
Abstract
Introduction
Since OA is a slowly developing disease, surrogate outcome measures are essential for clinical trials to reduce required sample sizes, duration, and costs. 1 Following the BIPED criteria, a surrogate outcome must demonstrate a statistically significant relationship with relevant clinical or radiographic OA outcomes. 2
This study, among overweight/obese women free of knee OA at baseline, women with a decrease in body weight showed a significant reduction in cartilage cavity on magnetic resonance imaging (MRI) after 2.5 years (adjusted odds ratio [OR] 0.55, 95% confidence interval [CI] 0.37-0.83). An increase in body weight was not significantly associated to cartilage cavity (adjusted OR 0.84, 95% CI 0.56-1.26). Subsequently, the change in cartilage cavity over 2.5 years was significantly associated to incident radiographic (adjusted OR 1.65, 95% CI 1.29-2.11), but not to incident clinical (adjusted OR 1.11, 95% CI 0.86-1.44) knee OA after 6.5 years. Herewith, cartilage cavity meets the criteria for an efficacy of intervention or surrogate biomarker, which is deemed highly desirable for the short-term evaluation of potential interventions for OA.
Method, Results, and Discussion
The current study used data from the PROOF study (ISRCTN 42823086). 3 The study was approved by the Medical Ethical Committee of Erasmus MC and all participants gave written informed consent.
In short, women aged 50 to 60 years registered with the 50 participating general practitioners in the Rotterdam area in the Netherlands were contacted. Those reporting a body mass index (BMI) ≥27 kg/m2, free of knee OA according to the clinical ACR (American College of Rheumatolgy) criteria were invited for baseline measurements. For further PROOF details, see elsewhere. 3
At baseline, 2.5 years, and 6.5 years, the following measurements were obtained: age, knee symptoms (“pain in or around the knee in the past 12 months”) and history of knee injury using questionnaires, a standardized semiflexed posteroanterior radiograph of both knees to assess Kellgren and Lawrence (KL) grade, physical examination to determine body weight and height for BMI calculation, and a multisequential MRI of both knees using a 1.5-T scanner. 4 Additionally, body weight was measured at 6, 12, 18, and 24 months.
PROOF used different 1.5T Siemens Symphony/Magnetom Essenza and Philips Intera scanners using sagittal 3-dimensional (3D) sequences with water excitation. The voxel sizes differed between scanner models: Siemens Symphony had 1.5 × 0.42 × 0.42 mm, Siemens Magnetom Essenza had 1.5 × 0.5 × 0.5 mm, and Philips Intera had 1.5 × 0.31 × 0.31 mm. For a subset of 25 knees, the medial tibial and femoral and the patellar cartilage compartments were manually segmented on a sagittal 3D water selective (WATS) sequence with fat saturation. 5 These segmentations were used for training of the Knee Imaging Quantification (KIQ) framework that automatically segmented all baseline and 2.5-year MRIs. 6 KIQ provided cartilage thickness maps from which we quantified the mean thickness over the total area of bone and the cartilage cavity as the total volume of indentations/lesions for each compartment. These indentations were detected as deviations from a smoothly varying thickness map using multiscale anisotropic blob detection. The resulting cavity estimate is measured as the total volume (in mm3) of the indentations and was normalized for total cartilage volume (in %). This method was previously validated on artificial lesions demonstrating high correlation with ground truth and against radiologist lesion scores. 7
For the grouping of subjects, previously reported subgroups of patients with comparable evolution of body weight over 2.5 years were used; a group that gained weight (7.2 ± 4.1 kg after 2.5 years), a relatively stable group (0.6 ± 3.4 kg), and a group that lost weight (−7.7 ± 6.3 kg). 8
The change in the normalized cavity score from baseline to 2.5 years served as outcome for the evaluation of the differences between the groups of body weight evolution. For the subsequent incidence of knee OA after 6.5 years, knee OA was defined using radiographic (incident KL ≥ 2) and clinical definitions (incident clinical knee OA according to the clinical and radiological ACR criteria 9 ).
For the present study, all subjects with baseline and 2.5-year MRIs and OA incidence measure available after 6.5 years were selected for analyses.
Baseline characteristics were compared between the entire cohort and the current selection to evaluate possible selective drop-out using t tests for continuous and chi-square tests for dichotomous variables. Using generalized estimated equations to account for the correlation between knees within subjects (unstructured correlation matrix), the change in normalized cavity from baseline to 2.5 years was compared between groups, with the “stable” group as reference. Parameter estimates were adjusted for covariates. Subsequently, the 2.5 years change in normalized cavity was used as independent variable to study its effect on the two outcome measures, using generalized estimated equations adjusted for covariates, as well as weight loss group from the latent growth curve analysis.
For comparison, the change in cartilage thickness was also compared between the body weight trajectories and the association between 2.5-year change in cartilage thickness and subsequent knee OA development was evaluated, using identical statistics.
A total of 456 knees were available. Mean age was 55.8 ±3.2 years and mean BMI was 31.9 ± 3.8 kg/m2. At baseline, only BMI was slightly different between those selected for the current analyses and the individuals without complete follow-up data (31.9 ± 3.8 vs. 33.0 ± 4.7 kg/m2).
Mean change in normalized cartilage cavity from baseline to 2.5 years for the 3 body weight groups and corresponding adjusted odds ratios are presented in Table 1 . Compared with the group with stable body weight, the 2.5-year change in normalized cartilage cavity score was significantly lower in the group with a decreased body weight (P = 0.005).
Change (± Standard Deviation; Minimum to Maximum) in Normalized Cartilage Cavity Score and Cartilage Thickness (Baseline to 2.5 Years) for Subgroups of Patients and Corresponding Adjusted Odds Ratios.
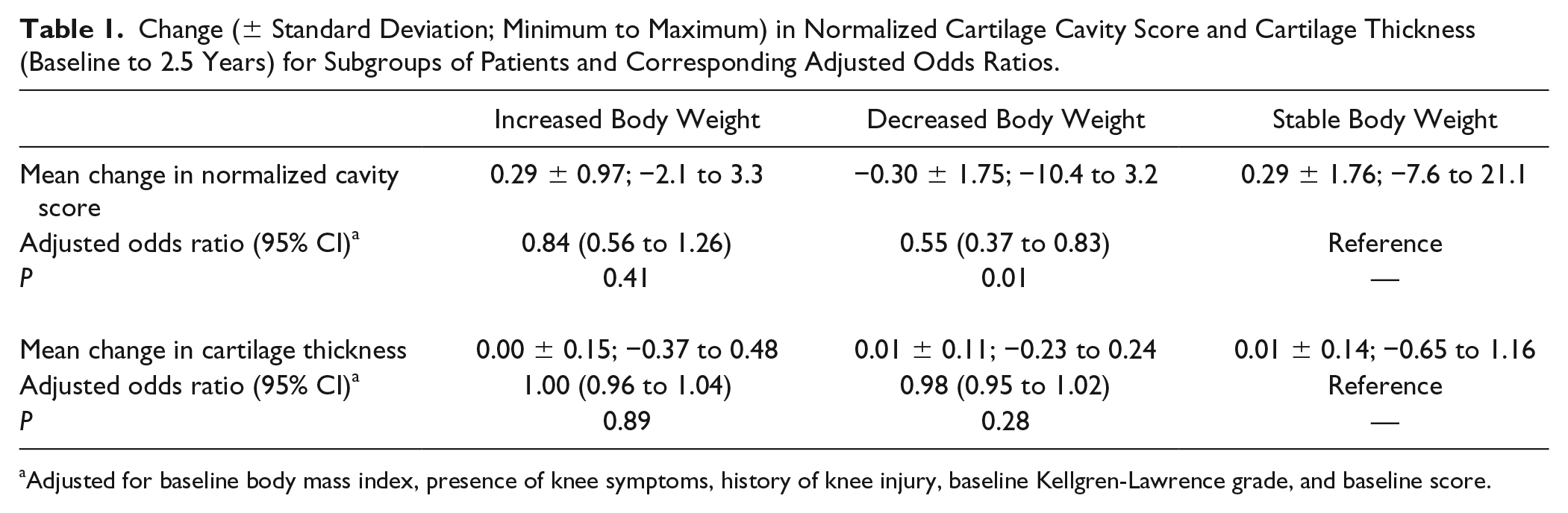
Adjusted for baseline body mass index, presence of knee symptoms, history of knee injury, baseline Kellgren-Lawrence grade, and baseline score.
The change in normalized cartilage cavity was significantly associated to the incidence of radiographic knee OA after 6.5 years, with an adjusted OR of 1.65 (95% CI 1.29 to 2.11; P < 0.001) for each unit of change. There was no association with incident clinical knee OA after 6.5 years (adjusted OR of 1.11, 95% CI 0.86 to 1.44; P = 0.42).
Additionally, the change in normalized cartilage cavity from baseline to 2.5 years was split into tertiles and used as predictor for incident radiographic and clinical knee OA (see Table 2 ).
Associations Between Tertiles of Change in Cartilage Cavity Score Over 2.5 Years and Incident Knee Osteoarthritis (OA) after 6.5 Years.
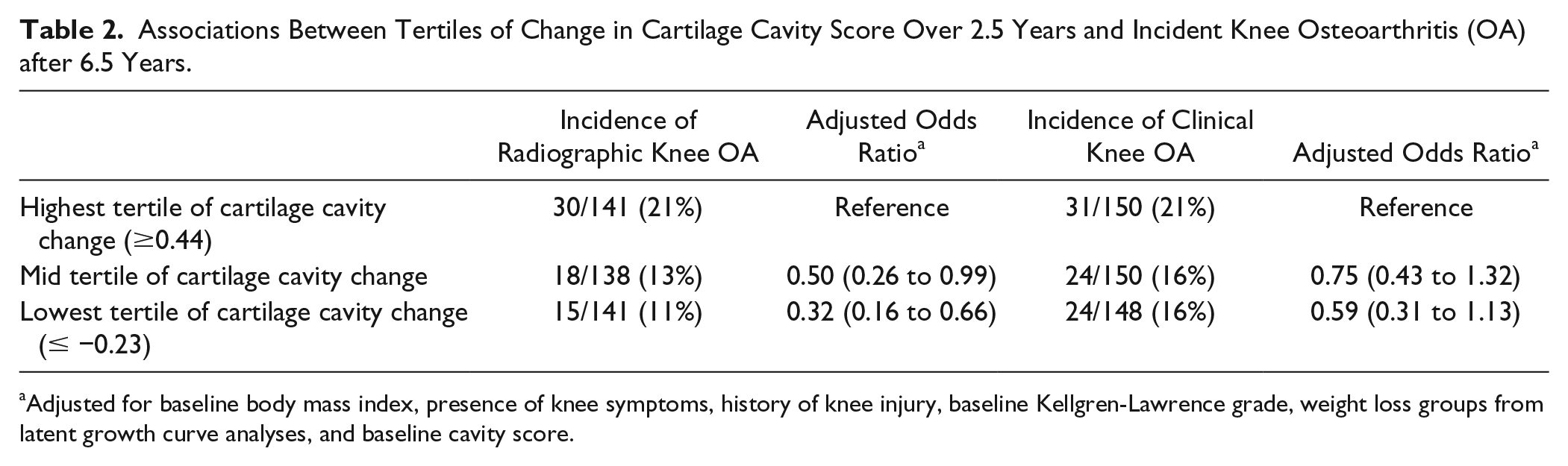
Adjusted for baseline body mass index, presence of knee symptoms, history of knee injury, baseline Kellgren-Lawrence grade, weight loss groups from latent growth curve analyses, and baseline cavity score.
There were no significant associations between the 2.5-year change in cartilage thickness and radiographic (adjusted OR 0.12, 95% CI 0.003 to 5.12, P = 0.26) or clinical knee OA (adjusted OR 0.20, 95% CI 0.03 to 1.32, P = 0.09) development after 6.5 years.
As required by the definition of an efficacy of intervention biomarker, 2 the current results showed that the change in cartilage cavity over the first 2.5 years was significantly associated to clinical relevant weight loss and to subsequent development of radiographic knee OA among a high-risk group of overweight/obese women free of knee OA. The association between change in cartilage cavity and subsequent clinical OA development was not statistically significant (P = 0.42), with only a statistically nonsignificant trend in the lowest tertile of 2.5-year cavity change (P = 0.11). Clinically relevant weight changes were not associated to significant changes in cartilage thickness over time in the present study.
Although biomarkers that respond to treatment have been reported in OA before (e.g., markers of matrix turnover and inflammation after diet and exercise, 10 biochemical markers of cartilage degeneration after residronate administration, 11 and bone marrow lesions after a brace intervention 12 ), the association of the change in there markers to future OA development, and thus the clinical relevance of the change in the biomarker, has not been studied widely. Moreover, the evaluation of these intervention effects and the association to future OA has hardly been studied within the same cohort. The current results warrant external validation to confirm cartilage cavity as an efficacy biomarker and to provide insights in the proportion of treatment effect explained. 2 When validated, it might serve as a relevant outcome measure to study short-term intervention effects. Within the present cohort, cartilage cavity showed to be more sensitive to clinically relevant weight loss and more strongly related to incident radiographic knee OA development than cartilage thickness.
The current study has some limitations. The current results were not obtained from an effective intervention, but rather from the observational significant and clinically relevant associations between weight loss and clinical and structural OA development.13,14 A limitation of our validation of the compartment-accumulated cavity score is that the score does not show to what extent the quantification corresponds to few larger lesions or multiple smaller lesions, or whether focal defects such as fibrillations or fissures contribute to the score. Therefore, further validation could be performed against more invasive scorings from optical coherence tomography 15 or from histopathology. 16 Because of the long follow-up period, there was substantial loss to follow-up, which limited the statistical power to detect significant associations, such as the difference in incidence of clinical knee OA for the decrease/increase in cartilage cavity. The loss to follow-up might also have introduced a bias due to selective drop-out. However, only BMI showed a statistically significant difference and the clinical relevance of this is likely minimal.
In conclusion, clinically relevant weight loss among a high-risk population of middle-aged women free of knee OA resulted in a significant reduction in the cartilage cavity score over 2.5 years. The change in cartilage cavity score was significantly associated to radiographic knee OA development in the subsequent period of 4 years. Herewith, cartilage cavity meets the criteria for an Efficacy of intervention or surrogate biomarker, which is deemed highly desirable for the short-term evaluation of potential interventions for OA.
Footnotes
Authors’ Note
The work presented here was done in collaboration between the Department of General Practice of Erasmus MC University Medical Center Rotterdam and Biomediq A/S.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PROOF study was funded by the Netherlands Organisation for Health Research and Development. The research leading to these results has received funding from the D-BOARD consortium, a European Union Seventh Framework Programme (FP7/2007-2013) under grant agreement number 305815. None of the study sponsors was involved in drafting the study questions, data acquisition, data analyses and interpretation, or the writing of the manuscript.
Author Contributions
All authors contributed to the conception and design of the study, interpretation of data, revising the manuscript critically for important intellectual content and approved the final version of the manuscript as submitted. JR, SMAB-Z, and EBD were responsible for acquisition of the data. JR performed the data analysis and drafted the manuscript. JR, SMAB-Z, and EBD take responsibility for the integrity of the work as a whole, from inception to finished article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Erik B. Dam is a Biomediq shareholder. The other authors declare no conflicts of interest.
Ethical Approval
The study was approved by the Medical Ethical Committee of Erasmus MC (MEC-2014-333).
Informed Consent
All participants gave written informed consent.