
Abstract
Introduction
A prospective clinical investigation was carried out in order to clarify whether Matrix-associated autologous chondrocyte implantation (MACI) results in clinical improvement at long-term follow-up.
Hypothesis
MACI will result in clinical improvement at long-term follow-up.
Study Design
Case series; level of evidence, 4.
Methods
Thirty-eight patients were treated with MACI. These patients were evaluated for up to a mean of 16 years (range 15-17 years) after the intervention. Three different scores (Lysholm-Gilquist score, International Cartilage Repair Society score, and Tegner score) formed the basis of this study. Overall, we were able to obtain valid preoperative and postoperative results from 18 (47%) of 38 patients. In 1 patient, both knees were treated. In 4 patients, an arthroplasty was implanted over the course of time; thus they were excluded from this case series. In conclusion, follow-up of 15 knees was performed in the recent series.
Results
In subjective rating, 12 out of 14 patients (86%) rated the function of their knee as much better or better than before the index procedure. All numerical outcome scores showed significant improvement compared to the preoperative value (preoperative/postoperative at 5 years/postoperative at 15 years): Lysholm score 59.6 (±24.6)/78.6 (±21.5)/82.7 (±11.3), International Knee Documentation Committee score 50.6 (±22.7)/64.7 (±21.6)/69.7 (±18.7), Tegner score 3.0 (±2.2)/3.6 (±1.5)/5.2 (±1.7).
Conclusion
The significantly improved results on 3 scores after 15 years suggest that MACI represents a suitable treatment of local cartilage defects in the knee.
Introduction
The limited intrinsic healing potential of damaged articular cartilage is a well-known problem in orthopedic surgery. 1 Cartilage degeneration may be accompanied by pain, immobility, stiffness, loss of quality of life, and can potentially lead to severe osteoarthritis in the long term. A plethora of emerging treatments and associated surgical techniques have been described to improve cartilage repair techniques. 2 The treatment should aim at alleviating pain and restoring functionality in the first place eventually leading to the formation of an entirely new articulating surface that essentially duplicates the original articular cartilage in its structure, composition, and function. 3 In addition, cartilage repair should delay the need for total knee arthroplasty. 4
Since the clinical introduction of autologous chondrocyte implantation (ACI) by Brittberg et al., 5 a variety of clinical studies have documented the clinical effectiveness of implanting autologous culture expanded chondrocytes for the regeneration of cartilage. 1 For classical ACI, a periosteal flap is sutured to the surrounding healthy cartilage rim, creating a reservoir for the injection of the autologous chondrocyte cell suspension. The need for an intact cartilage rim limits the use of classical ACI to some regions of the knee. 6 Furthermore, the periosteal graft covering the defect gave rise to problems. 7 To overcome the intrinsic technical disadvantages of classical ACI, cartilage tissue engineered grafts were developed. An innovative procedure was developed by Behrens and colleagues,8,9 performing a chondrocyte implantation matrix-associated with a porcine collagen I/III membrane (matrix-associated autologous chondrocyte implantation [MACI]). A prospective clinical investigation was carried out in order to clarify whether MACI proves suitable to treat cartilage defects and confirms objective and subjective clinical and radiological improvement over a period of up to 16 years.
Materials and Methods
Patients were selected for the MACI procedure after conservative measures and imaging procedures confirmed cartilage damage requiring arthroscopy. Inclusion criteria were patients between 18 and 60 years old with localized cartilage defects. Exclusion criteria were inflammatory arthritis, total meniscectomy, knee instability, an inoperable valgus or varus deformity, patellofemoral dysplasia, and massive overweight (body mass index >35 kg/m2). All patients gave informed consent and treatment was approved by the ethical review board of the University of Luebeck, Germany (file number 98/056).
As described before, the surgical procedure is done in 2 steps. 9 After inspection of the defect area showing localized cartilage lesions of grade III and IV according to the Outerbridge classification, 10 200 to 300 mg of full thickness cartilage was biopsied from a non-weightbearing area of the intercondylar notch and placed in the transport medium. While in 2 patients the cartilage defect was due to a trauma, the other cartilage lesions were of unknown origin. Autologous patient serum was added and sent to Verigen Transplantation Service (VTS; Copenhagen, Denmark). Chondrocytes were isolated from the biopsy specimen by means of enzymatic digestion of the surrounding matrix. The cells were cultured subsequently for 4 weeks before being seeded (about 1 million cells/cm2) on the rough side of the porcine collagen I/III matrix (Chondro-Gide, Geistlich Pharma, Wollhusen, Switzerland). The loaded matrix was cultured with autologous serum for 3 days. In a second operative procedure, the cell-loaded matrix was implanted into the cartilage defect area. Following arthrotomy, the cartilage defect was prepared by curettage to remove any fissured and undermined cartilage. Debridement of the subchondral bone plate was performed with care to prevent perforation or subchondral bone bleeding. The dimensions of the defect were transferred to a template reflecting size and geometry of the defects. The collagen membrane loaded with cells was cut back to the template size and fitted into the defect with the cell-loaded surface facing the subchondral bone. The joint was manipulated intraoperatively to ensure adherence of the implant.
A standard postoperative rehabilitation program was performed in all cases, as described before. 3
Three different scores formed the basis for evaluation of the therapeutic success: the Tegner score, the Lysholm-Gilquist score and the ICRS (International Cartilage Repair Society) score, representing the IKDC (International Knee Documentation Committee) evaluation endorsed by the ICRS (www.cartilage.org). Postoperative findings that resulted from follow-up examination were documented and compared with the preoperative findings and the results after 5 and 15 years. The statistical analysis included a tabular description of the demographic data, subjective clinical scores and in selected cases x-ray findings. Statistical tests were performed using the Wilcoxon test and the Kruskal-Wallis test. During the initial 5-year postoperative evaluation phase, diagnostic rearthroscopy was indicated for 6 patients. Biopsies could be obtained in 4 cases, as described before. 9 In selected cases, a weightbearing x-ray of the knee was done and possible osteoarthritic degenerations were evaluated by 2 independent observers using the Kellgren-Lawrence scoring system. 11 The observers were blinded to the procedure. A Kellgren-Lawrence score of greater than or equal to 2 is defined as osteoarthritis.
Results
From November 1998 to March 2001, 38 patients were treated with MACI. These knee patients were monitored during the period from November 2014 to March 2015. Overall, we were able to obtain valid preoperative and postoperative results from 18 (47%) of 38 patients with a minimum of 15-year follow-up postoperatively. Two patients were known to have died. Four patients had a total knee replacement between 5 and 10 years with an average of 7 years; thus they were excluded from this case series. In 1 patient, both knees were treated, so that 15 knees were available for follow-up ( Table 1 ). The remaining patients were lost to follow-up. The mean follow-up period was 16 years (minimum 15 years, maximum 17 years). Eight patients were female and 6 male. According to the clinical scores no gender-related differences between male and female patients were obvious.
Descriptive Data, Defect Characteristics, and Defect Location of 15 Treated Knees in 14 Patients.
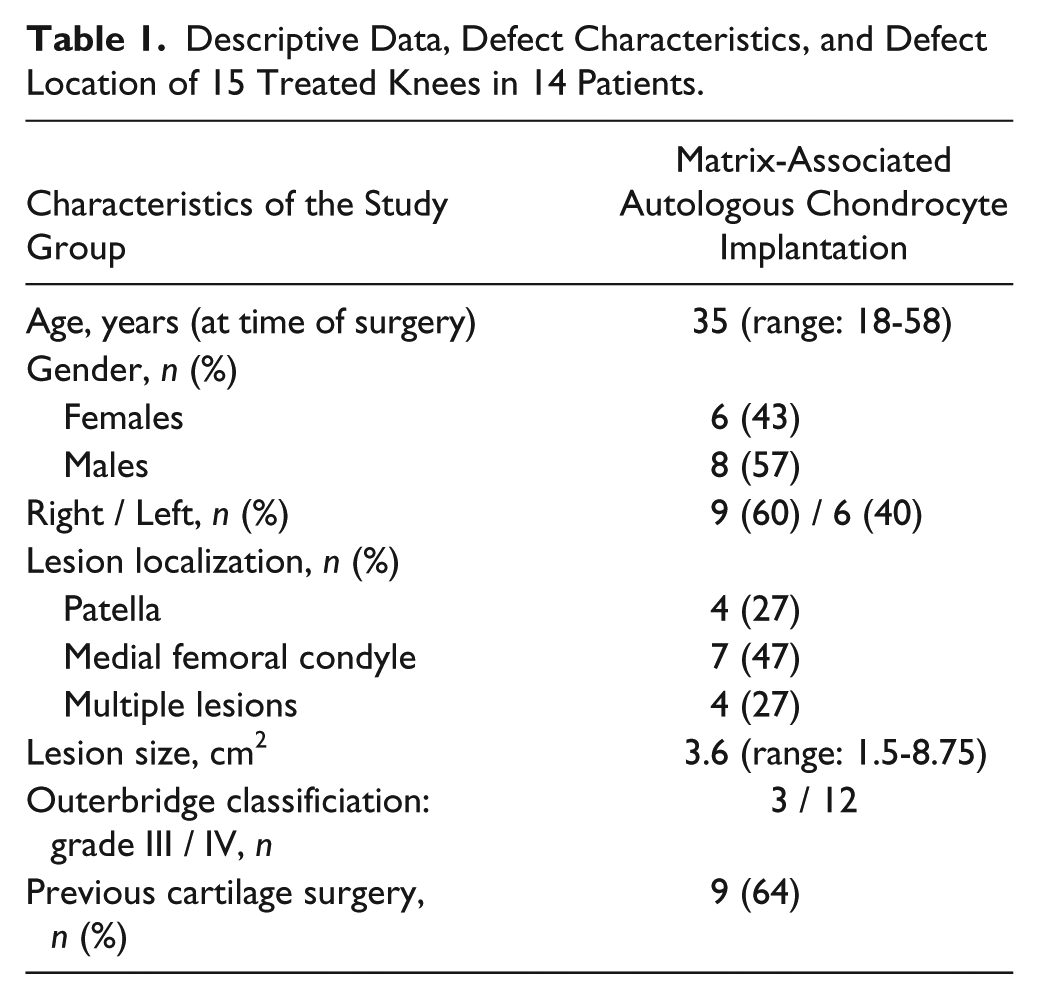
The mean age was 35 years (minimum 18 years, maximum 58 years) at the time of surgery ( Table 1 ). At the time of follow-up, the mean age was 50 years (minimum 34 years, maximum 74 years). In order to determine the influence of patient age at the time of surgery on the results, the patients were divided into 3 subgroups as published before 12 : patients aged between 18 and 32 years, patients from 33 to 46 years, and patients between 47 and 60 years. Looking at the results, none of the scores showed an age-related difference.
In most cases (n = 7, 46.7%) the defects were located at the medial femoral condyle. In 4 (26.7%) patients, the cartilage defect was diagnosed in the retropatellar area. A further 4 (26.7%) patients had multiple lesions ( Table 1 ). The location of the defect (medial or lateral femoral condyle, patellar or multiple lesions) did not influence the results.
Defect size varied between a total of 1.5 and 8.75 cm2, taken into account that the surface areas of the multiple lesions were added cumulatively. The mean value was 3.6 cm2. In order to evaluate the influence of the defect size on the clinical results 3 subgroups were analyzed as published before. 12 The individual groups (group I, defect size >0-3 cm2; group II, <3-6 cm2; group III, >3-6 cm2) did not differ significantly in the score values. In 6 (40%) patients, the cartilage defect was located in the left knee and 9 defects (60%) were diagnosed in the right knee. Analyzing the score values no significant differences were seen according to the affected side of the knee.
As only one of the patients was a smoker at the time of surgery, the impact of smoking on the clinical outcome cannot be evaluated.
Nine (64.3%) patients had previous surgery to their knee prior to undergoing MACI. Eight (53.3%) patients had already been operated once; only 1 patient had already 3 interventions. These surgeries included diagnostic arthroscopy, debridement and lavage, microfracture (MFx), lateral release, and anterior cruciate ligament (ACL) reconstruction. In order to investigate whether the score results were dependent on previous surgeries prior to the index procedure, patients were divided into 2 subgroups (no previous and previous surgery). The score results proved to be independent of whether or not the patients had been previously operated.
The mean height at that time was 174 cm (minimum 164 cm, maximum 184 cm) and the mean weight 83 kg (minimum 63 kg, maximum 110 kg). In order to investigate the influence of body weight on the clinical results patients were divided into 2 subgroups. Males less than 90 kg and women less than 70 kg of bodyweight were group A; patients with heavier bodyweight were group B. In summary, bodyweight did not have an influence on the clinical results, as no significant differences of the values in groups A and B were detectable.
In the subjective rating after 15 years, 12 out of 14 patients (86%) stated that their knee was “much better” or “better” than before surgery. The Lysholm-Gilquist score also showed a significant improvement postoperatively at 5 years (78.6 ± 21.5) and 15 years (82.7 ± 11.3) compared with the initial values prior to surgery (59.6 ± 24.6) ( Fig. 1 ). The IKDC score significantly improved as well; while the preoperative value was 50.6 ± 22.7, the values at 5-year and 15-year follow-up were 64.7 ± 21.6 and 69.7 ± 18.7, respectively ( Fig. 2 ). The Tegner score, compared with the preoperative values (3.0 ± 2.2) showed significant improvement at the time of follow-up at 5 years (3.6 ± 1.5) and 15 years (5.2 ± 1.7) ( Fig. 3 ). In conclusion, all scores significantly improved 5 and 15 years after surgery compared with the preoperative values. Comparing the score values of the follow-up investigations after 5 and 15 years, a slight increase is obvious, although this is not statistically significant.
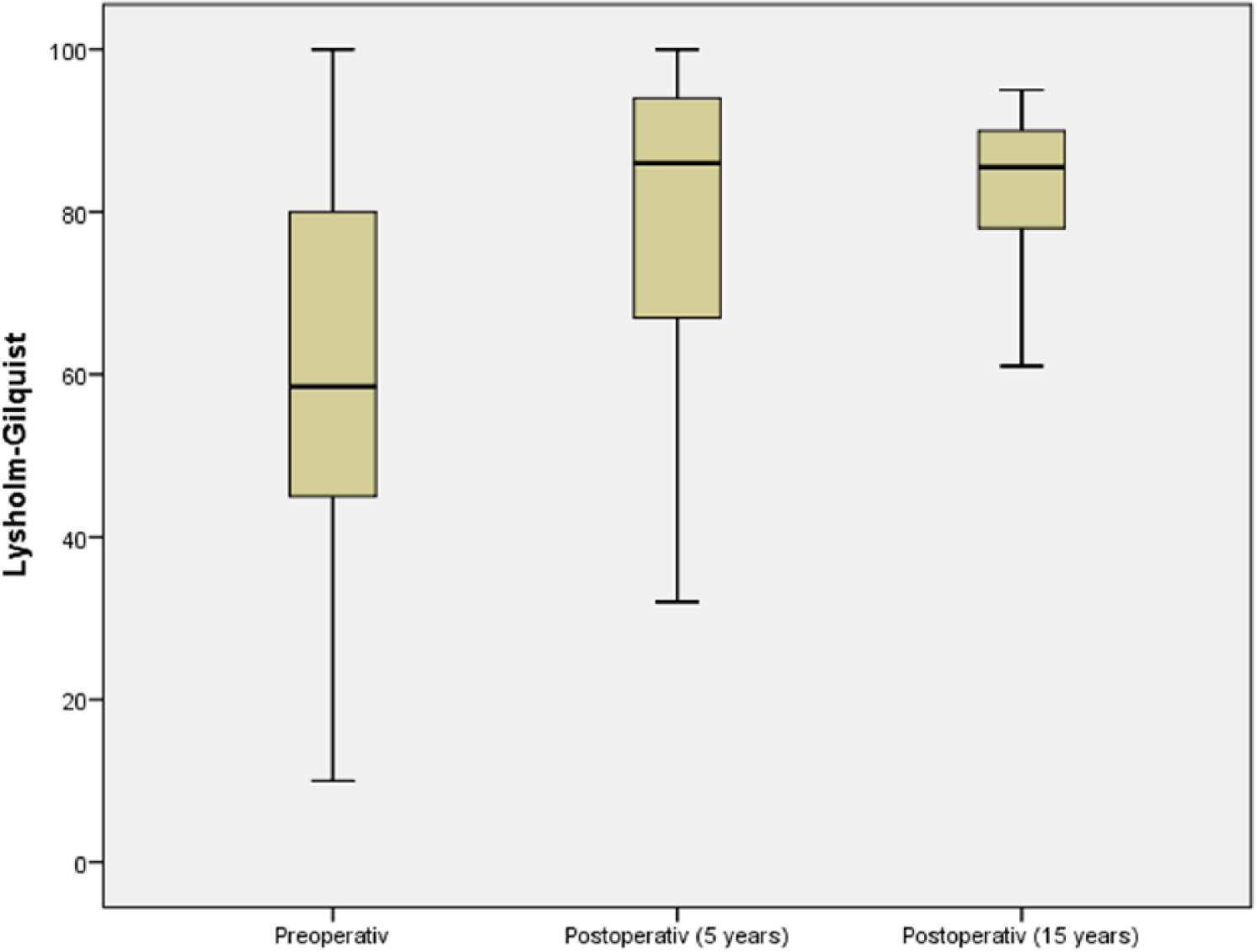
Box-and-whisker plot of the clinical outcome evaluated by the Lysholm-Gilquist score. The preoperative and follow-up times are as indicated. Scores are presented as medians; the ends of the boxes define the 25th and 75th centiles.
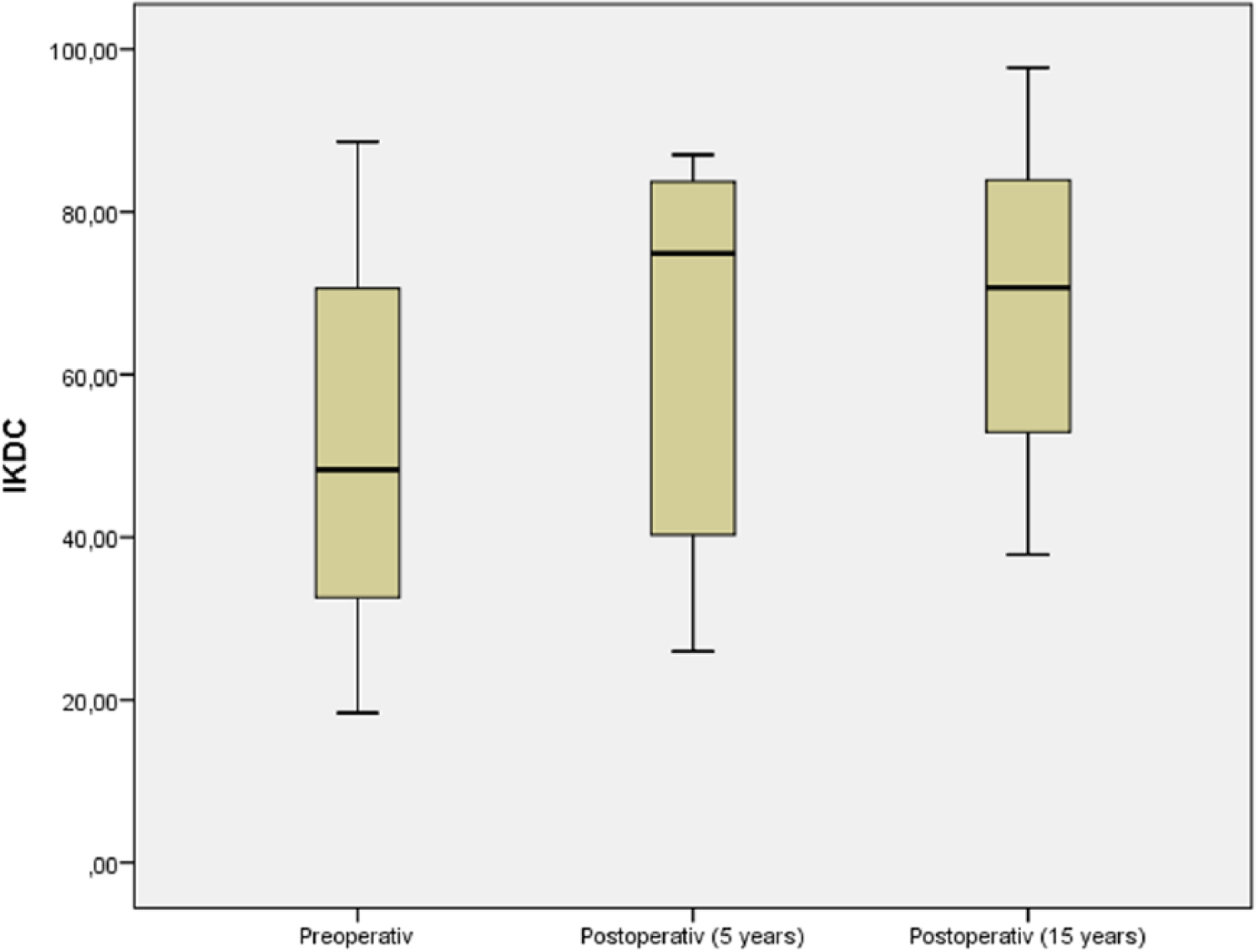
Box-and-whisker plot of the clinical outcome evaluated by the IKDC (International Knee Documentation Committee) score. The preoperative and follow-up times are as indicated. Scores are presented as medians; the ends of the boxes define the 25th and 75th centiles.
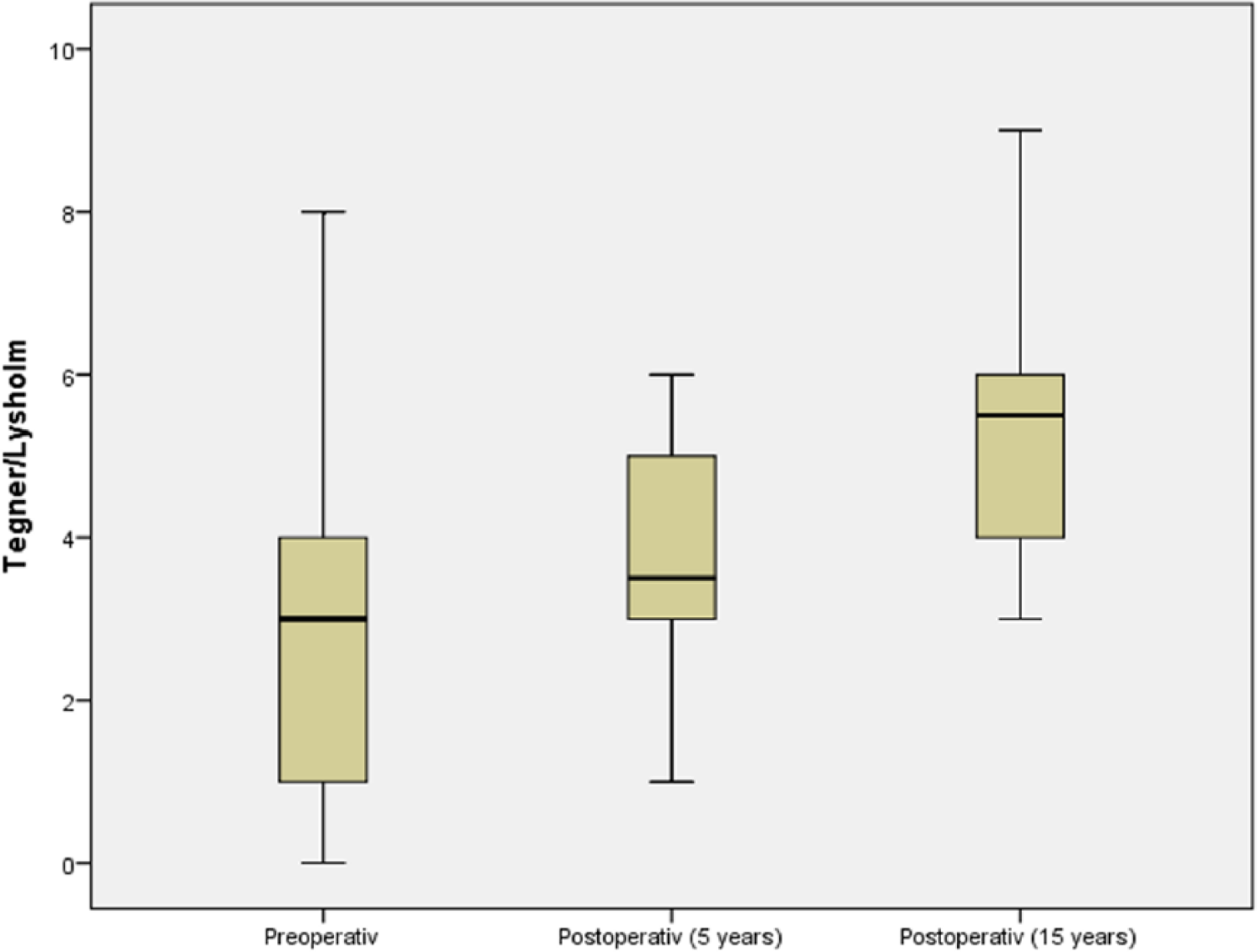
Box-and-whisker plot of the clinical outcome evaluated by the Tegner score. The preoperative and follow-up times are as indicated. Scores are presented as medians; the ends of the boxes define the 25th and 75th centiles.
Results of Imaging Diagnostics
The state of osteoarthritis was evaluated by the well-established Kellgren and Lawrence score, staging osteoarthritis from grade I to grade IV. 13 In selected cases, weightbearing x-rays were performed at the time of follow-up. Some patients already returned for clinical follow-up with current radiographies (posteroanterior and lateral). Some radiographs were weightbearing radiographies and others not. Because narrowing of the joint space is one of the major criteria of the Kellgren and Lawrence score, results were by implication not comparable and we did not perform statistical analysis. Irrespective of the joint space criterion, 6 of the follow-up radiographs showed signs of progressive osteoarthritis (osteophytes, subchondral sclerosis).
Discussion
This is one of the first uncontrolled clinical study presenting long-term results after MACI. The aim of the study was to evaluate if this technique results in objective and subjective improvements over a period of up to 15 years after surgery.
In an earlier study, we presented clinical improvement and good quality repair tissue at 5 years after MACI. 9 However, given the young age of patients being operated for such lesions, a longer duration of symptom relief would be of great importance. It remains questionable how the repaired tissue reacts during aging and how it follows the natural gradual development of osteoarthritis.
The present analysis is the first study reporting 15-year clinical and radiological outcomes after MACI procedure for articular chondral defects of the knee. As published earlier, the 5-year results provided strong support for the benefit of MACI. 9 This fact is underlined by the score values at 15-year follow-up showing still a slightly increase in clinical outcomes compared with the 5-year values. This is in contrast with the literature reporting a decline in the clinical outcome scores between the 5th and 10th year after matrix-associated autologous chondrocyte transplantation (MACT). 14
We had a follow-up rate of 47%; although this number implies a reduced reliability of our results, it might appear as an acceptable rate given the long follow-up as many treated patients could not be reached or tracked. 15 Moreover, many of the included patients were not followed during the last years; that makes it impossible to report the complication rate and any procedures performed during those years in a reliable way. Dropout is always a problem in studies with human participants, but especially so in longitudinal studies. For example, the dropout rate in large studies of musculoskeletal disorders has ranged between 7% and 57%. 16
In contrast to the literature, we did not see an impact of body weight on score results. As published in a series of 37 cases, a body mass index of more than 27.5 kg/m2 was associated with poor results in second-look arthroscopy after mesenchymal stem cell implantation for cartilage repair. 17 This is in accordance with the published data about an enhanced MFx technique at midterm follow-up. 18 In a prospective study by Mithoefer et al., 19 a lower body mass index correlated with higher scores for the activities of daily living and Short Form–36 after MFx in 48 symptomatic patients with isolated full-thickness articular defects in the knee joint. Worst results were seen in patients with a body mass index >30 kg/m2.
Like described in the literature, we could not show a correlation between clinical results and patient age. 20 In accordance with the recent study we could not show a significant impact of age on the results after autologous matrix-induced chondrogenesis (AMIC). 20 Results after ACI showed a failure rate in older patients that is comparable to rates reported in younger patient groups.12,21 Highlighting the patients age, de Windt et al. 22 showed in a prospective study treating 55 patients with MFx and ACI that the KOOS (Knee injury and Osteoarthritis Outcome Score) improvement was significantly better for patients under 30 years compared with older patients. Data of a randomized controlled trial with 80 human subjects treated with ACI or MFx by Knutsen et al. 23 are in accordance with findings from de Windt et al. 22 Both groups of authors concluded that the patient age influences the clinical outcome of ACI as of MFx.
In the present series, no gender-specific dimorphism was obvious. Opposed to this we demonstrated gender related results after AMIC in a former study. 20 Similarly, a follow-up study after ACI showed that female patients with patellar defects had worse prognostic factors. 24
Results presented in the literature strengthen the fact that clinical results and the incidence of complications is influenced by defect location. As it has been published before, there was a tendency for better clinical results at the femoral condyle compared with the patella. 24 Concerning the ACI, an increased rate of hypertrophy was found for patellar defects, but no correlation was found for the occurrence of delamination, insufficient regeneration, and disturbed fusion. 25 de Windt et al. 22 analyzed in a prospective cohort study the prognostic value of defect location (medial vs. lateral) on clinical outcome measures 3 years after cartilage therapy for a focal cartilage lesion in ACI and MFx. The authors found a significant better KOOS score for medial than for lateral lesions and therefore concluded that the defect location is related to clinical outcome of ACI and MFx. Another prospective cohort study by Kreuz et al. 24 confirmed the effect of defect location on clinical outcome measures after MFx procedures. IKDC and Cincinnati score as well as magnetic resonance imaging (MRI) findings showed significant better outcome measures when MFx was performed in femoral condyle versus tibia, trochlea, and retropatellar regions. Our recent data are in contrast with the literature as we could not see an impact of defect location on the outcome measures.
As reported in the literature, smoking has a negative impact on the results after cartilage repair procedures. 26 In the current series, only one of the patients was a smoker at the time of surgery, so the impact of smoking on the clinical outcome cannot be evaluated.
It is common that a patient population with cartilage defects of the knee may present with more than one isolated underlying pathology and thus needs more than one singular surgical procedure to address of all them. Previous surgical procedures did not prove to negatively influence the follow-up results in our series. This is in contrast with the literature, reporting defects that had prior treatment affecting the subchondral bone failed at a rate 3 times that of nontreated defects. 27 Data demonstrate that marrow stimulation techniques have a strong negative effect on subsequent cartilage repair with autologous chondrocyte implantation and therefore should be used judiciously in larger cartilage defects that could require future treatment with autologous chondrocyte implantation. This is in accordance with published data concerning midterm results after MACT. 9
Irrespective of the joint space criterion, 6 of the follow-up radiographs showed signs of progressive osteoarthritis (osteophytes, subchondral sclerosis). This is in accordance with the findings from a study by Knutsen et al., 28 who reported osteoarthritis in one-third of their patients 5 years after ACI or MFx. We did not obtain long radiographs from hip to ankle; thus, we could not measure alignment. Consequently, we could not assess a possible additional effect of malalignment. We did not perform MRI follow-up studies, as strong evidence is lacking to determine whether MRI is reliable in predicting clinical outcomes after cartilage repair. 29
There are limitations that need to be acknowledged and addressed regarding the present study. The first limitation concerns the heterogeneous patient population, which reflects the situation of patients with an indication for cartilage repair surgery.
The second limitation has to do with the extent to which the findings can be generalized beyond the cases studied. The number of cases is too small for broad generalizations.
In conclusion, MACI seems to be an effective and durable treatment for full-thickness cartilage defects in the knee. It provides satisfactory results in terms of both pain relief and knee function rehabilitation, which appear to be sustained in the majority of patients according to long-term follow-up results.
Footnotes
Acknowledgments and Funding
We gratefully acknowledge the assistance of Mr. Steffen Herzmann. We thank Dr. Friedrich Pahlke, EVIDAT, for statistical consulting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the ethical review board of the University of Luebeck, Germany (file number 98/056).
Informed Consent
Written informed consent was obtained from all patients before the study.