
Abstract
Objective
The purpose of this study was to investigate the degree of standardized evaluation and reporting of cartilage lesion characteristics in high-impact clinical studies for symptomatic lesions of the knee. We hypothesized that there are significant inconsistencies in reporting these metrics across orthopedic literature.
Design
A total of 113 clinical studies on articular cartilage restoration of the knee were identified from 6 high-impact orthopedic journals between 2011 and 2016. Full-text review was used to evaluate sources for details on study methodology and reporting on the following variables: primary procedure, location, size, grade, and morphology of cartilage lesions.
Results
All studies reported on the type of primary cartilage procedure and precise lesion location(s). Approximately 99.1% reported lesion morphology (chondral, osteochondral, mixed). For lesion size, 32.7% of articles did not report how size was measured and 11.5% did not report units. The lesion sizing method was variable, as 27.4% used preoperative magnetic resonance imaging to measure/report lesion size, 31.0% used arthroscopy, and 8.8% used both. The majority of studies (83.2%) used area to report size, and 5.3% used diameter. Formal grading was not reported in 17.7% of studies. Only 54.8% of studies reported depth when sizing osteochondral defects.
Conclusions
Recent literature on cartilage restoration provides adequate information on surgical technique, lesion location, and morphology. However, there is wide variation and incomplete reporting on lesion size, depth, and grading. Future clinical studies should include these important data in a consistent manner to facilitate comparison among surgical techniques.
Introduction
Articular cartilage lesions are debilitating injuries observed with a high prevalence in both the general population and high demand athletes.1-3 While the management of these injuries is complex and multifactorial, recent advancements in surgical techniques, and their subsequent clinical success, have resulted in an increased trend in operative management for symptomatic lesions.4-6 In addition to patient demographic factors (e.g., age and body mass index [BMI]), evidence-based management largely relies on accurate determination of the size/area, location, and depth of chondral defects to direct appropriate treatment strategies. Lesion characterization is often accomplished by the interpretation of advanced imaging studies (e.g., radiographs and magnetic resonance imaging [MRI]) and direct arthroscopic examination, which remains the gold standard to assess chondral/osteochondral pathology.
While current surgical algorithms rely heavily on the accurate characterization of articular cartilage defects, the extent to which current studies consistently employ and report appropriate methods for evaluating chondral pathology is unknown. Ultimately, standardized methods for evaluating these lesions facilitate meaningful data pooling and the ability to derive influential conclusions to direct clinical practice.
The purpose of this study was to document methods for evaluating cartilage lesions and to review their reporting in high-impact studies of knee cartilage surgery. We hypothesized that there would be wide variability in the methods used to evaluate and report characteristics of cartilage lesions. We aim to highlight current deficiencies and/or inconsistencies across high-impact works in order to move toward a consistent framework for evaluation in future studies.
Materials and Methods
Six high-impact orthopedic journals were selected for identification of source studies: (1) American Journal of Sports Medicine, (2) Journal of Bone and Joint Surgery–American Volume, (3) Knee Surgery, Sports Traumatology, and Arthroscopy, (4) Clinical Orthopaedics and Related Research, (5) Arthroscopy, and (6) Cartilage. All articles published in each of these journals, between January 2011 and August 2016, were reviewed to identify studies reporting clinical outcomes for treatment of articular cartilage defects of the knee. Inclusion criteria were primary research articles reporting clinical outcomes data following surgical treatment of articular cartilage lesions with a minimum sample size of 5 patients. Review articles, meta-analyses, and articles reporting only nonclinical outcomes (e.g., imaging, histology) were excluded.
Two computerized databases (PubMed, EMBASE) with a comprehensive index of each of the 6 journals were searched to identify relevant studies. “Cartilage” or “chondral” was searched with the phrases [“knee”] and [“outcomes”] as well as relevant iterations. All articles were screened initially by title and abstract to exclude irrelevant studies. Two researchers (WLS and AA) independently performed full-text review of the remaining studies to determine eligibility for inclusion. Discrepancies between reviewers were resolved through consensus with the senior authors (KJJ and SLS).
Each article was assessed to determine the following data elements of interest: lesion number, size, depth, location, grade with corresponding classification system, and lesion morphology. For each study, the level of evidence reported and primary cartilage restoration procedure was also noted. For lesion location, each article was analyzed based on whether or not the authors mentioned a focal cartilage defect in 1 of 5 location categories: (1) medial femoral condyle (MFC), (2) lateral femoral condyle (LFC), (3) patella, (4) trochlea, and (5) tibial plateau. For lesion size, the dimension of measurement (e.g., diameter or area), pre- or postdebridement size reporting, and sizing modality (MRI, arthroscopic/open-arthrotomy visualization, or both) was recorded. When reported, lesion depth was also recorded. For lesion morphology, each article was categorized based on whether cartilage lesions were characterized as chondral, osteochondral, or both. Data were recorded on whether the International Cartilage Repair Society (ICRS) or Outerbridge classification system was used to document lesion grade.
Results
Reporting on Interventions
The identified articles reported outcomes on a variety of primary procedures, including autologous chondrocyte implantation (ACI), microfracture (MF), osteochondral allograft (OCA), osteochondral autograft transfer (OATs), and other novel procedures. ACI was the most commonly reported procedure (42.5% of articles). Data on MF, OCA, and OATs were reported in 15.0%, 11.5%, and 5.3% of articles, respectively (Figure 1).
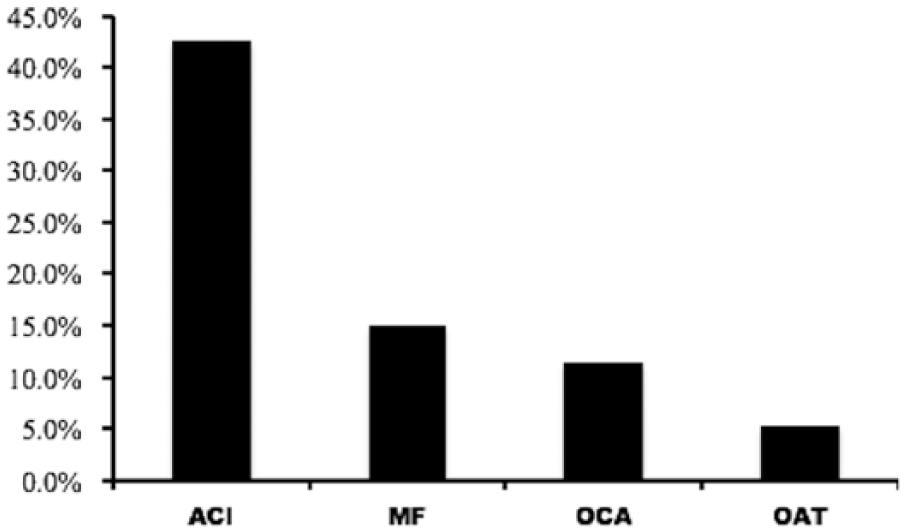
Primary intervention reported in identified article cohort (N = 113 studies).
Reporting of Chondral Lesion Characteristics
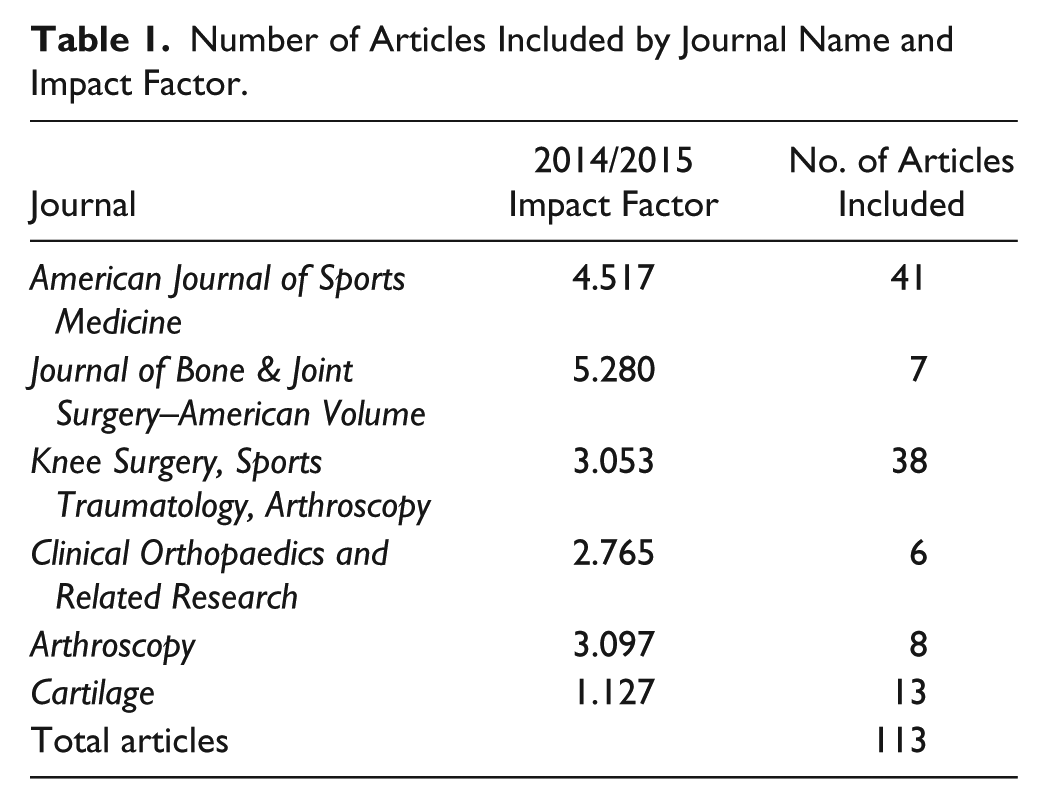
A total of 113 articles reporting clinical outcomes data on treatment of articular cartilage lesions of the knee were identified (Table 1). Of the 113 articles, only 13 studies reported clinical outcomes for singular chondral lesions, while all other studies treated multiple lesions.
Number of Articles Included by Journal Name and Impact Factor.
Across all studies, lesion locations were described anatomically using 1 of 5 categories: MFC, LFC, patella, trochlea, and tibial plateau. Of these, 85.8% of articles reported patients with lesions involving the MFC, and 81.4% reported lesions involving the LFC. Approximately 25.7%, 52.2% and 53.9% reported data on tibial plateau, patellar and trochlear lesions, respectively.
Approximately 83.2% of studies reported lesion size using area (cm2 or mm2), while 5.3% reported diameter (cm or mm); 13 studies (11.5%) did not report units or dimensions for size measurements. Lesion size was determined either by MRI (27.4%), arthroscopic visualization (31.0%), or a combination of both (8.8%); sizing modality was not reported in 32.7% of articles. Sizing was performed preoperatively in 36.3% of articles and intraoperatively in 31.0% of articles; the remaining articles did not specify when the lesion sizes were determined. When reported, lesion depth was recorded by manual probe and reported in only 31.9% of articles (Table 2).
Percent of Articles with Variations in Reporting.

Lesions were classified as chondral, osteochondral, or both depending on the degree of subchondral bone involvement. Only one article did not specify the morphology of treated lesions. Fifty-six articles (49.6%) reported chondral lesions, 31 articles (27.4%) reported osteochondral lesions, and 25 articles (22.1%) reported both. Of these, 32.0% of mixed-morphology articles and 54.8% of articles reporting osteochondral lesions reported lesion depth when sizing defects (Table 2). A total of 84.1% of studies reported cartilage grade. Of these, 87 articles (77.0%) reported grade III or higher (ICRS or Outerbridge classifications), while 8 studies (7.1%) included more superficial lesions (grade I and II lesions). An additional 15.9% of articles did not specify the grade of the cartilage lesions at the time of intervention. To characterize lesions, the ICRS classification was used in 62.8% of articles and the Outerbridge classification was used in 17.7% of articles; twenty studies (17.7%) did not specify the classification system used.
Discussion
Our study evaluated current high-impact publications on cartilage repair to determine the accuracy/standardization of reporting for lesion specific characteristics (location, morphology, and size). Of concern is the wide variability observed, which makes it difficult to critically evaluate and compare outcomes across studies and surgical techniques. Our most important findings noted that the most consistently reported lesion specific factors were location (100%), morphology (99.1%), size (88.5%) and grade (82.3%); and the least consistently reported characteristics included lesion depth (68.1%), measurement method (67.3%), and timing of the measurement (67.3%).
Clinical outcomes following cartilage repair procedures depend on many patient-specific (age, weight, BMI) and lesion-specific factors (size, depth, etc.).7-12 While patient-specific factors such as increased age and BMI tend to negatively affect clinical outcomes for some procedures, lesion specific factors and the articular comorbidities do not uniformly affect all treatment modalities.7-12 Therefore, these lesion specific factors should be considered of utmost importance when reporting outcomes in clinical studies. This is critical information when comparing clinical results, specifically with respect to understanding the reasons for operative success and failure. As such, this study sought to evaluate variability in lesion specific reporting, focusing on location, size, morphology, and advanced lesion characteristics.
Location of the lesion was described in all studies. This description is important given that better outcomes and long-term survivorship are typically reported for lesions involving the femoral condyles, with less favorable outcomes noted for lesions of the tibial plateau, trochlea and the patella.8,13,14 However, more recent studies show that with adequate realignment and unloading procedures, patellofemoral lesions can have similar outcomes to the femoral condyles.8,15 Further evidence to resolve the current conflicting results can only be possible with continued adequacy in reporting.
Accurate sizing of the lesion is a primary factor when determining treatment modalities for chondral and osteochondral lesions, as algorithms consider technical feasibility and known outcomes to define upper size limit recommendations for each intervention. In general, small lesions, <2 to 4 cm2 may be treated with MF and OATs, given comparative studies and clinical trials with conflicting outcomes do not demonstrate superior results with higher cost procedures such as cell-based therapies (ACI, matrix-induced ACI [MACI]) or OCA for such lesions.16-18 Large lesions, >2 to 4 cm2, likely have better outcomes with cell-based therapy or OCA.19-23 Currently, treatment modalities are based on absolute sizing and depth of the lesion, irrespective to the relative size of the lesion compared with the surrounding anatomic area (e.g., MFC, LFC, patella, etc.). However, it may be clinically important to note the relative size of the defect to the overall dimensions of the articular surface. For example, it is possible that a defect, while small in absolute size according to current measurement standards, encompasses a large proportion of the relevant articular surface in a patient with smaller anatomic dimensions of the femoral condyle, trochlea, or patella. Future studies should include these relative measurements to determine if relative sizing may be more important for clinical decision making.
Interestingly, while lesion size was reported in the majority of studies (88.5%), we found only 31% of studies used the widely considered gold standard of arthroscopy for lesion sizing and only 31% reported the postdebridement size. As reported by Gomoll et al., 24 there is an average difference of 65% when measuring lesion size (cm2) between preoperative measurements on MRI (by standard protocols for cartilage evaluation) and intra-operative measurements after debridement, with the MRI underestimating the lesion in 85% of cases. It is widely known that the zone of cartilage injury can extend beyond the full-thickness component of the defect, and that surrounding areas of degenerative cartilage that require debridement is difficult to accurately assess on preoperative MRI. This variation in final defect sizing (by advanced imaging or direct visualization) and timing of lesion measurement (pre- or postdebridement) highlights the importance of the need to report all sizing modalities for accurate correlation. Given the well-established correlation between clinical outcomes for various cartilage restoration procedures and lesion size, we believe standardized reporting is necessary to reliably compare results across studies and techniques. This applies to the management of both regular/circular and irregular defects alike. For these reasons, it is the authors’ opinion that if only one standardized measurement is to be reported, it should be performed after complete debridement, as this will reflect the actual/absolute size of the treated lesion, regardless of shape, relative size of the defect’s location, or defect irregularity. For irregular defects, the 2 larger diameters should be recorded. While no gold standard measurement technique exists to our knowledge, we suggest that postdebridement lesion size should be measured by a calibrated arthroscopic probe and reported as either lesion diameter (in mm) or surface area (i.e., πr2, πAB) in cm2.
Lesion morphology is an important factor when deciding between a surface-based procedure (e.g., ACI) or one that replaces the entire osteochondral unit, (e.g., OAT and OCA). This was reported adequately, along with a satisfactory rate of reporting for the grade of the lesion (ICRS or Outerbridge classifications). Interestingly, we noted that even though cartilage restoration procedures are largely indicated for advanced lesion grades (ICRS grade 3 and 4), some studies included the treatment of more superficial lesions (ICRS grade 1 and 2). Unfortunately, a direct comparison of results between advanced and more superficial lesions without adequate reporting is impossible. As noted, lesion depth was not uniformly reported in the majority of studies (55%). Management of abnormal bone is strongly guided by the depth of the lesions. In general, lesions with normal osseous architecture may be treated with standard cell based techniques, while significant subchondral bone loss or irregularity may require additional bone grafting procedures or osteochondral allograft/autograft transplantation to address these abnormalities. It is important to uniformly record lesion depth to determine if surface procedures such as ACI/MACI may be more suitable for superficial lesions that do not affect the underlying subchondral bone. In fact, recent literature suggests that even the presence of bone marrow edema can negatively affect early clinical outcomes following ACI; however, the long-term clinical relevance is unknown. 25 Overall, in order to compare clinical results and improve the management of bony pathology in cartilage defects, it is extremely important to quantify them more appropriately with regard to lesion morphology.
The present study reveals a need for standardized reporting when evaluating lesion specific factors that may influence clinical outcomes following cartilage restoration for symptomatic lesions of the knee. Overall, many of the lesion specific characteristics in clinical studies evaluating cartilage repair procedures, although extremely important, are not satisfactorily reported, and efforts to improve the quality of future studies should be undertaken. Furthermore, ongoing clinical studies should be performed prospectively or at least entail retrospective analysis of prospectively collected registry data in an effort to reduce the observed variability in this study. Additionally, data collected in this manner are less subject to selection bias than retrospective case series (level 4 evidence). Ultimately, data collection within procedure and pathology-specific registries is important to promote multicenter collaborative studies and pool data to maximize the information yield in clinical outcomes studies. Current efforts by the ICRS are using important resources and technologic infrastructure to facilitate widespread utilization of a cartilage specific database to guide future directions of research.
This study should be considered in the context of its limitations. We only included studies published in 6 high-impact orthopedic journals, including a dedicated journal to cartilage repair research, instead of searching large databases such as Pubmed, EMBASE, CINAHL, and Cochrane Collaboration Library independent of impact factors. Moreover, the study focused on the most recent 5-year period. Therefore, while these studies represent a collection of modern literature with the potential to influence practice guidelines, our results may not fully represent the average standards of publication for clinical studies in cartilage repair. Furthermore, confirming the lack of standardization of patients and lesion characteristics, even in high impact journals, suggest that the quality of currently published clinical studies is not satisfactory, as the inclusion of additional studies from lower impact journals would likely reinforce the results of the study.
In conclusion, reporting on lesion specific characteristics in clinical studies evaluating cartilage restoration procedures in the knee is widely variable and inconsistent. While important factors such as lesion location is reported amongst all studies, other important criteria such as morphology, size, and the grade are less consistent (80%). Furthermore, lesion depth, method used for size measurement and timing of the measurement are reported in approximately two-thirds of the studies. These findings highlight the need for more standardized methods to be applied in future research.
Footnotes
Authors’ Note
This study was primarily performed at the Department of Orthopedic Surgery in the David Geffen School of Medicine at UCLA.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.