
Abstract
Objective
To evaluate clinical, functional, and radiographic outcomes of patients who underwent bipolar osteochondral allograft transplantation (OCAT) of the patellofemoral joint (PFJ).
Design
Prospectively collected data on 18 knees who underwent fresh osteochondral allograft transplantation of the patella and trochlea by a single surgeon were reviewed. Inclusion criteria were: high-grade chondral lesions of PFJ (5 knees), or recurrent patella dislocations with trochlear dysplasia and chondral injury to the patella and/or trochlea (13 knees). Functional scores were obtained preoperatively and at follow-up appointments included Knee injury and Osteoarthritis Outcome Score (KOOS), International Knee Documentation Committee (IKDC), Oxford, Cincinnati, Tenger-Lysholm, visual analogue scale (VAS)–pain, and Single Assessment Numeric Evaluation (SANE). Grafts were also evaluated using Osteochondral Allograft MRI Scoring System (OCAMRISS).
Results
Three patients were lost to follow-up, leaving 4 knees in group 1, and 11 knees in group 2. Average age was 28.9 years (range 16-52 years). The average follow-up was 33.2 months (range 12-64 months). There was significant improvement of KOOS (from 38.7 to 83.1), IKDC (from 28.2 to 76.6), Tegner-Lysholm (from 38.3 to 88.3), Oxford (from 22.7 to 42.9), Cincinnati (from 35.1 to 83.6), VAS (from 71 to 17.9.), and SANE (from 43.3 to 83) (P < 0.0001). The OCAMRISS score for patella was 2.23 and for trochlea 4.69. There were no revisions or conversions to arthroplasty
Conclusion
Bipolar OCAT of the patella and trochlea provide significant improvement in functional outcomes, relief from pain, activity level, and prevent recurrent instability.
Keywords
Introduction
Cartilage defects of the knee are a common finding on arthroscopy occurring in 60% to 66% of cases,1,2 and can be found in 36% of asymptomatic cases without concomitant injuries.3,4 Treatments for these lesions vary from microfracture, autologous chondrocyte implantation (ACI), osteochondral allografts (OCA), and arthroplasty.5-8 OCAs are often the treatment of choice for lesions >2 cm2 in area2,6,9 or with more advanced arthrtitis, 10 and have demonstrated good to excellent results in treating defects of the femoral condyles.11-16 OCAs are now the treatment of choice for younger more active patients 2 and has been successful even in pediatric patients.17,18 Patients have even been able to return to athletics following an OCA.19,20
The patellofemoral joint, however, has proven to be more challenging with higher failure rates.2,11,21-24 This is often attributed to the high joint forces that occur across this joint. Patellofemoral lesions have been studied in terms ACI, osteochondral autografts (OAT), and microfracture.8,25 To date, there have been limited studies with small populations that focused solely on the outcomes of OCAs to the patella or patellofemoral joint.22,25-28 The results of these studies have shown promise with survival rates as high as 78% at 10 years when unipolar. 27 Few authors have reported on combined OCAs to both the patella and trochlea, which have been shown to have an increased risk of failure.22,24,29,30 Giannini et al. 29 hypothesized that this may be due in part to underappreciated immunogenicity of the allografts, which has been supported by basic science reasearch.31-33 Others have argued that the size of the allograft tissue and mechanical factors lead to failure. 30
Patellofemoral instability is a source of these patellar and trochlear lesions, and the treatment of patellofemoral instability continues to be investigated. The biggest risk factors for recurrent patellar instability include trochlear dysplasia, patella alta, ligamentous stabilizers and abnormal limb geometries.34,35 The medial patellofemoral ligament is responsible for stabilization of the patella in the first 30° of flexion, then osseous anatomy and shape of the trochlea stabilizes the patella engages the trochlea. Bollier et al. 34 helped demonstrate the importance of trochlear morphology on patellofemoral instability. Despite advances in medial patellofemoral ligament reconstruction and tibial tubercle realignment, trochlear dysplasia remains a challenge and failing to address it is a primary reason for failure of patella-stabilizing procedures.36,37 Albee 9 was the first to address patellar instability by correcting trochlear dysplasia, and modern deepening trochleoplasty as described by Dejour and Le Coultre 38 has had some success. 39 However, these trochleoplasty techniques are noncongruent and nonanatomic with the patella and do not address preexisting chondral lesions from recurrent dislocations. Our series addressed trochlear dysplasia in patients with patellofemoral instability with bulk trochlear allograft transplantation from a donor with a normal trochlear groove to reconstruct the proximal trochlear morphology as well as resurfacing the entire patella with the same donor to provide a congruent, anatomic surface to the trochlear graft. We evaluated outcomes of the bipolar OCAs to the patellofemoral joint in terms of graft survival as well as patient outcome scores and radiographic assessment.
Methods and Materials
With institutional review board approval, we retrospectively reviewed prospectively gathered data on 18 knees in 17 patients for a minimum of 1 year follow-up who underwent osteochondral allograft transplantation to the patella and trochlea. Three patients were lost to follow-up. Inclusion criteria were 3 patients (4 knees) without trochlear dysplasia, with documented grade III or IV lesions of the patellofemoral joint, on magnetic resonance imaging (MRI) and diagnostic arthroscopy (patellofemoral arthritis) who declined to undergo a patellofemoral arthroplasty because they wanted to maintain a high activity level. The other 11 patients had trochlear dysplasia with patellofemoral instability and recurrent dislocations (more than 2 dislocations) with and chondral loss of the patella and/or trochlea.
Clinical Assessment
Primary outcomes were graft survival (defined as need for revision surgery or conversion to arthroplasty). Secondary outcomes included functional scores of Knee injury and Osteoarthritis Outcome Score (KOOS), 40 International Knee Documentation Committee (IKDC), 41 Oxford, 42 Cincinnati, 43 Tenger-Lysholm, 44 , viual analogue scale (VAS)–pain, 45 and Single Assessment Numeric Evaluation (SANE) 46 that were completed preoperatively and at routine follow-up appointments.
Radiographic Assessment
Preoperative standard bilateral anterior-posterior, Merchant, and true lateral radiographs were obtained. In patients with patellar instability, trochlear dysplasia was classified on the lateral radiograph according to the Dejour classification. 35 Lateral radiographs were also used to measure the Blackburne-Peel 47 and Cantons-Deschamps 48 ratios. MRIs were used to evaluate chondral injuries. tibial tuberosity–trochlear groove (TT-TG) distance 49 and tibial tubercle–posterior cruciate ligament (TT-PCL) 50 distances were measured as well. Patellar and trochlear grafts were also evaluated postoperatively using Osteochondral Allograft MRI Scoring System (OCAMRISS). 51
Graft
All grafts were obtained from Joint Restoration Foundation (Centennial, CO). The grafts are aseptically recovered and processed per American Association of Tissue Banks and Food and Drug Administration standards. Grafts are released for transplantation after a complete evaluation of the social history, medical record, serology testing, and microbial cultures. They must be negative for microbial growth on three separate cultures and do not undergo any sterilization to ensure maximization of chondrocyte viability. Grafts are stored at 1°C to 10°C, in a proprietary cartilage preservation storage media, which includes fetal bovine serum for up to 28 days from donor death. Garrity et al. 52 has shown this method helps maintain chondrocyte viability. All grafts were implanted prior to 28 days from time of passing of the donor.
Surgical Technique
The patients were placed in a supine position and underwent general anesthetic with preoperative regional nerve block for pain control. A midline incision was used and a lateral parapatellar arthrotomy was performed, leaving the medial sleeve of tissues intact for a medial patellofemoral ligament reconstruction (MPFL) with an allograft for patients with instability.
Trochlear Preparation in the Patient
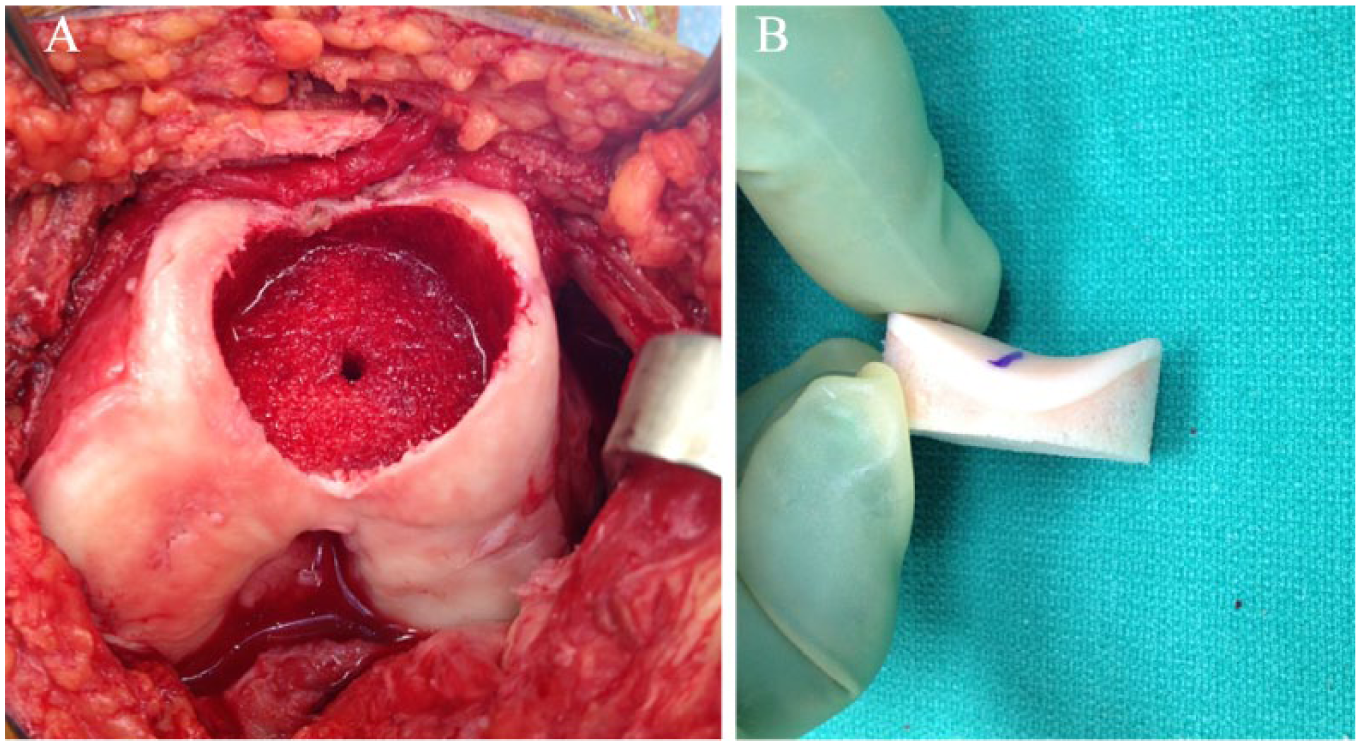
Cannulated trochlear sizing guides are used to cover the entire trochlea of the patient and determine the correct size/diameter. The cylindrical guide made two points of contact on the medial and lateral flares of the trochlea. The superior and inferior aspects of the guide were adjusted to determine the proper trajectory. Typically, the distance from the bottom of the guide to the articular surface should be the same at the superior and inferior aspects of the guide. In cases with trochlear dysplasia, the superior side of the guide should be placed as proximal on the trochlea as possible; essentially abutting the anterior femoral cortex and where the dysplasia is most pronounced. Once the guide is in the desired position, a guide pin is placed through it into the patient’s bone to secure the guide and determine the proper trajectory. A score is then used over the guide pin to cut into the cartilage for the intended trough creation. A triple reamer is used to create the socket ( Fig. 1A ). It is vital that in large diameter (35 mm) sockets, sequential reaming starting at 20 mm, followed by 22.5, 25, 27.5, 30 mm, and finally 35 mm (or desired size) to avoid the reamer from wobbling and creating an oval socket. The socket should be reamed until the 6 o’clock of the socket is 5- to 6-mm deep. A depth gauge is used to measure the height of the socket at 12, 3, 6, and 9 o’clock positions of the socket and recorded.
(
Trochlear Graft Preparation
The trochlear graft is secured in the graft station. The appropriate cannulated sizing guide (typically 35 mm and matching to the defect on the recipient knee) is then placed through the aiming guide of the graft station. The sizing guide should be oriented in the superior-inferior direction while maintaining 2 points of contact (the lateral and medial flares) and reproduce the same trajectory used in the patient. A coring reamer is used to harvest the cylindrical graft. If the reamer cannot be completely advanced, a small sagittal saw can be used to cut toward the coring line and remove the surrounding bone and cartilage piecemeal. The 4 points of measurement made in the defect of the patient’s trochlea are then measured in the donor plug ( Fig. 1B ) and a small sagittal saw is used to cut the excess bone from the plug, often 1 mm shorter than measured in defect to avoid the graft from remaining proud. The sharp edges of the plug are beveled (“bulleted”) to make insertion into the socket easier in the patient. The bone plug is thoroughly pulse-lavaged to remove immunogenic marrow elements from the graft. Leukocyte-poor platelet rich plasma or bone marrow aspirate concentrate from the patient can then be injected into the bone component of the plug and kept in the back table.
Patellar Preparation in the Patient
The patella is everted and held in a horizontal position (similar to a total knee arthroplasty) with two towel clamps. Calipers are used to measure the patellar height in order to reproduce it once the allograft is secured to the native bone. A sagittal saw is used to cut the articular side of the patient’s patella. A minimum of 12 mm of native bone was left behind in all cases ( Fig. 2 ).
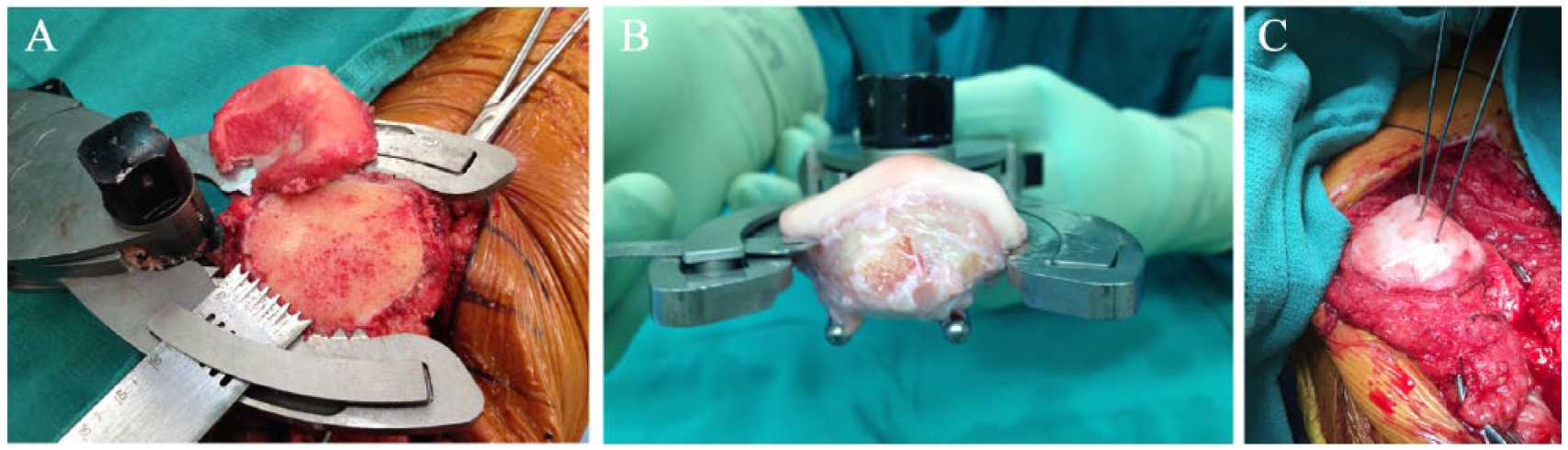
Preparation and fixation of the patellar component. (
Patellar Preparation in Donor
All soft tissue is sharply dissected off of the donor patella, including patellar tendon and quadriceps tendons, if still attached to the patella. The patellar height is measured with calipers. The patellar graft is then secured into a patellar clamp (DePuy, Warsaw, IN) and the appropriate height is confirmed with a metal ruler through the slots of the clamp. Care is taken to leave at least 2 mm of bone behind the articular surface of the donor patella. The patellar bone is thoroughly pulse lavaged as well.
Transplantation of Grafts
Trochlea
The trochlear socket in the patient is prepared by placing 5 cm3 of demineralized bone matrix putty in order to back fill the graft as it was cut 1 mm shorter than the depth of the socket. The trochlear graft is then placed into the socket and the tapered edges of the plug allow for initial temporary fixation to hold the graft in place. A tamp is then used and gently malleted to insert the graft into the socket. Care should be taken to do so evenly from all corners of the graft so it evenly enters the socket circumferentially. The most critical aspect is the 6 o’clock position of the graft, which should be flush with the native cartilage so the patella does not catch after deep flexion. Press fit excludes the need for fibrin glue or chondral darts to secure the graft. If the graft is felt too be unstable, headless compression screws can be used to achieve fixation of the graft.
Patella
Demineralized bone matrix putty is placed over the native patellar bone to make up for any irregularities in the cuts of the patellae and to ensure maximal bone-to-bone contact between native and donor patellar bone. The donor patella with the articular surface is placed onto the native patellar bone and held in place with a clamp. Three guide wires of a headless, compression screw system are then placed from the articular side of the patella at the median ridge (thickest portion of the patella) and advanced through the anterior surface of the native patellar bone. A cannulated drill is then placed over the guide wires one at a time and drilled proximal to the subchondral bone of the donor patella. The depth of the drill hole is measured and a headless compression screw is placed from an anterior to posterior direction of the patella, thus avoiding violation of the articular cartilage of the donor patella articular surface. The final fixation of the patella and trochlea are seen in Figure 3 . The screw placement and length are verified with fluoroscopy intraoperatively ( Fig. 4A ).
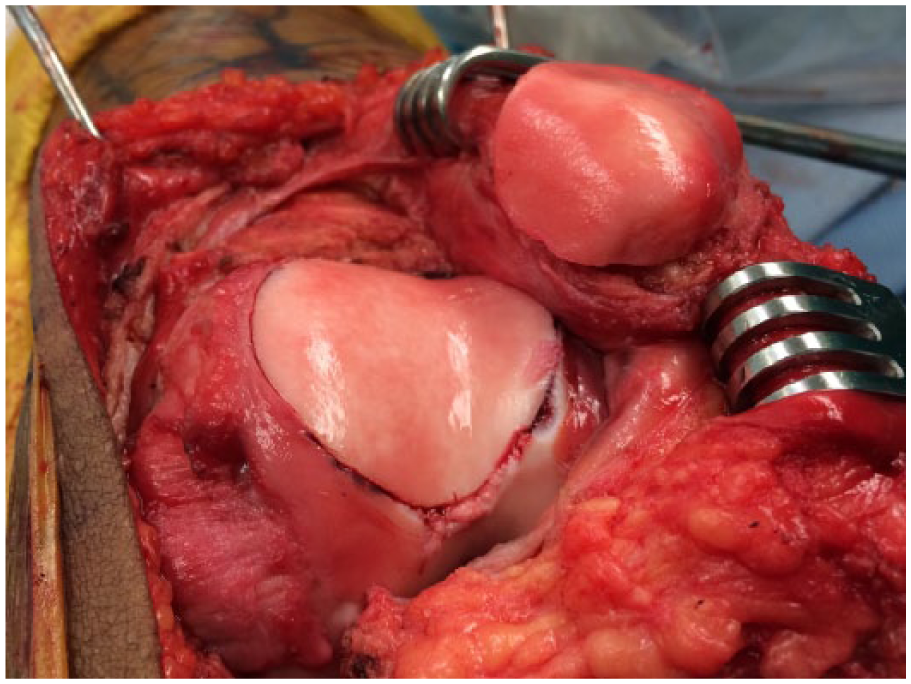
Final reconstruction demonstrating press-fit fixation of the trochlear graft and screw fixation of the patella from the anterior to posterior direction, thus not violating the patellar cartilage.
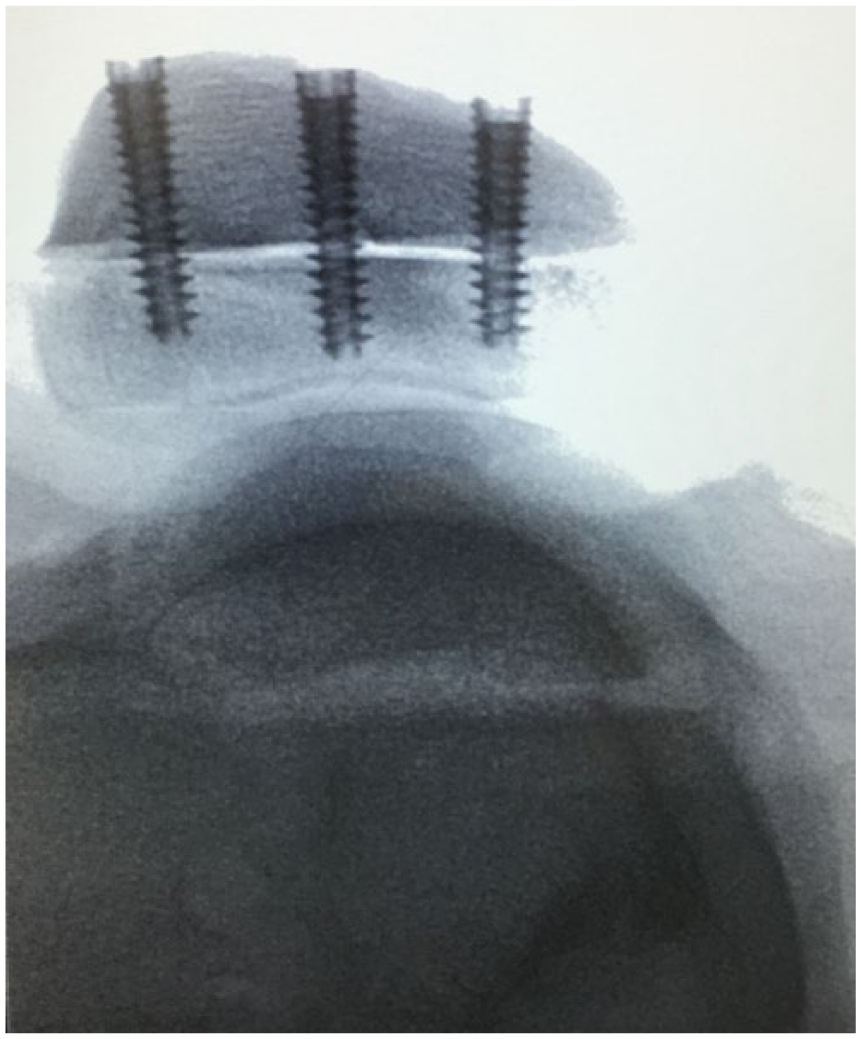
Intraoperative fluoroscopic radiograph confirming screw length.
Medial Patellofemoral Ligament Reconstruction
All patients with patellar instability also underwent an MPFL reconstruction using a gracilis allograft after closure of lateral arthrotomy. Layers II and III were isolated on the medial side and the graft was shuttled between those 2 layers without violation of the capsule. The origin of the MPFL 53 was identified and a 7-mm tunnel was reamed. The femoral origin was fixed with ACL TightRope button (Arthrex, Naples, FL) and a 6 × 25 mm BioComposite SwiveLock (Arthrex, Naples, FL) for additional fixation. The 2 free limbs of the grafts were sutured with No. 0 FiberWire suture (Arthrex, Naples, FL) to aid passage between the medial layers. Two 3.5 PEEK SwiveLock anchors (Arthrex, Naples, FL) loaded with No. 2 FiberWire are then placed into the superior half of the patient’s patellar bone and used to suture the graft and secure it to the patella. The graft was not placed into patellar tunnels to minimize risk of patella fracture.
Tibial Tubercle Osteotomy
One patient with severe patella alta required a tibial tubercle distalization. A 6-cm long sliver of bone was exposed distal to the patellar tendon insertion to the tubercle. A sagittal saw was used to make a 1-cm thick cut from the medial to lateral direction. A 1-cm wedge of bone was removed distally and the tubercle sliver was advanced distally and secured with 3 screws in lag fashion.
Postoperative Protocol
The patients are placed in a postoperative knee brace. They are kept nonweightbearing for 8 weeks. Immediate range of motion is initiated with a continuous passive motion machine for the first three weeks. No restriction is placed on range of motion. Isometric quadriceps strengthening is initiated on postoperative day 1. Closed chain exercises and strengthening are initiated at 8 weeks.
Statistics
The study population characteristics were summarized for all patients relative to their date of surgery. Descriptive statistics were performed on demographics, preoperative radiographic measures, and allograft measurements. OXFORD, KOOS, IKDC, Cincinnati, Tegner-Lysholm, and VAS scores were calculated pre- and postoperatively and compared within patients using paired t-tests or the non-parametric equivalent, Wilcoxon’s rank sum test, as appropriate. Statistical significance was defined at the 5% type I error rate and all hypothesis tests were 2-sided tests of the null hypothesis of no difference in mean scores before and after surgery. Normality was checked for all continuous variables using Anderson-Darling’s test
Results
Patient Demographics
The average age was 28.9 years (range 16-52 years). There were 12 males, and 2 females. The average follow up was 32.2 months (range 12-64 months). Four patients in the instability group, had OCA performed in other parts of the knee, including lateral femoral condyle (2 patients) and medial femoral condyle (2 patients). All patients with patellar instability underwent MPFL reconstruction. One patient with severe patella alta underwent tibial tubercle distalization.
Graft Information
The patellar and trochlear grafts were from the same donor to ensure a perfect match in congruency of the articular surfaces. The diameter of trochlear graft was 35 mm in all but 3 cases (20, 22.5, and 30 mm) with an average of 32.8 mm (8.45 cm2) (range 20-35 mm). Two trochlear grafts did require additional fixation with compression screws. These were from the early cases in the series when sequential reaming was not performed. None of the trochlear grafts required fixation if the recipient socket was sequentially reamed.
All patellar grafts were whole shell grafts and exact dimensions were not recorded in order to calculate area of patellar graft. The average patellar thickness of patients was 25.1 mm (range 16-29 mm) prior to osteotomy. The average patellar thickness of donors was 26.1 mm (range 22-29 mm). The average combined patellar thickness after fixation of graft to patient was 26.0 mm (range 22-31 mm). The patella required an average of 3.4 compression screws (range 3-5) for adequate fixation. Earlier in the series, 5 screws were used but eventually, 3 midline screws were found to be sufficient.
Clinical Outcomes
All 15 knees had graft survival at last follow-up. There were neither revision or plans for revisions nor conversion to arthroplasty. Functional outcomes are summarized in Table 1 . The Oxford knee scores improved from 22.7 (10.0-42.0) to 42.9 (25.0-48.0) (P < 0.0001). The KOOS scores improved from 38.7 (12.5-74.4) to 83.1(34.5-100) (P < 0.0001). The IKDC improved from 28.2 (11.5-54.0) to 76.6 (28.7-100) (P < 0.0001). The Tegner-Lysholm scores improved from 38.3 (2.0-72.0) to 88.3 (56-100) (P < 0.0001). The Cincinnati Knee scores went from 35.1 (8.0-71.0) to 83.6 (29.0-100) (P < 0.0001). The SANE improved from 43.3 (10-70) to 83 (50-100) (P < 0.0001). The VAS scores improved from 71 (30-100) to 17.9 (0-70) (P < 0.0001). No patients sustained patellar redislocation. One patient was on a division I college basketball team on full scholarship.
Pre- and Postoperative Outcome Scores.
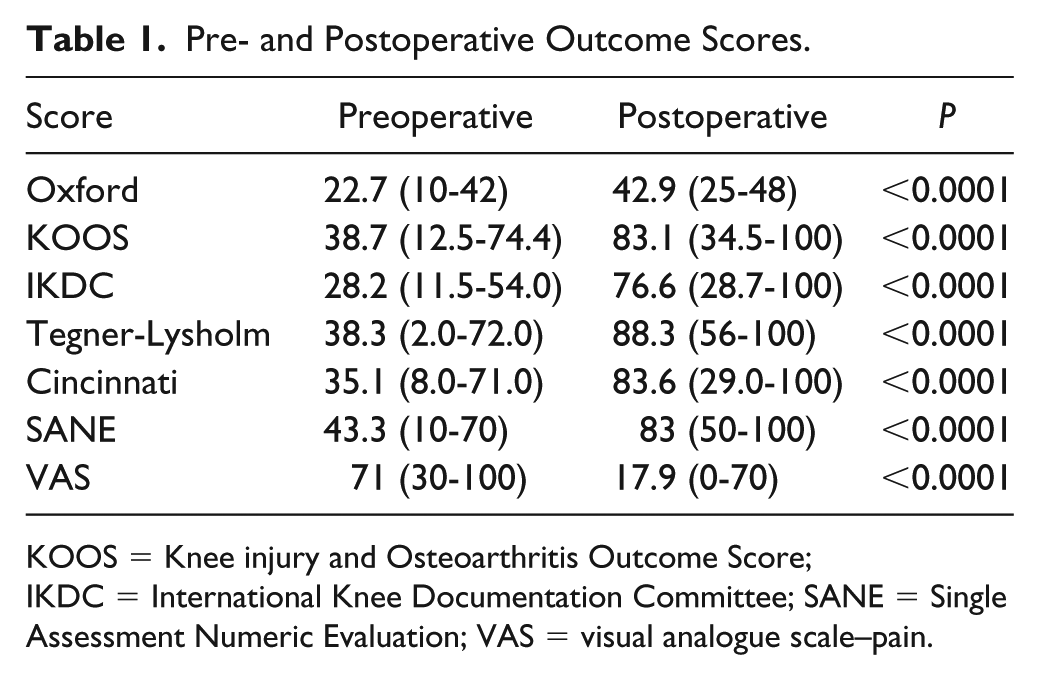
KOOS = Knee injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee; SANE = Single Assessment Numeric Evaluation; VAS = visual analogue scale–pain.
Imaging Studies
The degree of trochlear dysplasia amongst the patients included 5 type D, 1 type C, 1 type B, 1 type A, and 1 with no dysplasia. The mean Insall-Salvati ratio was 1.1 (range 0.8-1.6), Canton-Deschamps ratio was 1.1 (range 0.9-2.4), and Blackburn-Peel ratio was 1.1 (range 0.9-2.2). The mean TT-PCL was 23.7 mm (range 18.9-31.7) and the mean TT-TG was 15.9 mm (range 10.6-28.9).
Postoperative plain radiographs were obtained on all patients. In 2 patients, there was incomplete incorporation of the proximal portion of the donor patella (<10% of the donor patella). Both these patients underwent arthroscopies to have the superior screws removed to prevent damage to the trochlear graft ( Fig. 5A ).
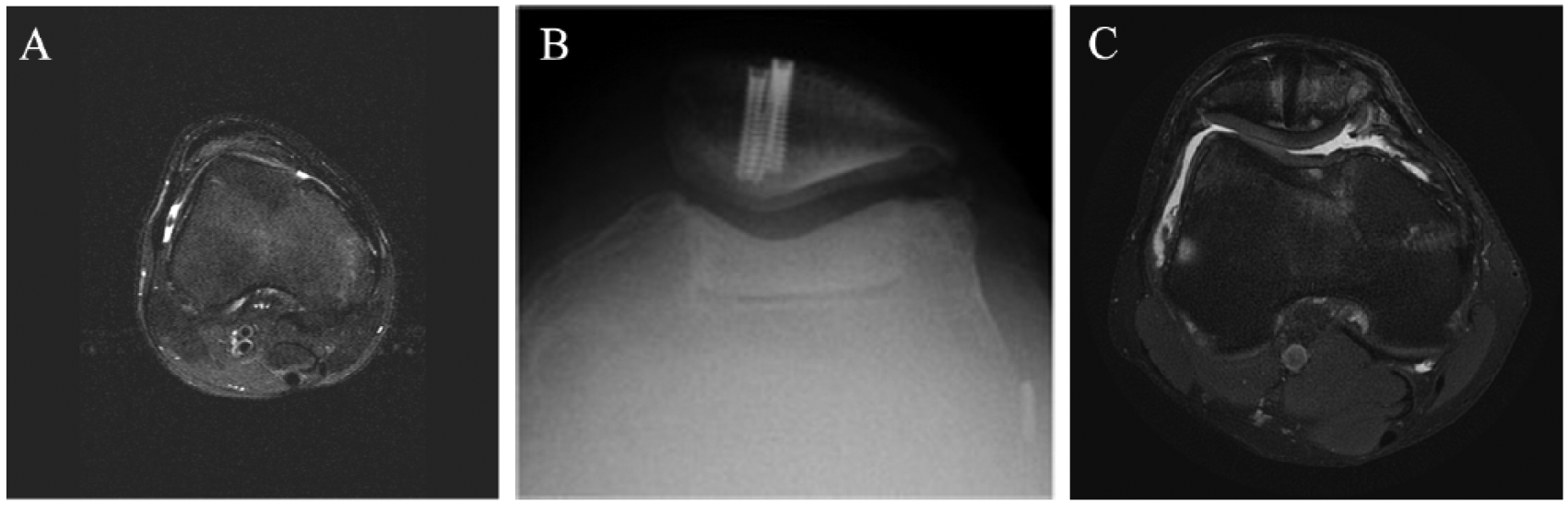
(
Postoperative MRI evaluation demonstrated good incorporation of the allografts based on the OCAMRISS grading system ( Fig. 5C ). The average OCAMRISS score was 3.46 (0-9). Patellar grafts had, on average, a lower (more favorable) score than the trochlear grafts (2.23 vs. 4.69, respectively).
Complications
Two patients required reoperations. One patient with Ehlers Danlos developed severe postoperative stiffness and required three arthroscopic lysis of adhesions. She also had incomplete incorporation of the donor patella with a prominent superior screw, which was removed. The other patient had pain in the superior aspect of the patella with deep squats. He was noted to have incomplete incorporation of the donor patella at the proximal patellar screw, which was also removed and resolved his symptoms.
Discussion
Numerous studies demonstrate survival rates of osteochondral allograft transplantation and functional improvements with short- to long-term follow-up.10,11,13,16-22,24,26,27,29,51,54-56 However, studies of bipolar OCA for the patellofemoral joint are few and are limited to less than 12 patients.22,24,30 Our study is the largest to date involving bipolar allografts of the patellofemoral joint. It is also the only study to date to use an osteochondral allograft to address trochlear dysplasia.
While most of our patients are at short- to mid-term follow-up (⩽5 years), we still have 100% graft survival. Overall osteochondral allografts of the knee have at least 85% survivorship at 5 years.13,16,21,26,27,54-56 Specific to patellofemoral OCAs, Jamali et al. 22 had a 67% graft survival at 10 years, but 4 of the 5 failures occurred within 4 years and 2 within 13 months of the primary surgery. Spak et al. 24 had 11 patients with 14 bipolar or patellar OCAs, of which 6 failed. Of the failures, 2 occurred within the first 2 years of the study. Meric et al. 30 have also reported on 14 bipolar patellofemoral OCAs with an overall survival of 64% at 5 years. While our results are early, we feel this bodes well for graft survival.
In terms of graft integration, our OCAMARISS scores were low (favorable). OCAMARISS is designed to evaluate cartilage graft integration and has moderate correlation with IKDC scores, 51 unfortunately, discerning where these scores correlate in terms excellent, good, fair, and bad graft integration is difficult to determine.
Our patients had significant functional improvements similar to what has been seen in previous knee OCA studies. On the KOOS evaluation, patients improved from 38.7 to 83.1. Krych et al. 19 saw improvement in the activities of daily living (ADL) KOOS from 62 ± 15.96 to 82.82 ± 14.18. 19 Similar to our results improvements across all KOOS subcategories, including symptoms pain, ADL, sport, and quality of life have occurred after OCA surgery.13,54 Our IKDC scores 28.2 preoperatively to 76.6 postoperatively demonstrates a significant improvement in terms of pain and function that parallels and often exceeds previous studies.11,13,15,18,19,26,27,54,56 An improvement of the IKDC score of greater then 40 points has only been seen in one previous OCA study. 54 It is also superior to the average improvement (37.1 to 64.3) seen in the systematic review by Chahal et al. 11 These studies have predominantly been mixed studies of unipolar condylar OCA grafts, which has previously shown to have superior results.2,11,21-24
Lysholm-Tegner scores 38.3 to 83.6 were superior to previous studies that analyzed all OCA allografts with a mean improvement of approximately 30 points.11,13 Torga Spak et al., 24 however, with a focus on patella and patellofemoral grafts had similar excellent outcomes with improvement from 27 to 80. 24 The Oxford score, which evaluates a patient’s pain and ability to perform tasks of daily life, has not been previously used to analyze patient outcomes in OCA interventions. Our results demonstrate improvement from moderate to severe arthritic symptoms to near normal knee functions 42 with postoperative mean of 42.9 out of 48 possible points. Pain was also significantly reduced from 71 to 17.9. Eight patients had zero pain at the last follow-up.
In comparison with other surgical techniques currently used to address patellofemoral chondral defects, our study demonstrates superior outcomes in the short term. Two studies on microfracture demonstrated improvement of Lysholm score of 50.1 to 85.2 57 and 59 to 89. 58 Although these scores reflect interventions to all areas of the knee, these two studies had large groups of patellofemoral lesions. Our data show superior results as our patients on average, had lower (worst) preoperative scores. Osteochondral autograft transplantation has also had success with improvement of the Lysholm score of 57 to 81 59 and 74 to 95, 60 but both these studies were isolated patellar lesions with grafts smaller than 2.5 cm2. Nho et al. 61 also demonstrated similar improvements in terms of IKDC scores (47.2 to 74.4) compared with our results (28.2 to 76.6). Bipolar and larger sized grafts are often risk factors for increased failure and worse outcomes.25,30 ACI has been well studied, and studies of the patellofemoral joint demonstrates improvements of Lysholm score of 56 to 86, 62 while another demonstrated improvements in IKDC scores of 38.1 to 76.7. 63 Although these studies were similar in that additional soft tissue procedures were performed, they remain unipolar interventions, and are often combined with tibial tubercle anteriorization to offload the patellofemoral compartment. Our results were even superior to patellofemoral arthroplasty, as Willekens et al. 28 only improved from 50.5 to 73.2 on the KOOS score. Our results demonstrate that bipolar OCAs to the patellofemoral joint provide equal and sometimes superior functional outcomes in the short term compared with other chondral salvage procedures despite historically being higher risk for failures.
With no dislocations in our cohort at time of last follow-up, our intervention shows promise in treating patellar instability in patients with trochlear dysplasia. Patellar instability is multifactorial 35 and addressing these factors can increase success in preventing recurrent dislocations. Hopper et al. 36 demonstrated treating instability in isolation when multiple factors are present will lead to higher failure rates. A recent review reaffirmed a multifaceted approach to patellar instability. While MPFL reconstruction in isolation and trochleoplasty with extensor mechanism balancing had similar functional outcomes, the group receiving the trochleoplasty and soft tissue procedures had lower postoperative dislocations. 64 Deepening trochleoplasty, however, does not address preexisting chondral lesions like OCAs can. Our results not only give credence to OCAs successfully treating patellofemoral chondral lesion but also as an alternative method of treating recurrent patellar instability in patients with (severe) trochlear dysplasia.
In our study, there was only one patient with severe patella alta requiring tibial tubercle distalization. An anteromedialization was not performed in our series to isolate the effect of trochlear reconstruction with an OCA, even in patients with an increased TT-TG or TT-PCL. The average combined patellar thickness after fixation of graft to patient was 26.0 mm, similar to the patients’ native thickness (25.1 mm). Re-creating the patient’s natural patellar thickness ensures no changes in the fulcrum of the extensor mechanism and increasing loads across the joint.
Our current study has several strengths and weaknesses. Our study is a small cohort in comparisons with other OCA studies. It is, however, the largest cohort of patients in a study focused solely on the patellofemoral joint, and the only study to have all bipolar allografts. We included numerous functional outcomes scores that can be compared with past and future studies. This is crucial as previous studies best summarized by Meric et al., 30 Assenmacher et al., 21 and Chahal et al. 11 demonstrate that most groups pooled their data from allografts to all locations of the knee. Our study allows analysis of the outcomes in isolation to the patellofemoral joint, which allows better comparison to other OCA studies. In terms of weaknesses, our study is retrospective in nature, though all data was collected prospectively. Our follow up is only short to mid-term and it is important to continue observation for long-term graft survivorship and functional outcomes. As mentioned previously, studies have shown many failures of OCAs to the patellofemoral joint occurred within the first 2 years.22,24 With continued follow-up, our goal will be to examine if our graft survival parallels the results of Jamali et al. 22 or will it be more comparable to unipolar grafts to the condyle.
Conclusion
Patellofemoral chondral lesions are a common finding in the setting of instability and arthritis and are a major source of pain. Previous studies have demonstrated the patellofemoral joint has an increased risk of failure for osteochondral allografts. Our short-term results demonstrate that bipolar OCAs to the patellofemoral joint can provide excellent outcomes comparable to unipolar grafts to the condyle. Furthermore, there is promise of OCAs in conjunction with soft tissue procedures being a successful treatment for patients with recurrent patellar instability with trochlear dysplasia and chondral injury. Further follow-up will be necessary to evaluate overall long term survival of grafts.
Footnotes
Authors’ Note
This investigation was carried out at Kaiser Permanente Southern California, Department of Orthopaedic Surgery, Baldwin Park, CA.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Raffy Mirzayan receives or has received honorarium from Arthrex; research support from Arthrex and Joint Restoration Foundation; royalties from Thieme and Wolters-Kluwer; and is an associate editor of the American Journal of Orthopaedics.
Ethical Approval
Ethical approval for this study was obtained from Kaiser Permanente Southern California Institutional Review Board (approval #10595).
Informed Consent
Informed consent was not sought for the present study because it was retrospective in nature and was not required by our Institutional Review Board.
Trial Registration
Not applicable.