
Abstract
Objective
The paediatric knee is prone to pure chondral shear-off lesions due to the developing osteochondral unit. Refixation of the chondral fragment is commonly done using metalwork or absorbable biomaterials. Both fixation methods come with biomaterial-related drawbacks. Earlier work on chondral allografts for cartilage repair in adults has shown successful osteochondral integration when the chondral allograft is treated with multiple incisions and then glued to the subchondral bone using fibrin glue. This is commonly referred to as the “hedgehog technique.” This study investigates the feasibility of a modification of the hedgehog technique in autologous cartilage to repair shear-off lesions in children.
Design
Three consecutive patients (aged 11, 12, and 14 years) with shear-off chondral fragments of 2, 5, and 8 cm2 were treated using this modified hedgehog technique. The calcified side of the chondral fragments were multiply incised and trimmed obliquely for an interlocking fit in the defect site. Fibrin glue and, if indicated sutures, were applied to fix the fragment to the defect. In 1 patient, an anterior cruciate ligament (ACL) repair was also performed. Patients were evaluated clinically and by magnetic resonance imaging (MRI) up to 12 months postoperatively.
Results
Twelve months after surgery, all patients reported no pain and showed complete return to sport and full range of motion. MRI showed no signs of fragment loosening.
Conclusions
The modified hedgehog technique is a feasible treatment option to repair pure chondral shear-off lesions in the paediatric knee. This was the first time this technique was used in autografting.
Introduction
Traumatic osteochondral fractures and osteochondritis dissecans (OCD) are among the most commonly encountered orthopedic pathologies in pediatric and adolescent knees.1-3 Fortunately, osteochondral fragments can be surgically reattached yielding good results.4,5 This technique relies mainly on osseointegration between autologous bone-to-bone tissue, similar to the osteochondral autograft transfer system (OATS) technique.
6
The matter becomes more complicated when the fragment consists solely of cartilage with no, or minimal attached bone. Regrettably, damaged cartilage has limited spontaneous self-repair, even in these young individuals,
3
and if left untreated cartilage defects can propagate and eventually lead to osteoarthritis.
7
Pure chondral defects in young individuals can result from shear-off trauma
5
or from type 3 OCD lesions.
8
Particularly children are prone to shear-forces due to their developing osteochondral unit.
1
These shear-forces can lead to delamination of cartilage from the subchondral bone leaving the developing calcified cartilage layer attached to the loose fragment.
1
It is not completely understood if, and how, the reparative capacities between grade 3 OCD lesions and shear-off traumas differ,
5
but often the same therapies are used.4,5,8 Therapies for shear-off traumas range from fragment removal and debridement to resurfacing using OATS or allografting, up to ideally restoring the native joint surface by refixation of the chondral fragment.
5
The idea of transplanting pure chondral tissue onto the subchondral bone is not new but has been considered ineffective on the notion that cartilage is passive and indifferent.
9
Refixation techniques often employ metal pins or screws for initial stability, or more recently, degradable biomaterials to overcome the need for additional removal procedures.4,5,8 For instance, darts were used for the refixation of pure chondral fragments which resulted in reasonable results.
10
These darts are composed of stiff and slow degrading poly-
Bardos et al. performed a preclinical study with 9-month old pigs 19 and a clinical study in adults 9 in which a method is described for the treatment of cartilage defects using pure chondral allografts. As opposed to previously described methods, this technique does not require additional fixation biomaterials. Multiple incisions were made in the deep and intermediate zone of a chondral allograft on the side facing the subchondral bone. 19 The intact superficial layer was confirmed histologically. 19 Theoretically, incising the deep cartilage zones greatly increases the integrational surface, provides mobility for the chondrocytes and allows easier access for bone marrow–derived stem cells. 19 Sparing the superficial zones preserves the tensile strength of the collagen fibers and the reservoir of progenitor cells. 19 The typical appearance of the osseous side after this modification has led to the name “hedgehog technique.” 19 Finally, the allograft was secured in the defect site by sutures and sealed using fibrin glue. 19 Both studies showed satisfying results,9,19 even when compared with autologous chondrocyte implantation (ACI). 19
We modified the hedgehog technique to reattach shear-off chondral fragments in 3 pediatric cases. A critical step of this modification is providing initial mechanical stability. This is obtained by trimming the edges of both the shear-off fragment and the defect site; thereby creating oblique, interlocking shoulders. The major prerequisite for this step is that the fragment is larger than the defect site. It is well-known that cartilage swells due to increased water uptake when the integrity of its collagen network and bone plate is disrupted. 20 As a proof of concept, first an ex vivo experiment was set up to investigate if this swelling would be sufficient to allow for modification. Subsequently, the modified hedgehog technique was applied in 3 children. These patients were followed for 1 year for clinical evaluation and MRI.
Methods
Ex Vivo Swelling Tests
Fresh osteochondral resections of 3 patients undergoing total knee arthroplasty (local ethical approval 2017-0183), aged 41, 52, and 64 years, were collected. Seven pure chondral cylindrical explants measuring 6 mm in diameter were punched out from Outerbridge 0-1 areas on the medial femoral condyle. Seven similar-sized chondral explants were obtained from 3 young sheep (age: 20 months) in order to compensate for potential loss of osmotically active proteoglycans in the human osteoarthritic cartilage. 21 NaCl 11.6 μL 5M was dissolved per mL Dulbecco’s modified Eagle’s Medium to mimic the synovial fluid osmolarity of 400 mmol/kg. 22 Explants were placed in this hypertonic fluid at 37°C directly after harvest. High-quality photographs (Nikon D5600, Nikon micro lens 105 mm fixed distance) were obtained at 5 minutes, 3 hours, and 24 hours. Synedra view software (Synedra GmbH, Austria) was calibrated and subsequently used to analyze the surface area of the explants over time. Two observers did the measurements. The swelling was assessed using the paired-samples T-Test SPSS 23 (IBM Analytics, Armonk, NY, USA).
Subjects
This study was conducted in accordance with the World Medical Association Declaration of Helsinki. All participants and their caretakers provided oral and written informed consent. The local ethics committee approved the study. Demographics of the subjects are shown in Table 1 .
Demographics of the 3 Cases.
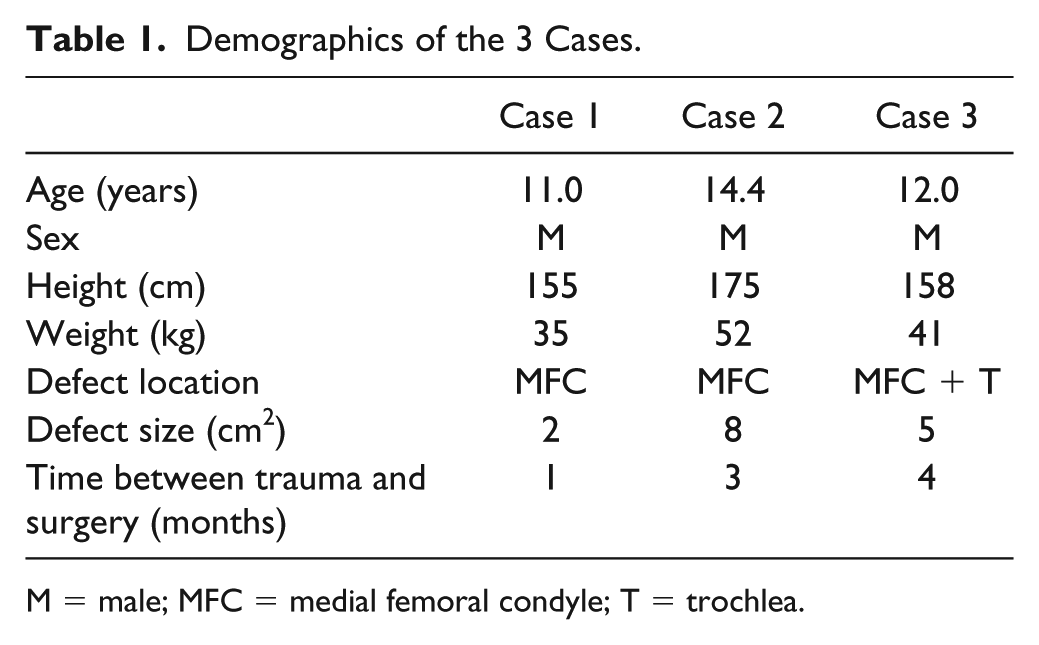
M = male; MFC = medial femoral condyle; T = trochlea.
Case 1
An 11-year-old boy presented to our clinic complaining of pain in his right knee 3 days after sustaining an injury while playing soccer. Physical examination revealed effusion of his right knee and an extension deficit of 10° to 20°. Tests for ligamentous or meniscal injury were negative. Conventional radiographs of the knee did not show any abnormalities. MRI showed an interruption in the cartilage covering the medial side of the medial femoral condyle ( Fig. 1 ). The missing shear-off fragment was situated on the ventral side of the knee between the medial femoral condyle and the tibial plateau. Further findings included bone bruise of the medial femoral condyle and extensive effusion. No abnormalities of the menisci and ligamentous structures were found.
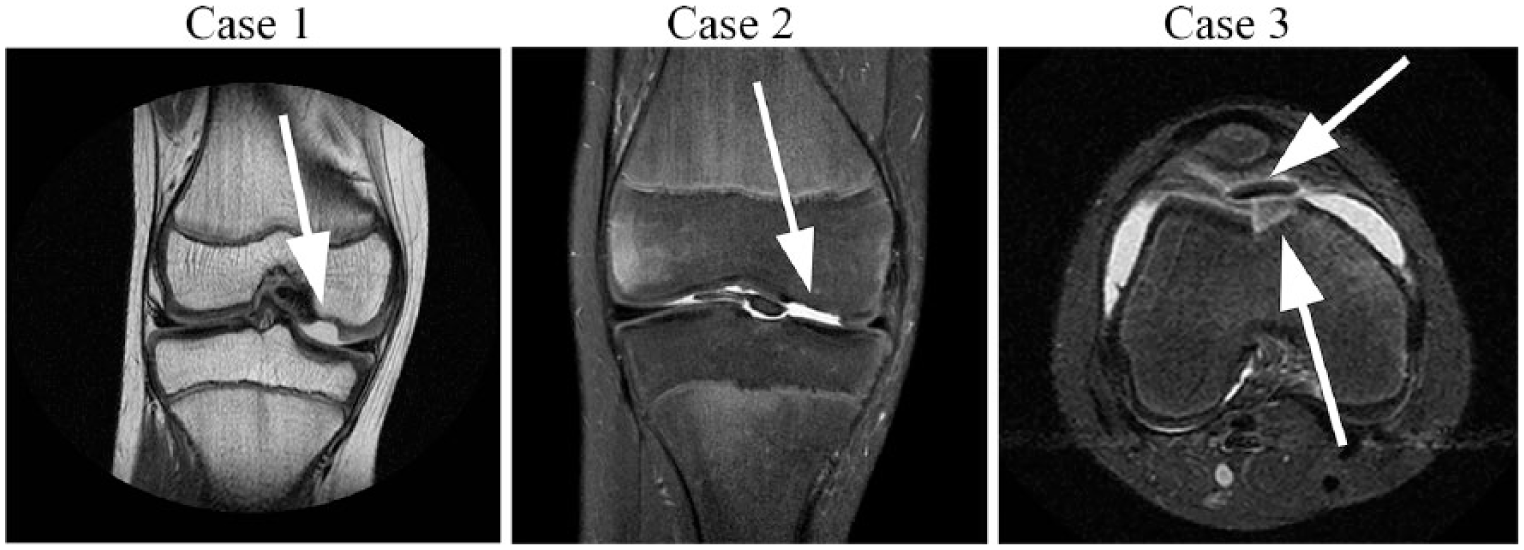
Preoperative magnetic resonance imaging. Case 1: depicted as a proton density weighted coronal section showing a cartilage defect (2 cm2, white arrow) in the medial femoral condyle. Case 2: depicted as spectral presaturation with inversion recovery coronal section showing a chondral defect on the medial femoral condyle (8 cm2, white arrow). Case 3: depicted as a short tau inversion recovery axial section showing a cartilage defect (5 cm2, lower white arrow) in the junction between the medial facet of the trochlea and the medial femoral condyle. Note the shear-off fragment (upper white arrow) that is larger in diameter than the defect site.
Case 2
A 14-year-old boy was referred to our clinic after suffering from a soccer trauma. He was complaining of pain and instability of his right knee. Physical examination revealed joint effusion and a positive anterior drawer and pivot shift test. The MRI showed an anterior cruciate ligament (ACL) rupture and a large chondral defect of his right medial femoral condyle ( Fig. 1 ). The shear-off fragment ( Fig. 2 ) was situated in the infrapatellar recesses.
Large shear-off chondral defect of case 2. (
Case 3
A 12-year-old boy presented to our clinic complaining of swelling and locking of his right knee after suffering a rotational trauma whilst playing soccer. Physical examination showed joint effusion, an extension deficit of 5° and no clues for ligamentous injuries. MRI revealed a chondral lesion of the junction between the medial facet of the trochlea and the medial femoral condyle ( Fig. 1 ). No abnormalities of the patella, menisci, cruciate, or ligamentous structures were noted.
Surgical Technique
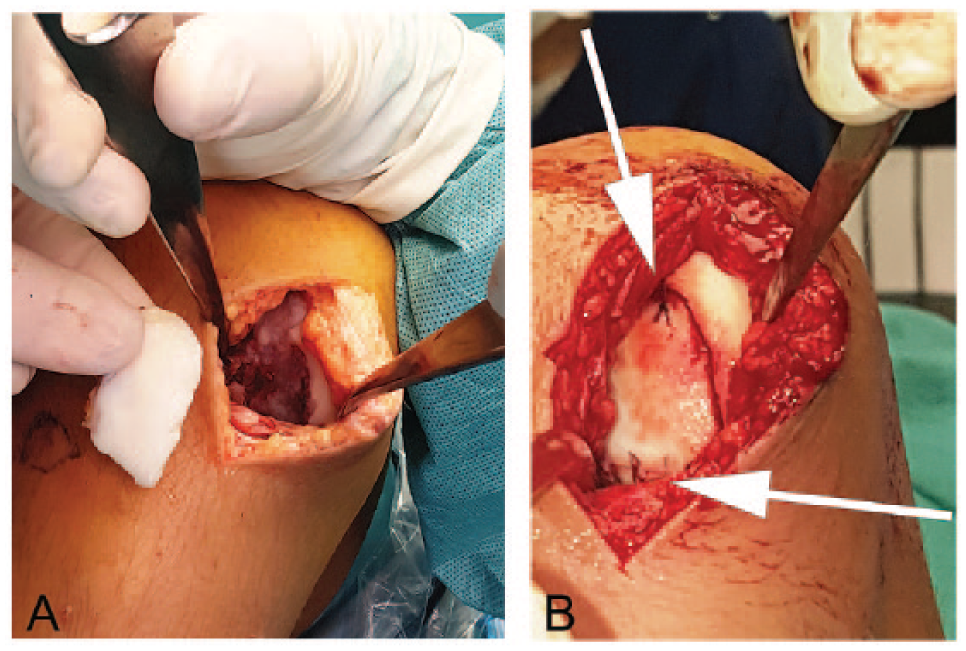
All surgeries were performed by the senior author (PJE). During the arthroscopy, the defect site was inspected and the chondral fragment was identified. Via an arthrotomy, the fragment was pulled out of the joint and placed in Ringers lactate solution to prevent deterioration while awaiting further processing ( Fig. 4A and B ). 23 The defect site was then abraded using a small surgical curette, removing fibrous tissue. The bone was abraded until bleeding of the bone was affected. Then, the defect rim was trimmed using a small surgical knife (No. 15 blade) to create oblique 60° to 80° shoulders ( Fig. 3 ). In order to further contribute to a stable interlocking of the shear-off fragment, chisels were used to create sharp 60° to 80° angles at the cartilage-bone transition of the defect ( Fig. 3 ).
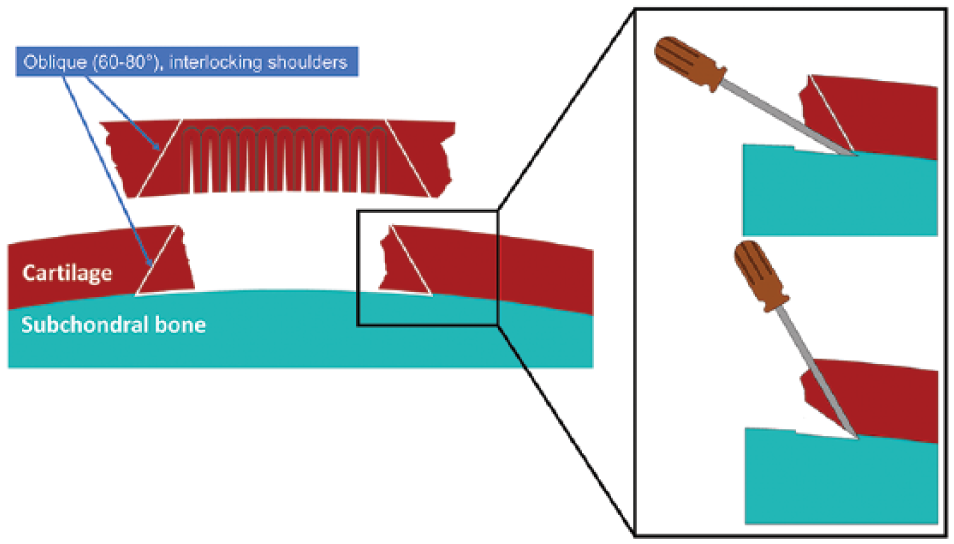
Schematic overview of surgical technique. Swelling of the shear-off fragment allows trimming of the edges in an approximately 60° to 80° angle of both the edges of the fragment as well as the defect, creating an interlocking match. The fibrous tissue is removed from the subchondral bone using a curette exposing vital, slightly bleeding subchondral bone, ultimately placing the fragment flush or slightly recessed to the surrounding cartilage. Magnification: For a proper press-fit fixation of the fragment, it is important to create the sharp angle in the bottom parts using a small chisel.
The shear-off fragment was then processed. First, the edges were trimmed in order to create a 60° to 80° angle and to fit the fragment in the defect site ( Fig. 3 ). Macroscopically and on palpation the osseous side of the fragment appeared hard which is in line with the presence of the calcified layer after shear-off trauma in children. 1 Therefore, instead of using an automated device,9,19 multiple incisions were meticulously performed freehand spaced approximately 1 mm apart ( Fig. 4C and D ). Subsequently, the debrided defect site was filled with fibrin glue (Tissucol, Baxter, the Netherlands) ( Fig. 4E ), and the fragment was placed back to its original position ( Fig. 4F ). Fibrin glue was also applied between the adjacent cartilage and the fragment. Removal of fibrous tissue on both the calcified part of the shear-off fragment as well as the subchondral bone of the defect led to a flush or slightly recessed press-fit position of the graft ( Fig. 2B ). In case 2, biodegradable Vicryl 5.0 sutures were used to secure the processed fragment in its position ( Fig. 2B ). The fresh construct was tested by several flexion-extension iterations before closing the wound. For case 2, the modified hedgehog autografting was performed directly after the ACL reconstruction.
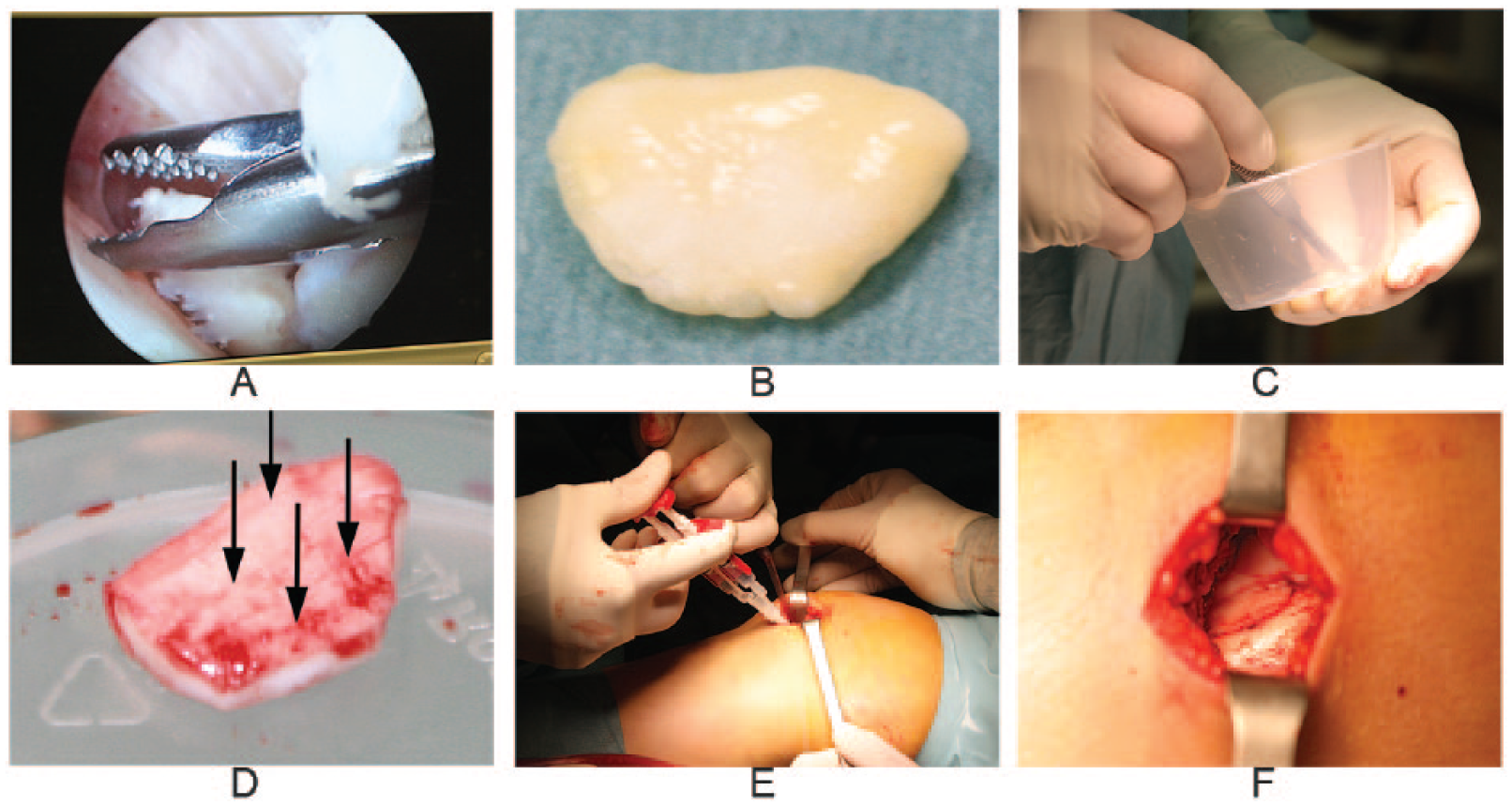
Intraoperative steps of the modified hedgehog autografting technique using case 3 as example. (
Rehabilitation Protocol
Early-stage rehabilitation was initiated by 2 weeks nonweightbearing with the knee fully extended in an adjustable hinged brace, followed by incremental steps of 25%, 50%, and 100% weightbearing and simultaneously 30° and 60° flexion followed by full range of motion in a 8 week period. This protocol was based on the fast tibiofemoral rehabilitation of the ACI protocol by Hambly et al. 24 Next, from 8 to 12 weeks, patients were allowed for gradual increases in training load and volume under physiotherapist supervision. After 12 weeks, patients were allowed to gradually increase sports activities.
Magnetic Resonance Imaging
MRI pulse sequence protocols were applied for the 1.0 T dedicated peripheral MRI system (OrthOne, ONI INC., Wilmington, MA, USA). Subjects were seated with their knee extended and centered in the circumferential extremity coil. Fast spin echo proton density weighted (PDW) T1, and short tau inversion recovery (STIR) T1 sequences were obtained. MR images were obtained approximately 3 and 12 months postoperatively and evaluated by an experienced musculoskeletal radiologist (DL). The images were examined for fragment delamination and morphology, displacement of the fragment and for interface gaps. Both the signal intensity of the cartilage and the subchondral bone were evaluated.
Clinical Assessment
All patients were seen after 2 weeks for wound inspection and at 3 and 12 months postoperatively. Patients were asked for pain, activities of daily living, sports activity and the presence of any restriction. A standard physical examination was performed at the outpatient clinic.
Results
Ex Vivo Swelling Test
After 24 hours, human cartilage explants increased 7% ±7 % (mean ± SD) in surface area (P = 0.06), whereas the caprine cartilage increased 54% ± 34% (mean ± SD) in surface area (P = 0.03). Most of the swelling took place in the first 3 hours (4% and 48%, respectively) after which it plateaued ( Fig. 5 ). Interobserver agreement was excellent with a Cronbach alpha intraclass correlation of 0.897. For the smallest cartilage fragment of 2 cm2, 1 mm trimming translates to 26% swelling, which was considered achievable in the 3 pediatric cases.
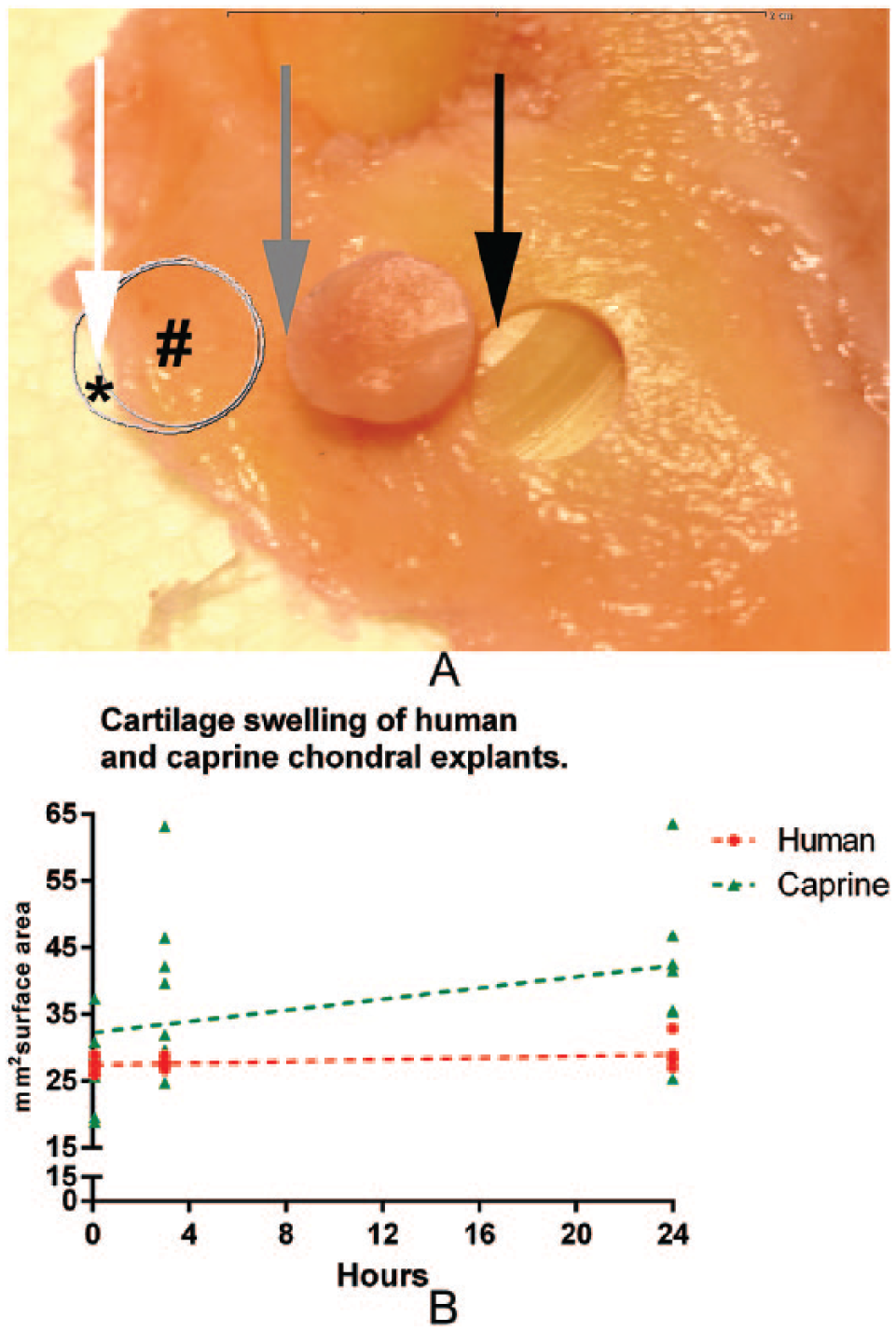
Cartilage swelling test. (
Surgery
No intra- or postoperative complications were observed. The articulating and calcified cartilage layer could easily be identified on all fragments by visual inspection and probing. None of the loose fragments showed any macroscopic evidence of residual bone. All fragments had a good fit in the defect site after trimming with no gaps observed between fragment and adjacent cartilage.
Magnetic Resonance Imaging
None of the subjects showed fragment delamination, displacement, large interface gaps, osteophytes or subchondral cysts one year postoperatively ( Fig. 6 ). At 3 months postoperatively in cases 2 and 3, MR images demonstrated normal cartilage signal intensity of the implanted shear-off fragment. Case 1 showed mild hyperintense signal of the fragment compared with the surrounding cartilage, persistent after 12 months. Cases 2 and 3 demonstrated a mild irregular cartilage fragment surface at 3-month follow-up. At 12-month follow-up, case 3 showed a smooth fragment surface, the mild irregularity of the cartilage persisted in case 2. Case 2 demonstrated mild depression of the fragment of about 1 mm at 3- and 12-month follow-up. Edematous changes in the subchondral bone were visible at the preoperative and first postoperative MRI in all 3 cases, which decreased and completely normalized after 12 months. A small sclerotic band was visible in the subchondral bone in all cases at the first postoperative MRI, and only case 1 demonstrated this mild sclerosis after 1 year. The thickness of the cartilage did not change over time.
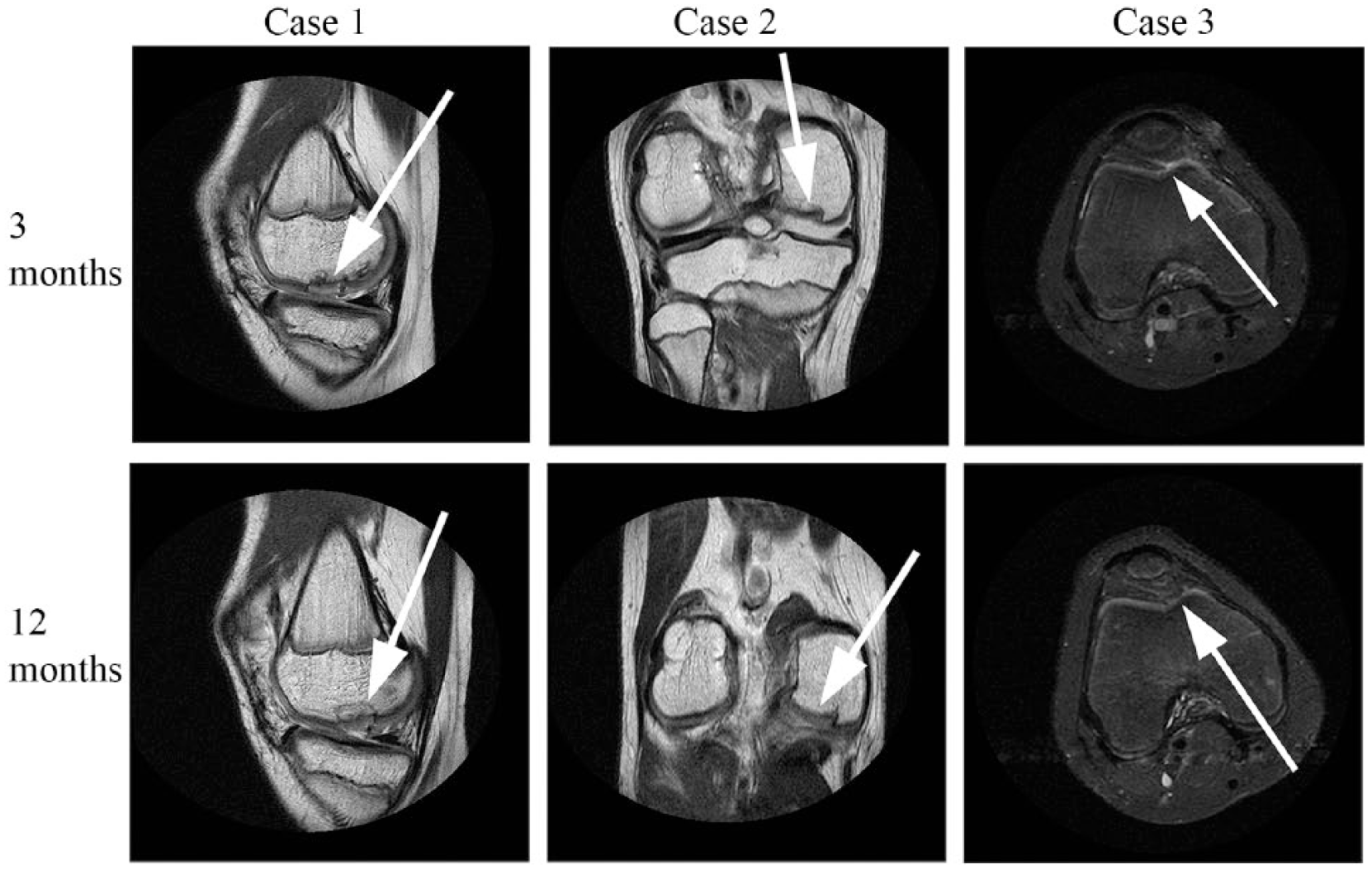
Postoperative magnetic resonance images of the 3 cases in the best representative sequence. Case 1 is depicted as a proton density weighted sagittal section showing good osteochondral integrity at 3 and 12 months (white arrows). Case 2 is depicted as proton density weighted coronal section showing good osteochondral integrity at 3 and 12 months. Note the pre-existent calcified depression (white arrows) at 3 months, which gradually improved at 12 months; Case 3 is a short tau inversion recovery axial section showing no abnormalities at 3 and 12 months (white arrows are the former defect location).
Clinical Assessment
Two weeks after surgery, all wounds were healed, and all patients had stopped using painkillers. At the clinical assessment at 3 months both patients 1 and 3 had regained full range of motion (>130° of flexion) and were playing sports under supervision while patient 2 was on schedule within the ACL protocol. At 3 months, patients 1 and 3 reported no pain and gradual return to sports. Complete return to sports was achieved after 6 months for patients 1 and 3 and after 12 months for patient 2.
Discussion
The present study describes 3 pediatric cases in which the hedgehog technique is modified to reattach shear-off chondral fragments to the subchondral bone of the knee. Thereby, to the best of our knowledge, using this technique for the first time in autografting. After 1 year, MR images showed no signs of fragment loosening. All patients completely recovered with full return to sports.
Already in the 1980s, Kaplonyi et al. investigated the use of fibrin adhesives for refixation of (osteo)chondral fragments in both animal and humans.14,15 In case of pure chondral fragments, the subchondral bone was drilled prior to fixation to allow for a healing response. 14 For osteochondral fragments, joint function after 5 years was generally good to excellent and radiographs showed good osseointegration. 14 The integration of pure chondral fragments could not be evaluated, however, due to the absence of MR images or histology. 14 In 2009, Bardos et al. 19 reported for the first time on the results of the hedgehog technique using chondral allografts to repair cartilage defects in 9-month-old pigs. The chondral allografts were prepared by removing the cartilage from the subchondral bone using a blade. It was not described if the calcified cartilage layer was included when using this harvesting method.9,19 Six weeks after the hedgehog technique, histological assessment revealed cell invasion within the incisions of the allograft. 19 Eighteen weeks later histological evidence of hyaline cartilage and complete osteochondral integration was found. The former cartilage cuts in the deep zone were no longer visible. 19 Results, based on the histological International Cartilage Repair Society score, were comparable to ACI and superior to microfracture. 19 Despite the fact that chondrocytes suffer from steric hindrance, cell migration in cartilage has been proven before in the presence of injury or lesions.25,26 The cell invasion and the following disappearance of the incisions in the study by Bardos et al. 19 are therefore indicative for cell mobility and deposition of extracellular matrix following the hedgehog technique. In 2015, the same group conducted the first clinical study of 8 focal chondral lesions in 7 patients, aged 34.3 ± 8.4 years (mean ± SD), and found reasonable results. 9 The MRI at 1- and 2-year follow-up showed normal graft intensity and graft thickness in 83% of the cases. Short Form–36 health survey and Lysholm scores increased significantly after 1 year but had dropped at the 2-year mark without clear explanation. 9 Long-term follow-up of these patients would be valuable.
Encouraged by the results of Kaplonyi et al. on the prointegrative capabilities of fibrin glue and the histological evidence of osteochondral integration provided by Bardos et al., we further modified the hedgehog technique for shear-off fragments in children. Modification included the use of autografts instead of allografts, the creation of oblique interlocking edges, the addition of using fibrin glue in between the cartilage and bone and performing the incisions freehand. Instead of drilling into the subchondral bone, as described by Kaplonyi et al., we abraded the subchondral bone to expose vital, bleeding bone. If, and how, the process of integration of allografts as described by Bardos et al. differs from the integration of shear-off autografts in this study is not known, nor is the role of potentially including the calcified cartilage layer in our cases known. Including histology in future studies could unravel these unanswered questions. Furthermore, in hedgehog allografting the appropriate graft size can be selected. In contrast, for the shear-off fragments it had to be proven that the fragments swell sufficiently to allow for trimming. It was hypothesized that the degree of swelling of pediatric cartilage would be between that of a young animal and that of osteoarthritic cartilage. The fact that all 3 fragments fitted well after modification confirmed this concept. It remains to be determined if shear-off fragments of adults swell sufficiently to allow for the same modified hedgehog technique.
Alternative methods to reattach chondral tissue have been described yielding varying success. 5 These include metal screw fixation or the use of biodegradable fixation materials.10,27 Although reasonable results can be achieved by metal screws, 27 the costs and invasiveness of an additional surgery are important drawbacks. Biodegradable fixation methods such as PLLA darts overcome the need for an additional surgery and showed promise in a small case series. 10 However, PLLA remnants and degradation products can remain present for years.28,29 These potentially jeopardize osteochondral integration due to its negative effects on chondrogenesis and bone formation.12,13 Moreover, both metal and PLLA are stiff biomaterials which can erode the opposing articulating tissues. 11 The modified hedgehog technique does not have these biomaterial-related drawbacks.
The present study has several limitations. First, we did not evaluate our clinical assessment by patient reported outcome measures. Although none of the patients reported any restriction and all had regained full functionality, validated questionnaires would have made comparison with other techniques easier. Second, therapies like microfracture also yield good results up to 2 years, making the follow-up in the present study rather short. 30 We also rationalized that the calcified layer was attached to the loose fragment, but this requires histological confirmation. Last, survival of the fragments and its viability after a period in the joint space is still not completely known. In 2007, Hembree et al. 31 investigated loose osteochondral fragments 5 days after joint trauma and found impaired chondrocyte viability at the cartilage edges but intact viability in the middle and deep zones, supporting our trimming method. In 2016, Pascual-Garrido et al. 32 found no differences in viability of chondrocytes derived from loose osteochondritis dissecans fragments and unaffected cartilage (time not mentioned). Loose fragments have even been used as viable cell source for ACI. 33 Still, it remains to be investigated what the maximum period is after trauma that such fragment can be considered viable and what the effect was of the time to surgery in current cases.
For decades, cell-based therapies have been considered most promising to regenerate hyaline cartilage. In recent years, there has been an increasing interest, however, in reintroducing intact cartilage extracellular matrix to the defect, such as with particulated cartilage. 34 In this study, the hedgehog technique showed great promise to repair shear-off lesions in children. As such, it contradicts the long-standing dogma of cartilage being indifferent and passive during cartilage repair by showing integration of full-thickness cartilage to the subchondral bone. Future researchers are encouraged to include longer follow-up periods and make comparison with established techniques. Ideally, higher tesla scans should be obtained to allow for dynamic evaluation of bone and cartilage at a highly detailed level and to allow for magnetic resonance observation of cartilage repair tissue (MOCART) scoring. 35
Footnotes
Acknowledgments and Funding
P.P.W. van Hugten, MD, of our department is gratefully acknowledged for creating Figure 3. M.J.M. Peters, MSc, of our department is gratefully acknowledged for her meaningful insights during the writing of this article. J.K. Bossen, MD (Zuyderland Medical Center), is gratefully acknowledged for providing the additional imaging files of case 2. Wiel Wijnen, nurse practitioner, is gratefully acknowledged for monitoring all the cartilage repair patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was conducted in accordance with the World Medical Association Declaration of Helsinki. The local ethics committee approved the study (2017-0183).
Informed Consent
All participants and their caretakers provided oral and written informed consent.
Trial Registration
Not applicable.