospective and retrospective comparative (i.e., level III evidence and higher) studies. The primary study hypothesis is that autologous chondrocyte implantation (ACI) and osteochondral autograft (OAT) provide superior activity-related outcomes when compared with microfracture. A secondary study hypothesis is that (a) no significant difference in rate of return-to-sport exists between all techniques at 2 years follow-up and (b) at longer follow-up, return-to-sport and performance in sport deteriorates following microfracture versus ACI or OAT.
Method
To address the study hypotheses, a systematic review of the literature was conducted. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed in performing this review. 17 The following databases were used: PubMed (MEDLINE), the Cochrane Central Register of Controlled Trials, CINAHL (Cumulative Index for Nursing and Allied Health Literature), and MDconsult. The search was conducted on August 1, 2012. The search period was from January 1, 1985 to August 1, 2012. Only abstracts for articles published in English with a minimum of 2 years of follow-up were reviewed. The electronic search strategy used was “(((cartilage OR articular cartilage OR chondrocyte OR chondrocytes OR osteoarticular OR mosaicplasty OR osteochondral OR osteochondritis dissecans OR chondral) AND (transplant OR transplants OR allograft OR transplantation OR autologous OR autograft OR implant OR implantation) AND (athlete OR athletes OR sport OR sports OR athletic OR “sport medicine” OR “athletic performance” OR “athletic injuries”) AND (“knee osteoarthritis” OR knee OR “knee joint” OR “knee injuries”)) OR (knee AND microfracture))”. For those that met inclusion and exclusion criteria full-text was obtained and reviewed. The reference lists for each included article were manually cross-checked to avoid missed articles. Those studies that potentially met inclusion criteria were discussed among the authors to reach a consensus decision on inclusion/exclusion.
Studies were included if they reported clinical outcomes of cartilage repair or restoration procedures in the knee such as microfracture, ACI, OAT, or osteochondral allograft; if they provided level of evidence of I, II, or III (according to the Oxford Centre for Evidence-Based Medicine);18 if they reported clinical outcomes with a minimum of 2 years follow-up; and if they reported activity-based outcomes, specifically the Knee Injury and Osteoarthritis Outcome Score (KOOS) Sports and Recreation subscore, 19 the Tegner Score, 20 the Cincinnati Knee scores, 21 the International Knee Documentation Committee (IKDC) subjective score, 22 the Marx activity score, 23 and/or the rate of return-to-sport.11,14,24,25 Studies were excluded if written in languages other than English, constituted level IV or V evidence, provided less than 2 years follow-up, were published prior to 1985, reported outcomes in joints other than the knee, did not report clinical outcomes, did not report outcomes of a cartilage repair or restoration procedure, or did not report activity-based outcome scores. In cases where inclusion/exclusion could not be determined from the abstract alone, full-text was obtained.
Study methodological quality was assessed via the Modified Coleman Methodology Score (MCMS). 26 Applicable to both randomized and nonrandomized orthopedic trials, this 15-item instrument has a scaled potential score ranging from 0 to 100. Scores from 85 to 100 are excellent, 70 to 84 are good, 55 to 69 are fair, and less than 55 are poor.
Statistical Analyses
All analyses were conducted using Excel X (Microsoft, Redmond, WA) and SPSS 16 (IBM, Armonk, NY). Data were extracted from sources in their original form and then standardized to arithmetic means and standard deviations as a measure of variance. If variance or standard deviation were not given, it was calculated from standard error or 95% confidence intervals (CIs). All means were then weighted for sample size. Descriptive statistics were calculated for each study and parameter/variable analyzed. Continuous variable data was reported as mean ± standard deviation (weighted means where applicable). Categorical data were reported as frequencies with percentages. For all statistical analysis, P < 0.05 was deemed statistically significant. Mean and standard deviation subject, surgical, and study data were compared using 2-sample and 2-proportion Z-test calculators with α = 0.05. These tests allow comparison with a difference in sample sizes between the compared groups.
Results
General Cohort Characteristics
The search yielded 877 citations after the removal of duplicates. These abstracts were then considered for possible inclusion. After application of inclusion and exclusion criteria, 25 studies were identified for inclusion. Nine of these studies11-14,24,25,27-29 reported on 4 populations and thus 5 of these studies were excluded.11,14,24,28,29 In these cases, the study most recently published, providing the highest level of evidence and reporting on the largest number of subjects was included. Overall, data were extracted from 20 studies ( Table 1 ). Twenty studies were included (1,375 patients) for further analysis ( Tables 2 and 3 ). Nine studies were randomized controlled trials and 11 studies compared a minimum of 2 different surgical procedures. Seventy percent of studies either reported the presence of a financial conflict of interest or failed to report its presence or absence. Overall MCMS was 49.4 ± 10.5 (poor rating). High scoring individual items on MCMS were length of follow-up, treatment description, group comparability, and sample size. Poor scoring items on MCMS were blinding, clinical effect size measurement, and number needed-to-treat analysis. Overall, subjects were young (mean age = 33 years) males (65%) with a preoperative symptom duration of more than 3 years and one prior surgery on the index knee. There were no significant differences in age between microfracture, ACI, and OAT cohorts (32.6 ± 4.5, 32.9 ± 4.1, and 29.9 ± 4.3, respectively, P > 0.05 for all comparisons). Twenty-three percent of subjects were professional or amateur competitive athletes. Most defects were located on the femoral condyles (81%) and were nearly 4 cm2 in surface area. The ACI cohort had a significantly larger mean defect size than the microfracture or OAT cohorts (4.33 ± 1.6, 3.34 ± 1.5, and 2.95 ± 0.44, respectively, Z = 3.25 and P = 0.001 for microfracture vs. ACI and Z = 2.8 and P = 0.005 for ACI vs. OAT). There was no significant difference in mean lesion size between microfracture and OAT cohorts (Z = 0.79, P = 0.43). All studies reported surgical indications of Outerbridge grade 3 or 4, International Cartilage Repair Society grade 3 or 4, or “full-thickness” chondral or osteochondral defects. ACI was the most common technique performed and analyzed (61%), whereas partial meniscectomy was the most common concomitant technique performed. Nearly all studies (90%) reported a detailed postoperative rehabilitation program, with use of CPM and a progression of weight bearing. Multiple clinical outcome scores were used throughout the studies ( Table 4 ). Return-to-sport outcomes were reported in only 5 studies ( Table 5 ). Mean subject follow-up was 3.7 years. Complication and reoperation rates were reported in 17 studies ( Table 6 ). Overall, the rate of reoperation was 25%, 21%, and 28% for ACI, microfracture, and OAT, respectively. Of all reoperations following ACI, microfracture, and OAT, 81%, 51%, and 48% were unplanned (usually because of pain and symptoms), respectively. Revision articular cartilage surgery following ACI, microfracture, and OAT comprised 12%, 29%, and 6% of all reoperations, respectively.
Summary of Included Studies.
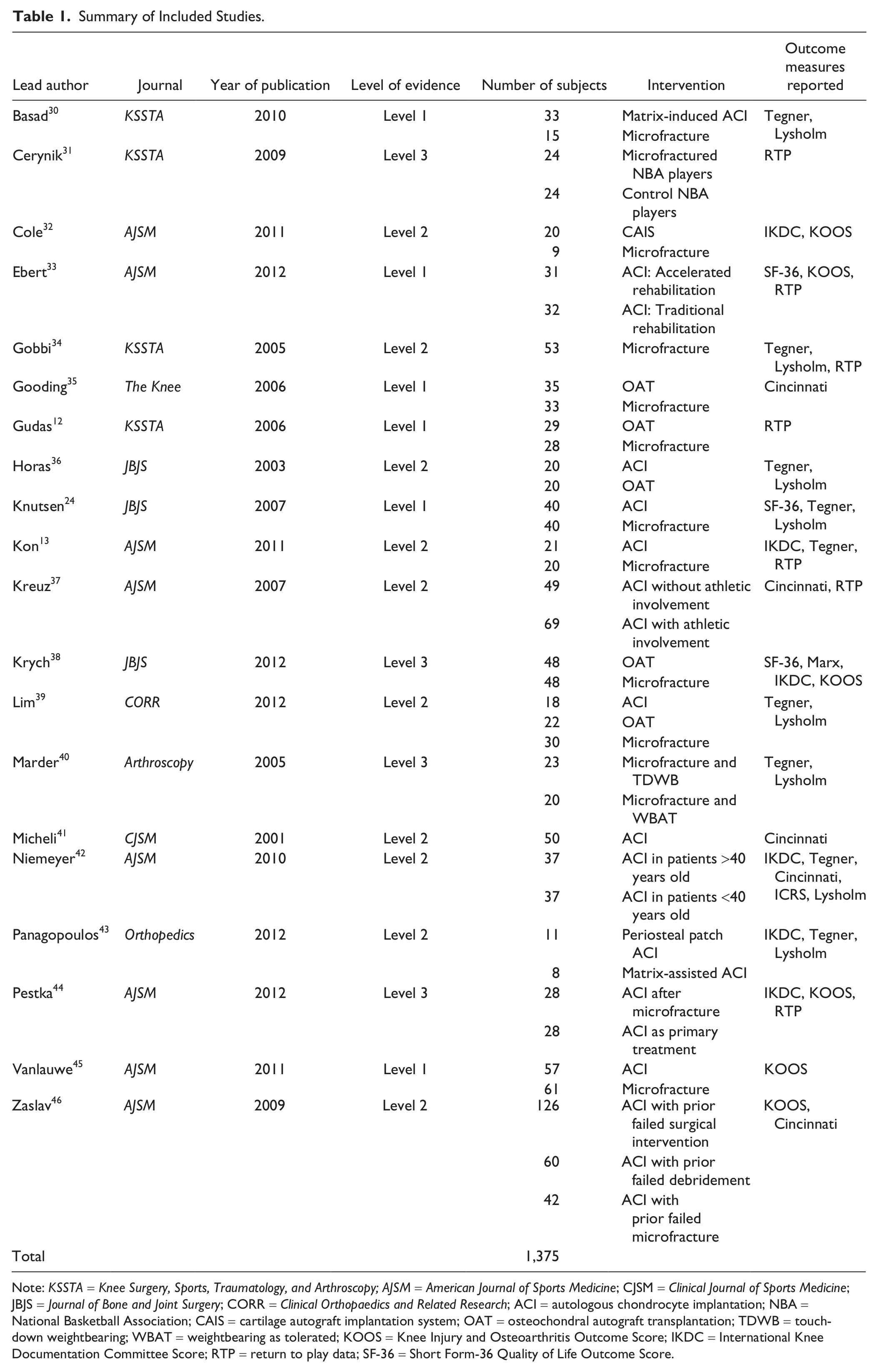
Note: KSSTA = Knee Surgery, Sports, Traumatology, and Arthroscopy; AJSM = American Journal of Sports Medicine; CJSM = Clinical Journal of Sports Medicine; JBJS = Journal of Bone and Joint Surgery; CORR = Clinical Orthopaedics and Related Research; ACI = autologous chondrocyte implantation; NBA = National Basketball Association; CAIS = cartilage autograft implantation system; OAT = osteochondral autograft transplantation; TDWB = touch-down weightbearing; WBAT = weightbearing as tolerated; KOOS = Knee Injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee Score; RTP = return to play data; SF-36 = Short Form-36 Quality of Life Outcome Score.
Pre-, Intra-, and Postoperative Details Extracted from Studies Analyzed.
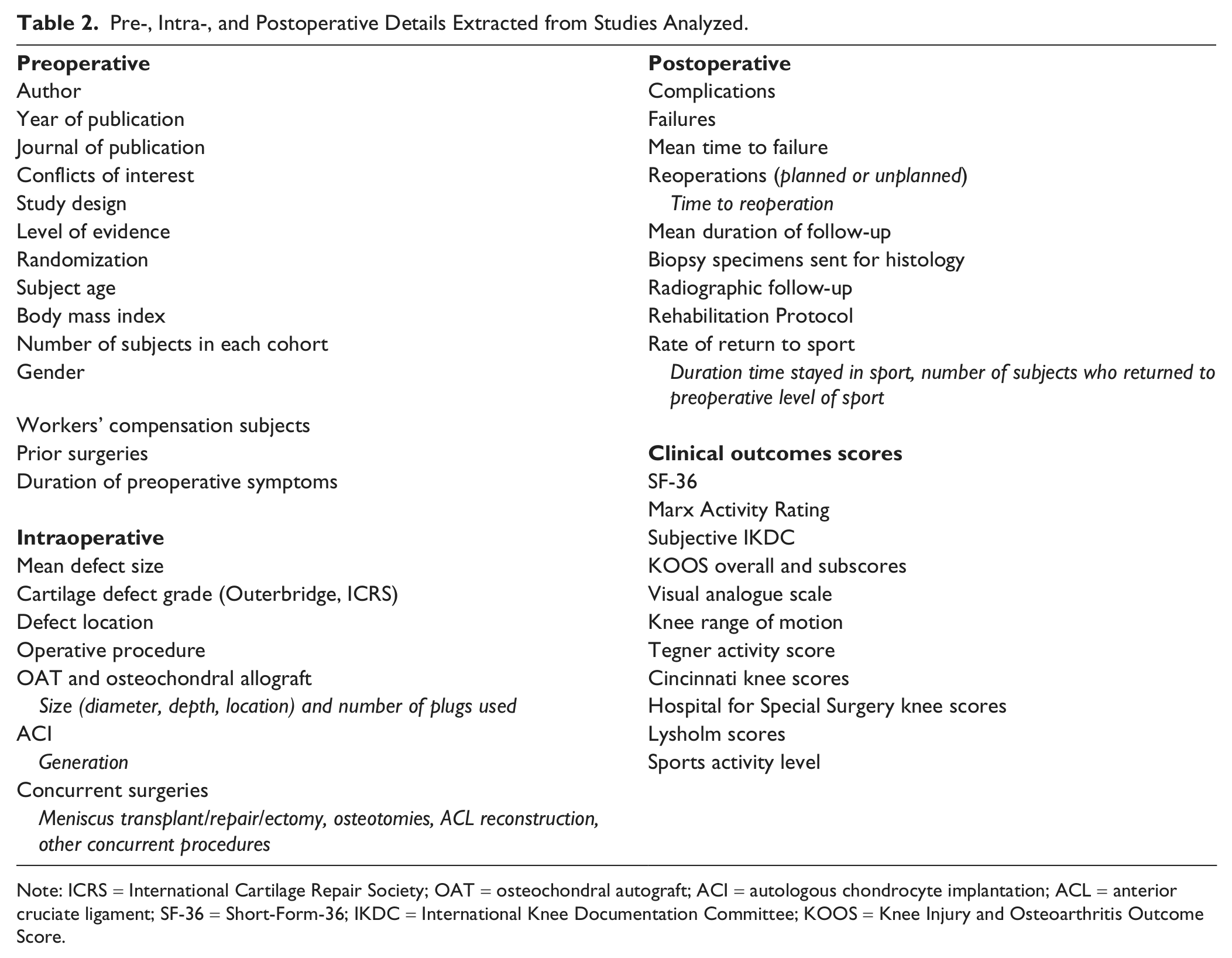
Note: ICRS = International Cartilage Repair Society; OAT = osteochondral autograft; ACI = autologous chondrocyte implantation; ACL = anterior cruciate ligament; SF-36 = Short-Form-36; IKDC = International Knee Documentation Committee; KOOS = Knee Injury and Osteoarthritis Outcome Score.
Patient and Defect Characteristics.
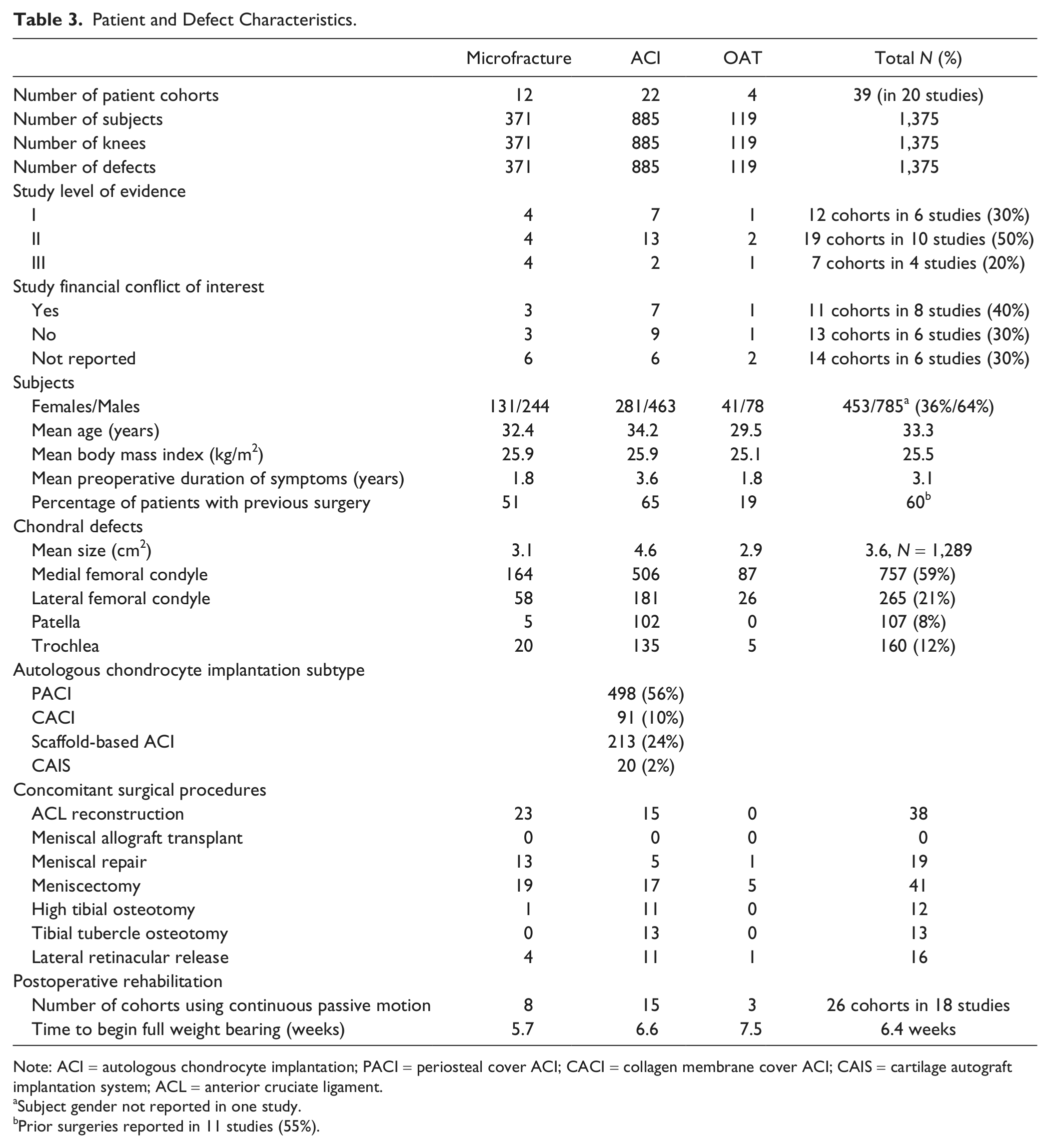
Note: ACI = autologous chondrocyte implantation; PACI = periosteal cover ACI; CACI = collagen membrane cover ACI; CAIS = cartilage autograft implantation system; ACL = anterior cruciate ligament.
Subject gender not reported in one study.
Prior surgeries reported in 11 studies (55%).
Clinical Outcomes.
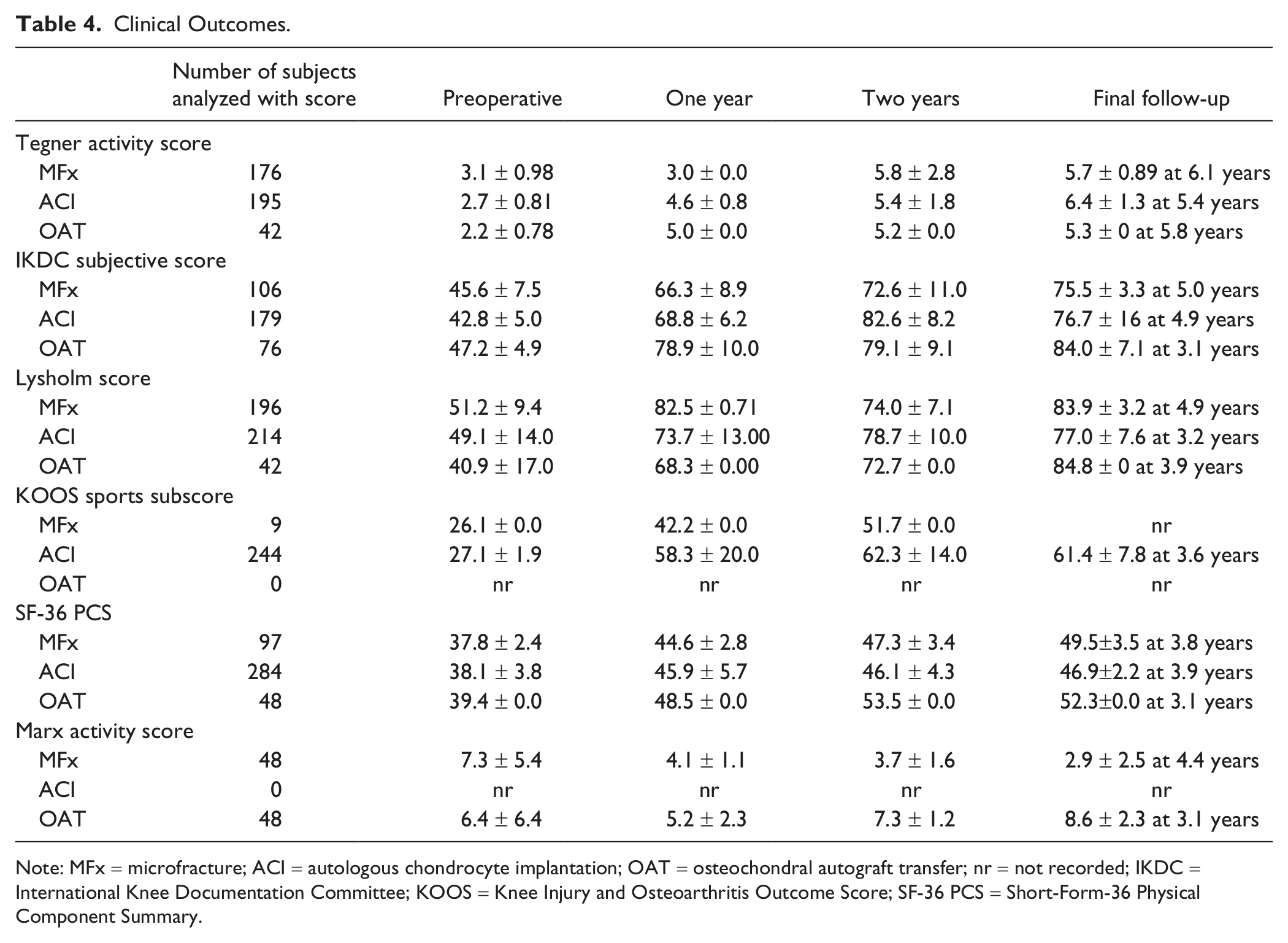
Note: MFx = microfracture; ACI = autologous chondrocyte implantation; OAT = osteochondral autograft transfer; nr = not recorded; IKDC = International Knee Documentation Committee; KOOS = Knee Injury and Osteoarthritis Outcome Score; SF-36 PCS = Short-Form-36 Physical Component Summary.
Results of Z-Test Statistical Comparisons.
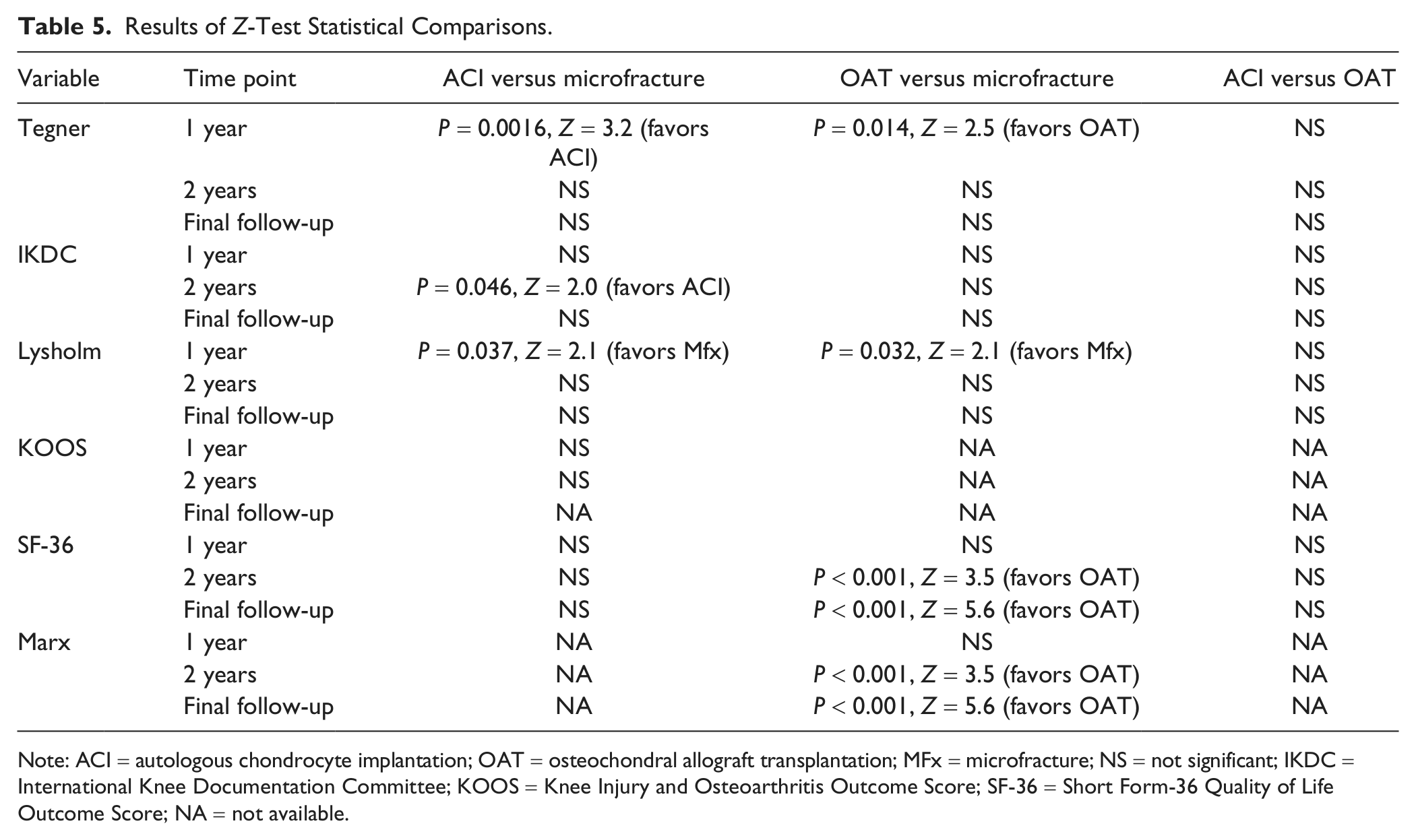
Note: ACI = autologous chondrocyte implantation; OAT = osteochondral allograft transplantation; MFx = microfracture; NS = not significant; IKDC = International Knee Documentation Committee; KOOS = Knee Injury and Osteoarthritis Outcome Score; SF-36 = Short Form-36 Quality of Life Outcome Score; NA = not available.
Complications and Reoperations After All Surgical Procedures. a .
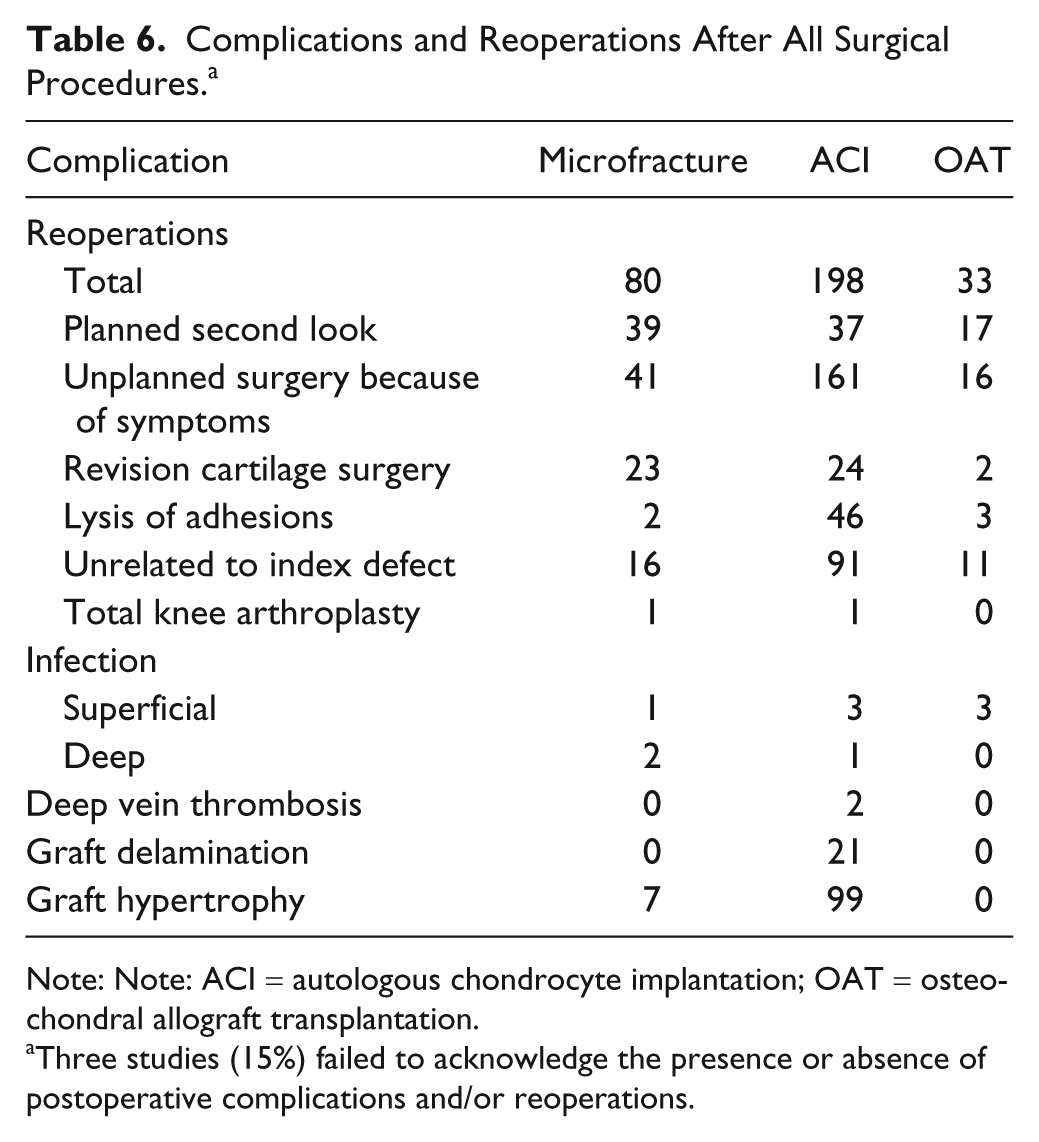
Note: Note: ACI = autologous chondrocyte implantation; OAT = osteochondral allograft transplantation.
Three studies (15%) failed to acknowledge the presence or absence of postoperative complications and/or reoperations.
Activity-Based Clinical Outcomes
Clinical outcomes were significantly improved (P < 0.05) at final follow-up versus preoperative values using all outcome measures (Tegner activity scores, IKDC, Lysholm, and SF-36 PCS [Physical Component Summary] scores, and KOOS Sports and Recreation subscores) for all 3 surgical techniques ( Table 4 ). Techniques were compared for those time points and outcomes where comparison was possible. The number of subjects, the means, and the standard deviations for these statistical comparisons are given in Table 4 . Results of these comparisons are given in Table 5 . When ACI and microfracture were compared significant advantages were found for ACI in Tegner scores at 1 year and IKDC scores at 2 years, whereas a significant advantage was found for microfracture in Lysholm scores at 1 year. When ACI and OAT were compared, significant advantages were found for OAT in Tegner scores at 1 year, SF-36 scores at 1 year and final follow-up, and for Marx scores at 2 years and final follow-up whereas a significant advantage was found for microfracture in Lysholm scores at 1 year. Overall, these results are heterogeneous but suggest that there may be advantages for ACI and OAT over microfracture at some time points in some clinical outcomes. When the amount of improvement in clinical scores was compared, significant advantages were found for Tegner scores (3.7 vs. 2.6 for ACI vs. microfracture, P = 0.023, Z = 2.3), Marx scores (2.2 vs. −4.4 for OAT vs. microfracture, P < 0.001), and Lysholm scores (43.9 vs. 27.9 for OAT vs. ACI, P = 0.04, Z = 2.1).
Several individual studies did identify significant differences in clinical outcomes between different techniques. However, only one study compared all 3 surgical techniques, demonstrating no significant differences (Lysholm and Tegner). 39 In a comparison of microfracture and OAT, the change in Marx activity score was significantly improved following OAT and significantly reduced following microfracture versus preoperatively, with a significant difference between the two at final follow-up. 38 No difference was demonstrated between the latter 2 groups in IKDC subjective and SF-36 PCS scores, suggesting that the Marx score may be a more sensitive measure of knee outcome differences than the IKDC or SF-36 score. In a separate study, a significant difference was identified at 1, 2, and 3 years follow-up using IKDC subjective score. 12 Five studies compared ACI and microfracture, with significantly better KOOS Sports subscores at 1 and 2 years, 32 Lysholm at 1 and 2 years, 30 IKDC at 1 year, 32 2 years, 32 and 7 years, 13 and Tegner at 1 and 2 years 30 following ACI. Only one study compared ACI and OAT, with significantly slower recovery (Lysholm score) following ACI at 6, 12, and 24 months. 36
Return-to-Sports Outcomes
Only 5 studies reported rates of return-to-sport and performance on return-to-sport ( Table 5 ). These studies demonstrate a significantly earlier return to competition with microfracture (range 6.5-8 months)12,13,31 versus ACI (12.5 months) 13 (P < 0.01), but deterioration of IKDC and Tegner scores beyond 2 years follow-up following microfracture (P < 0.05) whereas ACI outcomes remain stable. 13 The overall rate of return to professional soccer was not significantly different between ACI (86%) and microfracture (80%). 13 There was, however, a significant difference in rate of return to competitive soccer and basketball favoring OAT (93%) versus microfracture (52%; P < 0.05). 12 Both rate of return to and performance on return to NBA basketball following microfracture was decreased—21% of players never returned to another game and player efficiency and power ratings significantly decreased. 31 Furthermore, although Tegner activity score significantly improved at 2 years follow-up following microfracture in professional and amateur athletes, in one clinical study it significantly deteriorated from 2 years to final follow-up with only 55% of athletes competing in strenuous sports activity at 6 years (vs. 80% at 2 years). 34 In the overall study population no deterioration of outcomes was observed between short- and mid-term follow-up ( Table 4 ).
Discussion
The purpose of this systematic review was to compare activity-based outcomes and rate of return-to-sport after articular cartilage surgery in the knee in prospective and retrospective comparative (i.e., level III and higher) studies. The study authors hypothesized that cartilage restoration using ACI or OAT provides superior activity-related outcomes when compared with microfracture. Furthermore, it was hypothesized that (a) no significant difference in rate of return-to-sport exists between all techniques at 2 years follow-up and (b) at longer follow-up, return-to-sport and performance in sport deteriorates following microfracture versus ACI or OAT. The authors’ hypotheses were partially confirmed. Analysis of activity-based outcomes demonstrated significantly better outcomes using cartilage restoration techniques of ACI and OAT versus microfracture at some time points despite larger lesional size for the ACI technique, but results were heterogeneous.13,30,32,36 Only 5 studies reported return-to-sport outcomes. Return-to-sport is fastest following microfracture. Although several individual studies showed deterioration of performance and rate of return-to-sport both before and after 2 years after microfracture,12,13,31 the overall study population did not demonstrate deterioration of microfracture outcomes between short- and mid-term follow-up. Overall, reoperation rates were similar at 25%, 21%, and 28% for ACI, microfracture, and OAT, respectively. Of reoperations, a higher proportion of those following ACI were unplanned at 81% as compared with 51% and 48% following microfracture and OAT, with the majority of ACI reoperations being performed for graft delamination or hypertrophy.
Our objective in this study was to examine activity related outcomes. However, heterogeneity between outcome scores for the same patient populations likely reflects that these outcome measures are examining different facets of the same clinical picture. Tegner, Marx, and return-to-play rates may more closely reflect actual activity rates, whereas Lysholm, IKDC, and SF-36 scores likely provide only a coarse measure of athletic activity or function. The aspect of the clinical picture provided by each outcome measure should influence interpretation of differences or lack thereof between clinical groups in these outcome measures.
Our study has several limitations. First, by design, this analysis compares cohort studies performed by different authors. Heterogeneity between these studies limits interpretation. As with any systematic review, the quality of the original data limits the quality of our findings and the ability to draw clinical recommendations from them. Several biases within the underlying studies could potentially limit our findings, including selection bias, performance bias, transfer bias, detection bias, nonresponder bias, publication bias, and study design biases. The relatively small sample size for each individual study also limits our conclusions. Heterogeneity between studies includes surgical technique, postoperative rehabilitation, ACI technique (with regards to whether a periosteal or collagen patch was used, whether characterized chondrocytes were used, and the generation of procedure used), OAT plug size, subject demographics, and outcome measures. In addition, at the present time only short- and mid-term follow-up is available, which limits our ability to comment on long-term outcomes, particularly limiting especially considering that one of the potential goals of cartilage restoration is to prevent or slow progression to osteoarthritis. A further selection bias may be introduced by limiting inclusion to only those studies that report on activity-based outcome measures. Limiting inclusion to level III and higher studies introduces a further selection bias and may potentially exclude series demonstrating high rates of return-to-play at mid-term follow-up. 16 A further limitation of our study is that not all included subjects were athletes—indeed the minority of our subjects were athletes (23%) and thus our findings may not apply to a strictly athletic population but merely to an active one. One potential limitation of our study is that prospective cohort studies with subgroups where considered as level II evidence, while some authors would argue this constitutes level IV evidence.46,47 However, the original journals that published these studies had labeled them as such and in the current Centre for Evidence-Based Medicine guidelines prospective cohort studies are designated as level II evidence.46,47 One further limitation is the lack of a power analysis to guide interpretation of nonsignificant differences, which could represent type II error. In addition, the outcomes reported by each of the source studies were often secondary and not primary outcomes and thus each of the individual studies could have been underpowered, further increasing the likelihood of type II error.
Chondral defects are common, especially in active populations. 48 These lesions may cause pain. 10 Although the natural history remains unknown, a variety of surgical treatments have been proposed to improve pain and function in symptomatic patients.11-16 Although many patients include return to activity as a primary reason for seeking treatment, the ability of surgical reparative and restorative cartilage techniques to return patients to activity has been questioned.11-16 Surgical decision making in the active patient is a complex, multifactorial problem. In the athlete, these decisions become even more complex as contracts and scholarships, in addition to the athlete’s desires (and those of family, coaches, trainers, agents, and media), may limit the amount of time for recovery and rehabilitation out of sport. Long-term outcomes may be less relevant to some patients, as their entire goal is to return to activity as expeditiously as possible, without pain and with improved performance. As a result, in this review we selected activity-based outcome measures as those most pertinent to this patient population.
Each of the currently available surgical techniques has possible advantages and disadvantages. Advantages of the microfracture technique include rapid return-to-play12,13,31 and an ability to perform the technique in a single arthroscopic procedure. 16 Advantages of the ACI technique include improved the ability to cover larger lesions, 32 whereas disadvantages include the need for 2 procedures, a longer rehabilitation period, and the expense of the procedure. 13 Advantages of the OAT technique include ability to address defects in the subchondral bone and replacement with hyaline cartilage, 36 whereas disadvantages include donor site morbidity and the limited availability of donor cartilage, limiting application to larger lesions.49-51 The optimal treatment thus depends on matching these advantages and disadvantages with the characteristics of the lesion and the characteristics of the patient.
Although no level III or higher evidence exists to address osteochondral allograft procedures, a recent level IV study has been performed addressing athletes specifically confirming return-to-play rates of 88%, with 79% at their preinjury level. 52 Additional higher level studies will be necessary to determine the role for this procedure in the treatment of chondral defects in active patients.
Conclusion
ACI and OAT may have some benefits over microfracture, although return-to-sport is fastest following microfracture. Heterogeneity in technique, outcome measures, and patient populations hampers systematic comparison within the current literature.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study does not require institutional review board approval.