
Abstract
Objective
The aim of this study was to evaluate the factors that can affect long-term results of arthroscopic resection of medial synovial plica of the knee.
Design
A total of 52 knees in 50 consecutive patients with medial plica syndrome (MPS) were enrolled to prospective study. Preoperatively the age, gender, level of activity, symptoms’ duration, Lysholm knee scoring scale (LKSS), Q angle, range of motion (ROM), and quadriceps output torque (QOT) were recorded. The plica was then arthroscopically excised while plica morphological type and cartilage lesions (International Cartilage Repair Society [ICRS] classification) were registered. The postoperative evaluation was done after 1 month, 3 months, 6 months, 3 years, and 10 years. The final assessment after 10 years covered LKSS, ROM, QOT, and was enriched with functional tests: the single leg squat test (SLS), the modified Ober test (MO), and the manual palpation of the vastus medialis obliquus (VMO).
Results
The mean LKSS increased from 52 (15-85, SD 16.479) preoperative to 80 (48-100, SD 15.711) at final follow-up examination. A significant negative correlation was found between LKSS and the patients’ age. Cartilage lesions higher than ICRS 1 significantly decreased the final LKSS. Results were significantly better in the subgroups with normal outcome of functional tests.
Conclusions
Clinical results of arthroscopic plica resection are better in patients without coexisting cartilage lesions. Poor neuromuscular control may contribute to abnormal patella tracking, leading to both medial plica irritation and further cartilage deterioration.
Introduction
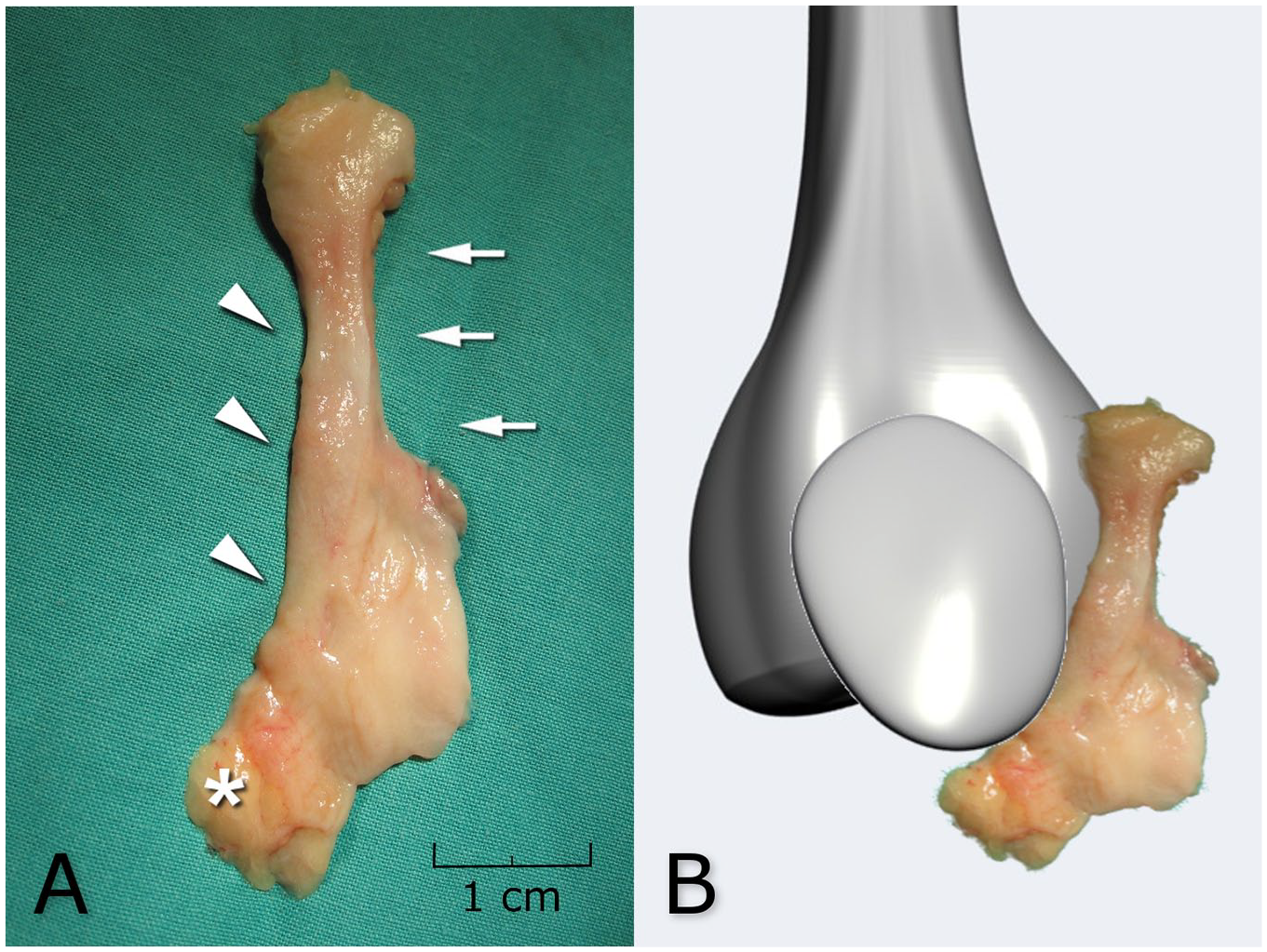
A remnant of the embryological development of the knee, the synovial medial plica is formed from the medial mesenchymal tissue. 1 It can become irritated by a single trauma or repetitive microtraumas caused by functional disorders of the patellofemoral joint (PFJ), leading to a typical pattern of symptoms, known as medial plica syndrome (MPS) with subsequent cartilage injuries. Thickened medial plica is found more often in patients suffering from anterior knee pain (AKP). Nevertheless, it remains unclear which of the above conditions is primary. 2 While the medial plica enters Hoffa’s pad distally, it proximally fades into the medial synovium at the level of the vastus medialis obliquus (VMO) insertion ( Fig. 1 ). The VMO is currently believed to be the main active PFJ stabilizer. 3 VMO distal insertion covers the proximal border of the main passive patella stabilizer, that is, the medial patellofemoral ligament (MPFL). It was proved that the VMO function in patients with AKP is impaired. 4 The exact role of medial plica in PFJ biomechanics and cartilage lesions remains unclear.
(
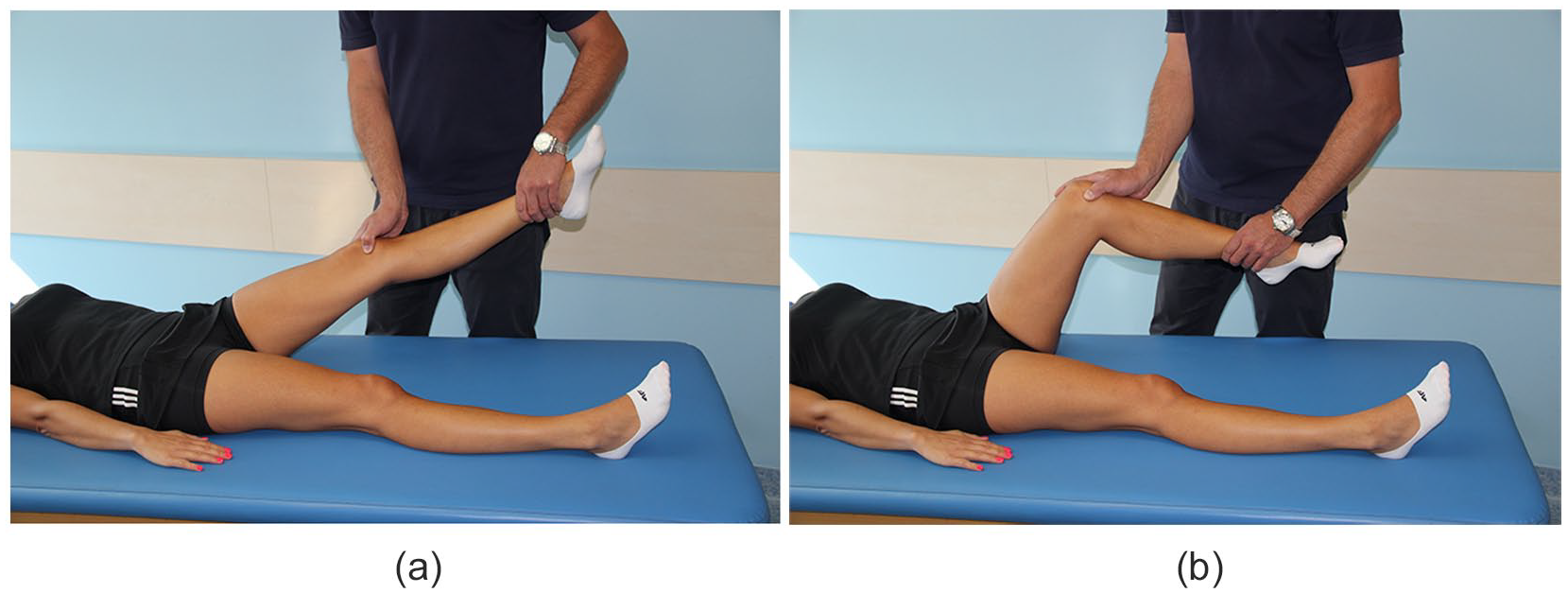
The diagnosis of MPS is based on nonspecific symptoms of intermittent, dull, aching pain in the area medial to the patella above the joint line and in the superomedial patellar area. 5 Kim et al. described an additional clinical feature. During their mediopatellar plica (MPP) test, manual force is applied to the inferomedial portion of the patellofemoral joint, after which the knee is flexed to 90°. The test is defined to be positive when the patient experiences pain with the knee in extension and the pain is eliminated or reduced with the knee in flexion ( Fig. 2a and b ). This test has shown high sensitivity and specificity for medial plica syndrome (89.5% and 88.7%, respectively, with diagnostic accuracy at 89.0%). 6
(
Conservative treatment in the initial phase of MPS should be considered, especially in younger patients. However, if the medial plica is catching over the medial femoral condyle, it may cause cartilage damage in the PFJ, which is an undeniable indication for arthroscopic treatment. 7
Amatuzzi described a physiotherapy protocol aimed at regaining the flexibility of tight knee flexors and concluded that exercises can play an important role in the treatment of pathological synovial plica. If physiotherapy is unsuccessful, then arthroscopic resection of the irritated plica becomes a treatment of choice. 8
The aim of this study was to evaluate the factors that can affect long-term results after medial plica arthroscopic resection.
Methods
Patient Selection
A total of 57 knees in 55 consecutive patients with clinical symptoms of medial plica were operated between 2005 and 2007 by 1 surgeon. The patients’ mean age was 18.3 (range 13-37) years on enrollment, while gender distribution was 36 women to 14 men. Five patients were excluded due to concomitant pathologies found during primary arthroscopy ( Table 1 ).
Excluded Cases.
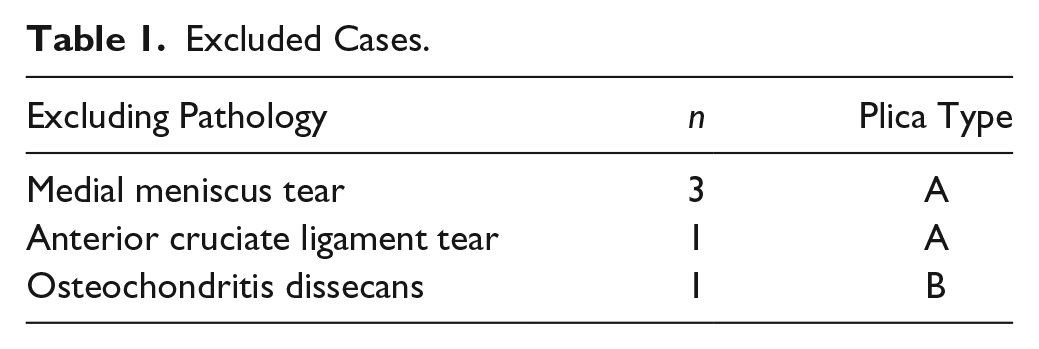
The inclusion criteria were medial plica suspicion established on typical symptoms, a positive MPP test, and a dynamic ultrasound examination, 9 with history of no improvement after minimum six months of conservative treatment. The exclusion criteria were a previous knee surgery, evidence of osteoarthrosis on the X-ray in 3 projections (anteroposterior, lateral, and Merchant view), the presence of intraarticular pathology (i.e., cartilage lesion) that was not associated directly with medial plica presence found during surgery, and genetic connective tissue disorders, such as Ehlers-Danlos syndrome, Marfan syndrome, and general joint hypermobility syndrome.
The study was approved by the local university Bioethics Committee, approval number KB/338/2005. All subjects gave informed consent.
Patients Flow
Of 50 subjects (52 knees) initially included into the study, 6 unilaterally operated patients were lost at the early stage as they refused to come to control check-ups. Three years postoperatively, partial data from 31 patients (32 knees) were collected by means of a postal questionnaire. Additional 2 participants were excluded from the final follow-up data analysis due to secondary surgery a few years after inclusion (one had anterior cruciate ligament [ACL] reconstruction and the other underwent meniscus tear treatment). Detailed patients’ flow is presented in Figure 3 . The final follow-up after 10 years covered 38 knees in 36 patients. The mean follow-up period of the statistically analyzed group was 123 (range 117-135) months. Both patients who were operated bilaterally were men.
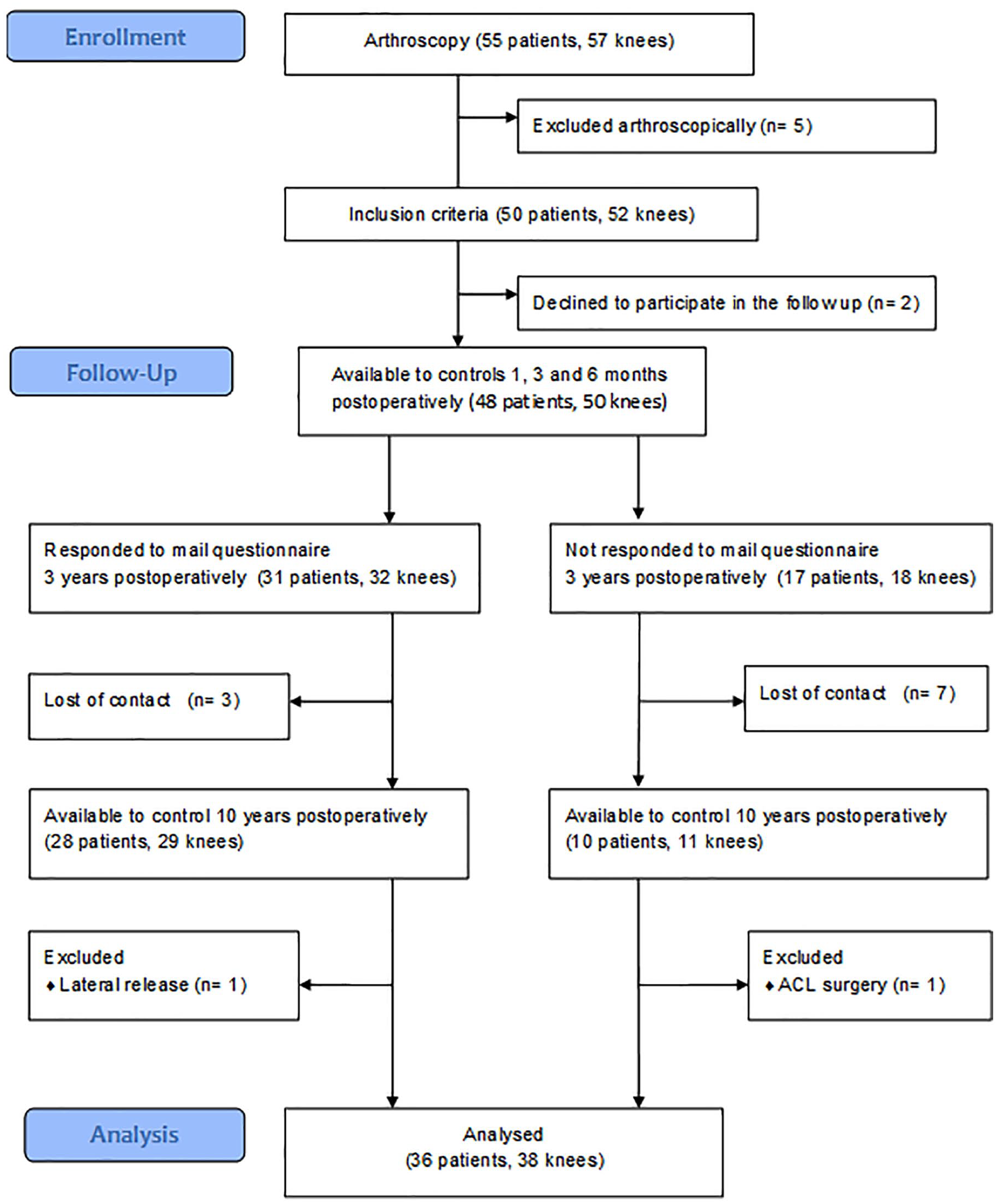
Flowchart illustrating the flow of patients through the study.
Patient Preoperative Assessment
The age, gender, sports activity, the period from the onset of symptoms until surgery, the Lysholm knee scoring scale (LKSS), Q angle measurement, 10 the range of motion and knee extension, and the maximum voluntary isometric contraction (MVIC) were recorded preoperatively. Force was measured using a chair dynamometer with both the knee and the hip locked at 90°. The MVIC was subsequently normalized to the patient’s weight to achieve the quadriceps output torque (QOT).11,12
Surgical Treatment
A standard 30° 5.6-mm arthroscope was inserted through standard arthroscopic portals. The plica position and possible impingement were observed during knee motion and checked with the arthroscopic probe. If a diagnosis other than plica syndrome was established, an appropriate procedure was performed. The plica was excised on the contact zone with the patella and the medial femoral condyle. A motorized shaver with suction was used (TPS 12K; Stryker Endoscopy, San Jose, CA). Cartilage was assessed by probe palpation and arthroscopic evaluation while coexisting cartilage degeneration was registered in line with the International Cartilage Repair Society (ICRS) classification.
13
The plicae were classified according to Sakakibara classification (
Figs. 4
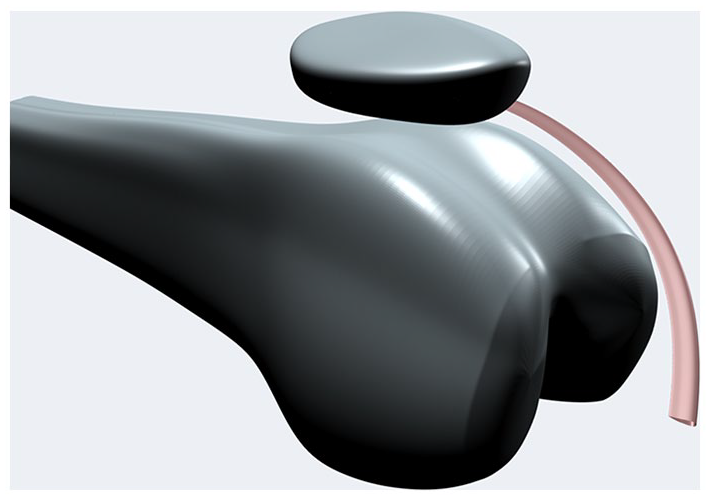
Visualization of plica type A; chord-like elevation of the synovium.
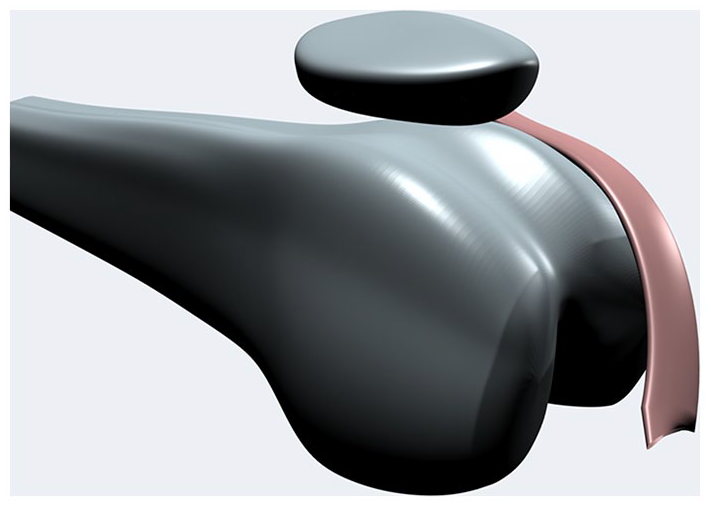
Visualization of plica type B; shelf partially covering medial femoral condyle.
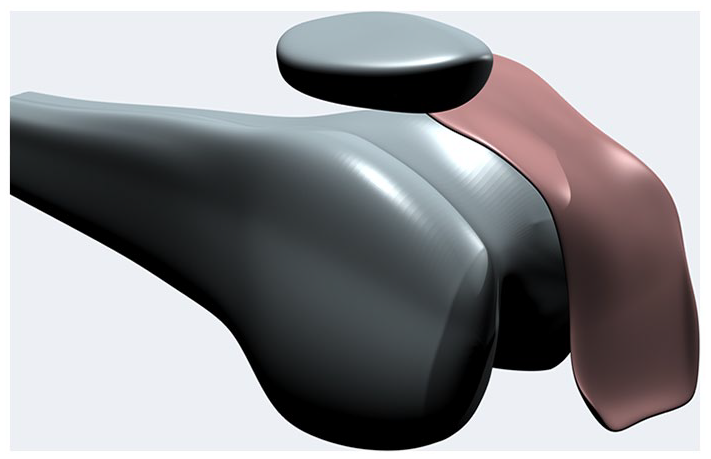
Visualization of plica type C; wide synovial band covering medial femoral condyle.
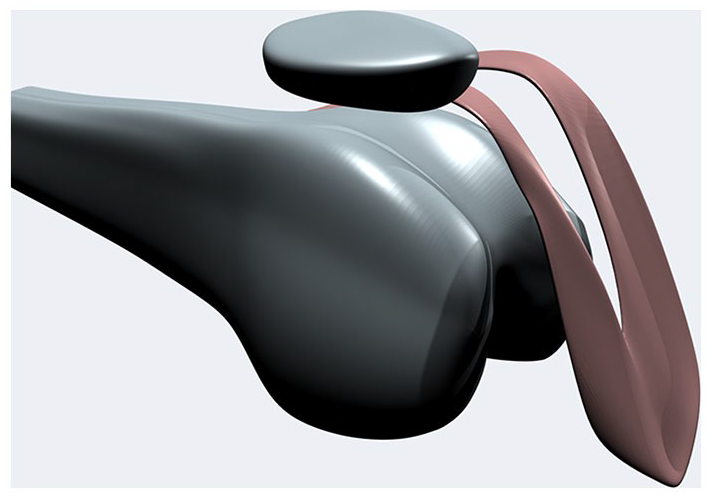
Visualization of plica type D; fenestrated band over medial femoral condyle.
Outcomes Assessment
The early postoperative evaluation (after 1, 3, and 6 months) consisted of LKSS as well as the range of motion and QOT measurements. Three years postoperative partial data from 31 patients (32 knees) were collected by means of a postal questionnaire in order to calculate LKSS.
The final assessment after at least 10 years was based on the initial protocol but—as our awareness of functional disorders of the PFJ increased—the evaluation was enriched with functional tests. The single leg squat (SLS) test, 15 the modified Ober (MO) test, and the manual palpation of the VMO were added at this stage.
The MO test was performed in line with original Kendall’s technique 16 with the patient side-lying with the underneath leg flexed at the hip and the knee to flatten the low back. The patient’s pelvis was manually stabilized by the examiner with the lateral trunk in contact with the table. The tested leg had the knee in extension and neutral hip rotation. The test was regarded negative (normal) if the leg dropped at least 10° below the horizontal plane. The MO test was found to be positive if the leg failed to drop below the horizontal plane.
The SLS test was done following the Ugalde protocol 15 previously described by Sciatica and Kibler. 17 The patient was asked to place their hands on their hips, stand on one limb and flex the opposing limb to 90°. Then, they were instructed to perform a partial single leg squat to 30° of knee flexion. Any arms flailing, Trendelenburg or collapse of the supporting knee into the valgus was noted as an abnormal response. We defined a positive SLS test if any of the above-described abnormal responses occurred during examination.
The VMO palpation was performed with the knee near extension in supine semisitting position. The examiner placed his finger just superior and medial to the patella. The patient was asked to extend the knee. The movement of the patella was observed due to rectus femoris activation. If instant contraction of the vastus medialis obliquus was felt, then VMO palpation was regarded as normal. If there was no activation at all or if the activation was delayed and hardly felt, then VMO palpation was regarded as weak.18,19
Statistical Evaluation
Variables were tested for normality by means of the Shapiro-Wilk test and for equal variances by Levene’s test. One-way analysis of variance, T test, Fisher’s exact test, chi-square test, and Pearson correlation coefficient were used for data analyses. All statistical calculations were performed using IBM SPSS Statistics v.25 (IBM Corp., Armonk, NY, USA). The charts were prepared with GraphPad Prism v.8.0.1 for Windows (GraphPad Software, La Jolla, CA, USA).
Results
A history of recreational sports activity at least once a week before the onset of symptoms was reported by 41 patients (82%). The activities included jogging (14 patients), team sports (14 persons), dancing (6 persons), martial arts (3 persons), aerobics (2 persons), and cycling (2 persons). Direct trauma as a trigger of pain was reported by 17 participants, whereas 8 persons indicated a twisting injury. The pain started with spontaneous locking of the knee in 6 patients. The remaining 19 subjects (38%) experienced a gradual increase in pain. The mean time from the onset of symptoms to surgery was 26 (range 6-60) months.
The arthroscopic distribution of plicae types according to the Sakakibara classification and concomitant cartilage lesions are presented in Table 2 . The most frequent plica was type C fold (60%), followed by type B (31%). Four knees showed type A fold and fenestrated plica was found only in one (type D). Only thicker type B and C plicas were associated with the presence of more severe (ICRS > 1) cartilage lesions. Statistical analysis did not show any significant correlation between the morphology of the plica and the extent of cartilage damage.
Distribution of Plicae Types.
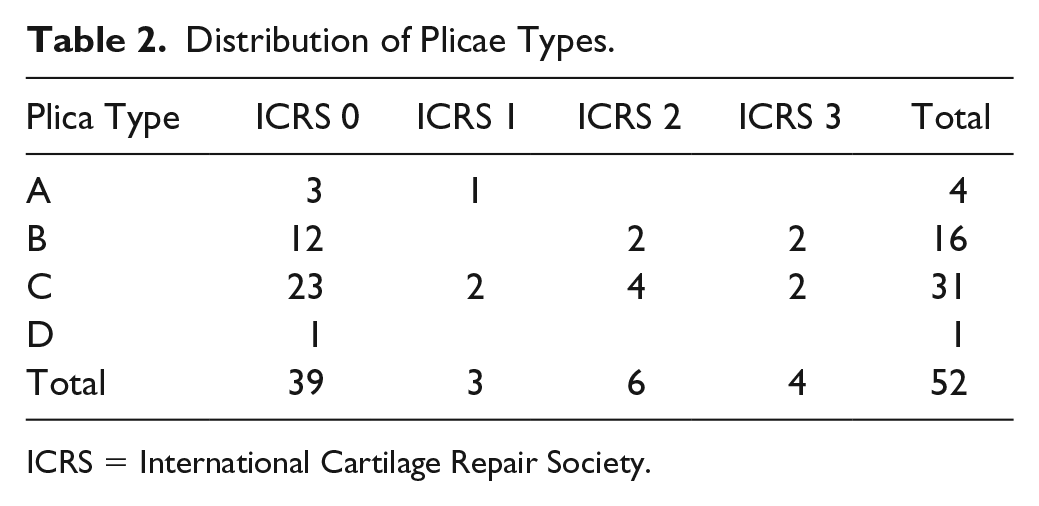
ICRS = International Cartilage Repair Society.
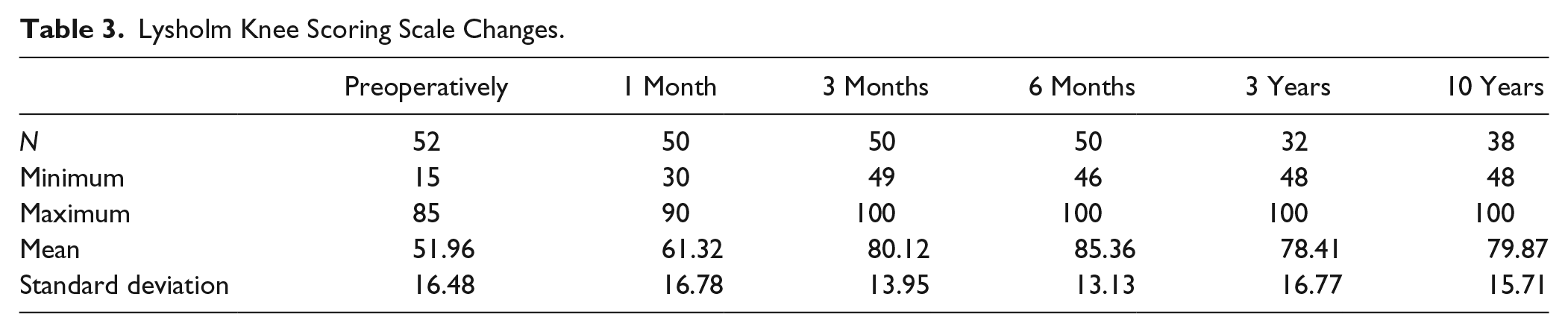
The mean value of LKSS increased significantly (P < 0.001) from 52 (range 15-85, SD 16.479) preoperative to 80 (range 48-100, SD 15.711) at final follow-up examination ( Table 3 ). A significant negative correlation was found between LKSS and the patients’ age. Males showed slightly better preoperative Lysholm scores (mean 54.63, SD 17.208 vs. 50.78, SD 16.25 in females) and comparably better final scores (mean 86.44, SD 11.886 vs. 77.83, SD 16.358 in females), but both differences were insignificant. There was no significant correlation between the outcome score and other numeric variables (Q angle and QOT, Table 4 ). Moreover, there were no significant differences in the QOT in the 10-year time span. There was no significant difference in preoperative and final LKSS between different plica types. The duration of symptoms had no significant influence on the LKSS score.
Lysholm Knee Scoring Scale Changes.
Correlations of Variables.
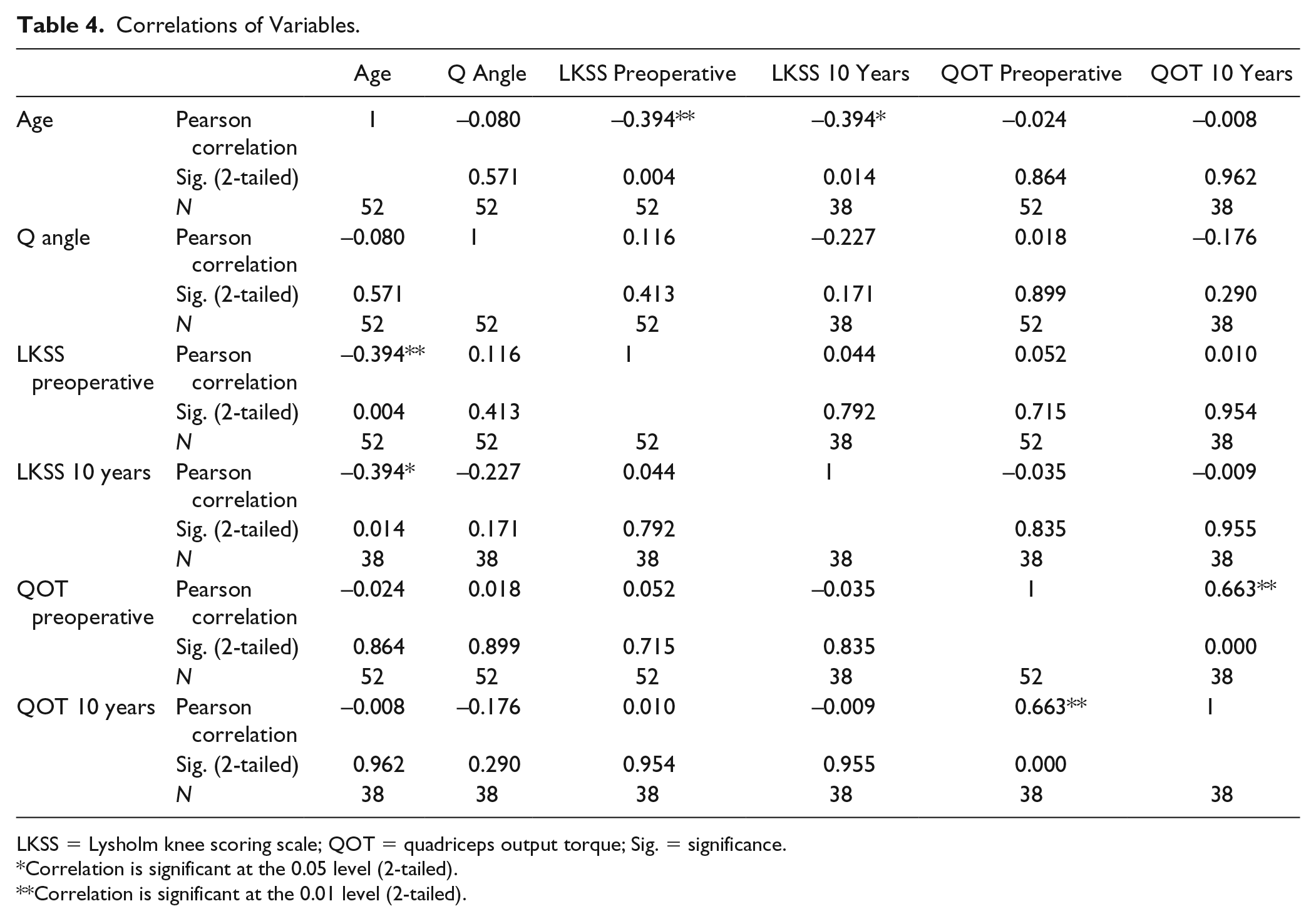
LKSS = Lysholm knee scoring scale; QOT = quadriceps output torque; Sig. = significance.
Correlation is significant at the 0.05 level (2-tailed).
Correlation is significant at the 0.01 level (2-tailed).
Coexisting cartilage lesions higher than ICRS 1 significantly decreased the final LKSS (P < 0.01, Table 5 , Fig. 8 ).
Relation between Lysholm Knee Scale Scoring (LKSS) and Coexisting Cartilage Lesions.
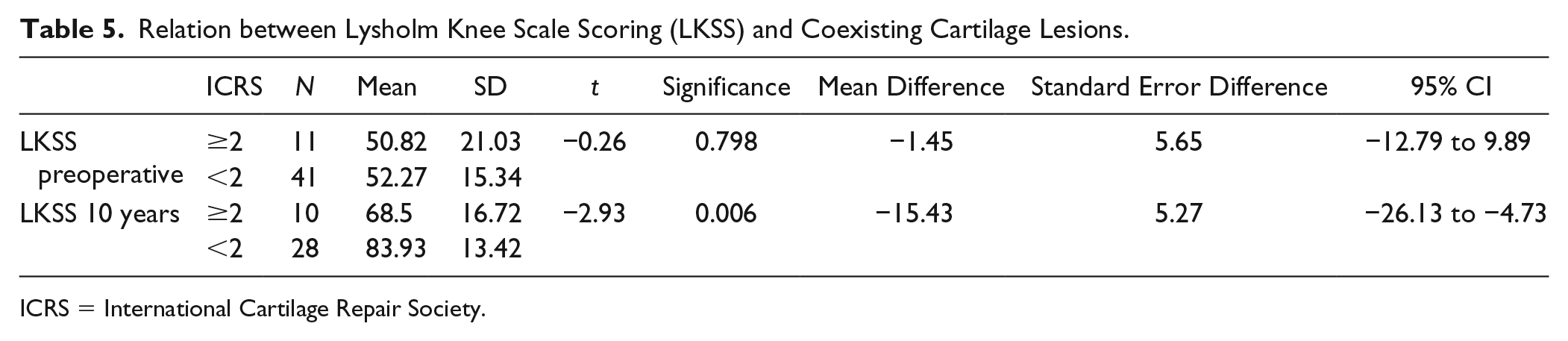
ICRS = International Cartilage Repair Society.
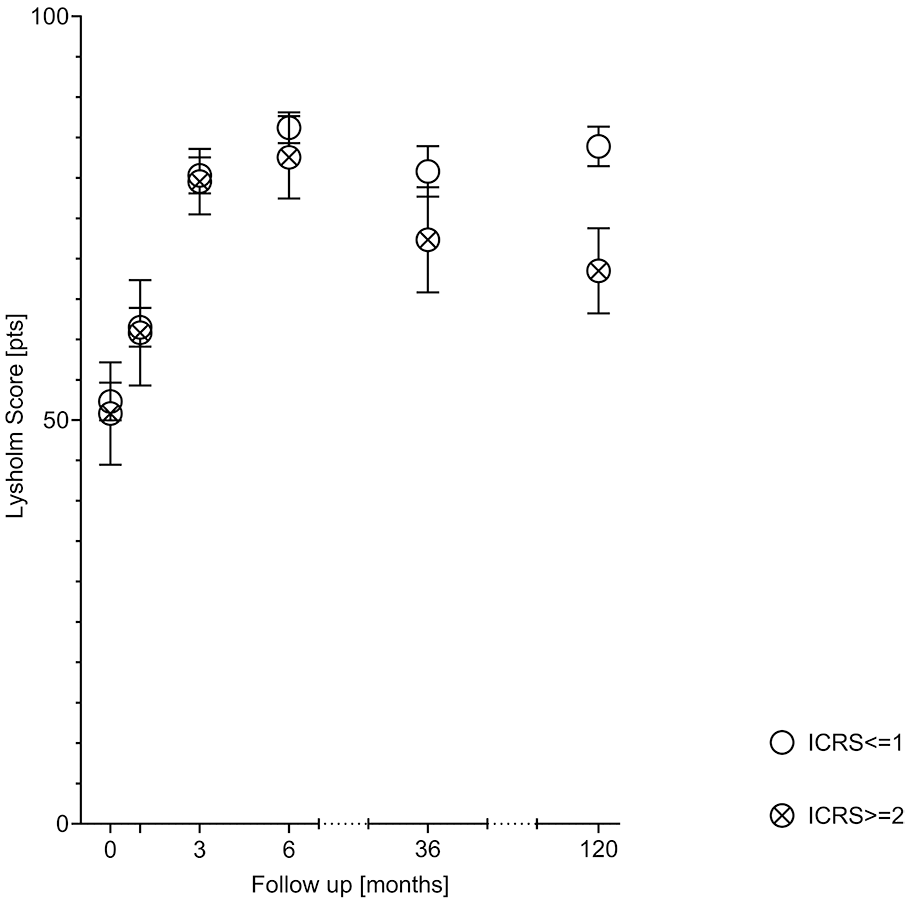
Changes of the Lysholm knee scoring scale in patients with cartilage lesions higher than International Cartilage Repair Society (ICRS) 1 and those with the cartilage under the plica in good condition. Error bars show the standard error.
Preoperative LKSS counts were not correlated with the outcomes of the functional tests checked 10 years later. Final results in LKSS were significantly better in the subgroups without abnormal functional tests. The strongest dependency was presented for VMO palpation and the SLS test (P < 0.001, Table 6 ). Positive MO test was more frequent in females than males (12/29 in females vs. 1/9 in males; P = 0.095). VMO was weak in 2 of 9 males and 15 of 29 females and SLS test was positive in 3 of 9 males and 17 of 29 females. In both VMO and SLS tests, this gender dependency was insignificant.
Comparison of Preoperative and Final Lysholm Knee Scale Scorings (LKSS) in Relation to Functional Tests’ Results on Final Visit.
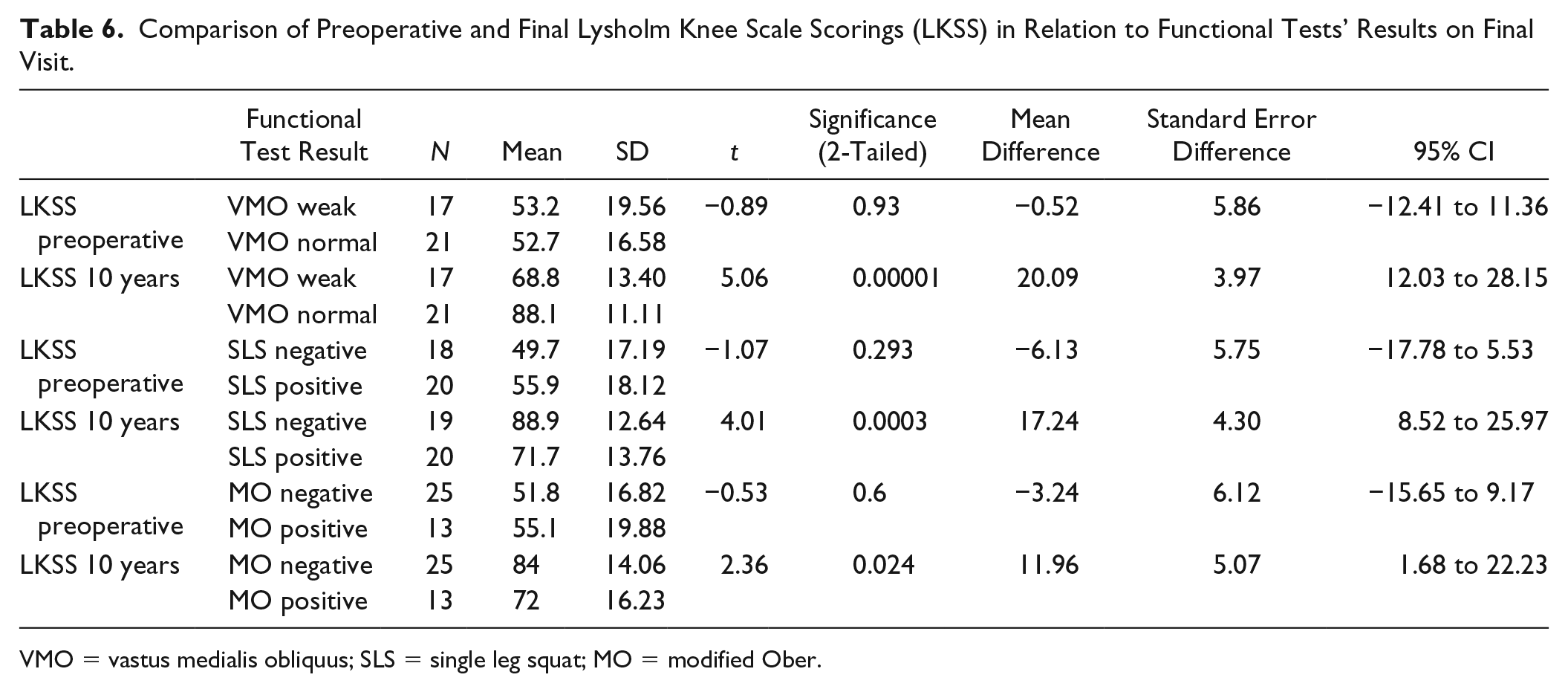
VMO = vastus medialis obliquus; SLS = single leg squat; MO = modified Ober.
No postoperative complications were detected during the follow-up period. All patients were mobilized on the first postoperative day and instructed on the same physiotherapy protocol, including active quadriceps exercises, VMO activation and proprioception. The mean length of hospital stay was 3 (range 2-5) days. Immediate up to full weightbearing was allowed as tolerated, crutches were used from 1 to 21 days (10 days on average).
Discussion
Plica studies with variable methodology and different results could be found in the literature ( Table 7 ). To the best of our knowledge, the present study has the longest follow-up and the worst outcome.
Plica Studies Found in the Literature in Relation to the Present Study.
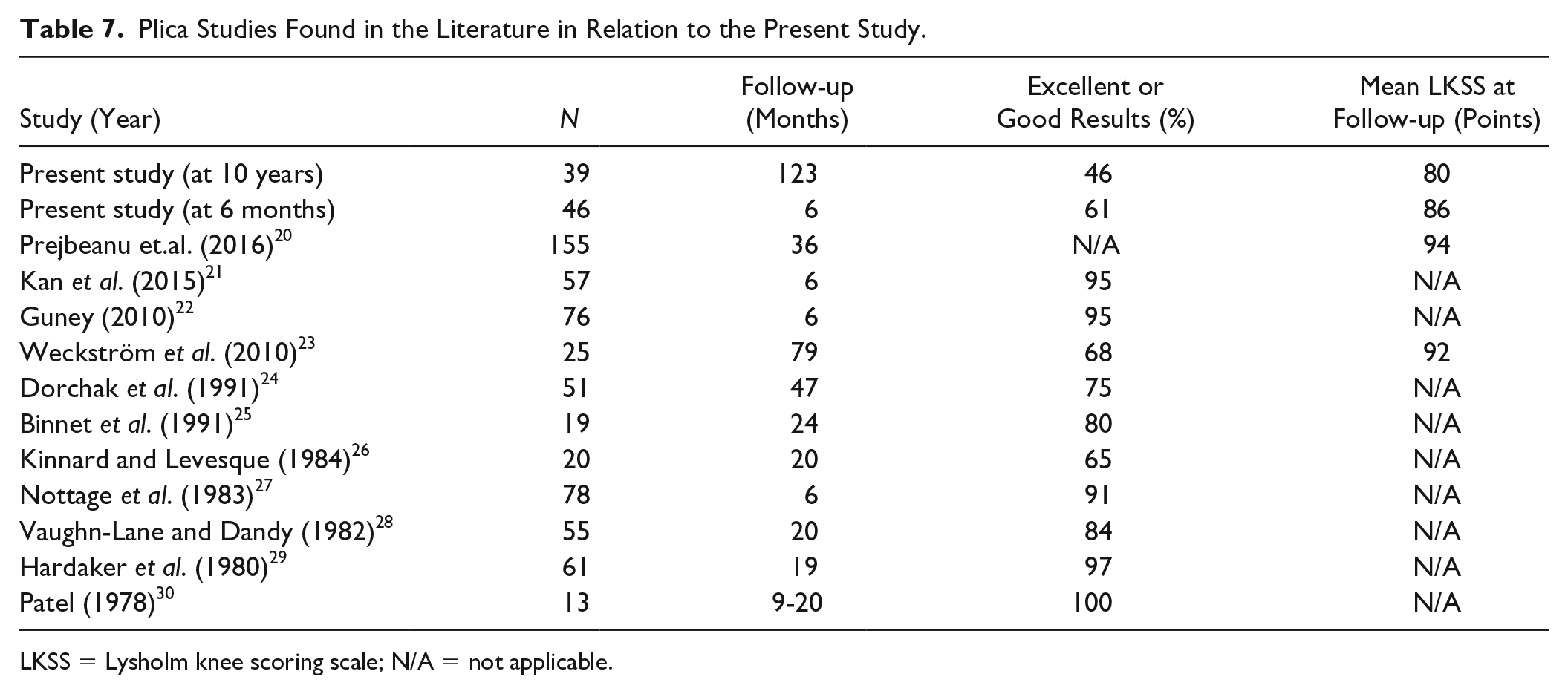
LKSS = Lysholm knee scoring scale; N/A = not applicable.
We found association between the poor plica syndrome treatment outcome and the presence of coexisting cartilage lesions. What is interesting, even evident (ICRS > 1) cartilage damage under the plica did not influence the primary functional score—those patients had similar mean LKSS to those without cartilaginous lesions. Patients with health cartilage did better in our long follow-up. Yang et al. 31 found an elevated level of matrix metalloproteinases in medial plicas of the knee joint at different stages of osteoarthritis. They concluded that medial plica may be involved in the process of cartilage destruction. 31 In the study conducted by Kang et al., 2 the presence of medial plica was considerably higher in the AKP group. They concluded that a careful assessment of patients with atraumatic AKP should include PF joint abnormalities, particularly the presence of medial plica and/or subtle abnormalities of the articular geometry. 2 In our study, patients with concomitant pathologies were excluded and medial plica syndrome was an isolated disorder. The only nonexcluding concomitant pathology was cartilage lesion. Even in the young population, we found a significant correlation between the ICRS grade and the clinical outcome. MPS may contribute to the development of further cartilage lesions; hence, the results of treatment will deteriorate with time.
In our study, type B plica was the most frequent finding. Liu et al. 32 analyzed a 3-dimensional dynamic finite element model of different plica types and its relation to femoral condyles. They found that type B plica generated the highest contact pressure on the medial femoral condyle. When simulated with Young’s module above 60 MPa, all analyzed types—A, B, and C—generated enough pressure to cause increased chondrocyte apoptosis.32,33 It is important that clinicians regard type B as a potential source of pain. Intuitively thinking that the larger type C plica is more painful can be misleading. We did not find any significant difference of cartilage damage degree between plica B and thicker C but no A type plica was accompanied by a deeper cartilage lesion. This phenomenon probably is the effect of different morphology and size of the plica, which may have an impact on cartilage area lesions. The exact relation between the plica size and its clinical manifestation requires future studies.
Gender may play an important role in surgical outcomes. Hewett et al. 34 demonstrated that growth and development play a role in the mechanism of decreased neuromuscular control of the knee in female, but not in male, adolescents. This finding may explain the predominance of female teenagers in our study. We observed that positive MO test was significantly more frequent in females. We also noted that females had more often SLS test positive and weak VMO palpation, but this dependency was insignificant.
Numerous authors described mainly good and excellent results after the arthroscopic treatment of MPS. Weckström et al. 23 reported good functional results in 17 of 25 patients in their follow-up; however, the study group was not free from concomitant knee joint pathologies. Dorchak et al. 24 demonstrated good and excellent results in 75% of cases, but the study was retrospective and had a very inconsistent follow-up. They noted better results in younger patients without cartilage lesions. The negative correlation of the outcome and age demonstrated in our study can confirm the results obtained by those researchers. 24 Excellent results were shown in the article by Guney et al. 22 (94% at 6 months), but only 26% of the patients in their group had isolated plica. The authors point out that a high percentage of concomitant cartilage and meniscal lesions found in the studies from the Middle and Far East could be connected with specific activities involving the hyperflexion of the knee, which is common in those regions of the globe.
Our long-term results are inferior to those achieved by Prejbeanu et al. 20 However, it should be noted that our cohort had the worst preoperative LKSS. In the current study, it increased from 53 to 80, while in theirs the increase was from 68 to 94. 20 Yilmaz et al. 35 excised retinacular bands lying beneath the medial plica and compared the results after this combined resection with standard plica resection. Surprisingly, this modification produced better results than plica resection alone. 35 They concluded that this type of procedure does not affect patellar stability; however, it is clear that the cause of symptoms in MPS is more complex than the plica alone.
We also investigated the influence of plicae resection on neuromuscular control of the extremity using 3 different clinical tests. Merican et al. 36 proved that the increase of iliotibial band tension had statistically significant effects on knee kinematics, including increased lateral tilt and translation of the patella, plus tibial external rotation in flexion. These effects could be responsible for significantly poorer results in patients with the positive MO test in our study. This statement should be treated with caution as there are studies showing that the outcome of the Ober test is highly influenced by the gluteus medius and minimus muscles as well as the hip joint capsule, not the iliotibial band tension alone. 37
The SLS test is a reliable tool to assess dynamic knee valgus. 15 Because of impaired muscle stabilization, dynamic valgus exerts increased lateral forces on the patella. Plica irritation could be attributed to abnormal patella kinematics. In these terms, dynamic valgus could yield worse results of plica resection causing cartilage damage due to patellofemoral joint overload. According to our findings, patients with abnormal PFJ biomechanics (i.e., positive SLS and poor VMO function) should not be treated with plica resection alone. Moreover, coexisting cartilage lesions are predictors of a poor outcome. In those cases, a more complex treatment of PFJ is required, including cartilage treatment and correction of biomechanics.
There are some important limitations to our study. The main drawback is that we enriched the examination protocol with functional tests (SLS, VMO, and OT) at the final follow-up. While designing the study protocol in 2004, we did not realize the possible importance of the whole limb kinematics on the MPS treatment outcome. The other limitation is the long break in the follow-up of our patients which may be responsible for a decreased number of the participants.
Conclusion
Clinical results of arthroscopic plica resection are better in patients without coexisting cartilage lesions. Poor neuromuscular control may contribute to abnormal patella tracking, leading to both medial plica irritation and further cartilage deterioration. Further investigation with control group is needed to indicate whether specific physiotherapy or plica resection should be performed in patients with this clinical entity.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the local university bioethics committee (approval number KB/338/2005).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Trial Registration
Not applicable.