
Abstract
Objective
The purpose of this study was to compare results of osteochondral fractures (OCF) after first-time lateral patella dislocation, when either refixation or debridement was performed in a mid- to long-term follow-up and to analyze redislocation and reintervention rates.
Design
Fifty-three consecutive patients with OCF were included in this retrospective comparative study. Indication for refixation was presence of subchondral bone at the fragment. Thirty-six OCF were located at the patellar surface, and 17 at the lateral condyle of the distal femur. Refixation was performed in 28 patients while 25 patients underwent removal and debridement. Mean follow-up was 8.9 years (±4.4, range 2.0-16.7 years). For assessment of clinical outcome, the International Knee Documentation Committee (IKDC) Score, Knee Injury and Osteoarthritis Outcome Score (KOOS), and Lysholm score were used. Redislocation rate and further surgical interventions within follow-up were evaluated.
Results
All clinical scores in the refixation group yielded significantly better results at mid- to long term follow-up (IKDC P < 0.001, KOOS P = 0.006, Lysholm P = 0.001). Significantly more surgical reinterventions were necessary after debridement (48% vs. 7.1%, P = 0.001). The overall redislocation rate in cases with medial reefing as single stabilizing procedure was 43.3%.
Conclusions
Refixation of OCF after lateral patella dislocation shows improved clinical outcome at mid- to long-term follow-up compared with debridement. Therefore, effort to try fragment refixation is recommended. Redislocation rate is high without proper restoration of patellofemoral instability.
Introduction
Lateral patella dislocation is a common injury in adolescents.1-9 The reported incidence is about 5.8 per 100,000, with a 5-fold increase in the age group of 10 to 17 years. 10 Multiple factors contribute to patella instability. Trochlear dysplasia and insufficiency of the medial patellofemoral ligament (MPFL) have been identified as main risk factors for recurrent dislocations.11-15 Osteochondral fractures (OCF) are complications of lateral patella dislocations and can occur either at the retropatellar surface or the lateral femoral condyle during dislocation or repositioning.3,4,16-19 These injuries have been reported to dramatically increase the risk of osteoarthritis in further course.9,20 Different types of cartilage lesions can be found, ranging from visible bone bruise in magnetic resonance imaging (MRI) to OCF of the knee joint.19,21 Multiple treatment options for this condition have been proposed over the past years, including refixation, removal of fragments with debridement, microfracture, mosaic plasty, and chondrocyte transplantation.22-28 There has been some controversy on the ideal treatment of OCF in the past years: A number of studies reported good results after refixation of OCF4,7,16,17,21,26,28-32; however, some studies found better results with microfracture or fragment removal and debridement.21,33 There exist only very little data on results of refixation and debridement in a long follow-up,4,31,34 and there are only few studies available that directly compare these treatment options.21,33 Furthermore, there are also scarce data on the risk of redislocation in cases of patellofemoral instability with OCF and concomitant procedures for patellar stabilization.4,20,34
Therefore, the purpose of this retrospective comparative study was to investigate and compare the mid- to long-term outcome after either refixation or debridement of OCF in a large series of cases with first time lateral patella dislocation and OCF. Secondarily, redislocation and reintervention rate were evaluated.
Methods
Only cases of acute OCF after first time lateral patella dislocation with diagnosis within 1 week were evaluated. Diagnosis was made using X-rays or MRI ( Fig. 1 ). All patients underwent subsequent surgical intervention within the first week after dislocation with either refixation of OCF or debridement of defect site at our institution between 2006 and 2016.
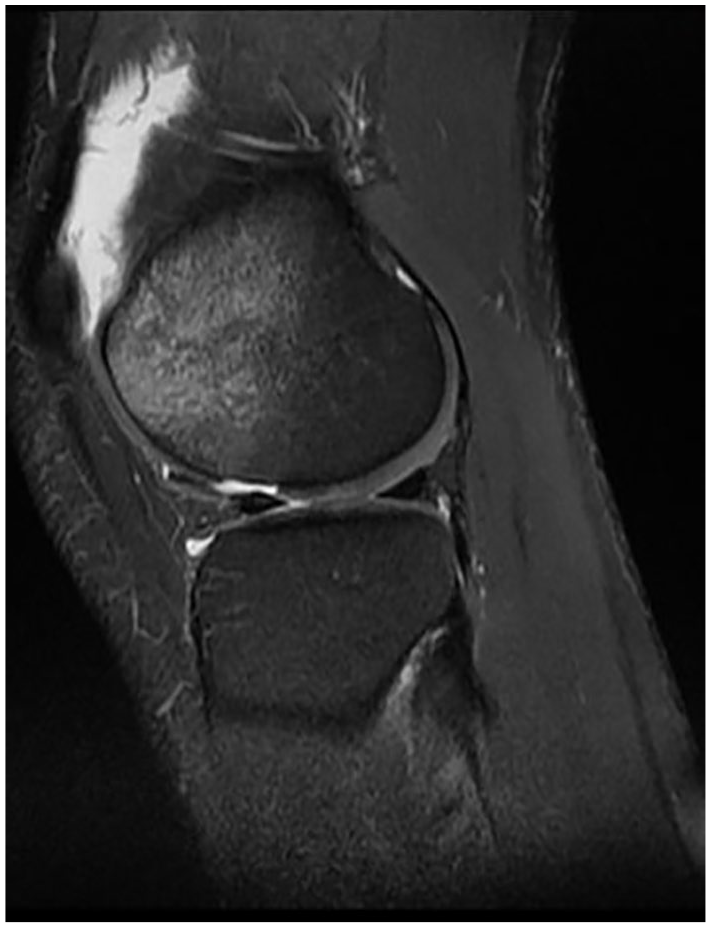
Magnetic resonance imaging with acute osteochondral fracture (OCF) on the lateral femoral condyle with displaced fragment (sagittal view, PD FSE [proton density fast spin echo] sequence).
Following were the inclusion criteria acute OCF within the weightbearing zone of the lateral femoral condyle or the retropatellar surface, complete documentation of defect size and additional procedures. Exclusion criteria were concomitant intraarticular injuries, history of previous knee surgery, absence of ability for consistent reevaluation, patients presenting with chronic conditions after OCF or fragments older than 1 week. Bony avulsion fractures of the MPFL at the medial patellofemoral margin were excluded as well as osteochondral rim lesions at the lateral distal femur which were located outside the weightbearing zone.
From 72 consecutive cases, 6 were excluded because of additional intra-articular injury, 4 because of previous knee surgery and 2 because of neurologic or psychiatric disorders. From the remaining 60 cases, follow-up could be completed in 53 patients (88%). Patients were contacted by telephone and postal questionnaire. The mean follow follow-up period was 8.9 years (±4.4, range 2.0-16.7 years). The medical records of these cases were retrospectively analyzed with special regard to fragment description, size, and localization, which was obtained during diagnostic arthroscopy using a graduated measuring rod. For assessment of clinical outcome, the International Knee Documentation Committee (IKDC) Score, Knee Injury and Osteoarthritis Outcome Score (KOOS), and Lysholm score were used. Further surgery for cartilage symptoms and redislocations were also recorded. A subanalysis including 42 cases with a mid- to long-term follow-up (>5 to 16 years) was performed.
Patients’ characteristics and anthropometric data are presented in Table 1 . There was no significant difference between the refixation and the debridement group according to sex, affected knee, age, postoperative follow-up, additional medial reefing, and localization of osteochondral injury. The mean defect size was 3.1 cm2 (±2.6) and was significantly larger in the refixation group with 3.7 cm2 (±2.6) than in the debridement group 2.0 ± 1.4 cm2 (P = 0.001), respectively.
Patients’ Characteristics, Reinterventions and Redislocations.
The study protocol was approved by the competent research ethics board of our institution (IRB-2018-008). All patients gave their written informed consent to the study.
Surgical Technique
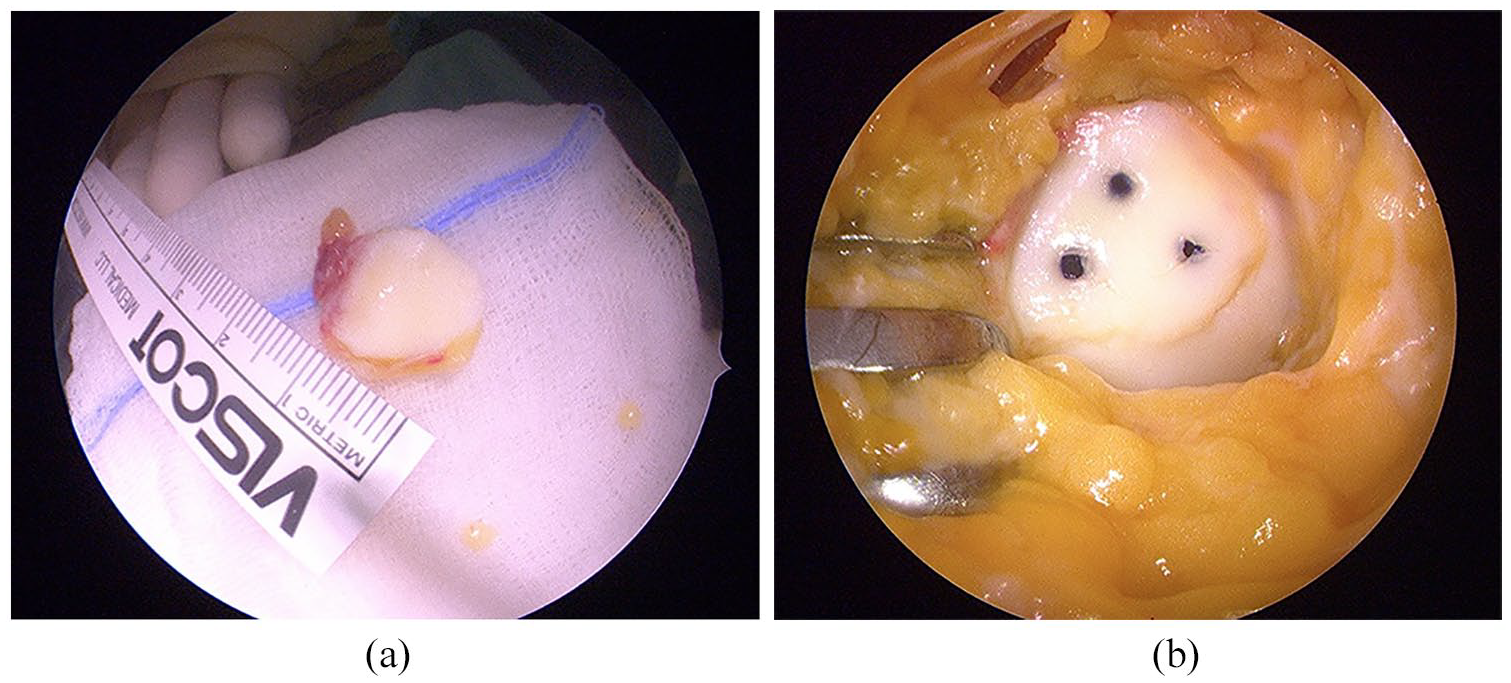
During a diagnostic arthroscopy all visible fragments were taken out the knee joint and inspected on the back table ( Fig. 2a ). Refixation of OCF was conducted whenever possible in all fragments independent of size or number of fragments with presence of subchondral bone. In the event of retropatellar OCF, a medial parapatellar arthrotomy was performed with patella everted. In case of OCF at the lateral femoral condyle a lateral mini arthrotomy was performed. For refixation of fragments bioabsorbable pins with 1.3 mm diameter and customized length (Ethipins 1.3 mm, Ethicon, Norderstedt, Germany) consisting of poly-p-dioxanon (PDS) were used. Depending on size of each fragment 1 to 6 pins per patient were implanted ( Fig. 2b ). If crushed fragments were obtained and refixation was not possible due to severity of damage or complete absence of subchondral bone, the defect site underwent arthroscopic debridement with complete opening of subchondral bone with a curette or a shaver to induce fibrocartilage formation. In 47 patients (88.7%), an additional open medial reefing of the medial retinaculum was performed when lateralization of patella was present, using mattress-sutures for reefing of the vastus medialis and the medial retinaculum as described before. 8 No further stabilization procedures (e.g., MPFL reconstruction) were performed within the years of the study. All patients were mobilized with partial weightbearing from the next day to 6 weeks. In case of retropatellar defects, a limitation of range of motion was carried out depending on the contact between defect and trochlea using a brace for 6 weeks. Defects on the lateral femoral condyle were also mobilized with partial weightbearing for 6 weeks. All patients received continuous passive motion therapy until full weightbearing. Postoperative MRI after refixation of OCF at the lateral femoral condyle with 3 bioabsorbable pins is shown in Figure 3 .
(

Magnetic resonance imaging after refixation of osteochondral fracture (OCF), 5-month postoperative (sagittal view, PD FSE [proton density fast spin echo] sequence).
Statistics
Data were obtained and analyzed retrospectively. Statistical analysis was performed using IBM SPSS Statistics for Windows (version 24, IBM Corp., Armonk, NY). Parametric data were analyzed using a t test. Nonparametric data was analyzed with the Mann-Whitney U test. For nominal data, the Pearson chi-square test or Fisher’s exact test was used. All reported P values are 2-tailed, with an alpha level <0.05 considered as significant. Unless otherwise stated, descriptive results are demonstrated as mean ± standard deviation and range.
Results
Clinical outcome scores for all patients were significantly higher in the refixation group (IKDC P < 0.001, Lysholm P = 0.001, KOOS P = 0.006). No differences were present in the outcome scores with regard to defect location. Follow-up scores for refixation in the general survey were: IKDC (88.9 ± 7.4), Lysholm (88.5 ± 8.1), and KOOS Symptoms (87.3 ± 7.8) while scores in the debridement group showed inferior results: IKDC (73.4 ± 14.6), Lysholm (77.8 ± 11.9), KOOS Symptoms (78.2 ± 14.3).
A subanalysis including 42 patients with a mid- to long-term follow-up (>5 to 16 years) confirmed significantly higher outcome scores for refixation (IKDC P < 0.001, Lysholm P = 0.003, KOOS P = 0.007) The detailed evaluation of outcome scores of patients with mid- to long-term follow-up is demonstrated in Table 2 and Figure 4 .
Evaluation of Outcome Scores of Patients With Mid- to Long-Term Follow-up (>5 to 16 Years). a
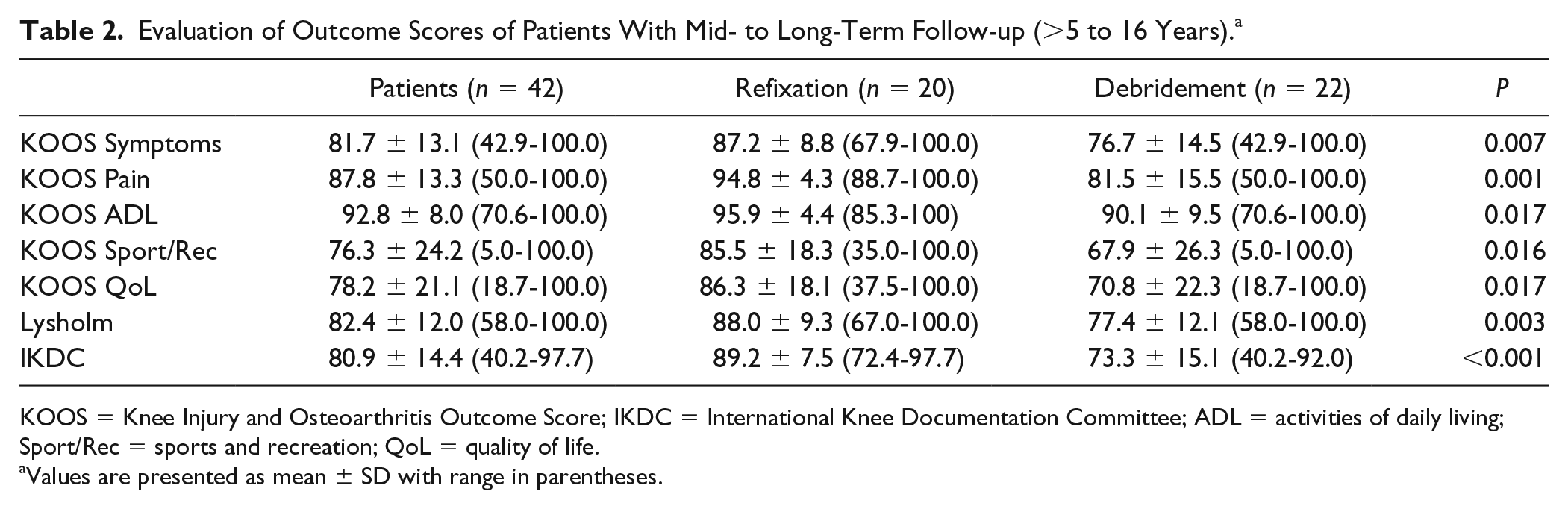
KOOS = Knee Injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee; ADL = activities of daily living; Sport/Rec = sports and recreation; QoL = quality of life.
Values are presented as mean ± SD with range in parentheses.
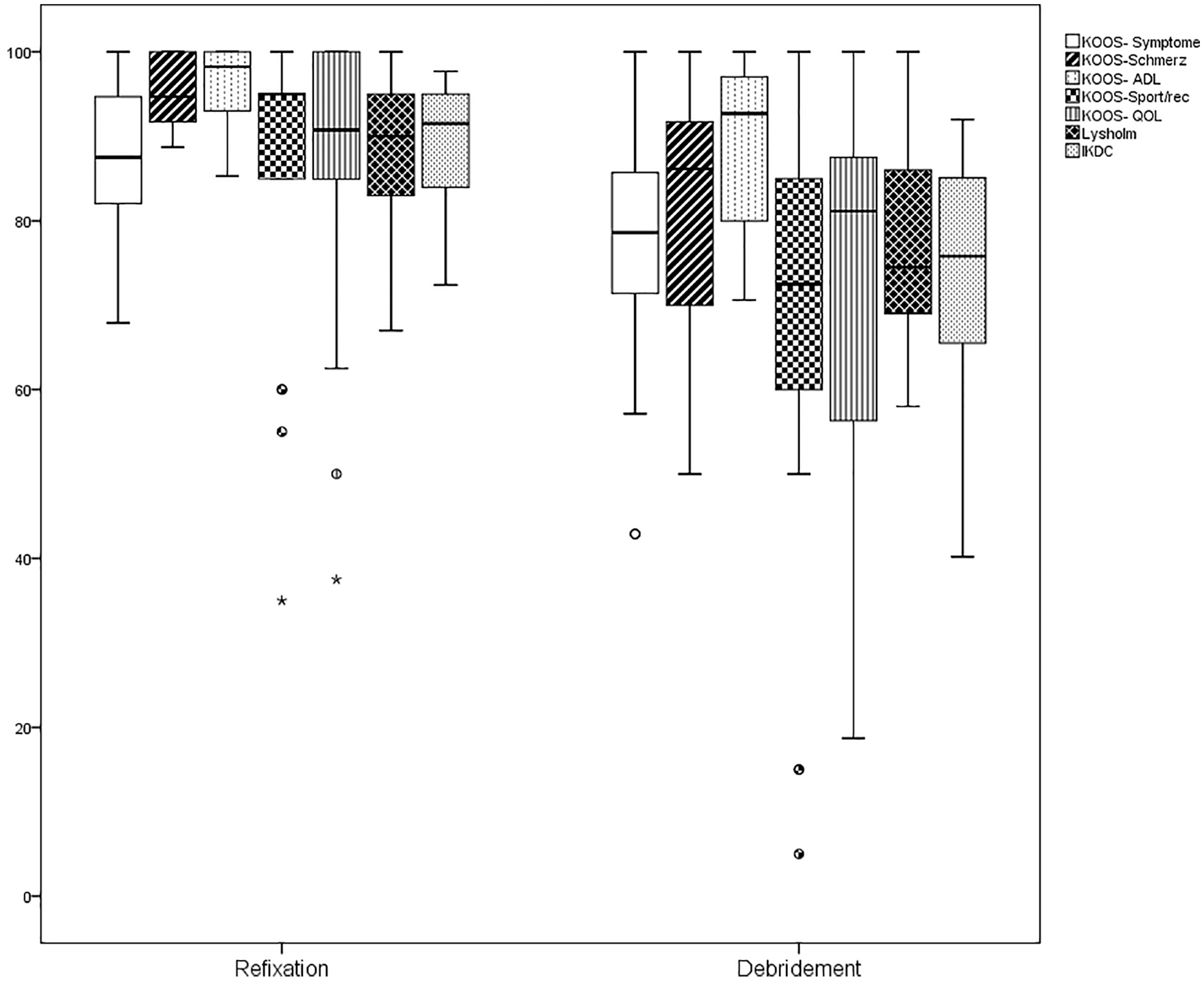
Boxplot of outcome scores of patients with mid- to long-term follow-up (>5 to 16 years) (range, median, 95% confidence interval). KOOS = Knee Injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee; ADL = activities of daily living; Sport/Rec = sports and recreation; QoL = quality of life.
There were significantly more surgical reinterventions because of symptomatic cartilage defects in the debridement group (48.0%) compared with the refixation group (7.1%) (P = 0.001).
An overall redislocation rate of 43.3% was found within follow-up, without significant difference between the 2 groups (P = 0.101).
Discussion
The most important finding of this study is that refixation of OCF after patella dislocation yields good clinical outcomes in a mid- to long-term follow-up and is superior to debridement. Furthermore, patients without proper individual treatment of the underlying patellofemoral instability show a high rate of redislocations.
Previous studies demonstrated the feasibility and good clinical outcome of OCF refixation after patella dislocation using different methods3,4,7,23,32,34,35 while 2 other studies advocated superior short-term results for debridement and microfracture.21,33 Only scarce data are available regarding the course of OCF with regard to mid- and long-term outcome.9,20
Lee et al. 21 compared the results of OCF after refixation in the weightbearing zone of the patella with debridement in a retrospective case series with 9 adolescent patients. In their study, 4 patients underwent refixation, while 5 patients underwent removal of fragments with microfracture. The authors found better IKDC and KOOS scores, as well as less symptomatic patients in the nonfixation group during short-term follow-up of 30.2 months but did not report significant difference between the 2 groups. Compared with the present study, their case series was rather small with a short-term follow-up period. Furthermore, OCF of the distal femur was not included although it is common as well. The small defect size (mean 1.2 cm2) and the limited number of patients in the microfracture group combined with younger age of patients might explain those results, but there is also evidence from previous studies that microfracture of patellofemoral lesions results in inferior short-term outcome in an older population.36,37 Seeley et al. 34 noted the importance of evaluating also OCF to the distal femur. They reported a significant inferior clinical outcome score compared with patellar injuries in OCF involving the weightbearing surface of the lateral femoral condyle in adolescents. But they did not provide distinct long-term results for this group of patients after refixation. 34 In a recent retrospective study by Kang et al. 33 the clinical outcome of OCF in 43 patients was evaluated comparing excision of fragments with refixation. This study included patellar and distal femur lesions and reported significant better results for excision of fragments over a short-term follow up of period of 28 months, but only when OCF did not involve the weightbearing surface of either patellofemoral or tibiofemoral joint. But unlike to the present study it remains unclear if the included rim lesions outside the femoral weightbearing zone influenced the results in favor of excision, especially in a short-term follow-up.
When comparing the short-term results of those studies with the present results, it is likely that the advantage of refixation over formation with fibrocartilage becomes more apparent at mid-to long-term follow-up in a larger group of patients, which is strength of this study. The present results demonstrate significant better long-term outcome scores for refixation in the bearing zone independent of injury location. The high rate of revision surgery due to symptoms of osteoarthritis in case of debridement underlines the need for restoring a normal weightbearing area in both, the patellar and femoral surface even when refixation of OCF cannot be performed. Different cartilage restoration procedures have been proposed in the past for those injuries, including autografts, allografts, treatment with different scaffolds as well as regenerative treatments.22,25,28,38-40 Considering the young age of those patients, procedures with a low morbidity and good long-term results should be preferred. Arthroscopic treatment with matrix autologous chondrocyte implantation, for example, has recently shown significantly improved results of the newly formed tissue compared with microfracture at mid-term follow-up for patellar and trochlear cartilage lesions. 39
Furthermore, any cartilage restoration procedures should be combined with optimization of patellofemoral stability, since persistent instability is a known risk factor for patellofemoral osteoarthritis.9,10,20,35,41 Previous studies have shown significant reduction of redislocations after MPFL reconstruction in cases of mild trochlear dysplasia, whereas medial reefing has been shown to have high failure rate as demonstrated in our study.9,42
There are several limitations of this study that have to be considered: First, the study was conducted retrospectively, with the inherent limitations. The comparison of refixation and debridement is limited by the fact that different kinds of lesions were treated with different procedures and baseline data scores of patients were not available. This clearly produces a bias that is not resolvable since debridement of chondral lesions is done arthroscopically while refixation requires arthrotomy. Surgeon’s decision therefore could have been biased toward refixation of larger fragments. Furthermore, outcome was obtained by interview and clinical scores only. It remains unknown whether some fragments partially resolved after refixation due to initial trauma as described before. 14 In future investigations standardized MRI protocols should be used to confirm the clinical results. Also, the influence of recurrent dislocations on the clinical outcome should be further evaluated since prevalence of high-grade trochlea dysplasia might contribute to redislocation and worse clinical outcome.2,20,43 Finally the reintervention rate of 48% might have influenced the clinical results. Nevertheless, the presented results support the effort to try fragment refixation in order to achieve primary restoration of the chondral surface at an early stage with good clinical mid- to long-term outcome.
Conclusion
Refixation of OCF after lateral patella dislocation shows improved clinical outcome at mid- to long-term follow-up compared with debridement. Therefore, effort to try fragment refixation is recommended. Redislocation rate is high without proper restoration of patellofemoral instability.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s note
Philipp Schuster is also affiliated with Department of Orthopedics and Traumatology Klinikum Nuremberg, Paracelsus Private Medical University Nuremberg, Nuremberg, Germany.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was approved by the competent research ethics board of our institution (IRB-2018-008).
Informed Consent
All patients gave their written informed consent to the study.
Trial Registration
Not applicable.